Psychiatry 2009 [VOLUME 6, NUMBER 1, JANUARY] 38 ABSTRACT We performed a comprehensive review of the literature to determine whether or not a relationship between depression and coronary artery disease exists. Our literature search supports the following: Depression and coronary artery disease have a bidirectional relationship, i.e., coronary artery disease can cause depression and depression is an independent risk factor for coronary artery disease and its complications; depression may contribute to sudden cardiac death and increase all causes of cardiac mortality; and depression contributes to unhealthy lifestyle and poor adherence to treatment. We review various pathophysiological links between depression and coronary artery disease and screening for depression in at-risk patients for coronary artery disease. We also discuss pharmacological treatments, their implications, and various behavioral treatments. INTRODUCTION Coronary artery disease (CAD) has emerged as the leading cause of death and disability in the United States. DEPRESSION AND CORONARY ARTERY DISEASE: The Association, Mechanisms, and Therapeutic Implications by IMRAN SHUJA KHAWAJA, MBBS; JOSEPH J. WESTERMEYER, MD, PhD; PRASHANT GAJWANI, MD; and ROBERT E. FEINSTEIN, MD Dr. Khawaja is from Department of Psychiatry, University of Minnesota/VA Medical Center, Minneapolis, Minnesota (currently doing a fellowship in sleep medicine at the Center for Sleep Medicine, Mayo Clinic, Rochester, Minnesota); Dr. Westermeyer is from the Department of Psychiatry, University of Minnesota/VA Medical Center, Minneapolis, Minnesota; Dr. Gajwani is from the Department of Psychiatry, Case Western Reserve University School of Medicine, Cleveland, Ohio; and Dr. Feinstein is from the Department of Psychiatry, University of Colorado School of Medicine, Denver, Colorado. Psychiatry (Edgemont) 2009;6(1):38–51 FINANCIAL DISCLOSURES: Drs. Khawaja, Westermeyer, and Feinstein have no conflicts of interest relevant to this manuscript. Dr. Gajwani is a consultant or member of the speakers bureau for AstraZeneca, Forest Laboratories, Pfizer, and Cyberonics, and has received research grants from Cyberonics, Pfizer, and Bristol-Myers Squib. ADDRESS CORRESPONDENCE TO: Dr. Imran Khawaja, Center for Sleep Medicine, Mayo Clinic, 200 First Street SW, Rochester, MN 55905; E-mail: [email protected] KEY WORDS: coronary artery disease, depression, antidepressant medications, SSRIs [REVIEW]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Psychiatry 2009 [ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ]38
ABSTRACTWe performed a comprehensive
review of the literature to determinewhether or not a relationship betweendepression and coronary artery diseaseexists. Our literature search supportsthe following: Depression and coronaryartery disease have a bidirectionalrelationship, i.e., coronary arterydisease can cause depression anddepression is an independent riskfactor for coronary artery disease andits complications; depression maycontribute to sudden cardiac deathand increase all causes of cardiacmortality; and depression contributesto unhealthy lifestyle and pooradherence to treatment. We reviewvarious pathophysiological linksbetween depression and coronaryartery disease and screening fordepression in at-risk patients forcoronary artery disease. We alsodiscuss pharmacological treatments,their implications, and variousbehavioral treatments.
INTRODUCTIONCoronary artery disease (CAD) has
emerged as the leading cause of deathand disability in the United States.
DEPRESSION AND CORONARYARTERY DISEASE:The Association, Mechanisms, andTherapeutic Implicationsby IMRAN SHUJA KHAWAJA, MBBS; JOSEPH J. WESTERMEYER, MD, PhD; PRASHANT GAJWANI, MD; andROBERT E. FEINSTEIN, MDDr. Khawaja is from Department of Psychiatry, University of Minnesota/VA Medical Center, Minneapolis, Minnesota (currently doing afellowship in sleep medicine at the Center for Sleep Medicine, Mayo Clinic, Rochester, Minnesota); Dr. Westermeyer is from the Department ofPsychiatry, University of Minnesota/VA Medical Center, Minneapolis, Minnesota; Dr. Gajwani is from the Department of Psychiatry, CaseWestern Reserve University School of Medicine, Cleveland, Ohio; and Dr. Feinstein is from the Department of Psychiatry, University ofColorado School of Medicine, Denver, Colorado.
Psychiatry (Edgemont) 2009;6(1):38–51
FINANCIAL DISCLOSURES: Drs. Khawaja, Westermeyer, and Feinstein have no conflicts ofinterest relevant to this manuscript. Dr. Gajwani is a consultant or member of the speakersbureau for AstraZeneca, Forest Laboratories, Pfizer, and Cyberonics, and has received researchgrants from Cyberonics, Pfizer, and Bristol-Myers Squib.
ADDRESS CORRESPONDENCE TO: Dr. Imran Khawaja, Center for Sleep Medicine, Mayo Clinic,200 First Street SW, Rochester, MN 55905; E-mail: [email protected]
KEY WORDS: coronary artery disease, depression, antidepressant medications, SSRIs
[ R E V I E W ]

[ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ] Psychiatry 2009 39
According to an estimate by the WorldHealth Organization (WHO), by theyear 2020, both CAD and depressionwill be the two major causes ofdisability-adjusted life years.1 CADcontinues to be a major focus ofclinical and epidemiological research.Nonmodifiable cardiovascular riskfactors, such as age, gender, familyhistory, and race, as well as modifiablerisk factors, such as hypertension,weight, smoking, sedentary lifestyle,abnormal lipid profiles, inflammatorymarkers, diabetes, metabolicsyndrome, and subclinical CAD, areassociated with increasedcardiovascular risk.2–7
Despite these findings, typicallymeasured risk factors do not fullyaccount for all the variation inoutcomes.8 There is a lack of adefinitive correlation between high-risk profiles, biological profiles, and theoccurrence of CAD. A number ofpsychological states and traits, such asdepression, anxiety, anger, and stress,have also been implicated as potentialrisk factors for CAD.
BIDIRECTIONAL RELATIONSHIP OFDEPRESSION AND CAD
Cross-sectional and longitudinaldata suggest a bidirectional linkbetween depression and CAD.
CAD can cause majordepressive disorder. In cross-sectional studies done in the past,between 19 and 66 percent of patientswith myocardial infarction (MI) havesome mental disorder, primarilydepressive and anxiety states.9,10,11–14 Inseveral studies,15–17 17 to 44 percent ofpatients with CAD also have adiagnosis of major depression. Anotherstudy found that 27 percent ofpatients undergoing coronary arterybypass graft surgery (CABG) haddepression after the surgery.18
In an another study,19 a history ofMI was independently associated within-hospital depressive symptoms.Results of these studies with highprevalence of depression in thispopulation of CAD patients gain moresignificance when they are comparedto 6.6 percent one-year prevalence ofmajor depressive disorder in acommunity sample.20
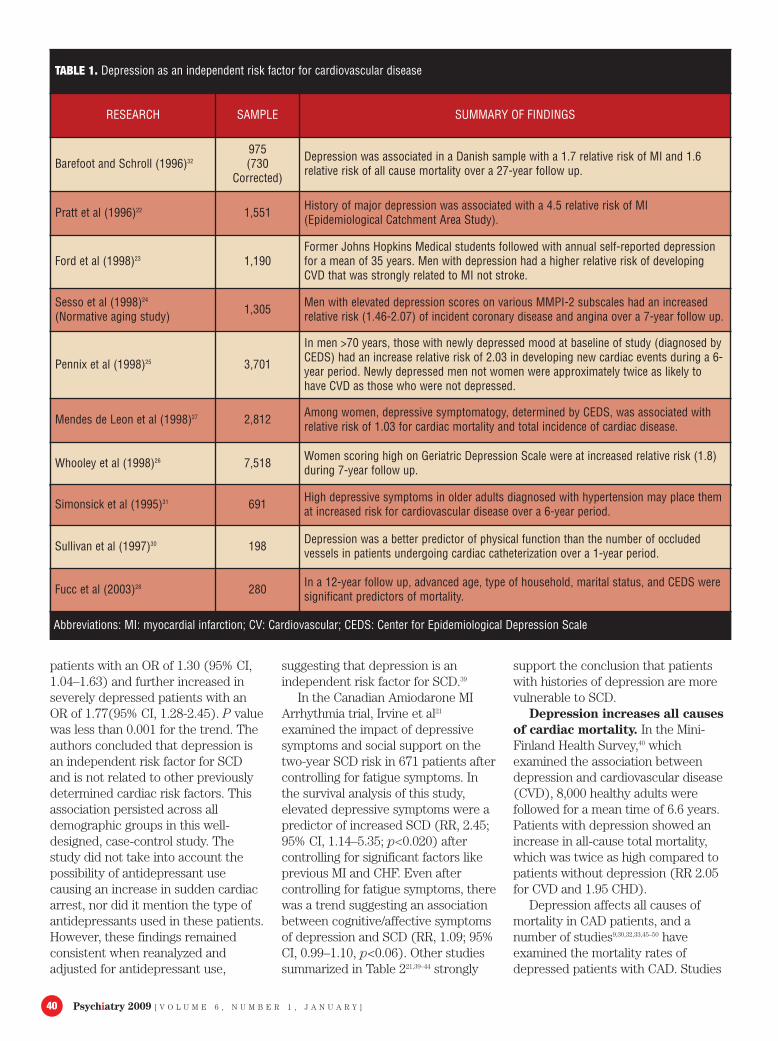
Depression is an independentrisk factor for CAD and itscomplications. The role ofdepression in the pathogenesis of CADhas been examined in variouslongitudinal studies.21–29 Studiessummarized in Table 1 support thetheory that depression is anindependent risk factor fordevelopment of CAD and itscomplications.22–28,30–32
In the Baltimore cohort of theEpidemiologic Catchments Area(ECA) Study, patients with a history ofdysphoria or depression have 4.5 timesthe relative risk of having an acute MIat follow up compared tonondepressed patients, independent ofthe coronary artery risk factors.22
Lesperance et al33 examined 222patients for depression after they wereadmitted to the hospital for acute MI.Patients were evaluated for depressionusing a modified version of theDiagnostic International Schedule(DIS). Depression ratings werecompleted at the initial hospitalizationfor MI and at one week, six months,and 12 months post-MI. This studycontrolled for patient’s age andcardiovascular health. At six months, 6to 12 months, and 13 to 18 months,there were six, seven, and eightdeaths, respectively (total of 21deaths), which were all associatedwith depression. Also patients whohad depression during hospitalizationwere more likely to have had previousdepression and to become depressedafter discharge.
The onset of an MI is oftenobserved to be preceded by aprodrome of decreasing energy,general malaise, and minordepression.34 In a large, prospective,follow-up study35 of 4,367 men andwomen older than 60 with isolatedsystolic hypertension, the risk of death(RR, 1.25; 95% CI, 1.15–1.36) andstroke or MI (RR, 1.18; 95% CI,1.08–1.30) was associated with aprogressive increase in depressivesymptoms during an average follow-uptime of 4.5 years
Previous history of depression is apredictor of congestive hear failure(CHF) after an acute MI.36 In amulticenter trial, Lauzon et al37
followed patients for a year to measureprevalence and prognostic effects ofdepression after acute MI. In recruitedpatients, a nurse practitionerdocumented acute MI within 2 to 3days of admission. Patients completedBeck Depression Inventory (BDI)during their hospitalization and then at30 days, six months, and one yearpost-MI.
Depressed patients had higher ratesof cardiac complications, includingrecurrent ischemia, infarction, or CHFduring their first hospital stay orreadmission for angina, recurrentacute MI, CHF, or arrhythmias(adjusted HR 1.4, 95% CI 1.05–1.86)as compared to nondepressedpatients.38 These results wereconsistent across all demographicsubgroups. These studies further addto the significance of depression andCAD relationship as they suggest thatdepression has an effect on CAD aswell as on its complications.
