Depressed Mood and Maternal Report of Child Behavior Problems: Another Look at the Depression–Distortion Hypothesis Maria A. Gartstein a , David J. Bridgett b , Thomas J. Dishion c , and Noah K. Kaufman d a Department of Psychology, Washington State University, PO Box 644820, Pullman WA, [email protected], (509) 335-4651 (telephone), (509) 335-5043 (fax); b Department of Psychology, Washington State University, PO Box 644820, Pullman WA, [email protected] c Department of Psychology, 1227 University of Oregon, Eugene, OR, 97403-1227, [email protected] d Department of Psychology, 1227 University of Oregon, Eugene, OR, 97403-1227 Abstract Caregiver depression has been described as leading to overreport of child behavior problems. This study examines this “depression–distortion” hypothesis in terms of high-risk families of young adolescents. Questionnaire and diagnostic interview data were collected from mothers, teachers, and fathers, and self-report information was obtained from youth between ages 10 and 14 years. First, convergent and discriminant validity were demonstrated for internalizing and externalizing multiagent constructs. Second, the depression–distortion hypothesis was examined, revealing a modest effect of maternal depression, leading to the inflation of reported son externalizing and daughter internalizing problems. The data suggest the need to consider multiple influences on parental perceptions of child behavior and psychopathology in research and clinical settings. Keywords Depression; Behavior problems; Adolescence; Parent report; Gender differences 1. Introduction Child behavior problems and maternal depression have been linked in a multitude of investigations involving both clinical and community samples (Downey & Coyne, 1990; Goodman & Gotlib, 1999). Children of mothers who experienced clinical levels of depression were found to be at increased risk for psychopathology in general and for behavior problems in particular (Fendrich, Warner, & Weissman, 1990; Weissman et al., 1984; Welsh-Allis & Ye, 1988). This association between mothers’ depressive symptoms and child behavioral and emotional difficulties has been demonstrated for families of preschoolers participating in the treatment of child disruptive disorders (Webster-Stratton & Hammond, 1988) and community Corresponding Author Maria A. Gartstein, Department of Psychology, Washington State University, PO Box 644820, Pullman, WA, [email protected], (509) 335-4651 (telephone), (509) 335-5043 (fax). Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. NIH Public Access Author Manuscript J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1. Published in final edited form as: J Appl Dev Psychol. 2009 March ; 30(2): 149–160. doi:10.1016/j.appdev.2008.12.001. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Depressed Mood and Maternal Report of Child BehaviorProblems: Another Look at the Depression–Distortion Hypothesis
Maria A. Gartsteina, David J. Bridgettb, Thomas J. Dishionc, and Noah K. Kaufmanda Department of Psychology, Washington State University, PO Box 644820, Pullman WA,[email protected], (509) 335-4651 (telephone), (509) 335-5043 (fax);b Department of Psychology, Washington State University, PO Box 644820, Pullman WA,[email protected] Department of Psychology, 1227 University of Oregon, Eugene, OR, 97403-1227,[email protected] Department of Psychology, 1227 University of Oregon, Eugene, OR, 97403-1227
AbstractCaregiver depression has been described as leading to overreport of child behavior problems. Thisstudy examines this “depression–distortion” hypothesis in terms of high-risk families of youngadolescents. Questionnaire and diagnostic interview data were collected from mothers, teachers, andfathers, and self-report information was obtained from youth between ages 10 and 14 years. First,convergent and discriminant validity were demonstrated for internalizing and externalizingmultiagent constructs. Second, the depression–distortion hypothesis was examined, revealing amodest effect of maternal depression, leading to the inflation of reported son externalizing anddaughter internalizing problems. The data suggest the need to consider multiple influences onparental perceptions of child behavior and psychopathology in research and clinical settings.
KeywordsDepression; Behavior problems; Adolescence; Parent report; Gender differences
1. IntroductionChild behavior problems and maternal depression have been linked in a multitude ofinvestigations involving both clinical and community samples (Downey & Coyne, 1990;Goodman & Gotlib, 1999). Children of mothers who experienced clinical levels of depressionwere found to be at increased risk for psychopathology in general and for behavior problemsin particular (Fendrich, Warner, & Weissman, 1990; Weissman et al., 1984; Welsh-Allis &Ye, 1988). This association between mothers’ depressive symptoms and child behavioral andemotional difficulties has been demonstrated for families of preschoolers participating in thetreatment of child disruptive disorders (Webster-Stratton & Hammond, 1988) and community
Corresponding Author Maria A. Gartstein, Department of Psychology, Washington State University, PO Box 644820, Pullman, WA,[email protected], (509) 335-4651 (telephone), (509) 335-5043 (fax).Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customerswe are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resultingproof before it is published in its final citable form. Please note that during the production process errors may be discovered which couldaffect the content, and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptJ Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
Published in final edited form as:J Appl Dev Psychol. 2009 March ; 30(2): 149–160. doi:10.1016/j.appdev.2008.12.001.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
samples that included children of various ages (Egeland, Kalkoske, Gottesman, & Erickson,1990; Krain & Kendall, 2000). The strength of the association between maternal depressivesymptoms and child behavior problems is borne out by the consistency of findings acrossdevelopmental stages from preschool (Campbell, Pierce, Moore, Marakovitz, & Newby,1996) through adolescence (Thomas, Forehand, & Neighbors, 1995). In addition, studies usingdiverse measurement approaches, including diagnostic interviews, self-report questionnaires,and observations, have yielded convergent findings (Egeland et al., 1990; Fendrich et al.,1990; Hops et al., 1987).
It should be noted that maternal depressive symptoms have been shown to predict increasedrisk for child externalizing and internalizing type problems differently as a function of childgender (Essex, Klein, Cho, & Kraemer, 2003). On the other hand, divergent results have alsobeen obtained. Hammen (1991), for example, did not detect gender differences in the impactof maternal depression. Interestingly, Hops (1996) found that girls of depressed mothersexperienced more pronounced effects, particularly when older, whereas other investigatorsreported more extensive effects for younger boys. More recently, maternal depression wasfound to be associated with both externalizing and internalizing behavior problems for boys,but not linked with behavior problems/symptoms for female offspring (Carter, Garrity-Rokous,Chazan-Cohen, Little, & Briggs-Gowan, 2001). Given these inconsistent findings, we exploredthe existence of gender differences in associations between maternal symptoms of depressionand child behavior problems, but did not formulate specific a priori hypotheses about the exactnature of such differences.
A number of mechanisms have been proposed to explain the association between maternaldepression and child behavior problems (Campbell et al., 1996; Cummings & Davies, 1994;Goodman & Gotlib, 1999; Patterson, 1980). First, mothers’ symptoms of depression may leadto an actual increase in child behavior problems, either directly via symptoms of depression(e.g., dysphoria) that manifest while parents interact with their children, or through the effectsof depressive symptoms on parenting/parent–child interactions. A presentation characterizedby emotional unavailability, negative affect, and cognitions associated with depression likelydiminish the quality of parent–child interactions (Cummings & Davies, 1994; Goodman &Gotlib, 1999). In addition, maternal depression has been linked with the use of ineffectivebehavior management practices (e.g., harsh or inconsistent discipline and inadequatesupervision) and marital/family discord, which in turn may contribute to the development andmaintenance of child behavior problems (Forehand, Lautenschlager, Faust, & Graziano,1986).
The depression–distortion hypothesis (Richters & Pellegrini, 1989) has also been proposed asan explanatory mechanism for the association between maternal depression and child behaviorproblems. Specifically, dysphoric emotions associated with depression were hypothesized toactivate a negative perceptual bias in the mothers’ ratings of child behaviors that, in turn, leadsto overreporting of child adjustment difficulties (Field, 1992; Geller & Johnston, 1995; Griest,Wells, & Forehand, 1979; Johnston & Short, 1993). A number of studies have called intoquestion the accuracy of maternal report of child behaviors when mothers experiencesymptoms of depression (Breslau, Davis, & Prabucki, 1988; Friedlander, Weiss, & Traylor,1986). Schaughency and Lahey (1985), for example, warned about the risk of pathologizingchild behavior on the basis of maternal ratings if the level of maternal depression is not takeninto account. Friedlander et al. (1986) concluded that maternal depressive symptoms had asignificant impact on the report of child behavior, although they did not regard maternal ratingsas completely invalid.
However, evidence contrary to the depression–distortion hypothesis has also been presented.For instance, Pellegrini (1989) and Richters (1992) examined correlations between ratings of
Gartstein et al. Page 2
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
child behavior problems provided by mothers and by teachers and reported that the associationswere not affected by the level of maternal depressive symptomatology or mood disorderdiagnosis, and they noted that this pattern of findings was not consistent with the depression–distortion hypothesis. When Richters and Pellegrini (1989) evaluated state–trait dimensionsof maternal depression as mediators of the agreement between teachers and mothers, theirfindings failed to demonstrate any significant differences in agreement as a function of maternaldepression status. However, children of mothers who experienced a current depressive episodeor who reported a history of one or more depressive episodes were described by mothers andteachers as having exhibited more frequent behavior problems than had control children.
Investigations into discrepancies between different sources of information about childsymptoms of psychopathology and behavior problems, and the impact of parents’ ownsymptoms on discrepancies between their ratings and those of other informants, havecontinued. Treutler and Epkins (2003), for example, examined whether parents’ symptomsmade unique contributions to mothers’ and fathers’ reports of children’s behavior problems,as well as to discrepancies between mother–child, father–child, and father–mother reports.Maternal and paternal symptomatology contributed to father–mother discrepancies regardinginternalizing and externalizing type difficulties, indicating that differences between caregivers’reports were a function of both caregivers’ symptoms. Chi and Hinshaw (2002) investigatedthe depression–distortion hypothesis by examining the effects of maternal depressivesymptoms on cross-informant discrepancies in reports of child behavior problems for a sampleof children identified as presenting with attention deficit hyperactivity disorder (ADHD),combined type. Overall, maternal depressive symptoms predicted negative biases in theirreports of their child’s ADHD symptoms, general behavior problems, and their own negativeparenting style. Interestingly, increases in mothers’ symptoms of depression were associatedwith maternal reports of negative parenting, but not with indicators based on laboratoryobservations of parent–child interactions, suggesting possible depression–distortion effects.De Los Reyes and Prinstein (2004) applied the depression–distortion hypothesis to theassessment of peer victimization from the perspective of the victim, and examined whetheradolescents’ depressive symptoms and aggressive behavior were associated with discrepanciesbetween self- and peer reports of peer victimization experiences. Adolescents’ aggression wasassociated with underestimation of peer victimization directed toward the teen, on self-reportinstruments relative to peer reports, whereas depressive symptoms were associated withoverestimations of own peer victimization on self-report compared with peer reports.
Structural equation modeling (SEM) techniques have been used to directly test the hypothesisthat maternal depression contributes to over-report of behavior problems and thus leads todivergence from indicators derived from other informants, and an increase in the errorassociated with maternal ratings of child behavior problems. Fergusson, Lynskey, andHorwood (1993) evaluated three models: (a) maternal depression was unrelated to maternalreport of child difficulties, (b) maternal depression causally influenced maternal report of childdifficulties, and (c) maternal depression was correlated with error in maternal report of childdifficulties. A sample of adolescent boys was included in this research, and informationregarding conduct disorder and attention deficit disorder was gathered from teachers, mothers,and children. Fergusson and colleagues detected moderate associations between maternaldepression and reporting errors, supporting the latter two models. However, questions remainregarding the applicability of these findings to girls as well as to other areas of child functioning(e.g., internalizing-type difficulties, including symptoms of depression and anxiety).
