The oncologist’s point of view: the promise and challenges of increasing options for targeted therapies in NSCLC Egbert F. Smit Department of Thoracic Oncology, Netherlands Cancer Institute, and Department of Pulmonary Diseases, VUMC, Amsterdam, Netherlands

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The oncologist’s point of view: the promise and challenges of increasing options for targeted therapies in NSCLC Egbert F. Smit Department of Thoracic Oncology, Netherlands Cancer Institute, and Department of Pulmonary Diseases, VUMC, Amsterdam, Netherlands

Patient selection in lung cancer: evolution over time
ADC, adenocarcinoma; NSCLC, non-small-cell lung cancer; SCLC, small-cell lung cancer. Adapted from Reck M, et al. Lancet. 2013;382:709-19.
1990 Lung cancer
2000 NSCLC SCLC
ADC
ADC and treatable oncogenic alterations
Large cell carcinoma
SCLC
Squamous cell carcinoma

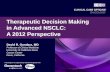
Patient selection in NSCLC: evolution over time
*Non-squamous = adenocarcinoma and large cell carcinoma NSCLC histology. CI, confidence interval; HR, hazard ratio; OS overall survival. Scagliotti GV, et al. J Clin Oncol. 2008;26:3543-51.
2008 Non-squamous cell carcinoma Squamous cell carcinoma
Median OS (months)
Pemetrexed + cisplatin 11.8 Gemcitabine + cisplatin 10.4
HR 0.81 (95% CI 0.70–0.94) p = 0.005
Survival time (months)
Prob
abili
ty o
f sur
viva
l
0 6 18 12 24 30
Non-squamous* (n = 1,000) Squamous (n = 473)
Median OS (months)
Pemetrexed + cisplatin 9.4 Gemcitabine + cisplatin 10.8
HR 1.23 (95% CI 1.00–1.51) p = 0.05
Survival time (months) Pr
obab
ility
of s
urvi
val
0 6 18 12 24 30
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
1.0

Timeline for the discovery of relevant alterations in lung cancer
ALK, anaplastic lymphoma kinase; BRAF, B-Raf proto-oncogene; DDR2, discoidin domain receptor 2; EGFR, epidermal growth factor receptor; FGFR1, fibroblast growth factor receptor 1; HER2, human epidermal growth factor receptor 2; KRAS, Kirsten rat sarcoma viral oncogene homologue; NGS, next-generation sequencing; NRAS, NRAS proto-oncogene; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase, catalytic subunit alpha; PTEN, phosphatase and tensin homolog; ROS1, ROS1 proto-oncogene receptor tyrosine kinase.
Adapted from Levy MA, et al. Genome Res. 2012;22:2101-8.
Before NGS NGS era
picking the right gene Difficulty: finding the relevant genes
1984 1997 1990 2002 2004 2005 2007 2008 2010 2012 2011
EGFR HER2
PIK3CA mutations
ALK ROS1
fusions NRAS
mutations
PTEN mutations
KRAS mutations
Lung ADC kinome
623 genes of lung ADC
BRAF mutations
Lung ADC copy numbers
Lung squamous ADC, SCLC exomes & genomes
First lung cancer
genomes
DDR2 mutations
FGFR1 amplifications

Frequencies in real life: French experience
WT, wild type. Barlesi F, et al. Lancet. 2016;387:1415-26.
EGFR 11%
KRAS 29%
BRAF 2%
HER2 1% PIK3CA
2% ALK 5%
Unknown 35%
Full WT 15%
Overall
EGFR 21%
KRAS 27%
BRAF 2%
HER2 1%
PIK3CA 3%
ALK 6%
Unknown 28%
Full WT 12%
Women
EGFR 12%
KRAS 31%
BRAF 2%
HER2 1% PIK3CA
2% ALK 5%
Unknown 32%
Full WT 15%
ADC
EGFR 44%
KRAS 9%
BRAF 3% HER2 4% PIK3CA 4%
ALK 14%
Unknown 13%
Full WT 9%
Never-smokers