DEPRESSION CAN CAUSE SUDDENCARDIAC DEATH AND INCREASESALL CAUSES OF CARDIACMORTALITY
Depression and sudden cardiacdeath (SCD). Several studies suggestthat patients who experiencedepression after an MI are at higherrisk for SCD. In a Washington statehealth maintenance organization(HMO) study from 1980 to 1994,Empana et al39 compared 2,228patients with depression to a controlgroup of 4,164 patients. Patients inboth groups were ages 40 to 79. Hefound that presence and severity ofclinical depression in patients isassociated with higher risk of cardiacarrest resulting in death. In this case-controlled study, they found thatclinically depressed patients had ahigher odds ratio (OR) of a cardiacarrest (OR, 1.88; 95% CI, 1.59–2.23).This finding persisted even afteradjustment for confounding factors,such as cigarette smoking, heavyalcohol consumption, diabetes,hypertension, prior MI, and prior CHF(OR, 1.43; 95% CI, 1.18–1.73).Compared with nondepressedpatients, the risk of cardiac arrestincreased in less severely depressed
Psychiatry 2009 [ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ]40
patients with an OR of 1.30 (95% CI,1.04–1.63) and further increased inseverely depressed patients with anOR of 1.77(95% CI, 1.28-2.45). P valuewas less than 0.001 for the trend. Theauthors concluded that depression isan independent risk factor for SCDand is not related to other previouslydetermined cardiac risk factors. Thisassociation persisted across alldemographic groups in this well-designed, case-control study. Thestudy did not take into account thepossibility of antidepressant usecausing an increase in sudden cardiacarrest, nor did it mention the type ofantidepressants used in these patients.However, these findings remainedconsistent when reanalyzed andadjusted for antidepressant use,
suggesting that depression is anindependent risk factor for SCD.39
In the Canadian Amiodarone MIArrhythmia trial, Irvine et al21
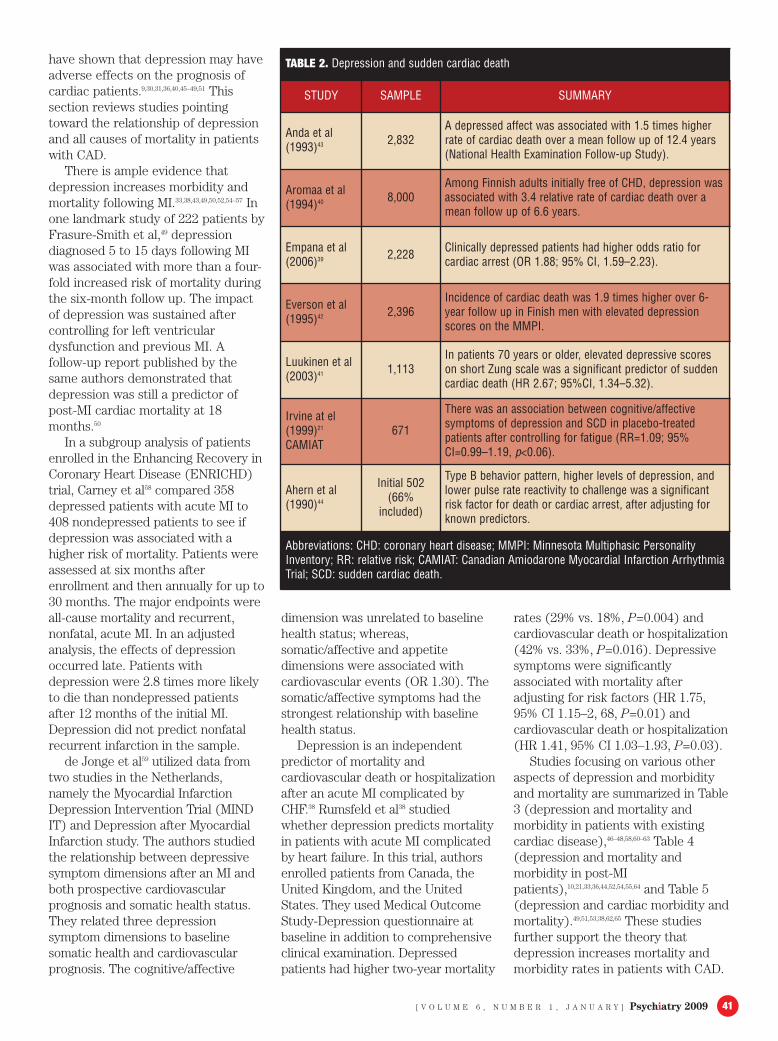
examined the impact of depressivesymptoms and social support on thetwo-year SCD risk in 671 patients aftercontrolling for fatigue symptoms. Inthe survival analysis of this study,elevated depressive symptoms were apredictor of increased SCD (RR, 2.45;95% CI, 1.14–5.35; p<0.020) aftercontrolling for significant factors likeprevious MI and CHF. Even aftercontrolling for fatigue symptoms, therewas a trend suggesting an associationbetween cognitive/affective symptomsof depression and SCD (RR, 1.09; 95%CI, 0.99–1.10, p<0.06). Other studiessummarized in Table 221,39–44 strongly
support the conclusion that patientswith histories of depression are morevulnerable to SCD.
Depression increases all causesof cardiac mortality. In the Mini-Finland Health Survey,40 whichexamined the association betweendepression and cardiovascular disease(CVD), 8,000 healthy adults werefollowed for a mean time of 6.6 years.Patients with depression showed anincrease in all-cause total mortality,which was twice as high compared topatients without depression (RR 2.05for CVD and 1.95 CHD).
Depression affects all causes ofmortality in CAD patients, and anumber of studies9,30,32,33,45–50 haveexamined the mortality rates ofdepressed patients with CAD. Studies
TABLE 1. Depression as an independent risk factor for cardiovascular disease
RESEARCH SAMPLE SUMMARY OF FINDINGS
Barefoot and Schroll (1996)32
975(730
Corrected)
Depression was associated in a Danish sample with a 1.7 relative risk of MI and 1.6relative risk of all cause mortality over a 27-year follow up.
Pratt et al (1996)22 1,551 History of major depression was associated with a 4.5 relative risk of MI(Epidemiological Catchment Area Study).
Ford et al (1998)23 1,190Former Johns Hopkins Medical students followed with annual self-reported depressionfor a mean of 35 years. Men with depression had a higher relative risk of developingCVD that was strongly related to MI not stroke.
Sesso et al (1998)24
(Normative aging study) 1,305 Men with elevated depression scores on various MMPI-2 subscales had an increasedrelative risk (1.46-2.07) of incident coronary disease and angina over a 7-year follow up.
Pennix et al (1998)25 3,701
In men >70 years, those with newly depressed mood at baseline of study (diagnosed byCEDS) had an increase relative risk of 2.03 in developing new cardiac events during a 6-year period. Newly depressed men not women were approximately twice as likely tohave CVD as those who were not depressed.
Mendes de Leon et al (1998)27 2,812 Among women, depressive symptomatogy, determined by CEDS, was associated withrelative risk of 1.03 for cardiac mortality and total incidence of cardiac disease.
Whooley et al (1998)26 7,518 Women scoring high on Geriatric Depression Scale were at increased relative risk (1.8)during 7-year follow up.
Simonsick et al (1995)31 691 High depressive symptoms in older adults diagnosed with hypertension may place themat increased risk for cardiovascular disease over a 6-year period.
Sullivan et al (1997)30 198 Depression was a better predictor of physical function than the number of occludedvessels in patients undergoing cardiac catheterization over a 1-year period.
Fucc et al (2003)28 280 In a 12-year follow up, advanced age, type of household, marital status, and CEDS weresignificant predictors of mortality.
Abbreviations: MI: myocardial infarction; CV: Cardiovascular; CEDS: Center for Epidemiological Depression Scale
[ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ] Psychiatry 2009 41
have shown that depression may haveadverse effects on the prognosis ofcardiac patients.9,30,31,36,40,45–49,51 Thissection reviews studies pointingtoward the relationship of depressionand all causes of mortality in patientswith CAD.
There is ample evidence thatdepression increases morbidity andmortality following MI.33,38,43,49,50,52,54–57 Inone landmark study of 222 patients byFrasure-Smith et al,49 depressiondiagnosed 5 to 15 days following MIwas associated with more than a four-fold increased risk of mortality duringthe six-month follow up. The impactof depression was sustained aftercontrolling for left ventriculardysfunction and previous MI. Afollow-up report published by thesame authors demonstrated thatdepression was still a predictor ofpost-MI cardiac mortality at 18months.50
In a subgroup analysis of patientsenrolled in the Enhancing Recovery inCoronary Heart Disease (ENRICHD)trial, Carney et al58 compared 358depressed patients with acute MI to408 nondepressed patients to see ifdepression was associated with ahigher risk of mortality. Patients wereassessed at six months afterenrollment and then annually for up to30 months. The major endpoints wereall-cause mortality and recurrent,nonfatal, acute MI. In an adjustedanalysis, the effects of depressionoccurred late. Patients withdepression were 2.8 times more likelyto die than nondepressed patientsafter 12 months of the initial MI.Depression did not predict nonfatalrecurrent infarction in the sample.
de Jonge et al59 utilized data fromtwo studies in the Netherlands,namely the Myocardial InfarctionDepression Intervention Trial (MINDIT) and Depression after MyocardialInfarction study. The authors studiedthe relationship between depressivesymptom dimensions after an MI andboth prospective cardiovascularprognosis and somatic health status.They related three depressionsymptom dimensions to baselinesomatic health and cardiovascularprognosis. The cognitive/affective
dimension was unrelated to baselinehealth status; whereas,somatic/affective and appetitedimensions were associated withcardiovascular events (OR 1.30). Thesomatic/affective symptoms had thestrongest relationship with baselinehealth status.
Depression is an independentpredictor of mortality andcardiovascular death or hospitalizationafter an acute MI complicated byCHF.38 Rumsfeld et al38 studiedwhether depression predicts mortalityin patients with acute MI complicatedby heart failure. In this trial, authorsenrolled patients from Canada, theUnited Kingdom, and the UnitedStates. They used Medical OutcomeStudy-Depression questionnaire atbaseline in addition to comprehensiveclinical examination. Depressedpatients had higher two-year mortality
rates (29% vs. 18%, P=0.004) andcardiovascular death or hospitalization(42% vs. 33%, P=0.016). Depressivesymptoms were significantlyassociated with mortality afteradjusting for risk factors (HR 1.75,95% CI 1.15–2, 68, P=0.01) andcardiovascular death or hospitalization(HR 1.41, 95% CI 1.03–1.93, P=0.03).