This study applied statistical advancements to understanding the extent to which maternaldepression distorts reports of child and adolescent psychopathology (Fergusson et al., 1993;Richters, 1992). First, an array of agents (e.g., mothers, fathers, teachers, and children) providedinformation about child adjustment that served as the bases for the multi-agent constructs of
Gartstein et al. Page 3
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

internalizing and externalizing problems. Second, a series of analyses was undertaken toascertain convergent and discriminant validity. These analyses were conducted to address theneed to establish superior validity of multiagent constructs used as criteria for ascertainingmaternal reporting errors (Fergusson et al., 1993; Richters, 1992). Finally, direct tests of thecontribution of maternal depressive symptoms to over-reporting, and thus the error associatedwith mother report of externalizing and internalizing difficulties in the context of multi-agentconstructs, were performed separately for sons and for daughters. The depression–distortionhypothesis was tested by using a series of SEM models, following methodologicalrecommendations (Fergusson et al., 1993; Stoolmiller, 1998). These tests were conductedseparately for females and for males based on past research suggesting gender differences inpsychopathology and behavior problems among youth (e.g.; Hayward & Sanborn, 2002;McManus, Alessi, Grapentine, & Brickman, 1984; Rutter, Izard, & Read, 1986).
First, it was hypothesized that the validity evaluations conducted in the course of this studywould support the validity of the multi-agent constructs addressing internalizing andexternalizing behavior problems. Specifically, results of the evaluation of convergent anddiscriminant validity were expected to support the appropriateness of independent, but related,internalizing and externalizing problems constructs. In addition, it was hypothesized thatmodels accounting for correlated residuals across different indicators provided by the sameinformant would be superior to those not accounting for the non-independence of these errorterms (Garber, Quiggle, Panak, & Dodge, 1991; Nelson, Hammen, Brennan, & Ullman,2003). Second, relations between maternal depressive symptoms and child behavior problemswere hypothesized, with higher levels of maternal depression being associated with higherlevels of child behavior problems. Third, we hypothesized that higher levels of maternaldepressive symptoms would be linked with increases in the measurement error associated withmothers’ report of adolescent psychopathology.
2. Method2.1. Participants
The data presented in this study were collected in the context of the Adolescent TransitionsProgram (ATP), a group intervention curriculum for teens and their parents. Participants inthis study were self-referred and had learned about the program through a variety of sources,including community and newspaper advertisements and teacher and counselor referrals (seeDishion & Andrews, 1995; Dishion, Andrews, Kavanagh, & Soberman, 1996). The programwas fully explained during the first telephone contact, which had been initiated by the parentsinquiring about ATP. During this initial contact, interested parents participated in a telephonescreening interview developed on the basis of risk factor research conducted by Bry, McKeon,and Pardina (1982). Parents were questioned regarding 10 dimensions of child risk (closenessto parents, emotional adjustment, academic engagement, involvement in positive activities,experience seeking, problem behaviors, the child’s substance use, peer substance use, familysubstance use history, and stressful life events), and the criterion for inclusion in theintervention was based on a cut-off of 4 factors out of 10 being endorsed by the parent (Bry etal., 1982; Dishion & Andrews, 1995). This inclusion/exclusion criterion led to the retention of50% of the original sample, all of whom participated in the baseline assessment. Thus, datawere collected from mothers (N = 219), teachers (N = 218), and fathers (N = 123) of 221 children(113 girls and 108 boys), who also provided self-report data. The youth were between ages 10and 14 years, M (SD) = 12.31 (.80) for females and M (SD) = 12.43 (.87) for males. Slightlymore than 47% of the participating families represented one-parent households, determined onthe basis of the mother’s report of having been a single parent for 1 or more years. The averagenumber of children per family was 2.2.
Gartstein et al. Page 4
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
This sample was primarily low income, but moderately well educated. The majority of mothers(85.7%) and fathers (78.6%) graduated from high school; more than 50% of mothers and 45%of fathers had some college education. However, the median annual household income wasbetween $15 000.00 and $20 000.00, and the level of unemployment (23.2%) and thepercentage of families receiving financial assistance (58%) were relatively high. More than90% of the families were European American, roughly representing the ethnic distribution inthe community (Dishion & Andrews, 1995).
2.2. MeasuresChild Behavior Checklist (CBCL)—The CBCL (Achenbach, 1991) is a widely usedmeasure of children’s social and academic functioning and behavioral problems. The behaviorproblems portion includes 118 items that yield scores for eight narrowband clinical scales, twobroadband (composite) scales, externalizing and internalizing behavior problems, and the totalbehavior problems score. The externalizing and internalizing composite scores, based on thereports of mothers and fathers, were used in this investigation. Adequate reliability and validityhave been reported for the CBCL (Achenbach, 1991). With the ATP sample, youthinternalizing items were found to be internally consistent on the basis of mother (α = .86) andfather report (α = .88); externalizing items were also found to be reliable (αmothers = .92;αfathers = .93).
2.2.1. Teacher Report Form (TRF)—The TRF (Achenbach, 1991) represents a teacherreport version of the CBCL. The TRF has been frequently used in a wide range of studies,providing evidence of its reliability and validity. This measure yields a number of narrowbandand composite scores parallel to the parent-report measure and can be scored in a manner thatproduces content consistent with that of the CBCL (Achenbach, 1991). Internalizing andexternalizing composite scores, based on teacher report, were used in this study (αexternalizing= .94; αinternalizing = .89).
2.2.2. Center for Epidemiological Studies Depression Scale (CES–D)—The CES–D (Radloff, 1977) is a 20-item self-report scale of depression, with questions addressingpresence or absence of negative and positive thoughts, feelings, and behaviors, as well as thesomatic manifestations of depression. Satisfactory reliability and validity have beendemonstrated for this screening measure of depressive symptoms. A total score (sum) wascomputed for mothers participating in this study, and items were found to be internallyconsistent (α = .92). The CES–D represents one of the indicators of maternal depressionevaluated in this study. The frequency of clinically significant reports of depression for mothers(34%) was somewhat higher in this sample than for the CES–D normative sample (21%;Radloff, 1977), based on the recommended cut-off score of 16 on the CES-D (Radloff,1977).
2.2.3. Brief Symptom Inventory (BSI)—The BSI (Derogatis, 1993) is a 53-item self-report symptom inventory developed to capture psychological symptomatology for clinicaland community samples. A brief form of the Symptom Checklist 90–Revised (SCL–90–R), ituses a 5-point Likert scale ranging from 0 (not at all distressful) to 4 (extremely distressful).The measure is scored to generate profiles spanning nine symptom dimensions and three globaldistress markers. Two of the nine symptom dimensions were used in this study: mother reportof depression (six items; α = .86) and youth report of both depression (six items; α = .85) andhostility (five items; α = .73). Mother depression score was used in the context of the depressionconstruct, along with the CES–D indicator, whereas youth depression and hostility scores wereincluded in the internalizing and externalizing multi-agent constructs, respectively.
Gartstein et al. Page 5
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
2.3. ProcedureMeasures reported in this study were administered at baseline of a longitudinal interventionevaluation project. Mothers and fathers completed the CBCL, teachers responded to the TRF,and youth filled out the BSI to assess youth externalizing and internalizing problems at baseline.At the same time, mothers completed both indicators of maternal depression (CES–D and theBSI). Parents and children completed their questionnaires at home at their convenience,returned them to researcher staff during a scheduled visit, and were reimbursed $10 for theireffort. Teachers completed their portion of the assessment in the school setting, returnedcompleted forms to the researchers, generally by mail, and were reimbursed $8.00 forparticipation. Parents and children participated in the ATP intervention after the baselineassessment. The intervention protocols are described in detail in Dishion and Andrews(1995), Dishion et al. (1996), and Poulin, Dishion, and Burraston (2001).
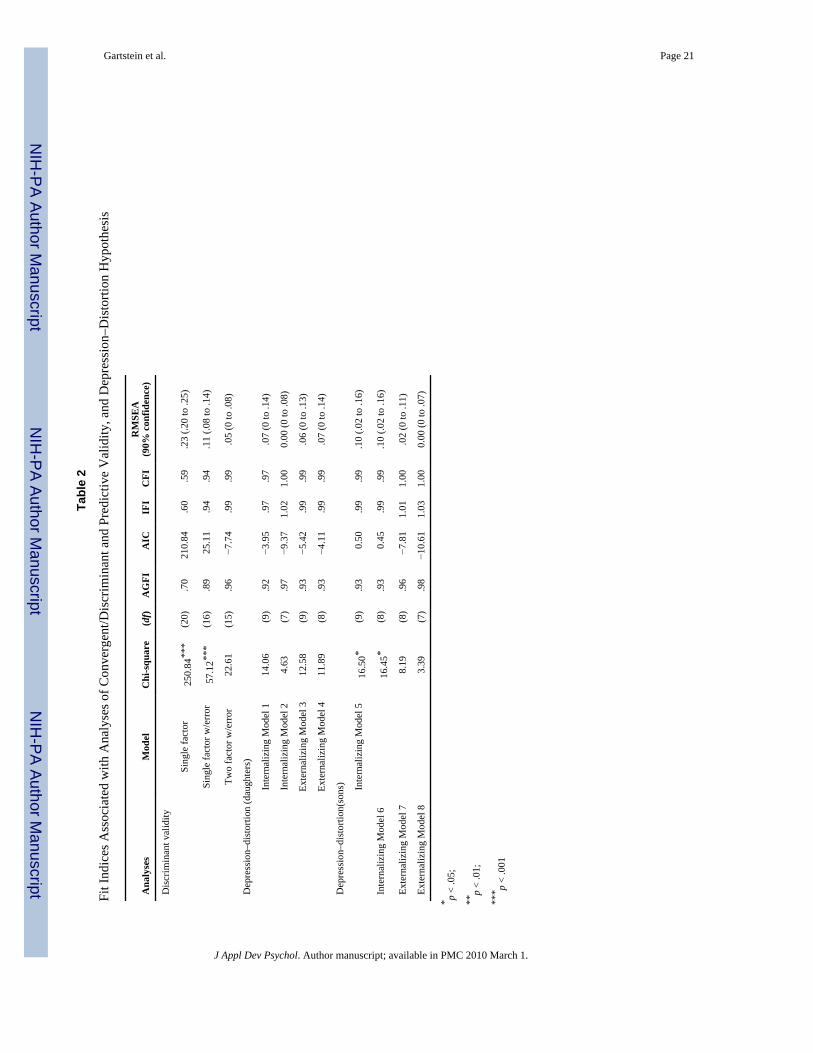
2.3.1. SEM Analytic Strategy—EQS 6.1 (Bentler, 2004) was used for all SEM analyses.All SEM analyses were conducted using maximum likelihood estimation for parameterestimation (Myung, 2003), with missing data handled using maximum likelihood estimators(Arbuckle, 1996). The following fit indices, in addition to chi-square tests, were reported forall models tested: Adjusted Goodness of Fit Index (AGFI; Raykov & Marcoulides, 2000),Akaike Information Criterion (AIC; Akaike, 1987), Incremental Fit Index (IFI; Bollen,1989), Comparative Fit Index (CFI; Bentler, 1990), and Root Mean-Square Error ofApproximation (RMSEA; Loehlin, 1998). Collectively, these fit indices satisfied the followingcriteria: (a) minimally impacted by sample size (Bollen, 1986), (b) sensitivity to modelmisspecification, and (c) lack of upward or downward systematic bias (Fan, Thompson, &Wang, 1999). For the AGFI, CFI, and IFI, values larger than .90 are indicative of adequatemodel fit, with values ranging between .95 and 1.00 considered a well-fitting model. For boththe RMSEA and the AIC, lower values reflect improved model fit relative to higher values,with the AIC not constrained by a lower or upper bound. However, for the RMSEA, valuesbetween 0 and .05 reflect good model fit, with values between .06 and .10 reflecting adequatemodel fit. RMSEA values greater than .10 reflect models with questionable fit. Finally, changein chi-square tests were used to examine differences between tested models.
To examine the convergent and the discriminant validity of child psychopathology, aconfirmatory factor analytic (CFA) approach was used, with a single-factor model, a singlefactor with correlated errors model, and a two-factor (externalizing and internalizing) modelwith correlated errors compared. Specifically, mother and father CBCL, teacher TRF, and childself-reported BSI Time 1 assessments of internalizing and externalizing behaviors were used.Correlated errors were anticipated because of the potential for rater bias, which can occur whenan individual reports on one or more constructs (e.g., an indication of one symptom mayincrease the likelihood of reporting other symptoms across different areas of functioning;Nelson et al., 2003). The best-fitting model resulting from the CFA approach described earlierwas adopted for subsequent analyses.