Oncogene-driven NSCLC: tailored treatment
PFS, progression-free survival. 1. Adapted from: Rosell R, et al. Lancet Oncol. 2012;13:239-46.
2. Adapted from: Shaw AT, et al. N Engl J Med. 2013;368:2385-94.
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 0
0.2
0.4
0.6
0.8
1.0 Erlotinib (n = 86) Chemotherapy (n = 87)
10.4 5.1
PFS
prob
abili
ty
Time (months) Patients at risk
Erlotinib 86 69 62 43 33 25 19 14 8 7 6 4 3 2 1 0 Chemotherapy 87 52 21 8 5 3 2 1 0 0 0 0 0 0 0 0
Log-rank p < 0.0001
HR (95% CI) 0.3402 (0.2341–0.4944)
Erlotinib vs chemotherapy in EGFR-driven advanced NSCLC1
0
20
40
60
80
100
0 5 10 15 20 25
Number at risk Erlotinib 173 93 38 11 2 0
Chemotherapy 174 49 15 4 1 0
Crizotinib (n = 173)
Chemotheraphy (n = 174)
Events, n (%) 100 (58) 127 (73) Median, mo 7.7 3.0 HR (95% CI) 0.49 (0.37–0.64)
p < 0.001
Crizotinib vs chemotherapy in ALK+ NSCLC2
Time (months)
Prob
abili
ty o
f sur
viva
l w
ithou
t pro
gres
sion
(%)

Number at risk Patients with oncogenic driver No targeted therapy 318 205 110 64 43 20
Targeted therapy 260 225 143 72 36 23 Patients with no driver 360 250 122 59 36 23
Targeted therapy: improved survival, no cure
Kris MG, et al. JAMA. 2014;311:1998-2006.
Time (years)
Surv
ival
pro
babi
lity
1.0
0.8
0.6
0.4
0.2
0 0 1 3 2 5 4
Log-rank p < 0.001
No targeted therapy
No driver
Targeted therapy

Patient selection in lung cancer: evolution over time
Adapted from Reck M, et al. Lancet. 2013;382:709-19.
1990 Lung cancer
2000
Established targets Mutation negative/unknown 2015 EGFR ALK ROS1
ADC
ADC and treatable oncogenic alterations
Large cell carcinoma
Small-cell lung cancer
Squamous cell carcinoma
NSCLC SCLC

Unknown oncogenic
driver detected 31%
KRAS 25%
EGFR sensitizing
17%
ALK 7%
EGFR other 4% MET 3% > 1 mutation
3% HER2 2% ROS1 2% BRAF 2% RET 2% NTRK1 1%
PIK3CA 1% MEK1 1%
ADC: targets and therapy
FDA, US Food and Drug Administration; MEK1, mitogen-activated protein kinase 1; MET, mesenchymal-epidermal transition; NTRK1, neurotrophic tyrosine kinase receptor 1; RET, rearranged during transfection. Tsao AS, et al. J Thorac Oncol. 2016;11:613-38.
Only three of these targets have agents
through approval by
the FDA
Key 1 - Phase 1 2 - Phase 2 3 - Phase 3 4 - Approved
EGFR sensitizing • Gefitinib4
• Erlotinib4
• Afatinib4
• Osimertinib4
• Necitumumab4
• Rociletinib3
ALK • Crizotinib4
• Alectinib4
• Ceritinib4
• Lorlatinib2
• Brigatinib2
MET • Crizotinib2
• Cabozantinib2
HER2 • Trastuzumab emtansine2
• Afatinib2
• Dacomitinib2
ROS1 • Crizotinib4
• Cabozantinib2
• Ceritinib2
• Lorlatinib2
• DS-6051b1
BRAF • Vemurafenib2
• Dabrafenib2
RET • Cabozatinib2
• Alectinib2
• Apatinib2 • Vandetanib2
• Ponatinib2
• Lenvatinib2
NTRK1 • Entrectinib2
• LOXO-1012
• Cabozantinib2
• DS-6051b1
PIK3CA • LY30234142
• PQR 3091
MEK1 • Trametinib2
• Selumetinib3
• Cobimetinib1