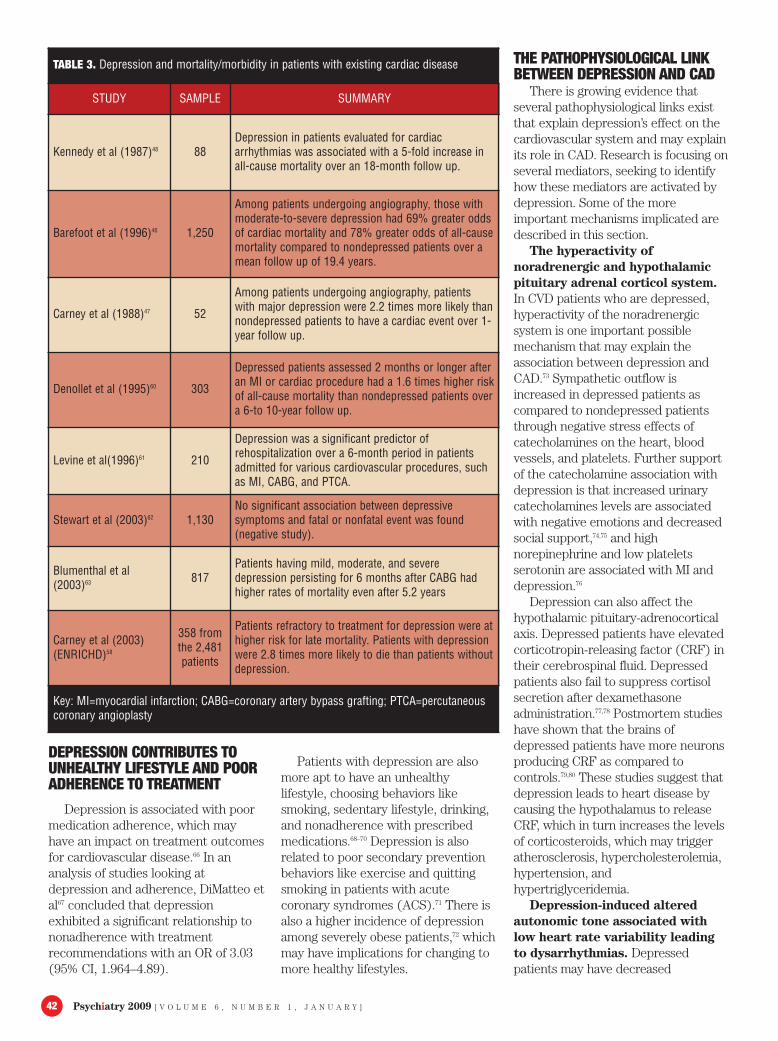
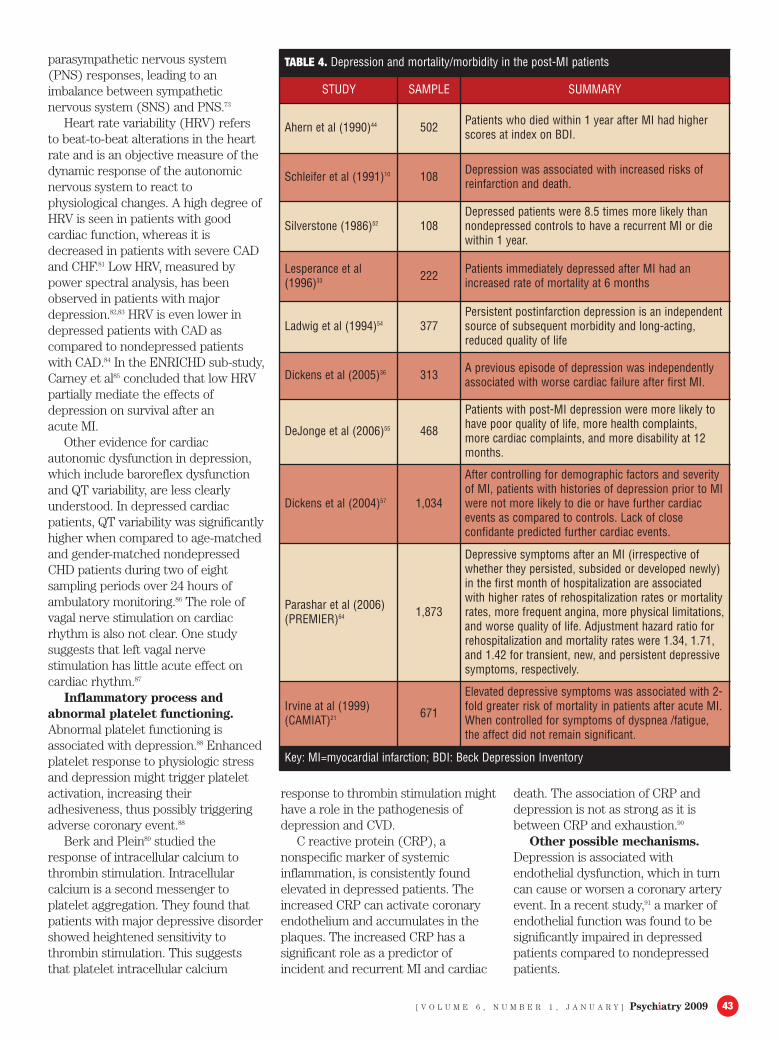
Studies focusing on various otheraspects of depression and morbidityand mortality are summarized in Table3 (depression and mortality andmorbidity in patients with existingcardiac disease),46–48,58,60–63 Table 4(depression and mortality andmorbidity in post-MIpatients),10,21,33,36,44,52,54,55,64 and Table 5(depression and cardiac morbidity andmortality).49,51,53,38,62,65 These studiesfurther support the theory thatdepression increases mortality andmorbidity rates in patients with CAD.
TABLE 2. Depression and sudden cardiac death
STUDY SAMPLE SUMMARY
Anda et al(1993)43 2,832
A depressed affect was associated with 1.5 times higherrate of cardiac death over a mean follow up of 12.4 years(National Health Examination Follow-up Study).
Aromaa et al(1994)40 8,000
Among Finnish adults initially free of CHD, depression wasassociated with 3.4 relative rate of cardiac death over amean follow up of 6.6 years.
Empana et al(2006)39 2,228 Clinically depressed patients had higher odds ratio for
cardiac arrest (OR 1.88; 95% CI, 1.59–2.23).
Everson et al(1995)42 2,396
Incidence of cardiac death was 1.9 times higher over 6-year follow up in Finish men with elevated depressionscores on the MMPI.
Luukinen et al(2003)41 1,113
In patients 70 years or older, elevated depressive scoreson short Zung scale was a significant predictor of suddencardiac death (HR 2.67; 95%CI, 1.34–5.32).
Irvine at el(1999)21
CAMIAT671
There was an association between cognitive/affectivesymptoms of depression and SCD in placebo-treatedpatients after controlling for fatigue (RR=1.09; 95%CI=0.99–1.19, p<0.06).
Ahern et al(1990)44
Initial 502(66%
included)
Type B behavior pattern, higher levels of depression, andlower pulse rate reactivity to challenge was a significantrisk factor for death or cardiac arrest, after adjusting forknown predictors.
Abbreviations: CHD: coronary heart disease; MMPI: Minnesota Multiphasic PersonalityInventory; RR: relative risk; CAMIAT: Canadian Amiodarone Myocardial Infarction ArrhythmiaTrial; SCD: sudden cardiac death.
Psychiatry 2009 [ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ]42
DEPRESSION CONTRIBUTES TOUNHEALTHY LIFESTYLE AND POORADHERENCE TO TREATMENT
Depression is associated with poormedication adherence, which mayhave an impact on treatment outcomesfor cardiovascular disease.66 In ananalysis of studies looking atdepression and adherence, DiMatteo etal67 concluded that depressionexhibited a significant relationship tononadherence with treatmentrecommendations with an OR of 3.03(95% CI, 1.964–4.89).
Patients with depression are alsomore apt to have an unhealthylifestyle, choosing behaviors likesmoking, sedentary lifestyle, drinking,and nonadherence with prescribedmedications.68–70 Depression is alsorelated to poor secondary preventionbehaviors like exercise and quittingsmoking in patients with acutecoronary syndromes (ACS).71 There isalso a higher incidence of depressionamong severely obese patients,72 whichmay have implications for changing tomore healthy lifestyles.
THE PATHOPHYSIOLOGICAL LINKBETWEEN DEPRESSION AND CAD
There is growing evidence thatseveral pathophysiological links existthat explain depression’s effect on thecardiovascular system and may explainits role in CAD. Research is focusing onseveral mediators, seeking to identifyhow these mediators are activated bydepression. Some of the moreimportant mechanisms implicated aredescribed in this section.
The hyperactivity ofnoradrenergic and hypothalamicpituitary adrenal corticol system.In CVD patients who are depressed,hyperactivity of the noradrenergicsystem is one important possiblemechanism that may explain theassociation between depression andCAD.73 Sympathetic outflow isincreased in depressed patients ascompared to nondepressed patientsthrough negative stress effects ofcatecholamines on the heart, bloodvessels, and platelets. Further supportof the catecholamine association withdepression is that increased urinarycatecholamines levels are associatedwith negative emotions and decreasedsocial support,74,75 and highnorepinephrine and low plateletsserotonin are associated with MI anddepression.76
Depression can also affect thehypothalamic pituitary-adrenocorticalaxis. Depressed patients have elevatedcorticotropin-releasing factor (CRF) intheir cerebrospinal fluid. Depressedpatients also fail to suppress cortisolsecretion after dexamethasoneadministration.77,78 Postmortem studieshave shown that the brains ofdepressed patients have more neuronsproducing CRF as compared tocontrols.79,80 These studies suggest thatdepression leads to heart disease bycausing the hypothalamus to releaseCRF, which in turn increases the levelsof corticosteroids, which may triggeratherosclerosis, hypercholesterolemia,hypertension, andhypertriglyceridemia.
Depression-induced alteredautonomic tone associated withlow heart rate variability leadingto dysarrhythmias. Depressedpatients may have decreased
TABLE 3. Depression and mortality/morbidity in patients with existing cardiac disease
STUDY SAMPLE SUMMARY
Kennedy et al (1987)48 88Depression in patients evaluated for cardiacarrhythmias was associated with a 5-fold increase inall-cause mortality over an 18-month follow up.
Barefoot et al (1996)46 1,250
Among patients undergoing angiography, those withmoderate-to-severe depression had 69% greater oddsof cardiac mortality and 78% greater odds of all-causemortality compared to nondepressed patients over amean follow up of 19.4 years.
Carney et al (1988)47 52
Among patients undergoing angiography, patientswith major depression were 2.2 times more likely thannondepressed patients to have a cardiac event over 1-year follow up.
Denollet et al (1995)60 303
Depressed patients assessed 2 months or longer afteran MI or cardiac procedure had a 1.6 times higher riskof all-cause mortality than nondepressed patients overa 6-to 10-year follow up.
Levine et al(1996)61 210
Depression was a significant predictor ofrehospitalization over a 6-month period in patientsadmitted for various cardiovascular procedures, suchas MI, CABG, and PTCA.
Stewart et al (2003)62 1,130No significant association between depressivesymptoms and fatal or nonfatal event was found(negative study).
Blumenthal et al(2003)63 817
Patients having mild, moderate, and severedepression persisting for 6 months after CABG hadhigher rates of mortality even after 5.2 years
Carney et al (2003)(ENRICHD)58
358 fromthe 2,481patients
Patients refractory to treatment for depression were athigher risk for late mortality. Patients with depressionwere 2.8 times more likely to die than patients withoutdepression.
Key: MI=myocardial infarction; CABG=coronary artery bypass grafting; PTCA=percutaneouscoronary angioplasty
[ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ] Psychiatry 2009 43
parasympathetic nervous system(PNS) responses, leading to animbalance between sympatheticnervous system (SNS) and PNS.73
Heart rate variability (HRV) refersto beat-to-beat alterations in the heartrate and is an objective measure of thedynamic response of the autonomicnervous system to react tophysiological changes. A high degree ofHRV is seen in patients with goodcardiac function, whereas it isdecreased in patients with severe CADand CHF.81 Low HRV, measured bypower spectral analysis, has beenobserved in patients with majordepression.82,83 HRV is even lower indepressed patients with CAD ascompared to nondepressed patientswith CAD.84 In the ENRICHD sub-study,Carney et al85 concluded that low HRVpartially mediate the effects ofdepression on survival after an acute MI.