After the convergent and discriminant validity of the multi-agent construct were established,the depression–distortion hypothesis was examined. For these analyses, the null model wasone without a path from the latent construct of maternal depression to the error term associatedwith maternal report of child (sons’ or daughters’) internalizing/externalizing symptoms. Themodel compared against the null model included a path from the latent construct of maternaldepression to maternal report of child internalizing/externalizing symptoms. This set ofanalyses resulted in four alternative models being tested against their respective null models.
Gartstein et al. Page 6
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
3. Results3.1. Preliminary Analyses
Prior to conducting SEM analyses, we examined the potential impact of missing data fromfathers (n = 101, or 47.34% of potential father respondents had missing data) on maternal andchild outcomes relevant to the multi-informant nature of the SEM analyses and the potentialimplications for maternal and child well-being in the presence of missing father data.Unfortunately, adequate data regarding divorce/marriage rates for the majority of participantswere not reported (74.3% did no respond to this question). Nevertheless, of the 58 participantswho responded to this particular question, 60.4% indicated being currently married, with 39.6%reporting either being divorced or never married. This information suggested that mothers andchildren participating in this study experienced rates of family disruption consistent withwidely reported rates of divorce across the country, and that it would not be appropriate toconclude that missing data from fathers (44.7%) was solely a function of family disruptionssuch as divorce. A series of 2 (child gender: male vs. female) × 2 (paternal report present:missing paternal data vs. no missing paternal data) ANOVAs were conducted on the followingvariables: a combined maternal depression score consisting of maternal CES-D and maternalBSI depression, child reports of their own BSI depression and hostility symptoms, and maternaland teacher reports of CBCL child internalizing and externalizing difficulties. No significanteffects were observed for child reports of their own BSI depression or hostility symptoms ormaternal and teacher reports of CBCL child internalizing difficulties (all p > .05). However,significant main effects for gender were observed with maternal, F(1, 215) = 6.95, p < .05, andteacher, F(1, 211) = 20.89, p < .05, report of externalizing difficulties. Both mothers andteachers indicated significantly higher externalizing symptoms for males (M = 20.58 and 14.85,respectively) compared with females (M = 16.81 and 6.98, respectively). These findings,consistent with those of recent investigations, showed similar discrepancies between male andfemale children on externalizing difficulties (Rescorla et al., 2007a; Rescorla et al., 2007b).Significant main effects of paternal report present on maternal- and teacher-reportedexternalizing difficulties were not observed, F(1, 215) = 0.33, p > .05 and F(1, 211) = 0.049,p > .05, respectively, nor were significant gender × paternal report present effects on maternal-and teacher-reported child externalizing difficulties noted, F(1, 215) = 0.36, p < .05 and F(1,211) = 0.074, p > .05, respectively.