Dabrafenib−trametinib in previously treated BRAF V600E patients
• One-half of responses (18/36) were ongoing at the time of data cutoff
CR, complete respose; NE, not evaluable; PD; progressive disease; PR, partial response; SD, stable disease.
Maximum change in target lesion by best investigator-assessed confirmed response
NE patients did not have a follow-up scan required for confirmation
−100
−80
−60
−40
−20
0
20
40
Max
imum
redu
ctio
n fr
om
base
line
mea
sure
men
t (%
)
Patients
Best confirmed response CR PR SD PD NE
ORR: 63% (95% CI 49–76)
Duration of response
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Patie
nts
DOR (months)
Number of previous systemic anticancer therapy regimens for metastatic disease
1 2–3
Investigator assessment n = 36
DOR, median (95% CI), months
9.0 (6.9–18.3)

cMET alterations in LUAC
• Polysomy – not sensitive to cMETi
• Amplification – sensitive to cMETi when highly amplified
• Mutation – exon 14 skipping mutations are highly sensitive to cMETi
cMETi, cMET inhibitor; LUAC, lung adenocarcinoma.

Tumour shrinkage seen with capmatinib treatment in intermediate and high MET cohorts
DCR, disease control rate; GCN, gene copy number. Schuler M, et al. Presented at ASCO 2016. Abstract 9067.
Best response n (%)
GCN < 4 (n = 17)
GCN ≥ 4 and < 6 (n = 12)
GCN ≥ 6 (n = 15)
CR 0 0 0 PR 0 2 (17) 7 (47) SD 8 (47) 3 (25) 5 (33) PD 5 (29) 3 (25) 2 (13) Unknown 4 (24) 4 (33) 1 (7) ORR 95% CI 0 2 (17)
2.1–48.4 7 (47)
21.3–73.4 DCR 95% CI
8 (47) 23.0–72.2
5 (42) 15.2–72.3
12 (80) 51.9–95.7
3+
3+
3+ 2+ 3+ 1+ 3+
3+ 0
cMET GCN < 4 n/N (%) = 11/17 (64.7%)
Bes
t % c
hang
e fr
om
base
line
−20
60 40 20 0
−40 −60 −80
−100
80 3+ 2+
3+
3+ 3+
3+ 3+
Bes
t % c
hang
e fr
om
base
line
cMET GCN ≥ 4 and < 6 n/N (%) = 7/12 (58.3%)
−20
60 40 20
0
−40 −60 −80
−100
80
3+ 3+
3+ 3+ 3+ 3+ 2+ 3+ 3+
2+ 3+ 3+
cMET GCN ≥ 6 n/N (%) = 12/15 (80.0%)
Bes
t % c
hang
e fr
om
base
line
−20
60 40 20
0
−40 −60 −80
−100
80

cMET exon 14 skipping mutations are sensitive to cMET inhibitors
TKI, tyrosine kinase inhibitor. Awad MM, et al. Presented at ASCO 2017. Abstract 8511.
0 12 24 36 48 60 0
0.2 0.4 0.6 0.8 1.0
0 12 24 36 48 60 0
0.2 0.4 0.6 0.8 1.0
OS from date of stage IV diagnosis
Time (months)
Time (months) O
S pr
obab
ility
O
S pr
obab
ility
Received a MET TKI
N = 27
Never received a MET TKI
N = 34
Median OS (95% CI) 8.1 months (5.3–NR)
Median OS (95% CI) 24.6 months (12.1–NR)

ROS1 rearrangement
cd74, cluster of differentiation antigen 74; FISH, fluorescent in-situ hybridization. Awad MM, et al. N Engl J Med 2013;368:2395-401.
FISH
Sequence of the CD74-ROS1 fusion transcript
Cytologic analysis of a pleural effusion

Crizotinib in ROS1-rearranged LUAC: results from a phase 1 extension cohort (n = 50)
DoR, duration of response. Shaw AT, et al. N Engl J Med. 2014;371:1963-71.
ORR: 72%
−100
−80
−60
−40
−20
0
20
40
60
80
100
Cha
nge
from
bas
elin
e (%
)
0 30 35 5 10 15 20 25 40
A M *
Time (months)
3 patients (6%) CR 33 patients (66%) PR 9 patients (18%) SD
PD SD PR CR
DoR