Other evidence for cardiacautonomic dysfunction in depression,which include baroreflex dysfunctionand QT variability, are less clearlyunderstood. In depressed cardiacpatients, QT variability was significantlyhigher when compared to age-matchedand gender-matched nondepressedCHD patients during two of eightsampling periods over 24 hours ofambulatory monitoring.86 The role ofvagal nerve stimulation on cardiacrhythm is also not clear. One studysuggests that left vagal nervestimulation has little acute effect oncardiac rhythm.87
Inflammatory process andabnormal platelet functioning.Abnormal platelet functioning isassociated with depression.88 Enhancedplatelet response to physiologic stressand depression might trigger plateletactivation, increasing theiradhesiveness, thus possibly triggeringadverse coronary event.88
Berk and Plein89 studied theresponse of intracellular calcium tothrombin stimulation. Intracellularcalcium is a second messenger toplatelet aggregation. They found thatpatients with major depressive disordershowed heightened sensitivity tothrombin stimulation. This suggeststhat platelet intracellular calcium
response to thrombin stimulation mighthave a role in the pathogenesis ofdepression and CVD.
C reactive protein (CRP), anonspecific marker of systemicinflammation, is consistently foundelevated in depressed patients. Theincreased CRP can activate coronaryendothelium and accumulates in theplaques. The increased CRP has asignificant role as a predictor ofincident and recurrent MI and cardiac
death. The association of CRP anddepression is not as strong as it isbetween CRP and exhaustion.90
Other possible mechanisms.Depression is associated withendothelial dysfunction, which in turncan cause or worsen a coronary arteryevent. In a recent study,91 a marker ofendothelial function was found to besignificantly impaired in depressedpatients compared to nondepressedpatients.
TABLE 4. Depression and mortality/morbidity in the post-MI patients
STUDY SAMPLE SUMMARY
Ahern et al (1990)44 502 Patients who died within 1 year after MI had higherscores at index on BDI.
Schleifer et al (1991)10 108 Depression was associated with increased risks ofreinfarction and death.
Silverstone (1986)52 108Depressed patients were 8.5 times more likely thannondepressed controls to have a recurrent MI or diewithin 1 year.
Lesperance et al(1996)33 222 Patients immediately depressed after MI had an
increased rate of mortality at 6 months
Ladwig et al (1994)54 377Persistent postinfarction depression is an independentsource of subsequent morbidity and long-acting,reduced quality of life
Dickens et al (2005)36 313 A previous episode of depression was independentlyassociated with worse cardiac failure after first MI.
DeJonge et al (2006)55 468
Patients with post-MI depression were more likely tohave poor quality of life, more health complaints,more cardiac complaints, and more disability at 12months.
Dickens et al (2004)57 1,034
After controlling for demographic factors and severityof MI, patients with histories of depression prior to MIwere not more likely to die or have further cardiacevents as compared to controls. Lack of closeconfidante predicted further cardiac events.
Parashar et al (2006)(PREMIER)64 1,873
Depressive symptoms after an MI (irrespective ofwhether they persisted, subsided or developed newly)in the first month of hospitalization are associatedwith higher rates of rehospitalization rates or mortalityrates, more frequent angina, more physical limitations,and worse quality of life. Adjustment hazard ratio forrehospitalization and mortality rates were 1.34, 1.71,and 1.42 for transient, new, and persistent depressivesymptoms, respectively.
Irvine at al (1999)(CAMIAT)21 671
Elevated depressive symptoms was associated with 2-fold greater risk of mortality in patients after acute MI.When controlled for symptoms of dyspnea /fatigue,the affect did not remain significant.
Key: MI=myocardial infarction; BDI: Beck Depression Inventory

Psychiatry 2009 [ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ]44
There is some evidence that lowred blood cell membrane levels of n-3polyunsaturated fatty acids areassociated with depression, which inturn can increase the risk of SCD.92
Less is known about the triadicrelationship among immune systemparameters, psychological factors, andCVD.90
Other immunological markers likeinterleukin 6 and tumor necrosis factorare elevated in depressed patients andin patients with CAD.90 Similarly,chronic infection and elevated levels ofantibodies to several pathogens areassociated with depression. However,another study suggested that theassociation may be confined topatients who are older and who areclinically depressed.93
SCREENING FOR DEPRESSION INAT-RISK PATIENTS FOR CAD
It is our opinion that physiciansshould screen all CAD patients for
depression. There is compellingevidence that depression affectscardiac mortality and morbidity,lifestyle, and medical adherence.Screening for depression in theprimary care setting can improveclinical outcomes.94 Moreover, rapidassessment of depression can also helpidentify patients at risk for poorsecondary prevention outcomes.71
Further, adding to the argument ofscreening is the evidence thattreatment of depression withantidepressants is safe in patients withCAD.95,97
A recent nationwide survey108 ofcardiovascular physicians wasconducted to determine their methodsto diagnose depression, determinetheir beliefs about the associationbetween depression and CVD, referralpatterns for depressed patients, andthe frequency of use and choice ofantidepressant medications. Thisrandomized, cross-sectional survey of
50 percent of US cardiovascularphysicians revealed that 71.2 percentof the cardiovascular physicians askless than half of their patients withCAD about depression and that 79percent of them use no standardscreening tool to diagnose depression.Of these physicians, 84.8 percent saidthat between 1 and 50 percent of theirpatients have depression; howeveronly 49.2 percent stated that they treatdepression.
Interestingly, this study alsorevealed that cardiovascular physiciansare aware of the indirect associationbetween depression and CAD, butsurprisingly 49 percent were unawareof depression as an independent riskfactor for CAD.
Some of the most frequently useddepression screening instruments arePRIME MD® PHQ 9 (Primary CareEvaluation of Mental Disorders PatientHealth Questionnaire), HospitalAnxiety and Depression Scale (HADS),Cardiac Depression Scale (CDS), andCardiac Depression Visual AnalogueScale (CD-VAS). BDI, HamiltonDepression Scale (HAM-D), andSymptom Checklist 90 (SCL 90) canbe used for diagnosing minor andmajor depression.96
HADS has 81-percent sensitivityand 54-percent specificity todetermine a PRIME MD diagnosis ofmajor depressive disorder.98 The CDSis suitable to diagnose and screen forless severe depressive symptoms,99 andthe CD-VAS is also a useful tool forrepeated assessments of depressivesymptoms in cardiac patients.100
The authors recommend usingPHQ-9 for screening for depression inCAD patients. It has been frequentlyused by primary care physicians todiagnose depression, and when used ina collaborative care model, can alsohelp physicians treat depression moreeffectively.101 There is also a trend bysome large insurers to reimburse forthese screenings.
One study recommended screeningpatients one month after coronaryrevascularization rather than at thetime of revascularization, as twomonths and six monthspostrevascularization are strongerpredictors of depression.102 Table 6
TABLE 5. Depression and cardiac morbidity and mortality
STUDY SAMPLE SUMMARY
Wassertheil-Smoller et al(2004) (TheWomen’s HealthInitiativeObservationalStudy)51
93,676
Older women were followed for 4.1 years. Depressionwas significantly related to CVD risk and comorbidity.Among women without history of CVD, history ofdepression was an independent predictor of CVD andall-cause mortality.
Frasure-Smith et al(1993)49 222
Adjusted 6-month all-cause mortality was 4.2 timeshigher in patients with major depression than innondepressed patients.
Ladwig et al(1991)53 560 Six-month cardiac mortality was 4.9 times higher in
depressed than nondepressed patients.
Rumsfeld et al(2003)65 526
After adjusting for various risk factors, history ofdepression was a significantly associated with moreangina, greater physical limitations and worse qualityof life.
Stewart et al(2003)62 1,130
Modest association between depressive symptoms andcardiovascular events was found, but not forcardiovascular death (negative study).
Rumsfeld et al(2005)38 143
Depressed patients had a higher 2-year mortality, rateof CVD, or hospitalization. Even after risk adjustment,depression remained significantly associated withmortality, CVD, or hospitalization.
Abbreviations: MI=myocardial infarction; CABG=coronary artery bypass grafting;CVD=cardiovascular disease; PREMIER=Prospective Registry Evaluating Outcomes afterMyocardial Infarction: Events and Recovery; CAMIAT=Canadian Amiodarone MyocardialInfarction Arrhythmia Trial; ENRICHD=Enhancing Recovery in Coronary Heart Disease
[ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ] Psychiatry 2009 4545
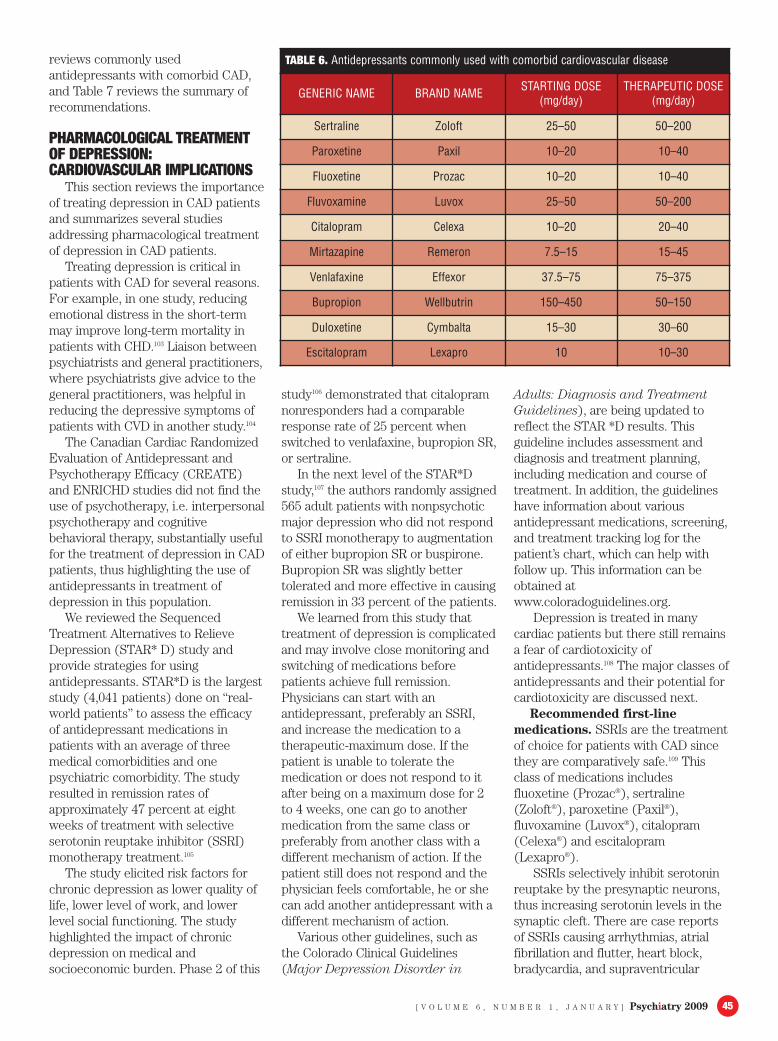
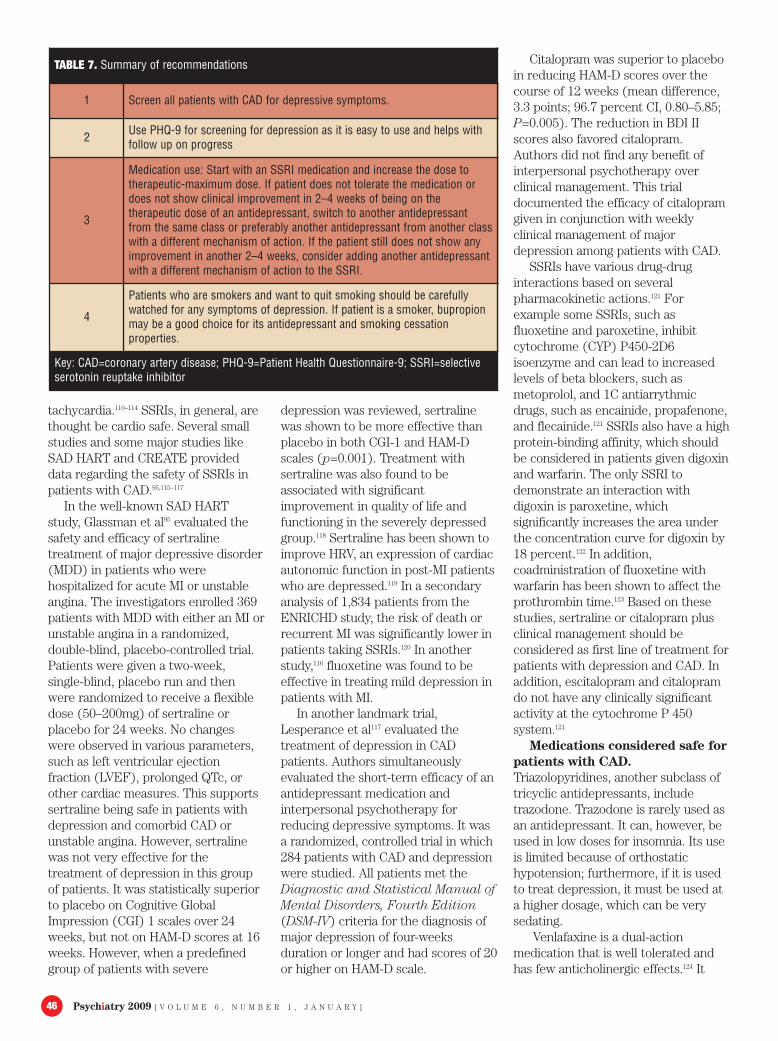
reviews commonly usedantidepressants with comorbid CAD,and Table 7 reviews the summary ofrecommendations.