For the purposes of this set of analyses, maternal CES-D and BSI depression scores weresummed to create a composite maternal depression score because of the association betweenmaternal CES-D and BSI depression scores, r(216) = .82, p < .001. Results of analyses relyingon this depression composite as a dependent variable indicated that there were no main effectsfor child gender, F(1, 214) = 0.061, p > .05, or paternal report present, F(1, 214) = 1.76, p > .05, nor was there a child gender × paternal report present interaction, F(1, 214) = 0.51, p > .05. Thus, evidence suggests that the ability of paternal caregivers to participate or notparticipate (for any reason) in the current study will have a negligible, if any, systematic impacton subsequent analyses.
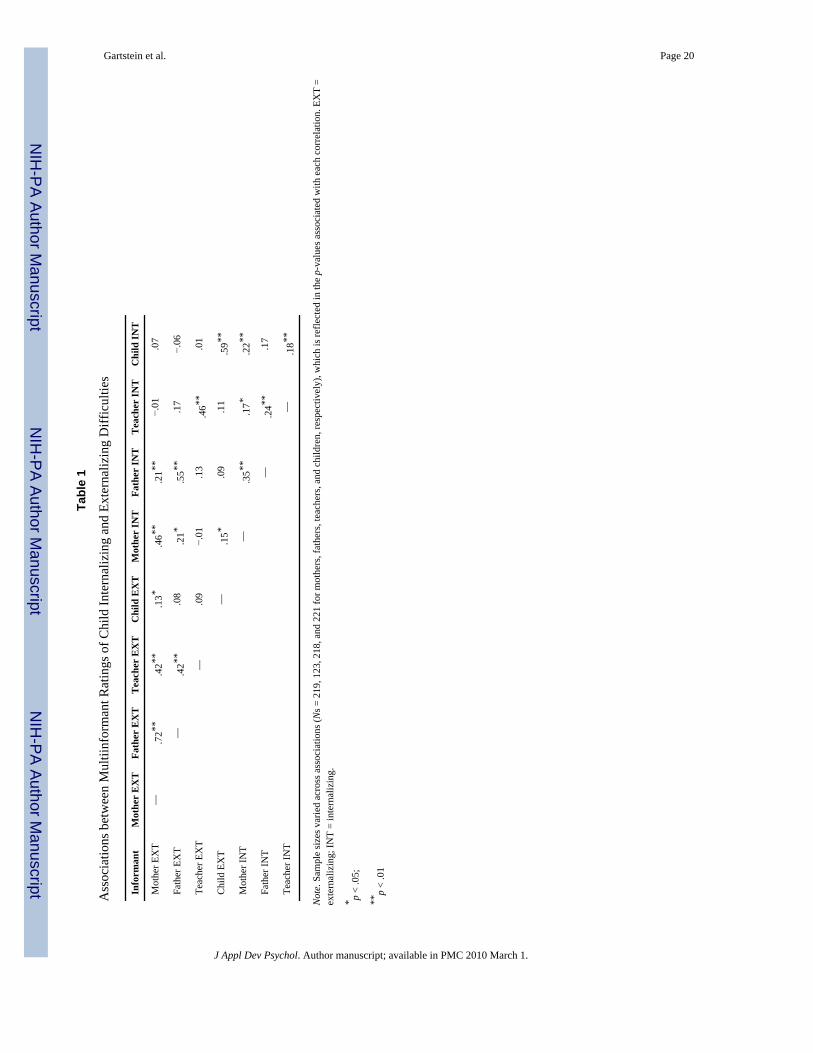
Finally, given the multi-informant nature of this study, associations between maternal, paternal,teacher, and child reports of internalizing and externalizing symptoms were examined. Thesefindings are presented in Table 1, with most associations emerging as significant and occurringin the anticipated direction across informants.
3.2. Validation of Externalizing and Internalizing Criterion MeasuresFindings associated with the discriminant validity analyses supported a model with twoseparate but related constructs of externalizing and internalizing behavior problems. The initialsingle-factor model provided a poor fit to the data. The final two-factor model with error
Gartstein et al. Page 7
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
provided a significant improvement in fit, Δ χ2 (df = 1) = 34.86, p < .001, relative to the single-factor, correlated error model. Examination of factor loadings from the final model (range .17to .83, average loading .49) provided support for convergent validity of the different indicators(i.e., mother, father, teacher, and child report) for the internalizing and externalizing constructs.
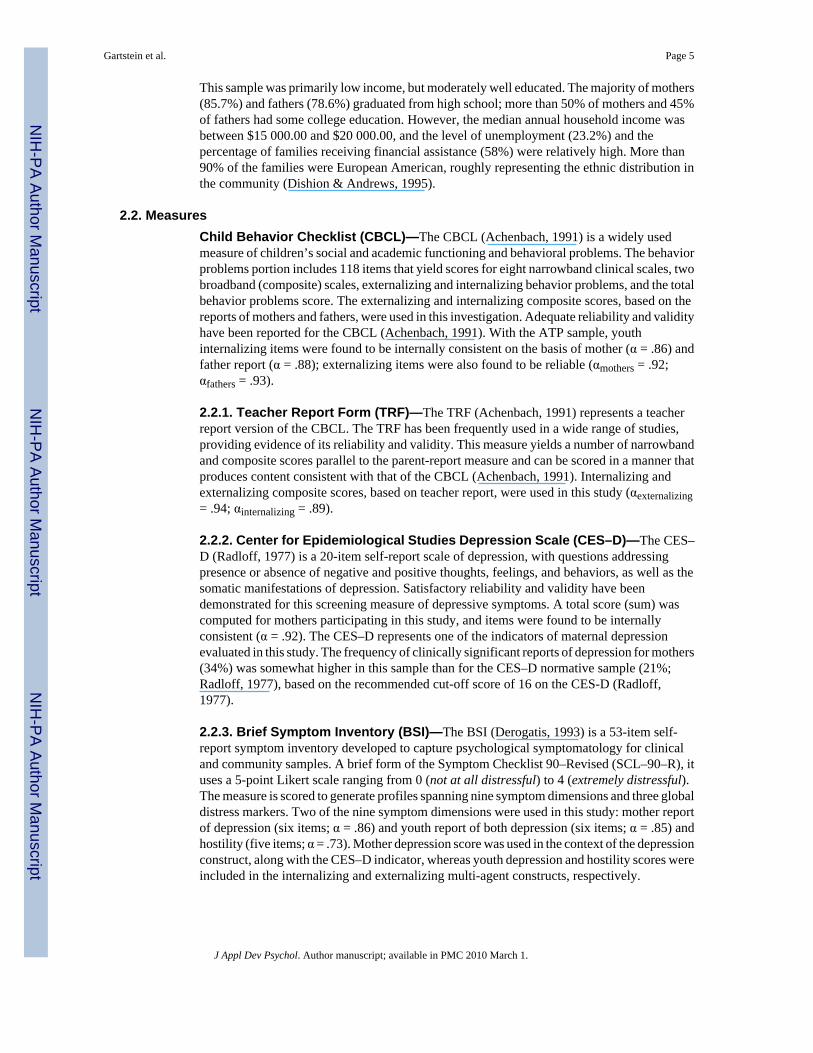
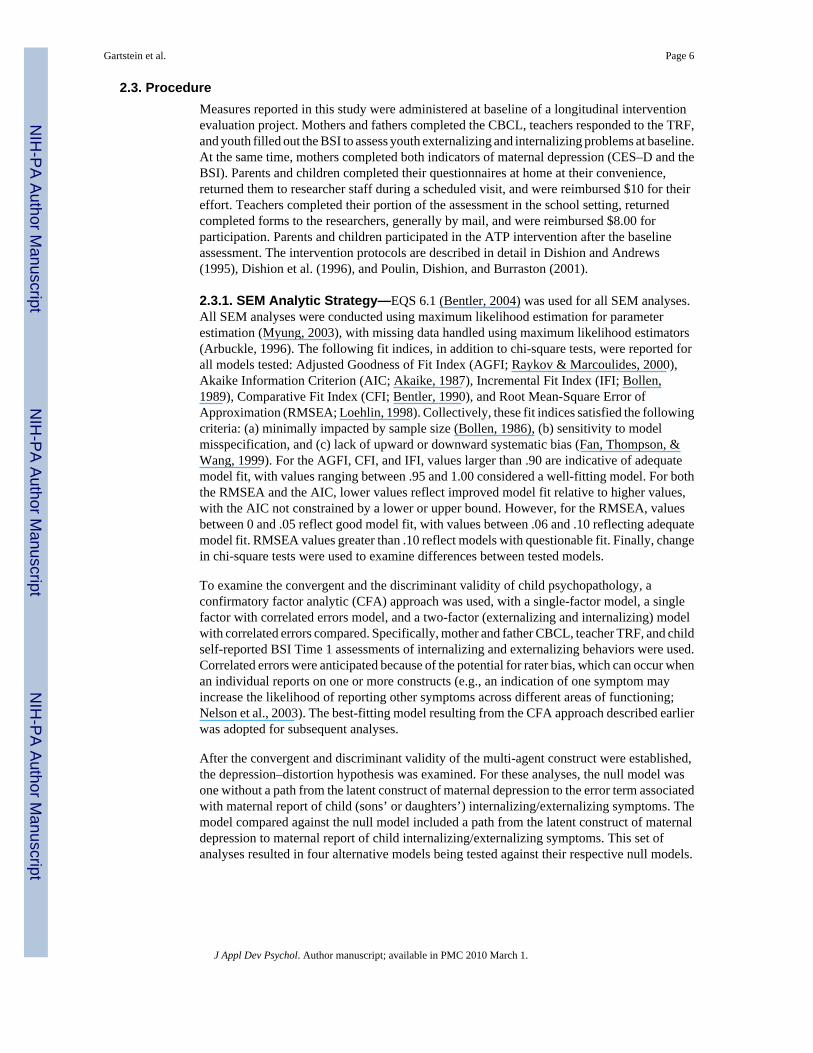
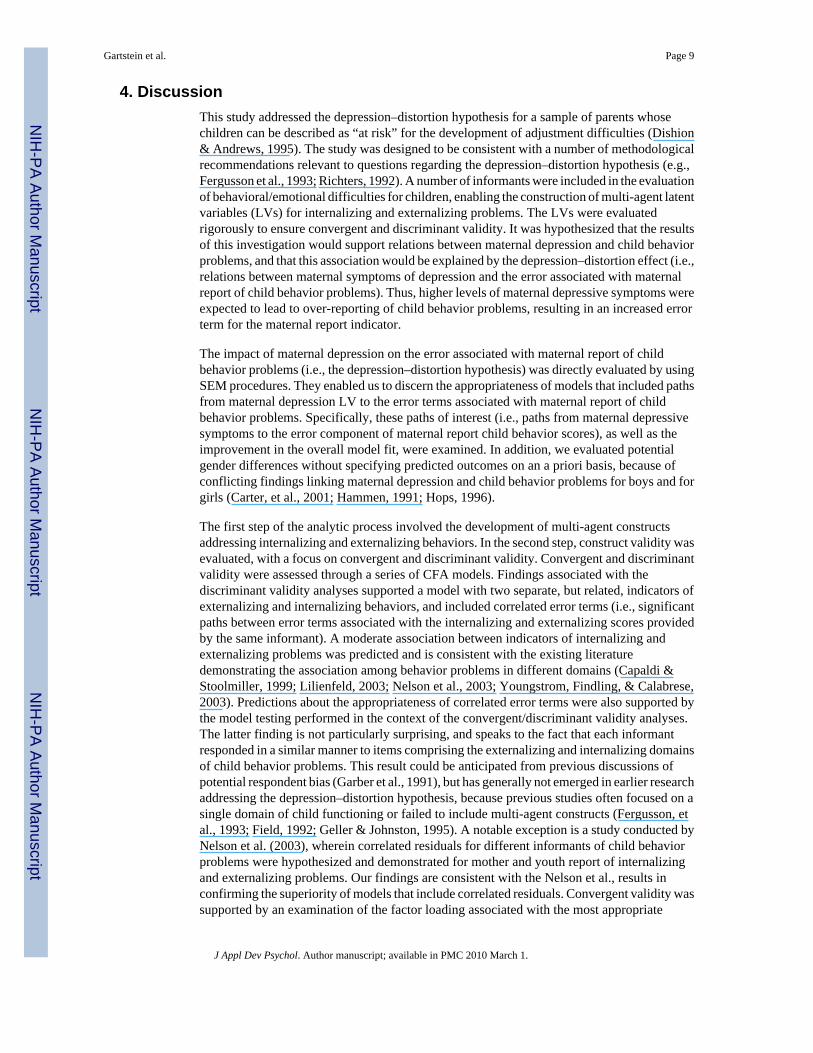
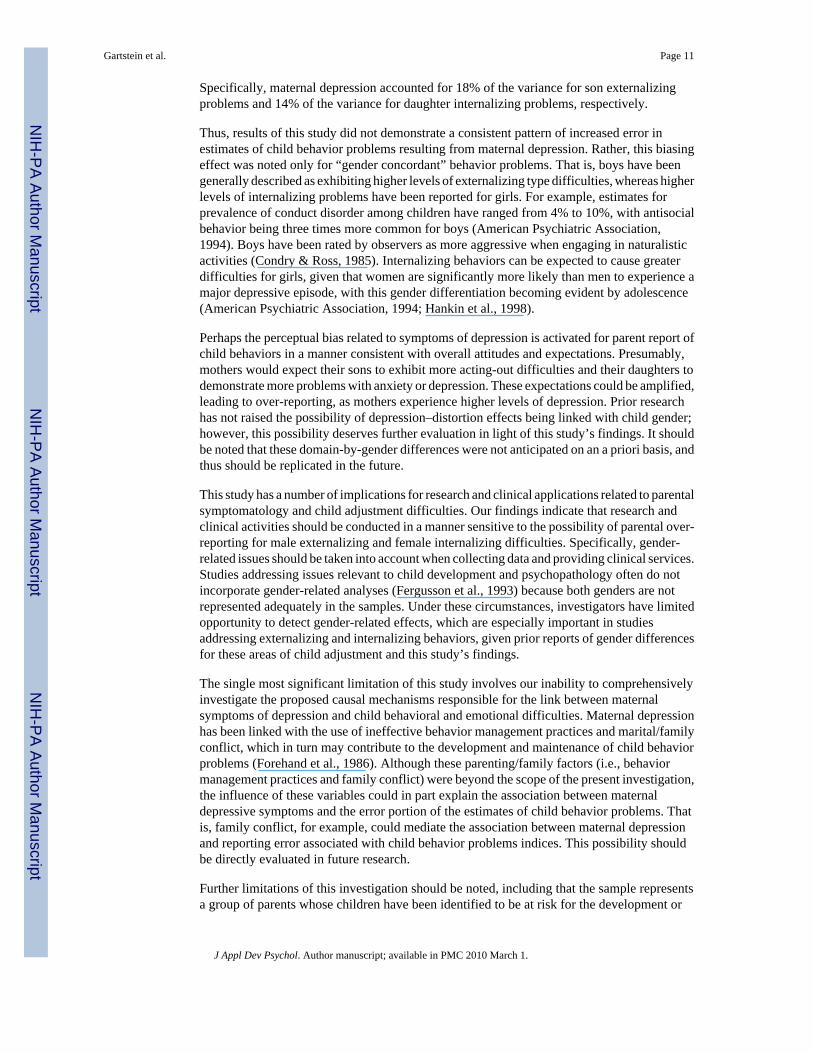
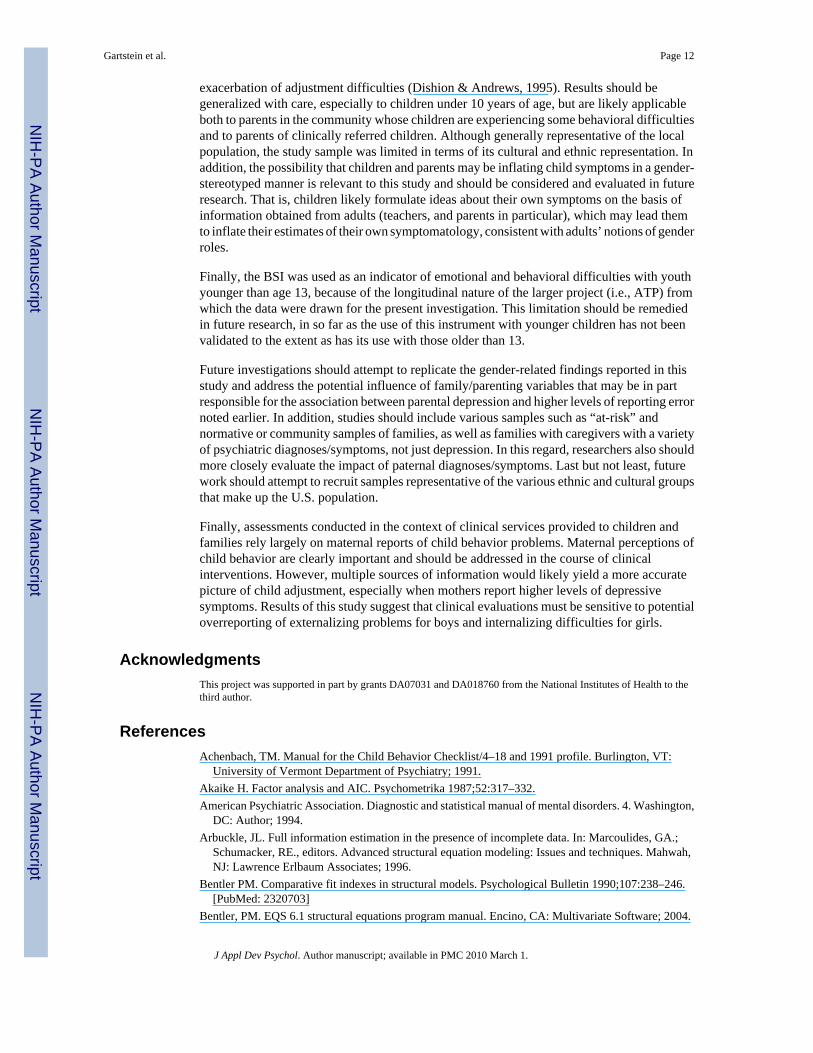
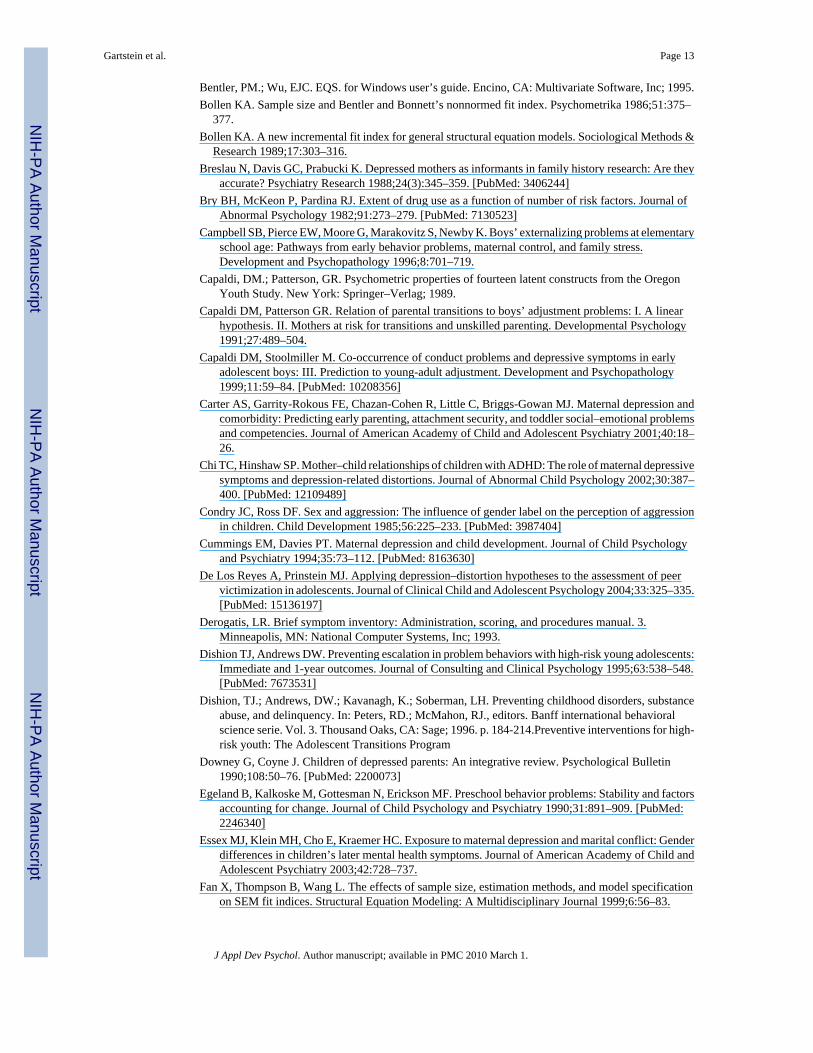
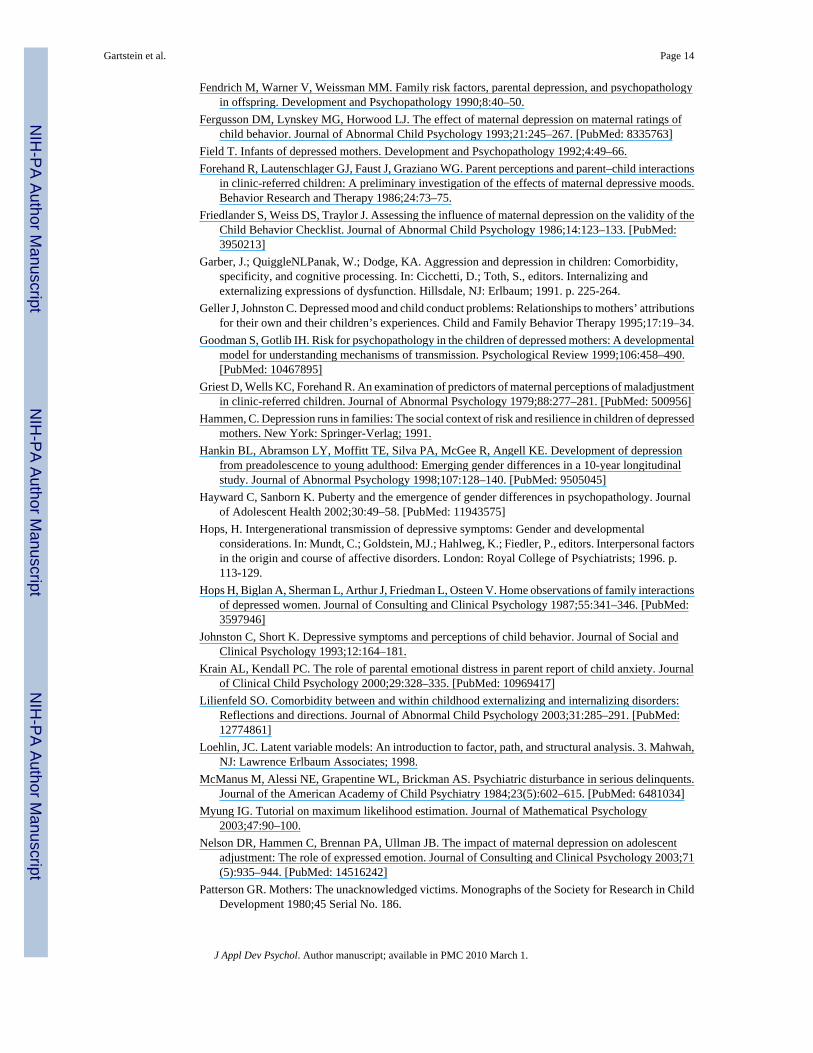
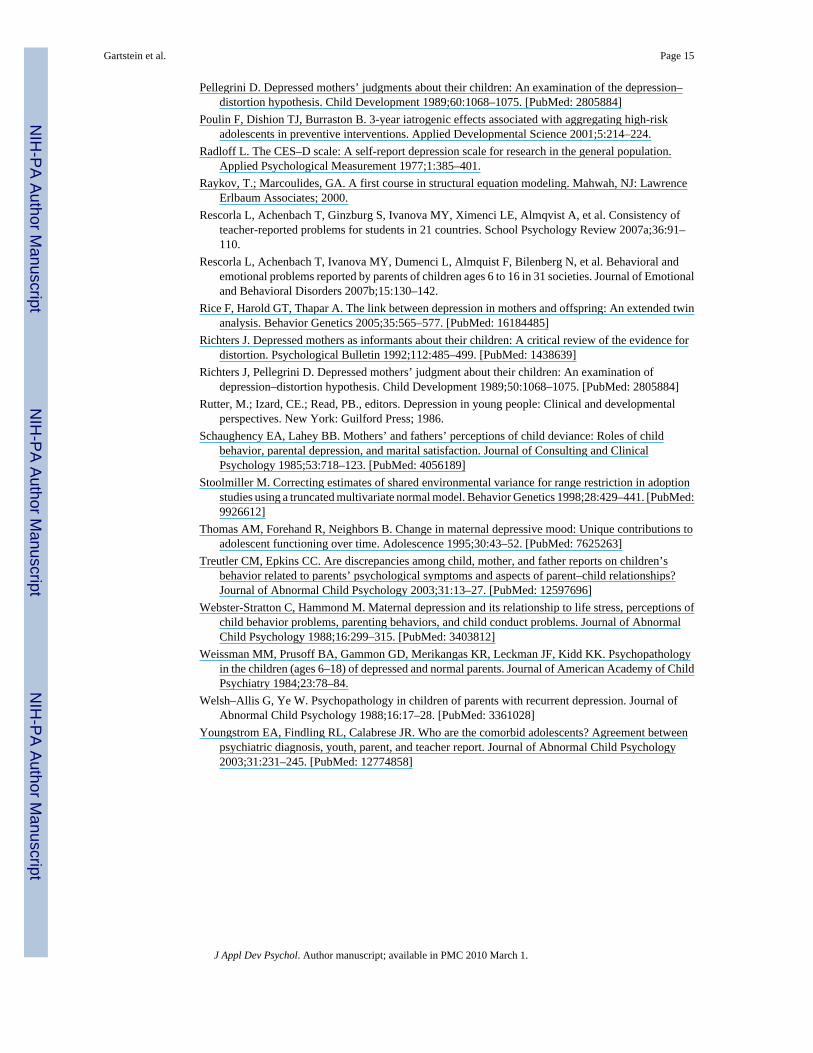
3.3. Depression–Distortion Hypothesis ResultsGiven the evidence of higher levels of externalizing difficulties in male offspring relative tofemale offspring as noted by both mothers and teachers (see Preliminary Analyses above), thestudy proceeded with separate depression–distortion SEM analyses for sons and daughters,with separate analyses on internalizing and externalizing constructs for each. The null andalternative model estimates for all depression–distortion models are presented in Table 2, withthe alternative models (i.e., daughters: Models 2 and 4; sons: Models 6 and 8), including pathsof interest from maternal depressive symptoms to the error term associated with mothers’ reportof child behavior problems (depicted schematically in Figures 1–4). It should be noted that inEQS software, residuals must be designated as independent variables (e.g., have no one-wayarrow leading to them from another variable). In order to test the depression–distortion modelsby using EQS, the residuals associated with mother report of child internalizing andexternalizing behaviors had to be redesignated as a latent/unobserved variable. Thisredesignation resulted in a change from an independent to a dependent variable status, but hadno effect on the meaning of the variable in the model or on the associated paths (Bentler &Wu, 1995).
3.3.1. Daughters—Model 2 (Figure 1), reflecting the distortion hypothesis, produced asignificantly better fit to the data than did the corresponding Model 1, Δχ2 (df = 2) = 9.42, p< .01. In Model 2, the path from the latent variable of maternal depression to the error termassociated with maternal report of daughter internalizing problems was significant, indicatingthat increased maternal depression was associated with higher error term values. However,Model 4, with a path from the latent variable of maternal depression to the error term associatedwith maternal report of daughter externalizing behavior (Figure 2), failed to improve overallmodel fit, relative to Model 3, Δχ2 (df = 1) = .69, p > .05. Furthermore, the path from the latentvariable of maternal depression to the error term of interest was not significant, indicating thatmaternal depression did not have a distorting effect on maternal report of daughters’externalizing symptoms.
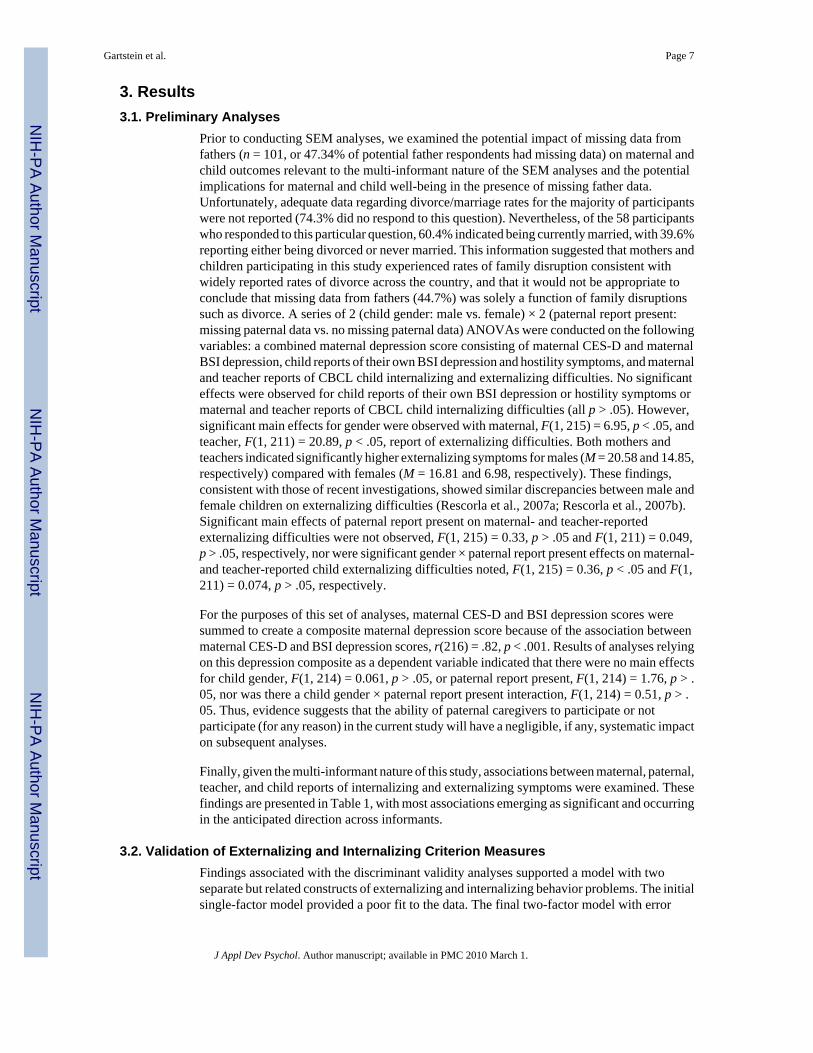
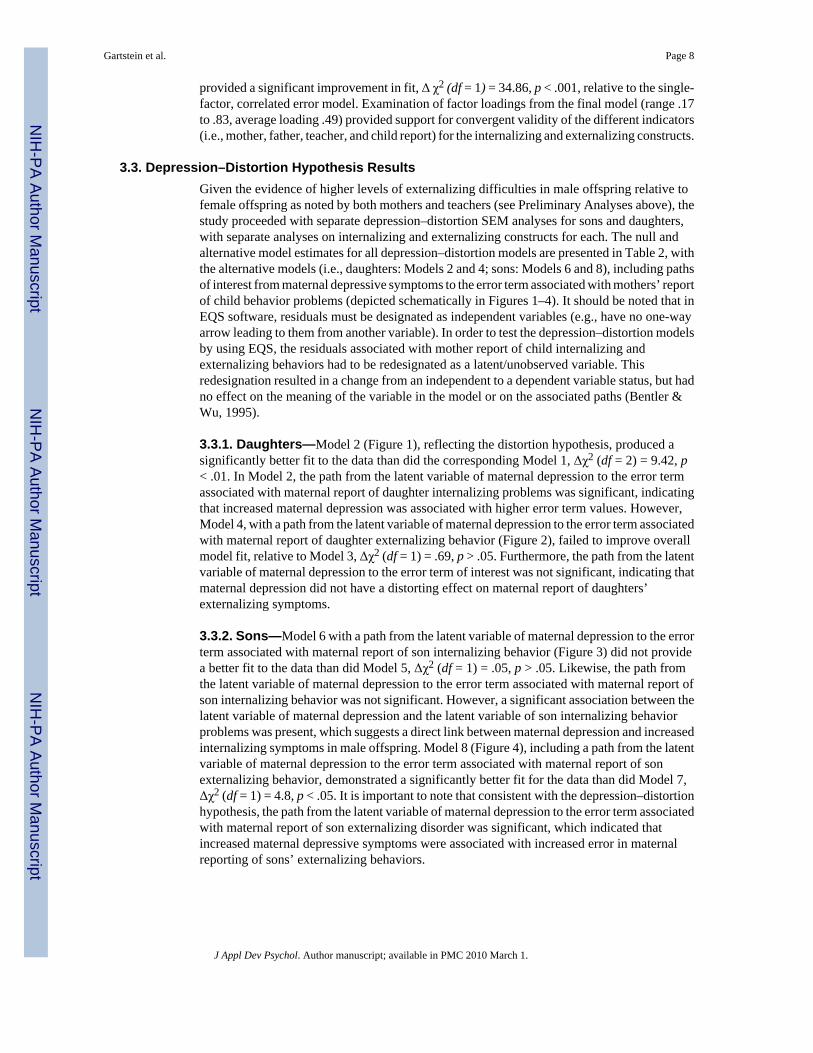
3.3.2. Sons—Model 6 with a path from the latent variable of maternal depression to the errorterm associated with maternal report of son internalizing behavior (Figure 3) did not providea better fit to the data than did Model 5, Δχ2 (df = 1) = .05, p > .05. Likewise, the path fromthe latent variable of maternal depression to the error term associated with maternal report ofson internalizing behavior was not significant. However, a significant association between thelatent variable of maternal depression and the latent variable of son internalizing behaviorproblems was present, which suggests a direct link between maternal depression and increasedinternalizing symptoms in male offspring. Model 8 (Figure 4), including a path from the latentvariable of maternal depression to the error term associated with maternal report of sonexternalizing behavior, demonstrated a significantly better fit for the data than did Model 7,Δχ2 (df = 1) = 4.8, p < .05. It is important to note that consistent with the depression–distortionhypothesis, the path from the latent variable of maternal depression to the error term associatedwith maternal report of son externalizing disorder was significant, which indicated thatincreased maternal depressive symptoms were associated with increased error in maternalreporting of sons’ externalizing behaviors.