PHARMACOLOGICAL TREATMENTOF DEPRESSION:CARDIOVASCULAR IMPLICATIONS
This section reviews the importanceof treating depression in CAD patientsand summarizes several studiesaddressing pharmacological treatmentof depression in CAD patients.
Treating depression is critical inpatients with CAD for several reasons.For example, in one study, reducingemotional distress in the short-termmay improve long-term mortality inpatients with CHD.103 Liaison betweenpsychiatrists and general practitioners,where psychiatrists give advice to thegeneral practitioners, was helpful inreducing the depressive symptoms ofpatients with CVD in another study.104
The Canadian Cardiac RandomizedEvaluation of Antidepressant andPsychotherapy Efficacy (CREATE)and ENRICHD studies did not find theuse of psychotherapy, i.e. interpersonalpsychotherapy and cognitivebehavioral therapy, substantially usefulfor the treatment of depression in CADpatients, thus highlighting the use ofantidepressants in treatment ofdepression in this population.
We reviewed the SequencedTreatment Alternatives to RelieveDepression (STAR* D) study andprovide strategies for usingantidepressants. STAR*D is the largeststudy (4,041 patients) done on “real-world patients” to assess the efficacyof antidepressant medications inpatients with an average of threemedical comorbidities and onepsychiatric comorbidity. The studyresulted in remission rates ofapproximately 47 percent at eightweeks of treatment with selectiveserotonin reuptake inhibitor (SSRI)monotherapy treatment.105
The study elicited risk factors forchronic depression as lower quality oflife, lower level of work, and lowerlevel social functioning. The studyhighlighted the impact of chronicdepression on medical andsocioeconomic burden. Phase 2 of this
study106 demonstrated that citalopramnonresponders had a comparableresponse rate of 25 percent whenswitched to venlafaxine, bupropion SR,or sertraline.
In the next level of the STAR*Dstudy,107 the authors randomly assigned565 adult patients with nonpsychoticmajor depression who did not respondto SSRI monotherapy to augmentationof either bupropion SR or buspirone.Bupropion SR was slightly bettertolerated and more effective in causingremission in 33 percent of the patients.
We learned from this study thattreatment of depression is complicatedand may involve close monitoring andswitching of medications beforepatients achieve full remission.Physicians can start with anantidepressant, preferably an SSRI,and increase the medication to atherapeutic-maximum dose. If thepatient is unable to tolerate themedication or does not respond to itafter being on a maximum dose for 2to 4 weeks, one can go to anothermedication from the same class orpreferably from another class with adifferent mechanism of action. If thepatient still does not respond and thephysician feels comfortable, he or shecan add another antidepressant with adifferent mechanism of action.
Various other guidelines, such asthe Colorado Clinical Guidelines(Major Depression Disorder in
Adults: Diagnosis and TreatmentGuidelines), are being updated toreflect the STAR *D results. Thisguideline includes assessment anddiagnosis and treatment planning,including medication and course oftreatment. In addition, the guidelineshave information about variousantidepressant medications, screening,and treatment tracking log for thepatient’s chart, which can help withfollow up. This information can beobtained atwww.coloradoguidelines.org.
Depression is treated in manycardiac patients but there still remainsa fear of cardiotoxicity ofantidepressants.108 The major classes ofantidepressants and their potential forcardiotoxicity are discussed next.
Recommended first-linemedications. SSRIs are the treatmentof choice for patients with CAD sincethey are comparatively safe.109 Thisclass of medications includesfluoxetine (Prozac®), sertraline(Zoloft®), paroxetine (Paxil®),fluvoxamine (Luvox®), citalopram(Celexa®) and escitalopram(Lexapro®).
SSRIs selectively inhibit serotoninreuptake by the presynaptic neurons,thus increasing serotonin levels in thesynaptic cleft. There are case reportsof SSRIs causing arrhythmias, atrialfibrillation and flutter, heart block,bradycardia, and supraventricular
TABLE 6. Antidepressants commonly used with comorbid cardiovascular disease
GENERIC NAME BRAND NAME STARTING DOSE(mg/day)
THERAPEUTIC DOSE(mg/day)
Sertraline Zoloft 25–50 50–200
Paroxetine Paxil 10–20 10–40
Fluoxetine Prozac 10–20 10–40
Fluvoxamine Luvox 25–50 50–200
Citalopram Celexa 10–20 20–40
Mirtazapine Remeron 7.5–15 15–45
Venlafaxine Effexor 37.5–75 75–375
Bupropion Wellbutrin 150–450 50–150
Duloxetine Cymbalta 15–30 30–60
Escitalopram Lexapro 10 10–30
Psychiatry 2009 [ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ]46
tachycardia.110–114 SSRIs, in general, arethought be cardio safe. Several smallstudies and some major studies likeSAD HART and CREATE provideddata regarding the safety of SSRIs inpatients with CAD.95,115–117
In the well-known SAD HARTstudy, Glassman et al95 evaluated thesafety and efficacy of sertralinetreatment of major depressive disorder(MDD) in patients who werehospitalized for acute MI or unstableangina. The investigators enrolled 369patients with MDD with either an MI orunstable angina in a randomized,double-blind, placebo-controlled trial.Patients were given a two-week,single-blind, placebo run and thenwere randomized to receive a flexibledose (50–200mg) of sertraline orplacebo for 24 weeks. No changeswere observed in various parameters,such as left ventricular ejectionfraction (LVEF), prolonged QTc, orother cardiac measures. This supportssertraline being safe in patients withdepression and comorbid CAD orunstable angina. However, sertralinewas not very effective for thetreatment of depression in this groupof patients. It was statistically superiorto placebo on Cognitive GlobalImpression (CGI) 1 scales over 24weeks, but not on HAM-D scores at 16weeks. However, when a predefinedgroup of patients with severe
depression was reviewed, sertralinewas shown to be more effective thanplacebo in both CGI-1 and HAM-Dscales (p=0.001). Treatment withsertraline was also found to beassociated with significantimprovement in quality of life andfunctioning in the severely depressedgroup.118 Sertraline has been shown toimprove HRV, an expression of cardiacautonomic function in post-MI patientswho are depressed.119 In a secondaryanalysis of 1,834 patients from theENRICHD study, the risk of death orrecurrent MI was significantly lower inpatients taking SSRIs.120 In anotherstudy,116 fluoxetine was found to beeffective in treating mild depression inpatients with MI.
In another landmark trial,Lesperance et al117 evaluated thetreatment of depression in CADpatients. Authors simultaneouslyevaluated the short-term efficacy of anantidepressant medication andinterpersonal psychotherapy forreducing depressive symptoms. It wasa randomized, controlled trial in which284 patients with CAD and depressionwere studied. All patients met theDiagnostic and Statistical Manual ofMental Disorders, Fourth Edition(DSM-IV) criteria for the diagnosis ofmajor depression of four-weeksduration or longer and had scores of 20or higher on HAM-D scale.
Citalopram was superior to placeboin reducing HAM-D scores over thecourse of 12 weeks (mean difference,3.3 points; 96.7 percent CI, 0.80–5.85;P=0.005). The reduction in BDI IIscores also favored citalopram.Authors did not find any benefit ofinterpersonal psychotherapy overclinical management. This trialdocumented the efficacy of citalopramgiven in conjunction with weeklyclinical management of majordepression among patients with CAD.
SSRIs have various drug-druginteractions based on severalpharmacokinetic actions.121 Forexample some SSRIs, such asfluoxetine and paroxetine, inhibitcytochrome (CYP) P450-2D6isoenzyme and can lead to increasedlevels of beta blockers, such asmetoprolol, and 1C antiarrythmicdrugs, such as encainide, propafenone,and flecainide.121 SSRIs also have a highprotein-binding affinity, which shouldbe considered in patients given digoxinand warfarin. The only SSRI todemonstrate an interaction withdigoxin is paroxetine, whichsignificantly increases the area underthe concentration curve for digoxin by18 percent.122 In addition,coadministration of fluoxetine withwarfarin has been shown to affect theprothrombin time.123 Based on thesestudies, sertraline or citalopram plusclinical management should beconsidered as first line of treatment forpatients with depression and CAD. Inaddition, escitalopram and citalopramdo not have any clinically significantactivity at the cytochrome P 450system.121
Medications considered safe forpatients with CAD.Triazolopyridines, another subclass oftricyclic antidepressants, includetrazodone. Trazodone is rarely used asan antidepressant. It can, however, beused in low doses for insomnia. Its useis limited because of orthostatichypotension; furthermore, if it is usedto treat depression, it must be used ata higher dosage, which can be verysedating.
Venlafaxine is a dual-actionmedication that is well tolerated andhas few anticholinergic effects.124 It
TABLE 7. Summary of recommendations
1 Screen all patients with CAD for depressive symptoms.
2 Use PHQ-9 for screening for depression as it is easy to use and helps withfollow up on progress
3
Medication use: Start with an SSRI medication and increase the dose totherapeutic-maximum dose. If patient does not tolerate the medication ordoes not show clinical improvement in 2–4 weeks of being on thetherapeutic dose of an antidepressant, switch to another antidepressantfrom the same class or preferably another antidepressant from another classwith a different mechanism of action. If the patient still does not show anyimprovement in another 2–4 weeks, consider adding another antidepressantwith a different mechanism of action to the SSRI.
4
Patients who are smokers and want to quit smoking should be carefullywatched for any symptoms of depression. If patient is a smoker, bupropionmay be a good choice for its antidepressant and smoking cessationproperties.