Gartstein et al. Page 8
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
4. DiscussionThis study addressed the depression–distortion hypothesis for a sample of parents whosechildren can be described as “at risk” for the development of adjustment difficulties (Dishion& Andrews, 1995). The study was designed to be consistent with a number of methodologicalrecommendations relevant to questions regarding the depression–distortion hypothesis (e.g.,Fergusson et al., 1993; Richters, 1992). A number of informants were included in the evaluationof behavioral/emotional difficulties for children, enabling the construction of multi-agent latentvariables (LVs) for internalizing and externalizing problems. The LVs were evaluatedrigorously to ensure convergent and discriminant validity. It was hypothesized that the resultsof this investigation would support relations between maternal depression and child behaviorproblems, and that this association would be explained by the depression–distortion effect (i.e.,relations between maternal symptoms of depression and the error associated with maternalreport of child behavior problems). Thus, higher levels of maternal depressive symptoms wereexpected to lead to over-reporting of child behavior problems, resulting in an increased errorterm for the maternal report indicator.
The impact of maternal depression on the error associated with maternal report of childbehavior problems (i.e., the depression–distortion hypothesis) was directly evaluated by usingSEM procedures. They enabled us to discern the appropriateness of models that included pathsfrom maternal depression LV to the error terms associated with maternal report of childbehavior problems. Specifically, these paths of interest (i.e., paths from maternal depressivesymptoms to the error component of maternal report child behavior scores), as well as theimprovement in the overall model fit, were examined. In addition, we evaluated potentialgender differences without specifying predicted outcomes on an a priori basis, because ofconflicting findings linking maternal depression and child behavior problems for boys and forgirls (Carter, et al., 2001; Hammen, 1991; Hops, 1996).
The first step of the analytic process involved the development of multi-agent constructsaddressing internalizing and externalizing behaviors. In the second step, construct validity wasevaluated, with a focus on convergent and discriminant validity. Convergent and discriminantvalidity were assessed through a series of CFA models. Findings associated with thediscriminant validity analyses supported a model with two separate, but related, indicators ofexternalizing and internalizing behaviors, and included correlated error terms (i.e., significantpaths between error terms associated with the internalizing and externalizing scores providedby the same informant). A moderate association between indicators of internalizing andexternalizing problems was predicted and is consistent with the existing literaturedemonstrating the association among behavior problems in different domains (Capaldi &Stoolmiller, 1999; Lilienfeld, 2003; Nelson et al., 2003; Youngstrom, Findling, & Calabrese,2003). Predictions about the appropriateness of correlated error terms were also supported bythe model testing performed in the context of the convergent/discriminant validity analyses.The latter finding is not particularly surprising, and speaks to the fact that each informantresponded in a similar manner to items comprising the externalizing and internalizing domainsof child behavior problems. This result could be anticipated from previous discussions ofpotential respondent bias (Garber et al., 1991), but has generally not emerged in earlier researchaddressing the depression–distortion hypothesis, because previous studies often focused on asingle domain of child functioning or failed to include multi-agent constructs (Fergusson, etal., 1993; Field, 1992; Geller & Johnston, 1995). A notable exception is a study conducted byNelson et al. (2003), wherein correlated residuals for different informants of child behaviorproblems were hypothesized and demonstrated for mother and youth report of internalizingand externalizing problems. Our findings are consistent with the Nelson et al., results inconfirming the superiority of models that include correlated residuals. Convergent validity wassupported by an examination of the factor loading associated with the most appropriate
Gartstein et al. Page 9
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

solution. Thus, results of the analyses addressing convergent and discriminant validity providedsupport for the construct validity of these LVs, consistent with earlier reports advocating theuse of such constructs (Capaldi & Patterson, 1989, 1991).
Results of this study can be described as partly consistent with the depression–distortionhypothesis and prior reports of a negative depression-related bias in parental ratings of childbehaviors (Field, 1992; Geller & Johnston, 1995; Griest, Wells, & Forehand, 1979; Johnston& Short, 1993). Overall, the association between maternal symptoms of depression and childbehavior problems (distorted or veridical) was supported in six of the eight examined models.This association did not emerge as statistically significant only in the analyses of maternaldepressive symptoms and daughter externalizing behavior problems. A significant associationbetween maternal depression and child behavior problems was supported by the initial modeladdressing boys’ externalizing symptoms. However, after the path representing the relationsbetween maternal depression and the error component of externalizing problems ratings forboys was introduced, the coefficient associated with the path from maternal depression to theexternalizing LV became nonsignificant. Conversely, a significant association between amaternal depression and boys’ internalizing problems LV was observed even after theintroduction of the path representing the distorting effect of maternal depressive symptoms.Thus, there was no support for the depression-related distortion in the evaluation of theassociation between maternal depressive symptoms and son internalizing problems. Rather,SEM analyses supported veridical relations between maternal depressive and son internalizingsymptoms, with son symptoms increasing at higher levels of maternal dysphoria.
Evaluations of the associations between maternal depressive symptoms and child behaviorproblems have focused primarily on disruptive or externalizing difficulties, especially for boys(Campbell et al., 1996; Egeland et al., 1990; Webster-Stratton & Hammond, 1988). However,results of our investigation indicate that the association between mothers’ depression and sons’internalizing problems (e.g., symptoms of depression and anxiety) may be equally important.This study’s findings are consistent with a recent report of similar gender-related differences,wherein boys’, but not girls’, internalizing symptoms were linked with the effect of maternaldepression (Essex et al., 2003). Specifically, boys exposed to maternal depression in infancydemonstrated a preponderance of internalizing behaviors, whereas for girls, internalizingsymptoms increased particularly as a result of exposure to marital conflict occurring in thetoddler/preschool period. Our findings suggest that for male children, mothers’ symptoms ofdepression may have a direct effect on son’s internalizing behavior problems later in childhood.A presentation that includes emotional unavailability, negative affect, and cognitionsassociated with depression likely contributes to this effect (Cummings & Davies, 1994;Goodman & Gotlib, 1999) and leads to a similar constellation of difficulties for male offspring.Alternatively, this link between maternal symptoms of depression and boys’ internalizingsymptoms may be a function of genetic influences, more pronounced in the male offspring.Previous research, however, has not provided evidence of differences in the genetictransmission of risk for depression for male and for female offspring, suggesting anenvironmental basis for the gender differences observed in this study (Rice, Harold, & Thapar,2005).
Perhaps most important, significant positive coefficients emerged as indicators of theassociation between maternal symptoms of depression and the error component of maternalreport for child behavior problems, indicating that the amount of reporting error increased athigher levels of depressive symptomatology, consistent with the depression–distortionhypothesis. It should be noted that the significance of this contribution varied as a function ofdomain of adjustment difficulties (i.e., internalizing versus externalizing) and child gender.Our findings indicated that mothers with higher levels of depressive symptoms over-reportedexternalizing behavior problems for sons and internalizing difficulties for daughters.
Gartstein et al. Page 10
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Specifically, maternal depression accounted for 18% of the variance for son externalizingproblems and 14% of the variance for daughter internalizing problems, respectively.
Thus, results of this study did not demonstrate a consistent pattern of increased error inestimates of child behavior problems resulting from maternal depression. Rather, this biasingeffect was noted only for “gender concordant” behavior problems. That is, boys have beengenerally described as exhibiting higher levels of externalizing type difficulties, whereas higherlevels of internalizing problems have been reported for girls. For example, estimates forprevalence of conduct disorder among children have ranged from 4% to 10%, with antisocialbehavior being three times more common for boys (American Psychiatric Association,1994). Boys have been rated by observers as more aggressive when engaging in naturalisticactivities (Condry & Ross, 1985). Internalizing behaviors can be expected to cause greaterdifficulties for girls, given that women are significantly more likely than men to experience amajor depressive episode, with this gender differentiation becoming evident by adolescence(American Psychiatric Association, 1994; Hankin et al., 1998).
Perhaps the perceptual bias related to symptoms of depression is activated for parent report ofchild behaviors in a manner consistent with overall attitudes and expectations. Presumably,mothers would expect their sons to exhibit more acting-out difficulties and their daughters todemonstrate more problems with anxiety or depression. These expectations could be amplified,leading to over-reporting, as mothers experience higher levels of depression. Prior researchhas not raised the possibility of depression–distortion effects being linked with child gender;however, this possibility deserves further evaluation in light of this study’s findings. It shouldbe noted that these domain-by-gender differences were not anticipated on an a priori basis, andthus should be replicated in the future.
This study has a number of implications for research and clinical applications related to parentalsymptomatology and child adjustment difficulties. Our findings indicate that research andclinical activities should be conducted in a manner sensitive to the possibility of parental over-reporting for male externalizing and female internalizing difficulties. Specifically, gender-related issues should be taken into account when collecting data and providing clinical services.Studies addressing issues relevant to child development and psychopathology often do notincorporate gender-related analyses (Fergusson et al., 1993) because both genders are notrepresented adequately in the samples. Under these circumstances, investigators have limitedopportunity to detect gender-related effects, which are especially important in studiesaddressing externalizing and internalizing behaviors, given prior reports of gender differencesfor these areas of child adjustment and this study’s findings.
The single most significant limitation of this study involves our inability to comprehensivelyinvestigate the proposed causal mechanisms responsible for the link between maternalsymptoms of depression and child behavioral and emotional difficulties. Maternal depressionhas been linked with the use of ineffective behavior management practices and marital/familyconflict, which in turn may contribute to the development and maintenance of child behaviorproblems (Forehand et al., 1986). Although these parenting/family factors (i.e., behaviormanagement practices and family conflict) were beyond the scope of the present investigation,the influence of these variables could in part explain the association between maternaldepressive symptoms and the error portion of the estimates of child behavior problems. Thatis, family conflict, for example, could mediate the association between maternal depressionand reporting error associated with child behavior problems indices. This possibility shouldbe directly evaluated in future research.
Further limitations of this investigation should be noted, including that the sample representsa group of parents whose children have been identified to be at risk for the development or
Gartstein et al. Page 11
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
exacerbation of adjustment difficulties (Dishion & Andrews, 1995). Results should begeneralized with care, especially to children under 10 years of age, but are likely applicableboth to parents in the community whose children are experiencing some behavioral difficultiesand to parents of clinically referred children. Although generally representative of the localpopulation, the study sample was limited in terms of its cultural and ethnic representation. Inaddition, the possibility that children and parents may be inflating child symptoms in a gender-stereotyped manner is relevant to this study and should be considered and evaluated in futureresearch. That is, children likely formulate ideas about their own symptoms on the basis ofinformation obtained from adults (teachers, and parents in particular), which may lead themto inflate their estimates of their own symptomatology, consistent with adults’ notions of genderroles.