Key: CAD=coronary artery disease; PHQ-9=Patient Health Questionnaire-9; SSRI=selectiveserotonin reuptake inhibitor

[ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ] Psychiatry 2009 47474747
does not have any significant effectson cardiac conduction, but canincrease blood pressure at higherdosages. It can be used safely if theblood pressure is monitored closely. Ithas minimal CYP P450 interactions.121
Mirtazapine, a presynaptic alpha-2antagonist, is a dual-action medication.It increases both nonadrenergic andserotonergic transmission.125
Mirtazapine does not have significantcardiovascular effects, except posturalhypotension at higher dosages, andcan be used safely in patients withCAD. It can, however, cause sedationand weight gain, which can be a long-term risk for CAD.
Bupropion is classified as amonocyclic drug, which is a weakinhibitor of noradrenaline anddopamine reuptake inhibitor.126
Bupropion is considered safe inpatients with CAD, especially if theirblood pressure and heart rate aremonitored.
Duloxetine, one of the newerantidepressants, is an inhibitor ofserotonin and norepinephrinereuptake. It has no significant affinityfor cholinergic, adrenergic, orhistaminergic receptors.127 Duloxetineis both a substrate and moderatelypotent inhibitor of CYP 450-2D6 andwarrants caution with beta blockersand 1-C antiarrythmic drugs, which aremetabolized by this isoenzyme.128 Notmuch is known about thecardiovascular safety of duloxetine atthis time. It is associated withincreased blood pressure.129 Therefore,blood pressure monitoring is advisedbefore and during treatment withduloxetine in patients with CAD.
In the MIND-IT study, which was amulticenter study of 2,177 patientswith MI, antidepressant treatment withmirtazapine did not show improvementin long-term depression post-MI statusor cardiac prognosis.130
Medications that can be usedwith extreme caution in patientswith CAD. Tricyclic antidepressantshave cardiovascular toxicity, whichseverely limits their use in patientswith heart disease. These drugs alsohave anticholinergic, antiadrenergic,and antihistamine effects. They cancause sinus tachycardia,
supraventricular tachyarrhythmias,ventricular tachycardia, andfibrillation, prolongation of PR, QRS,and QT intervals, first, second, andthird degree heart block, and ST andT wave segment changes.131 Thesedrugs can be fatal in cases ofoverdose. Patients receiving cardiacmedications, such as calcium channelblocker, alpha-adrenergic antagonist,diuretics, and beta-blockers, may be atrisk of side effects.
Recently, a transdermalformulation of selegiline was approvedfor the treatment of MDD. Low dose(5–10mg/day) of oral selegiline doesnot need dietary restrictions, but isnot an effective antidepressant.Compared with oral selegiline,selegiline transdermal system (STS)leads to steady plasma levels of thedrug, increasing the amounts of thedrug to the brain and decreasingmetabolite production. STSspecifically inhibits central nervoussystem monoamine oxidase (MAO) Aand B enzymes, with minimal effectson MAO A in the gastrointestinalsystem and hepatic system, thusreducing the risk of interaction withfoods rich in tyramine.133 Not muchdata are available regarding thecardiovascular properties of thismedication.
Medications to be avoided inpatients with CAD. The MAOinhibitors, the oldest class ofantidepressants, are used byphysicians to treat depression andanxiety disorders. The use of thesedrugs has declined because of theirpotential interaction with foods rich intyramine and other medications suchas cold remedies and otherantidepressants. This adverseinteraction can lead to fatal adrenergiccrisis or it may cause posturalhypotension.132 This side effect can beworsened in cardiac patients takingdiuretics or other antihypertensives.Beta adrenergic blockers are alsogenerally contraindicated in patientsreceiving MAO inhibitors becausetheir predominant clinical effect inthese patients may be to intensifyvasoconstriction, leading to worseninghypertension. MAO inhibitors arerarely used in CVD patients.
BEHAVIORAL INTERVENTIONSEven though behavioral
interventions are useful in treatment ofdepression, the data are not verysupportive of the use of behavioraltherapies for treating depression inCAD patients.
Behavioral treatments fordepression. There have been someclinical trials of psychosocial andbehavioral interventions in patientswith CHD that offer encouragement. Inone open-label trial of 17 patients,Koszycki et al134 found that medicatedand unmedicated cardiovascularpatients suffering from depressionrespond similarly to interpersonalpsychotherapy.
The ENRICHD study135 was arandomized, controlled trial of post-MIpatients, which was designed todetermine if treatment for depressionand/or low perceived social supportwould reduce mortality and/orrecurrent MI. Patients wererandomized to either cognitivebehavioral therapy (CBT) or usualcare. Patients in the CBT group weresupplemented with sertraline if theirdepression did not improve by fiveweeks (scores higher than 24 on theHAM-D or less than a 50-percentreduction on the BDI).
The intervention did not increaseevent-free survival.136 The interventionimproved depression, although therelative improvement in thepsychosocial group compared with theusual care group was less thanexpected. The intervention did notseem to affect late mortality (29months).
The selection criteria for thepatients in this study may havecontributed to the weaker findings,since those patients who were selectedfor the study had mild and transientdepression. Also, patients wereexcluded if they had any other life-threatening illnesses, cognitiveimpairment, other major psychiatricillness, were too ill, were takingantidepressants, or undergonepercutaneous coronary intervention orCABG surgery. The authors alsosuggested that psychopharmacologicaltreatments might have helped patientsin all the groups, thus decreasing the

Psychiatry 2009 [ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ]4848
difference in improvement betweenthe groups.136 One important finding inthe study was that treatment-refractory patients were at a higherrisk for late mortality than thosepatients who responded to treatment.Also the CREATE study reviewed inanother section did not findinterpersonal psychotherapy to bemore effective than care as usual.
Behavioral treatments toreduce cardiovascular risks.Blumenthal et al137 prospectivelyexamined the relationship of exerciseafter MI to mortality and nonfatalreinfarction. They followed 2,078individuals who were surveyed abouttheir exercise habits six months afterthe initial MI and followed them forfour years. After two years, thepatients reporting exercise had lessthan half the events compared topatients who did not report regularexercise. They concluded that exerciseis of potential value in reducingmortality and nonfatal reinfarction inacute MI patients at high risk foradverse effects because of beingdepressed or having low socialsupport.
In a study by del Pino et al,138 theinvestigators found that group CBTwas superior to standard medicaltreatment and health educationtreatment in male patients with lowsocial and educational levels to reducecertain aspects of physiologicalactivation. It was also found useful forreducing depression at the two-yearfollow up.
Patients in a lifestyle changeprogram, which incorporated a low-fatvegetarian diet, stress managementtraining including yoga, meditation,and group therapy, and moderateexercise with weekly support groupmeetings, showed regression of theiratherosclerotic lesions compared to acontrol group receiving usual care.Using angiography to monitorprogression, these improvements weremaintained at a four-year follow up.139
CONCLUSIONThere is convincing evidence about
the relationship between depressionand CAD. However, it is not clear iftreating depression can influence CAD
prognosis and morbidity. Lack of astandardized measurement ofdepression, repeat publications fromthe same data set, and lack ofstandardization of outcome definitionsand covariates tend to complicate theclarity of the association betweendepression and CAD. The NationalHeart and Lung Institute has organizeda working group to recommenddepression measurements for studiesof depression in CVD.
Depression is common in patientswith CAD. The data are consistent insupporting that depression is a riskfactor for both the development andworsening of CAD. A number ofpathophysiological mechanisms mayexplain this association. Because of theincreasing evidence of theseassociations between depression andCAD, it is strongly recommended thatphysicians screen patients with CHDfor depressive symptoms.
Several scales and tools can beused, such as PRIME-MD® PHQ-9,HADS, HAM-D, and CDS. Werecommend using PHQ-9, as it issimple and easily administered.
Because of lack of studiessupporting psychotherapy fortreatment of depression in patientswith CAD, use of antidepressants is thefirst line of treatment. The older drugs,such as MAO inhibitors and tricyclicantidepressants, have potential risksfor patients with CAD. The newerclasses of antidepressants are found tobe safe and effective for treatment ofdepressive symptoms in these patients.These classes of medications includeSSRIs, like sertraline, and other oneslike venlafaxine, mirtazapine, andbupropion. Because there is more datasupporting the use of SSRIs, thesedrugs should be considered as first-linetreatment for depression in CADpatients. Some of the studies inprogress may shed more light on theissue of whether treating depression inCAD patients can improve outcomes ofthe disease.
REFERENCES1. Murray CJL, Lopez AD. The Global
Burden of Disease: A ComprehensiveAssessment of Mortality and Disabilityfrom Diseases, Injuries and RiskFactors in 1990 and Projected to 2020.
Cambridge, MA: Harvard University Presson behalf of the World HealthOrganization and the World Bank, 1996.
2. Kannel WB, Wolf PA, Veter J, et al.Epidemiologic assessment of the role ofblood pressure in stroke: the Framinghamstudy. JAMA. 1970;21(4):301–310.
3. Veterans Administration and Co-operativeStudy Group on Antihypertensive Agents.Effects of treatment on morbidity inhypertension: results in patients withdiastolic blood pressures averaging 115through 129mmHg. JAMA.1967;202:116–122.
4. Hypertension Detection and Follow-upProgram Cooperative Group. Persistenceof reduction in blood pressure andmortality of participants in theHypertension Detection and Follow upProgram. JAMA. 1988;259:2113–2122.
5. Multiple Risk Factor Intervention TrialResearch Group. Multiple riskintervention trial--risk factor changes andmortality results. JAMA.1982;248:1465–1467.
6. Almdal T, Scharling H, Jensen JS, et al.The independent effect of type 2 diabetesmellitus on ischemic heart disease,stroke, and death: a population-basedstudy of 13,000 men and women with 20years of follow-up. Arch Intern Med.2004;164:1422–1426.
7. Kuller LH, Arnold AM, Psaty BM, et al.10-year follow-up of subclinicalcardiovascular disease and risk ofcoronary heart disease in theCardiovascular Health Study. Arch InternMed. 2006;166:71–78.
8. Hopkins PN, Williams RR. A survey of 246suggested coronary risk factors.Atherosclerosis. 1981;40:1–52.
9. Forrester AW, Lipsey JR, Teitlbaum ML,et al. Depression following myocardialinfarction. Int J Psychiatry Med.1992;22:33–46.
10. Schleifer SJ, Macari-Hinson MM, CoyleDA, et al. The nature and course ofdepression following myocardialinfarction. Arch Intern Med.1989;149:1785–1789.
11. Lloyd GG, Cawley RH. Distress or illness?A study of psychosocial symptoms aftermyocardial infarction. Br J Psychiatry.1983;142:120–125.
12. Kurosawa H, Shimizu Y, Nishimatsu Y, etal. The relationship between mentaldisorders and physical severities inpatients with myocardial infarction. JpnCirc Res. 1983;47:723–728.
13. Cay EL, Vetter N, Philip AE, et al.Psychological status during recovery froman acute heart attack. J Psychosom Res.1972;16:425–435.
14. Havik OE, Maeland JG. Patterns ofemotional reactions after a myocardialinfarction. J Psychosom Res.1990;34:271–285.
15. Freedland KE, Carney RM, Lustman PJ,et al. Major depression in coronary arterydisease patients with vs. without a priorhistory of depression. Psychosom Med.1992;4:416–421.
16. Carney RM, Rich MW, Tevelde MA, et al.
[ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ] Psychiatry 2009 49
Major depressive disorder in coronaryartery disease. Am J Cardiol.1987;60:1273–1275.
17. Hance M, Carney RM, Freedland KE, etal. Depression in patients with coronaryartery disease: a 12-month follow up. GenHosp Psychiatry. 1996;18:61–65.
18. McKhann GM, Borowicz LM,Goldsborough MA, et al. Depression andcognitive decline after coronary arterybypass grafting. Lancet.1997;349:1282–1284.
19. Spijkerman TA, van den Brink RH,Jansen JH, et al. Who is at risk of post-MIdepressive symptoms? J Psychosom Res.2005;58:425–432.
20. Kessler RC, Berglund P, Demler O, et al.The epidemiology of major depressivedisorder: results from the NationalComorbidity Survey Replication (NCS-R).JAMA. 2003;289(23):3095–3105.
21. Irvine J, Basinski A, Baker B, et al.Depression and risk of sudden cardiacdeath after acute myocardial infarction:testing for the confounding effects offatigue. Psychosom Med.1999;61:729–737.
22. Pratt LA, Ford DE, Crum RM, et al.Depression, psychotropic medication, andrisk of myocardial infarction: prospectivedata from the Baltimore ECA follow-up.Circulation. 1996;94:3123–3129.
23. Ford DE, Mead LA, Chang PP, et al.Depression is a risk factor for coronaryartery disease in men: the precursorsstudy. Arch Intern Med.1998;158:1422–1426.
24. Sesso HD, Kawachi I, Vokonas PS, et al.Depression and the risk of coronary heartdisease in the normative aging study. AmJ Cardiol. 1998;82:851–856.
25. Pennix BW, Guralnik JM, Mendes deLeon CF, et al. Cardiovascular events andmortality in newly and chronicallydepressed persons >70 years of age. AmJ Cardiol. 1998;81:988–994.
26. Whooley MA, Browner WS. Associationbetween depressive symptoms andmortality in older women. Study ofOsteoporotic Fractures Research Group.Arch Intern Med. 1998;158:2129–2135.
27. Mendes de Leon CF, Krumholz HM,Seeman TS, et al. Depression and risk ofcoronary heart disease in elderly men andwomen: New Haven EstablishedPopulation for the Epedemilogic Studiesof the Elderly (EPESE). 1982–1991.Arch Intern Med. 1998;158:2341–2348.
28. Fu CC, Lee YM, Chen JD. Associationbetween depression and 12-yearmortality among elderly in a ruralcommunity in Taiwan. J Formos MedAssoc. 2003;102:234–239.
29. Cheok F, Schrader G, Banham D, etal.Identification, course, and treatment ofdepression after admission for a cardiaccondition: rationale and patientcharacteristics for the IdentifyingDepression As a Comorbid Condition(IDACC) project. Am Heart J.2003;146:978–984.
30. Sullivan MD, LaCroix AZ, Baum C, et al.Functional status in coronary artery
disease: a one year prospective study ofthe role of anxiety and depression. Am JMed. 1997;103:348–356.
31. Simonsick EM, Wallace RB, Blazer DG, etal. Depressive symptomatology andhypertension associated morbidity andmortality in older adults. PsychosomMed. 1995;57:427–435.
32. Barefoot JC, Schroll M. Symptoms ofdepression, acute myocardial infarction,and total mortality in a communitysample. Circulation. 1996;93:1976–1980.
33. Lesperance F, Frasure-Smith N, Talajic M.Major depression before and aftermyocardial infarction: its nature andconsequences. Psychosom Med.1996;58:99–110.
34. Appels A. Mental precursors ofmyocardial infarction. Br J Psychiatry.1990;156:465–471.
35. Wassertheil-Smoller S, Applegate WB,Berge K, et al. Change in depression as aprecursor of cardiovascular events. ArchInt Med. 1996;156:553–561.
36. Dickens C, McGowan L, Percival C, et al.Association between depressive episodebefore first myocardial infarction andworse cardiac failure following infarction.Psychosomatics. 2005;46:523–528.
37. Lauzon C, Beck CA, Huynh T et al.Depression and prognosis followinghospital admission because of acutemyocardial infarction. CMAJ.2003;108:547–552.
38. Rumsfeld JS, Jones PG, Whooley M, et al.Depression predicts mortality andhospitalization in patients withmyocardial infarction complicated byheart failure. Am Heart J.2005;150:961–967.
39. Empana JP, Jouven X, Lemaitre RN, et al.Clinical depression and risk of out-of-hospital cardiac arrest. Arch Intern Med.2006;166:195–200.
40. Aromaa A, Raitasalo R, Reunanen A et al.Depression and cardiovascular diseases.Acta Psychiatr Scand.1994;377(suppl):77–82.
41. Luukinen H, Laippala P, Huikuri HV.Depressive symptoms and the risk ofsudden cardiac death among the elderly.Eur Heart J. 2003;24:2021–2026.
42. Everson SA, Kaplan GA, Goldberg D E.Depressive symptoms and risk ofmyocardial infarction and mortality(abstract). Am J Epidemiol.1995;141:[S37].
43. Anda R, Williamson D, Jones D, et al.Depressed affect, hopelessness, and therisk of ischemic heart disease in a cohortof U.S. adults. Epidemiology.1993;4:285–289.
44. Ahern DK, Gorkin L, Anderson JL, et al.Biobehavioral variables and mortality orcardiac arrest in the cardiac arrythmiapilot study. Am J Cardiol.1990;59:58–62.
45. Levine JB, Covino NA, Slack WV, et al.Psychological predictors of subsequentmedical care among patients hospitalizedwith cardiac disease. J CardiopulmRehab. 1996;16:109–116.
46. Barefoot JC, Helms MJ, Mark DB, et al.
Depression and long term mortality riskin patients with coronary artery disease.Am J Cardiol. 1996;78:613–617.
47. Carney RM, Rich MW, Freedland KE, etal. Major depressive disorder predictscardiac events in patients with coronaryartery disease. Psychosom Med.1988;50:627–633.
48. Kennedy GJ, Hofer MA, Cohen D, et al.Significance of depression and cognitiveimpairment in patients undergoingprogrammed stimulation of cardiacarrhythmias. Psychosom Med.1987;49:410–412.
49. Frasure-Smith N, Lesperance F, Talajic M.Depression following myocardialinfarction: impact on 6-month survival.JAMA. 1993;270:1819–1825.
50. Frasure-Smith N, Lesperance F, Talajic M.Depression and 18-month prognosis aftermyocardial infarction. Circulation.1995;91:999–1005.
51. Wassertheil-Smoller S, Shumaker S,Ockene J, et al. Depression andcardiovascular sequelae inpostmenopausal women. The Women’sHealth Initiative. Arch Intern Med.2004;164:289–298.
52. Silverstone PH. Depression and outcomein acute myocardial infarction. Br Med J.1987;24:219–220.
53. Ladwig KH, Kieser M, Konig J, et al.Affective disorders and survival afteracute myocardial infarction: results fromthe post infarction late potential study.Eur Heart J. 1991;12:959–964.
54. Ladwig KH, Roll G, Breithardt G, et al.Post infarction depression andincomplete recovery 6 months after acutemyocardial infarction. Lancet.1994;343:20–23.
55. de Jonge P, Spijkerman TA, van denBrink RH, et al. Depression aftermyocardial infarction is a risk factor fordeclining health related quality of life andincreased disability and cardiaccomplaints at 12 months. Heart.2006;92:8–10.
56. Rumsfeld JS, Majid DJ, Plomondon ME,et al. History of depression, angina andquality of life after acute coronarysyndromes. Am Heart J.2003;145:493–499.
57. Dickens CM, Mc Gowan L, Percival C, etal. Lack of close confidant, but notdepression, predicts further cardiacevents after myocardial infarction. Heart.2004;90:518–522.
58. Carney RM, Blumenthal JA, Catellier D,et al. Depression as a risk factor formortality after acute myocardialinfarction. Am J Cardiol.2003;92:1277–1281.
59. de Jonge P, Ormal J, van den Brink RH etal. Symptom dimensions of depressionfollowing myocardial infarction and theirrelationship with somatic health statusand cardiovascular prognosis. Am JPsychiatry. 2006;163:138–144.
60. Denollet J, Brutsaert DL. Personality andmortality after myocardial infarction.Psychosom Med. 1995;57:582–591.
61. Levine JB, Covino NA, Slack WV, et al.
Psychiatry 2009 [ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ]50
Psychological predictors of subsequentmedical care among patients hospitalizedwith cardiac disease. J CardiopulmonRehab. 1996;16:109–116.
62. Stewart RA, North FM, West TM, et al.Depression and cardiovascular morbidityand mortality: cause or consequence?Eur Heart J. 2003;24:2027–2037.
63. Blumenthal JA, Lett HS, Babyak MA, etal. Depression as a risk factor formortality after coronary artery bypasssurgery. Lancet. 2003;362:604–609.
64. Parashar S, Rumsfeld JS, Spertus JA, etal. Time course of depression andoutcomes of myocardial infarction. ArchIntern Med. 2006;166:2035–2043.
65. Rumsfeld JS, Havranek E, Masoudi FA, etal. Cardiovascular Outcomes ResearchConsortium. Depressive symptoms arethe strongest predictors of short-termdeclines in health status in patients withheart failure. J Am Coll Cardiol.2003;42:1811–1817.
66. Gehi A, Haas D, Pipkin S, et al.Depression and medicationnonadherance in outpatients withcoronary heart disease: findings from theHeart and Soul Study. Arch Intern Med.2005;165:2508–2513.
67. DiMatteo MR, Lepper HS, Croghan TW.Depression is a risk factor for noncompliance with medical treatment: metaanalysis of the effects of anxiety anddepression on patient adherence. AnnInt Med. 2000;160:2101–2107.
68. Bonnet F, Irving K, Terra JL, et al.Anxiety and depression are associatedwith unhealthy life style in patients at riskof cardiovascular disease.Atherosclerosis. 2005;178:339–344.
69. Glassman AH, Helzer JE, Covey LS, et al.Smoking, smoking cessation, and majordepression. JAMA. 1990;264:1546–1549.
70. Carney RM, Freedland KE, Eisen SA, etal. Major depression and medicationadherence in elderly patients withcoronary artery disease. Health Psychol.1995;14:88–90.
71. Covey LS, Glassman AH, Stetner F. Majordepression following smoking cessation.Am J Psychiatry. 1997;152:263–265.
72. Greenberg I, Perna F, Kaplan M, et al.Behavioral and psychological factors inthe assessment and treatment of obesesurgery patients. Obese Res.2005;13:244–249.
73. Vieth RC, Lewis N, Linares OA, et al.Sympathetic nervous system activity inmajor depression: Basal and desipramine-induced alterations in plasmanorepinephrine kinetics. Arch GenPsych. 1994:51:411–422.
74. Fleming R, Baum A, Gisriel MM, et al.Mediating influences of social support onstress at Three Mile Island. J HumStress. 1982;8:4–22.
75. Suarez EC. Hostility-related differences inurinary excretion rates ofcatecholamines. Presentation. Chicago,IL: Annual Meeting, Society forPsychophysiological Research, 1992.
76. Lechin F, van der Dijs B, Orzco B: Plasmaneurotransmitters, blood pressure, and
heart rate during supine-resting,orthostasis, and moderate exerciseconditions in major depressed patients.Biol Psychiatry. 1995;38:166–173.
77. Sachar EJ, Hellman L, Fukushima DK, etal. Cortisol production in depressiveillness: a clinical and biochemicalclarification. Arch Gen Psychiatry.1970;23:289–298.
78. Pfhol B, Rederer M, Coryell W, et al.Association between post-dexamethasonecortisol level and blood pressuremanagement in depressed inpatients. JNerv Ment Dis. 1991;17:44–47.
79. Raadsheer FC, Hoogendijk WJ, Stam FC,et al. Increased numbers of corticotropin-releasing hormone expressing neurons inthe hypothalamic paraventricular nucleusof depressed patients. Neuroendocrinol.1994;60:436–444.