Finally, the BSI was used as an indicator of emotional and behavioral difficulties with youthyounger than age 13, because of the longitudinal nature of the larger project (i.e., ATP) fromwhich the data were drawn for the present investigation. This limitation should be remediedin future research, in so far as the use of this instrument with younger children has not beenvalidated to the extent as has its use with those older than 13.
Future investigations should attempt to replicate the gender-related findings reported in thisstudy and address the potential influence of family/parenting variables that may be in partresponsible for the association between parental depression and higher levels of reporting errornoted earlier. In addition, studies should include various samples such as “at-risk” andnormative or community samples of families, as well as families with caregivers with a varietyof psychiatric diagnoses/symptoms, not just depression. In this regard, researchers also shouldmore closely evaluate the impact of paternal diagnoses/symptoms. Last but not least, futurework should attempt to recruit samples representative of the various ethnic and cultural groupsthat make up the U.S. population.
Finally, assessments conducted in the context of clinical services provided to children andfamilies rely largely on maternal reports of child behavior problems. Maternal perceptions ofchild behavior are clearly important and should be addressed in the course of clinicalinterventions. However, multiple sources of information would likely yield a more accuratepicture of child adjustment, especially when mothers report higher levels of depressivesymptoms. Results of this study suggest that clinical evaluations must be sensitive to potentialoverreporting of externalizing problems for boys and internalizing difficulties for girls.
AcknowledgmentsThis project was supported in part by grants DA07031 and DA018760 from the National Institutes of Health to thethird author.
ReferencesAchenbach, TM. Manual for the Child Behavior Checklist/4–18 and 1991 profile. Burlington, VT:
University of Vermont Department of Psychiatry; 1991.Akaike H. Factor analysis and AIC. Psychometrika 1987;52:317–332.American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington,
DC: Author; 1994.Arbuckle, JL. Full information estimation in the presence of incomplete data. In: Marcoulides, GA.;
Schumacker, RE., editors. Advanced structural equation modeling: Issues and techniques. Mahwah,NJ: Lawrence Erlbaum Associates; 1996.
Bentler PM. Comparative fit indexes in structural models. Psychological Bulletin 1990;107:238–246.[PubMed: 2320703]
Bentler, PM. EQS 6.1 structural equations program manual. Encino, CA: Multivariate Software; 2004.
Gartstein et al. Page 12
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Bentler, PM.; Wu, EJC. EQS. for Windows user’s guide. Encino, CA: Multivariate Software, Inc; 1995.Bollen KA. Sample size and Bentler and Bonnett’s nonnormed fit index. Psychometrika 1986;51:375–
377.Bollen KA. A new incremental fit index for general structural equation models. Sociological Methods &
Research 1989;17:303–316.Breslau N, Davis GC, Prabucki K. Depressed mothers as informants in family history research: Are they
accurate? Psychiatry Research 1988;24(3):345–359. [PubMed: 3406244]Bry BH, McKeon P, Pardina RJ. Extent of drug use as a function of number of risk factors. Journal of
Abnormal Psychology 1982;91:273–279. [PubMed: 7130523]Campbell SB, Pierce EW, Moore G, Marakovitz S, Newby K. Boys’ externalizing problems at elementary
school age: Pathways from early behavior problems, maternal control, and family stress.Development and Psychopathology 1996;8:701–719.
Capaldi, DM.; Patterson, GR. Psychometric properties of fourteen latent constructs from the OregonYouth Study. New York: Springer–Verlag; 1989.
Capaldi DM, Patterson GR. Relation of parental transitions to boys’ adjustment problems: I. A linearhypothesis. II. Mothers at risk for transitions and unskilled parenting. Developmental Psychology1991;27:489–504.
Capaldi DM, Stoolmiller M. Co-occurrence of conduct problems and depressive symptoms in earlyadolescent boys: III. Prediction to young-adult adjustment. Development and Psychopathology1999;11:59–84. [PubMed: 10208356]
Carter AS, Garrity-Rokous FE, Chazan-Cohen R, Little C, Briggs-Gowan MJ. Maternal depression andcomorbidity: Predicting early parenting, attachment security, and toddler social–emotional problemsand competencies. Journal of American Academy of Child and Adolescent Psychiatry 2001;40:18–26.
Chi TC, Hinshaw SP. Mother–child relationships of children with ADHD: The role of maternal depressivesymptoms and depression-related distortions. Journal of Abnormal Child Psychology 2002;30:387–400. [PubMed: 12109489]
Condry JC, Ross DF. Sex and aggression: The influence of gender label on the perception of aggressionin children. Child Development 1985;56:225–233. [PubMed: 3987404]
Cummings EM, Davies PT. Maternal depression and child development. Journal of Child Psychologyand Psychiatry 1994;35:73–112. [PubMed: 8163630]
De Los Reyes A, Prinstein MJ. Applying depression–distortion hypotheses to the assessment of peervictimization in adolescents. Journal of Clinical Child and Adolescent Psychology 2004;33:325–335.[PubMed: 15136197]
Derogatis, LR. Brief symptom inventory: Administration, scoring, and procedures manual. 3.Minneapolis, MN: National Computer Systems, Inc; 1993.
Dishion TJ, Andrews DW. Preventing escalation in problem behaviors with high-risk young adolescents:Immediate and 1-year outcomes. Journal of Consulting and Clinical Psychology 1995;63:538–548.[PubMed: 7673531]
Dishion, TJ.; Andrews, DW.; Kavanagh, K.; Soberman, LH. Preventing childhood disorders, substanceabuse, and delinquency. In: Peters, RD.; McMahon, RJ., editors. Banff international behavioralscience serie. Vol. 3. Thousand Oaks, CA: Sage; 1996. p. 184-214.Preventive interventions for high-risk youth: The Adolescent Transitions Program
Downey G, Coyne J. Children of depressed parents: An integrative review. Psychological Bulletin1990;108:50–76. [PubMed: 2200073]
Egeland B, Kalkoske M, Gottesman N, Erickson MF. Preschool behavior problems: Stability and factorsaccounting for change. Journal of Child Psychology and Psychiatry 1990;31:891–909. [PubMed:2246340]
Essex MJ, Klein MH, Cho E, Kraemer HC. Exposure to maternal depression and marital conflict: Genderdifferences in children’s later mental health symptoms. Journal of American Academy of Child andAdolescent Psychiatry 2003;42:728–737.
Fan X, Thompson B, Wang L. The effects of sample size, estimation methods, and model specificationon SEM fit indices. Structural Equation Modeling: A Multidisciplinary Journal 1999;6:56–83.
Gartstein et al. Page 13
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Fendrich M, Warner V, Weissman MM. Family risk factors, parental depression, and psychopathologyin offspring. Development and Psychopathology 1990;8:40–50.
Fergusson DM, Lynskey MG, Horwood LJ. The effect of maternal depression on maternal ratings ofchild behavior. Journal of Abnormal Child Psychology 1993;21:245–267. [PubMed: 8335763]
Field T. Infants of depressed mothers. Development and Psychopathology 1992;4:49–66.Forehand R, Lautenschlager GJ, Faust J, Graziano WG. Parent perceptions and parent–child interactions
in clinic-referred children: A preliminary investigation of the effects of maternal depressive moods.Behavior Research and Therapy 1986;24:73–75.
Friedlander S, Weiss DS, Traylor J. Assessing the influence of maternal depression on the validity of theChild Behavior Checklist. Journal of Abnormal Child Psychology 1986;14:123–133. [PubMed:3950213]
Garber, J.; QuiggleNLPanak, W.; Dodge, KA. Aggression and depression in children: Comorbidity,specificity, and cognitive processing. In: Cicchetti, D.; Toth, S., editors. Internalizing andexternalizing expressions of dysfunction. Hillsdale, NJ: Erlbaum; 1991. p. 225-264.
Geller J, Johnston C. Depressed mood and child conduct problems: Relationships to mothers’ attributionsfor their own and their children’s experiences. Child and Family Behavior Therapy 1995;17:19–34.
Goodman S, Gotlib IH. Risk for psychopathology in the children of depressed mothers: A developmentalmodel for understanding mechanisms of transmission. Psychological Review 1999;106:458–490.[PubMed: 10467895]
Griest D, Wells KC, Forehand R. An examination of predictors of maternal perceptions of maladjustmentin clinic-referred children. Journal of Abnormal Psychology 1979;88:277–281. [PubMed: 500956]
Hammen, C. Depression runs in families: The social context of risk and resilience in children of depressedmothers. New York: Springer-Verlag; 1991.
Hankin BL, Abramson LY, Moffitt TE, Silva PA, McGee R, Angell KE. Development of depressionfrom preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinalstudy. Journal of Abnormal Psychology 1998;107:128–140. [PubMed: 9505045]
Hayward C, Sanborn K. Puberty and the emergence of gender differences in psychopathology. Journalof Adolescent Health 2002;30:49–58. [PubMed: 11943575]
Hops, H. Intergenerational transmission of depressive symptoms: Gender and developmentalconsiderations. In: Mundt, C.; Goldstein, MJ.; Hahlweg, K.; Fiedler, P., editors. Interpersonal factorsin the origin and course of affective disorders. London: Royal College of Psychiatrists; 1996. p.113-129.
Hops H, Biglan A, Sherman L, Arthur J, Friedman L, Osteen V. Home observations of family interactionsof depressed women. Journal of Consulting and Clinical Psychology 1987;55:341–346. [PubMed:3597946]
Johnston C, Short K. Depressive symptoms and perceptions of child behavior. Journal of Social andClinical Psychology 1993;12:164–181.
Krain AL, Kendall PC. The role of parental emotional distress in parent report of child anxiety. Journalof Clinical Child Psychology 2000;29:328–335. [PubMed: 10969417]
Lilienfeld SO. Comorbidity between and within childhood externalizing and internalizing disorders:Reflections and directions. Journal of Abnormal Child Psychology 2003;31:285–291. [PubMed:12774861]
Loehlin, JC. Latent variable models: An introduction to factor, path, and structural analysis. 3. Mahwah,NJ: Lawrence Erlbaum Associates; 1998.
McManus M, Alessi NE, Grapentine WL, Brickman AS. Psychiatric disturbance in serious delinquents.Journal of the American Academy of Child Psychiatry 1984;23(5):602–615. [PubMed: 6481034]
Myung IG. Tutorial on maximum likelihood estimation. Journal of Mathematical Psychology2003;47:90–100.
Nelson DR, Hammen C, Brennan PA, Ullman JB. The impact of maternal depression on adolescentadjustment: The role of expressed emotion. Journal of Consulting and Clinical Psychology 2003;71(5):935–944. [PubMed: 14516242]
Patterson GR. Mothers: The unacknowledged victims. Monographs of the Society for Research in ChildDevelopment 1980;45 Serial No. 186.
Gartstein et al. Page 14
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Pellegrini D. Depressed mothers’ judgments about their children: An examination of the depression–distortion hypothesis. Child Development 1989;60:1068–1075. [PubMed: 2805884]
Poulin F, Dishion TJ, Burraston B. 3-year iatrogenic effects associated with aggregating high-riskadolescents in preventive interventions. Applied Developmental Science 2001;5:214–224.
Radloff L. The CES–D scale: A self-report depression scale for research in the general population.Applied Psychological Measurement 1977;1:385–401.
Raykov, T.; Marcoulides, GA. A first course in structural equation modeling. Mahwah, NJ: LawrenceErlbaum Associates; 2000.
Rescorla L, Achenbach T, Ginzburg S, Ivanova MY, Ximenci LE, Almqvist A, et al. Consistency ofteacher-reported problems for students in 21 countries. School Psychology Review 2007a;36:91–110.
Rescorla L, Achenbach T, Ivanova MY, Dumenci L, Almquist F, Bilenberg N, et al. Behavioral andemotional problems reported by parents of children ages 6 to 16 in 31 societies. Journal of Emotionaland Behavioral Disorders 2007b;15:130–142.