80. Radsheer FC, van Heerikhuize JJ,Lucassen PJ, et al. Corticotropin-releasing hormone mRNA levels in theparaventricular nucleus of patients withAlzheimer’s disease and depression. Am JPsychiatry. 1995;152:1372–1376.
81. Bigger JT, Kleiger RE, Fleiss JL.Components of heart rate variabilitymeasured during healing of acutemyocardial infarction. Am J Cardiol.1988;61:208–215.
82. Dalack GW, Roose SP. Perspectives in therelationship between cardiovasculardisease and affective disorder. J ClinPsychiatry. 1990;51(suppl):4–9.
83. Miyawaki E, Salzman C. Autonomicnervous system tests in psychiatry:Implications and potential uses of heartrate variability. Integrated Psychiatry.1991;7:21–28.
84. Carney RM, Saunders RD, Freedland KE,et al. Association of depression withreduced heart rate variability in coronaryartery disease. Am J Cardiol.1995;76:562–564.
85. Carney RM, Blumenthal JA, FreedlandKE, et al. Low heart rate variability andthe effect of depression on post-myocardial infarction mortality. ArchIntern Med. 2005;65:148–1491.
86. Carney RM, Freedland KE, Veithh RC.Depression, the autonomic nervoussystem, and coronary heart disease.Psychosom Med. 2005;67(suppl1):S29–S33.
87. Setty AB, Vaughn BV, Quint SR, et al.Heart period variability during vagalnerve stimulation. Seizure.1998;7:213–217.
88. Bruce EC, Musselman DL. Depression:alterations in platelet function andischemic heart disease. Psychosom Med.2005;67(suppl):S34–S36.
89. Berk M, Plein H. Platelet supersensitivityto thrombin stimulation in depression: apossible mechanism for the associationwith cardiovascular mortality. ClinNeuropharmacol. 2000;23:182–185.
90. Kop WJ, Gottdiener JS. The role ofimmune system parameters in therelationship between depression andcoronary artery disease. PsychosomMed. 2005;67:S37–S41.
91. Sherwood A, Hinderliter AL, Watkins LL,et al. Impaired endothelial function incoronary heart disease patients withdepressive symptomatology. J Am CollCardiol. 2005;46:656–659.
92. Siscovick DS, Raghunathan TE, King I , etal. Dietary intake and cell membranelevels of long-chain n-3 polyunsaturatedfatty acids and the risk of primary cardiacarrest. JAMA. 1995;274:1363–1367.
93. Steptoe A, Kunz-Ebrecht SR, Owen N, etal. Lack of association betweendepressive symptoms and markers ofimmune and vascular inflammation inmiddle aged men and women. PsychologMed. 2003;33:667–674.
94. Pignone MP, Gaynes BN, Rushton J L, etal. Screening for depression in adults: asummary of the evidence for the U.S.Preventive Services Task Force. AnnIntern Med. 2002;136:765–776.
95. Glassman AH, O’Connor CM, Califf RM, etal. Sertraline treatment of majordepression in patients with acute MI orunstable angina. JAMA.2002;288:701–709.
96. Strik JJ, Honig A, Lousberg R, et al.Sensitivity and specifity of observer andself-report questionnaires in major andminor depression following myocardialinfarction. Psychosomatics.2001;42:423–428.
97. Honig A, Huyper AM, Schene AH, et al.Treatment of post-myocardial depressivedisorder: a randomized, placebo-controlled trial with mirtazapine.Psychosom Med. 2007;69:606–13.
98. Bambauer KZ, Locke SE, Aupont O,et al.Using the Hospital Anxiety andDepression Scale to screen for depressionin cardiac patients. Gen HospPsychiatry. 2005;27:275–284.
99. Di Benedetto M, Lindner H, Hare DL, etal. Depression following acute coronarysyndromes: a comparison between theCardiac Depression Scale and the BeckDepression Inventory II. J PsychosomRes. 2006;60:13–20.
100. Di Benedetto M, Lindner H, Hare DL, etal. A Cardiac Depression Visual AnalogueScale for the brief and rapid assessmentof depression following acute coronarysyndromes.
101. Acadamic highlights: treatment ofdepression in primary care. J ClinPsychiatry. 2006;67:487. J PsychosomRes. 2005;59:223–229.
102. Poston WS, Haddock CK, Conard MW, etal. Assessing depression in the cardiacpatient. When is the appropriate time toassess depression in the patientundergoing coronary revascularization?Behav Modification. 2003;27:26–36.
103. Denollet J, Brutsaert DL. Reducingemotional distress improves prognosis incoronary heart disease: 9-year mortalityin a clinical trial of rehabilitation.Circulation. 2001;104:2018–2023.
104. Schrader G, Cheok F, Hordacre AL, etal.Effect of psychiatry liaison with generalpractitioners on depression severity inrecently hospitalised cardiac patients: arandomised controlled trial. Med J Aust.
[ V O L U M E 6 , N U M B E R 1 , J A N U A R Y ] Psychiatry 2009 51
2005;182:272–276.105. Tridevi MH, Fava M, Wisniewski SR, et al.
Evaluation of outcomes with citalopramfor depression using measurement-basedcare in STAR*D: Implications for clinicalpractice. Am J Psychiatry.2006;163:28–40.
106. Rush AJ, Tridevi MH, Wisniewski SR, etal. Bupropion-SR, sertraline, orvenlafaxine XR after failure of SSRIs fordepression. N Engl J Med.2006;354:1231–1242.
107. Tridevi MH, Fava M, Wisniewski SR, et al.Medication augmentation after failure ofSSRIs for depression. N Engl J Med.2006;354:1243–1252.
108. Feinstein RE, Blumenfield M, OrlowskiB,et al. A national survey ofcardiovascular physician’s beliefs andclinical care practices when diagnosingand treating depression in patients withcardiovascular disease. Cardiol Rev.2006;14:164–169.
109. Carney RM, Freedland KE, Sheline YI, etal. Depression and coronary heartdisease: a review for cardiologists. ClinCardiol. 1997;20:196–200.
110. Buff DD, Brenner R, Kirtane SS, et al.Dysrhythmia associated with fluoxetinetreatment with cardiac disease. J ClinPsychiatry. 1991;52:174–176.
111. Ahmed I, Dagincourt PG, Miller LG, et al.Possible interaction between fluoxetineand pimozide causing sinus bradycardia.Can J Psychiatry. 1993;38:62–63.
112. Roberge RJ, Martin TJ. Mixedfluoxetine/loxapine overdose and atrialflutter. Ann Emerg Med.1994;23:586–590.
113. Amital D, Amital H, Gross R, et al. Sinusbradycardia due to fluvoxamine overdose.Br J Psych. 1994;165:553–554.
114. Hillis LD, Lange RA. Serotonin and acuteischemic heart disease. N Eng J Med.1991;324:688–690.
115. Roose SP, Glassman AH, Attia E, et al.Cardiovascular effects of fluoxetine indepressed patients with heart disease.Am J Psychiatry. 1998;155:660–665.
116. Strik JJ, Honig A, Lousberg R et al.Efficacy and safety of fluoxetine in thetreatment of patients with majordepression after first myocardialinfarction: findings from a double-blind,placebo-controlled trial. Psychosom Med.2000;62:783–789.
118. Swenson JR, O’Connor CM, Barton D, etal. Influence of depression and effect oftreatment with sertraline on quality of lifeafter hospitalization for acute coronarysyndrome. Am J Cardiol.2003;92:1271–1276.
119. McFarlane A, Kamath MV, Fallen EL, etal. Effect of sertraline on the recoveryrate of cardiac autonomic function indepressed patients after acute myocardialinfarction. Am Heart J.2001;142:617–623.
117. Lesperance F, Frasure-Smith N, KoszyckiD, et al. Effects of citalopram andinterpersonal therapy on depression inpatients with coronary artery disease: theCanadian Cardiac Randomized Evaluationof Antidepressant and PsychotherapyEfficacy (CREATE) trial. JAMA.2007;297:367–379.
120. Taylor CB, Youngblood ME, Catellier D, etal. Effects of antidepressant medicationon morbidity and mortality in depressedpatients after myocardial infarction. ArchGen Psychiatry. 2005;62:792–798.
121. Spina E, Santoro V, D’Arrigo C. Clinicallyrelevant pharmacokinetic druginteractions with second-generationantidepressants: an update. Clin Ther.2008;30(7):1206–1227.
122. Bannister SJ, Houser VP, Hulse JD.Evaluation of the potential forinteractions of paroxetine with diazepam,cimetidine, warfarin, and digoxin. ActaPsychiatr Scan.1989;350(suppl):102–106.
123. Claire RJ, Servis ME, Cram DL. Potentialinteractions between warfarin sodiumand fluoxetine. Am J Psychiatry.1991;148:1604.
124. Holliday SM, Benfield P. Venlafaxine. Areview of its pharmacology andtherapeutic potential in depression.Drugs. 1995;49:280–294.
125. Westenberg HG. Pharmacology ofantidepressants: selectivity ormultiplicity? J Clin Psychiatry.1999;60(suppl)17:46–48.
126. Gobbi G, Slater S, Boucher N, et al.Neurochemical and psychotropic effectsof bupropion in healthy male subjects. JClin Psychopharmacol.2003;23(3):233–239.
127. Schatzberg AF. Efficacy and tolerability ofduloxetine, a novel dual reuptakeinhibitor in the treatment of major
depressive disorder. J Clin Psychiatry.2003;64(suppl):30–37.
128. Skiner MH, Kuan HY, Pan A, et al.Duloxetine is both an inhibitor and asubstrate of cytochrome P4502D6 inhealthy volenteers. Clin PharmacolTher. 2003;73:170–177.
129. Cymbalta Package Insert. Indianopolis,IN: Elli Lilly and Company, 2004.
130. van Melle JP, de Jonge P, Honig A, et al.Effects of antidepressant treatmentfollowing myocardial infarction. Br JPsychiatry. 2007;190: 460–466.
131. Stoudemire A, Atkinson P. Use of cyclicantidepressants in patients with cardiacconduction disturbances. Gen HospPsychiatry. 1988;10:389–397.
132. Halper JP, Mann J. Cardiovascular effectsof antidepressant medication. Br JPsych. 1988;(suppl):87–98.
133. Patkar AA, Pae CU, Masand PS.Transdermal selegiline: the newgeneration of monoamine oxidaseinhibitors. CNS Spectr. 2006;11:363–375.
134. Koszycki D, Lafontaine S, Frasure-SmithN, et al. An open-label trial ofinterpersonal psychotherapy indepressed patients with coronary disease.Psychosomatics. 2004;45:319–324.
135. ENRICHD Investigators. EnhancingRecovery in Coronary Heart Disease(ENRICHD) study intervention: rationaleand design. Psychosom Med.2001;63:747–755.
136. Berkman LF, Blumenthal JA, Burg M, etal. Effects of treating depression and lowperceived social support on clinicalevents after myocardial infarction: theEnhancing Recovery in Coronary HeartDisease Patients (ENRICHD) randomizedtrial. JAMA. 2003;289:3106–3116.
137. Blumenthal JA, Babyak MA, Carney RM,et al. Exercise, depression, and mortalityafter myocardial infarction in theENRICHD trial. Med Sci Sports Exerc.2004;36:746–755.
138. del Pino A, Gaos MT, Dorta R, et al.Modification of coronary-prone behaviorsin coronary patients of low socio-economic status. Sp J Psychol.2005;8:68–78.
139. Ornish D, Brown SE, Schwartz LW, et al.Can lifestyle changes reverse coronaryheart disease? The lifestyle heart trial.Lancet. 1990;336:129.
Related Documents