Rice F, Harold GT, Thapar A. The link between depression in mothers and offspring: An extended twinanalysis. Behavior Genetics 2005;35:565–577. [PubMed: 16184485]
Richters J. Depressed mothers as informants about their children: A critical review of the evidence fordistortion. Psychological Bulletin 1992;112:485–499. [PubMed: 1438639]
Richters J, Pellegrini D. Depressed mothers’ judgment about their children: An examination ofdepression–distortion hypothesis. Child Development 1989;50:1068–1075. [PubMed: 2805884]
Rutter, M.; Izard, CE.; Read, PB., editors. Depression in young people: Clinical and developmentalperspectives. New York: Guilford Press; 1986.
Schaughency EA, Lahey BB. Mothers’ and fathers’ perceptions of child deviance: Roles of childbehavior, parental depression, and marital satisfaction. Journal of Consulting and ClinicalPsychology 1985;53:718–123. [PubMed: 4056189]
Stoolmiller M. Correcting estimates of shared environmental variance for range restriction in adoptionstudies using a truncated multivariate normal model. Behavior Genetics 1998;28:429–441. [PubMed:9926612]
Thomas AM, Forehand R, Neighbors B. Change in maternal depressive mood: Unique contributions toadolescent functioning over time. Adolescence 1995;30:43–52. [PubMed: 7625263]
Treutler CM, Epkins CC. Are discrepancies among child, mother, and father reports on children’sbehavior related to parents’ psychological symptoms and aspects of parent–child relationships?Journal of Abnormal Child Psychology 2003;31:13–27. [PubMed: 12597696]
Webster-Stratton C, Hammond M. Maternal depression and its relationship to life stress, perceptions ofchild behavior problems, parenting behaviors, and child conduct problems. Journal of AbnormalChild Psychology 1988;16:299–315. [PubMed: 3403812]
Weissman MM, Prusoff BA, Gammon GD, Merikangas KR, Leckman JF, Kidd KK. Psychopathologyin the children (ages 6–18) of depressed and normal parents. Journal of American Academy of ChildPsychiatry 1984;23:78–84.
Welsh–Allis G, Ye W. Psychopathology in children of parents with recurrent depression. Journal ofAbnormal Child Psychology 1988;16:17–28. [PubMed: 3361028]
Youngstrom EA, Findling RL, Calabrese JR. Who are the comorbid adolescents? Agreement betweenpsychiatric diagnosis, youth, parent, and teacher report. Journal of Abnormal Child Psychology2003;31:231–245. [PubMed: 12774858]
Gartstein et al. Page 15
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Figure 1.Depression–distortion Model 2: Daughter internalizing problems.
Gartstein et al. Page 16
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Figure 2.Depression–distortion Model 4: Daughter externalizing problems.
Gartstein et al. Page 17
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
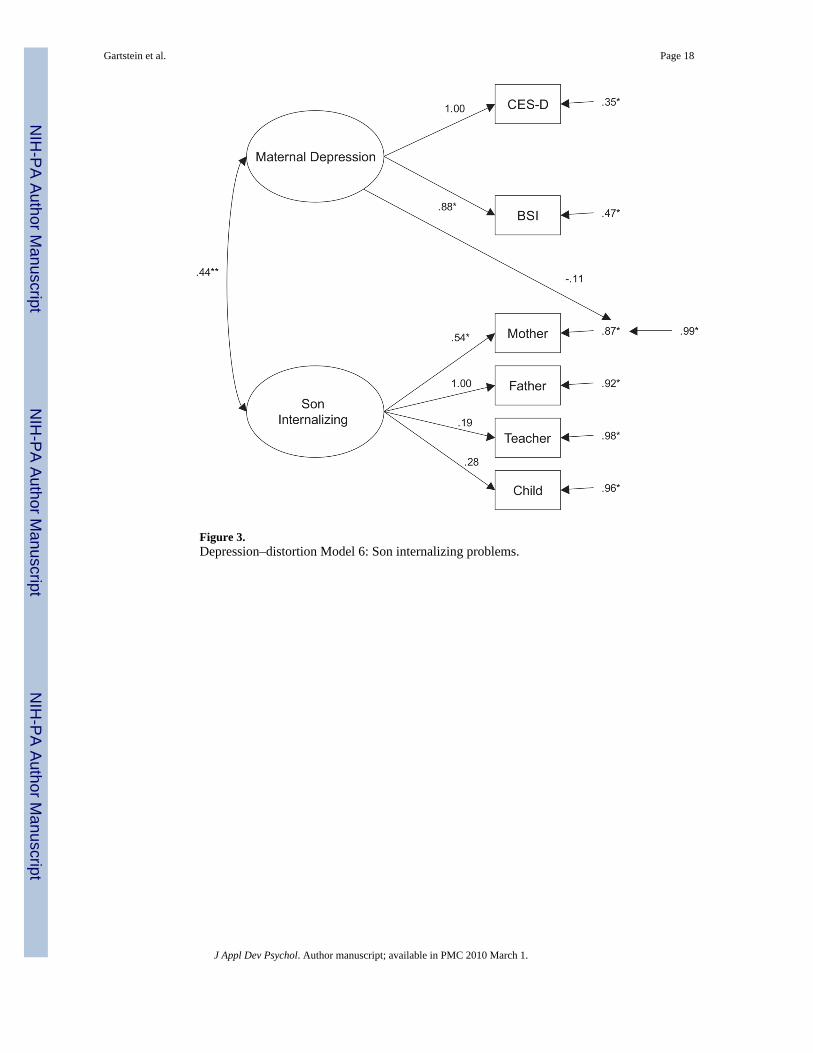
Figure 3.Depression–distortion Model 6: Son internalizing problems.
Gartstein et al. Page 18
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
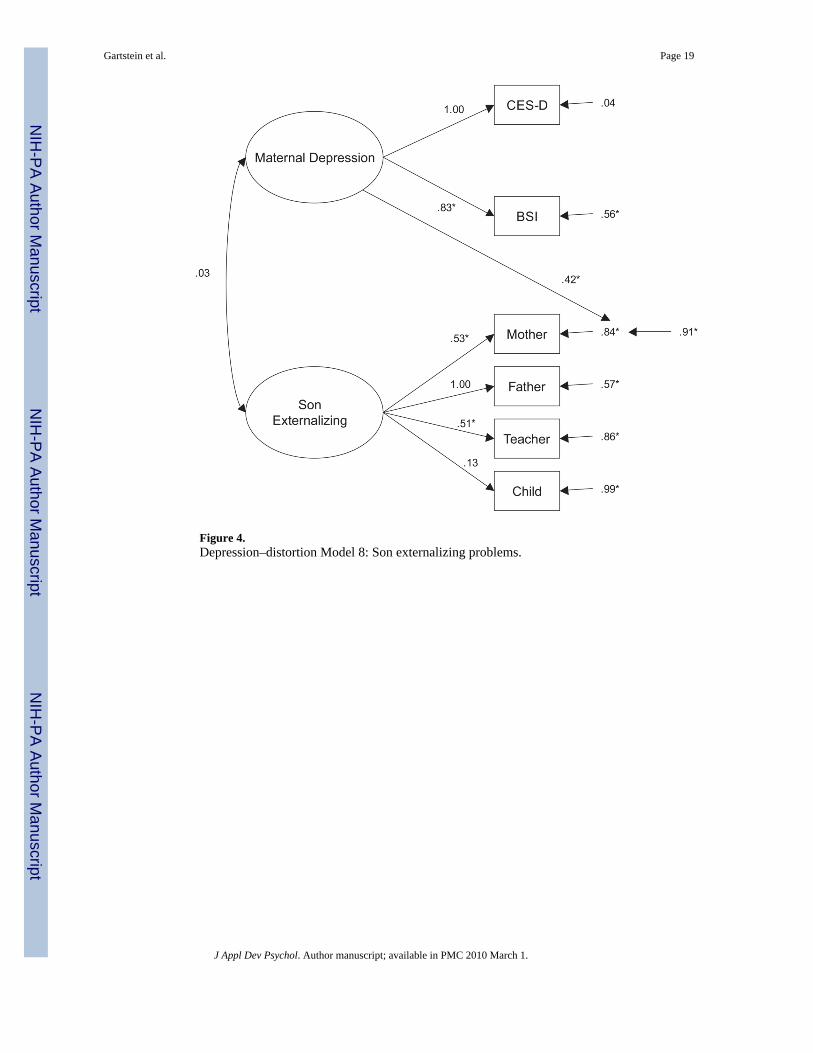
Figure 4.Depression–distortion Model 8: Son externalizing problems.
Gartstein et al. Page 19
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gartstein et al. Page 20
Tabl
e 1
Ass
ocia
tions
bet
wee
n M
ultii
nfor
man
t Rat
ings
of C
hild
Inte
rnal
izin
g an
d Ex
tern
aliz
ing
Diff
icul
ties
Info
rman
tM
othe
r E
XT
Fath
er E
XT
Tea
cher
EX
TC
hild
EX
TM
othe
r IN
TFa
ther
INT
Tea
cher
INT
Chi
ld IN
T
Mot
her E
XT
—.7
2**
.42*
*.1
3*.4
6**
.21*
*−.
01.0
7
Fath
er E
XT
—.4
2**
.08
.21*
.55*
*.1
7−.
06
Teac
her E
XT
—.0
9−.
01.1
3.4
6**
.01
Chi
ld E
XT
—.1
5*.0
9.1
1.5
9**
Mot
her I
NT
—.3
5**
.17*
.22*
*
Fath
er IN
T—
.24*
*.1
7
Teac
her I
NT
—.1
8**
Not
e. S
ampl
e si
zes v
arie
d ac
ross
ass
ocia
tions
(Ns =
219
, 123
, 218
, and
221
for m
othe
rs, f
athe
rs, t
each
ers,
and
child
ren,
resp
ectiv
ely)
, whi
ch is
refle
cted
in th
e p-
valu
es a
ssoc
iate
d w
ith e
ach
corr
elat
ion.
EX
T =
exte
rnal
izin
g; IN
T =
inte
rnal
izin
g.
* p <
.05;
**p
< .0
1
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Gartstein et al. Page 21
Tabl
e 2
Fit I
ndic
es A
ssoc
iate
d w
ith A
naly
ses o
f Con
verg
ent/D
iscr
imin
ant a
nd P
redi
ctiv
e V
alid
ity, a
nd D
epre
ssio
n–D
isto
rtion
Hyp
othe
sis
Ana
lyse
sM
odel
Chi
-squ
are
(df)
AG
FIA
ICIF
IC
FIR
MSE
A(9
0% c
onfid
ence
)
Dis
crim
inan
t val
idity
Sing
le fa
ctor
250.
84**
*(2
0).7
021
0.84
.60
.59
.23
(.20
to .2
5)
Sing
le fa
ctor
w/e
rror
57.1
2***
(16)
.89
25.1
1.9
4.9
4.1
1 (.0
8 to
.14)
Two
fact
or w
/err
or22
.61
(15)
.96
−7.7
4.9
9.9
9.0
5 (0
to .0
8)
Dep
ress
ion–
dist
ortio
n (d
augh
ters
)
Inte
rnal
izin
g M
odel
114
.06
(9)
.92
−3.9
5.9
7.9
7.0
7 (0
to .1
4)
Inte
rnal
izin
g M
odel
24.
63(7
).9
7−9
.37
1.02
1.00
0.00
(0 to
.08)
Exte
rnal
izin
g M
odel
312
.58
(9)
.93
−5.4
2.9
9.9
9.0
6 (0
to .1
3)
Exte
rnal
izin
g M
odel
411
.89
(8)
.93
−4.1
1.9
9.9
9.0
7 (0
to .1
4)
Dep
ress
ion–
dist
ortio
n(so
ns) Inte
rnal
izin
g M
odel
516
.50*
(9)
.93
0.50
.99
.99
.10
(.02
to .1
6)
Inte
rnal
izin
g M
odel
616
.45*
(8)
.93
0.45
.99
.99
.10
(.02
to .1
6)
Exte
rnal
izin
g M
odel
78.
19(8
).9
6−7
.81
1.01
1.00
.02
(0 to
.11)
Exte
rnal
izin
g M
odel
83.
39(7
).9
8−1
0.61
1.03
1.00
0.00
(0 to
.07)
* p <
.05;
**p
< .0
1;
*** p
< .0
01
J Appl Dev Psychol. Author manuscript; available in PMC 2010 March 1.
Related Documents