Ceritinib has activity in crizotinib-resistant ROS1-rearranged LUAC
Lim SM, et al. J Clin Oncol. 2017;35:2613-8.
Cha
nge
from
bas
elin
e in
sum
of
long
est t
umou
r dia
met
ers
(%) 100
80 60 40 20 0
−20 −40 −60 −80
−100
PD SD PR CR
0 3 6 9 12 15 18 21 24 24 33 30 0
0.2
0.4
0.6
0.8
1.0
Duration (months)
PFS
(pro
port
ion)
All Crizotinib-naive
PFS 9.3 months (95% CI 0–22) 19.3 months (95% CI 1–37)

Lorlatinib in ROS1 + NSCLC
Solomon BJ, et al. Presented at Proc ASCO 2016. Abstract 9009.
1 prior TKI No prior TKI Ongoing treatments
ROS + patients
0 10 20 30
−10 −20 −30 −40 −50 −60 −70 −80 −90
−100
Bes
t cha
nge
from
bas
elin
e (%
)

E768
A883 S891 M918
L790 Y791
• G533
• C609 • C611 • C618 • C620 • C630 • C634
RET rearrangements
Mulligan LM. Nat Rev Cancer. 2014;14:173-86.
• Real frequency unknown
• 1–2% of LUAC
• Responses observed • vandetanib • sorafenib • regorafenib • alectinib • cabozantinib
MEN2A FMTC
Y791
G691
V804
Mod
ifyin
g va
riant
s
FMTC MEN2B
FMTC
Papillary thyroid carcinoma
Lung adenocarcinoma
Chronic myelomonocytic leukaemia
FGFR1OP-RET
BCR-RET
KIF5B-RET
BCR
FGFR10P
KIF5B
RET-PTC1
713 CCDC6
RET-PTC3
101
NCOA4 238 713
713
426 713
713 375
575

Cabozantinib phase 2 in RET-rearranged LUAC
Drillon A, et al. Lancet Oncol. 2016;17:1653-60.
0 6 12 18 24 30 36 48 42 Time from start of treatment (months)
Number at risk (number censored) 25 (0) 15 (5) 7 (5) 6 (5) 6 (5) 6 (5) 4 (7) 1 (8) 0 (9)
0
20
40
60
100
80
OS
(%) 0
20
−100
− 80
40
− 20
− 40
− 60
Max
imum
redu
ctio
n fr
om
base
line
mea
sure
men
t (%
) PR SD
Best confirmed response

HER2 mutation and amplification are distinct molecular targets
CEP17, chromosome enumeration probe 17.
Li BT, et al. Presented at ASCO Annual meeting 2017. Abstract 8510.
Li BT, et al. J Thorac Oncol. 2016;11:414-9.
HER2 amplification Testing FISH
(HER2/CEP17 ≥ 2)
N = 175
5/175 = 3% (95% CI 1–7)
“Overlap” testing HER2 mutation and
HER2 amplifications
N = 145
0/175 = 0% (95% CI 0–3)
HER2 mutation Testing
Fragment analysis and mass spectrometry genotyping
(insertions, deletions, indels, recurrent point mutations
L755S, D769H, V777L, V777M)
N = 145
4/145 = 3% (95% CI 1–7)

TDM-1 in LUAC with HER2 ins mutations
Li BT, et al. Presented at ASCO Annual meeting 2017. J Thorac Oncol. 2016;11:414-9.
Adapted from: Arcila ME, et al. Clin Cancer Res. 2012;18:4910-8. Kris MG, et al. JAMA. 2014;311:1998-2006.Stephens P, et al. Nature. 2004;431:525-6.
2% of lung cancers Most common HER2 mutation
is insYVMA

1 0 12 11 10 9 8 7 6 5 4 3 2
TDM-1 in LUAC with HER2 ins mutations
RECIST, Response evaluation criteria in solid tumours.
Li BT, et al. Presented at ASCO Annual meeting 2017. J Thorac Oncol. 2016;11:414-9.
Median PFS: 4 months (95% CI 3.0 to NR, n = 18 with 13 events) Median DoR: 5 months (95% CI 3.0 to NR, n = 8 with 6 events)
PFS ORR by RECIST v1.1
ORR 44% (8/18; 95% CI 22–69), study met primary endpoint
0
75
−75
−50
−25
25
50
% B
est r
espo
nse
per R
ECIS
T v1
.1
Patients
HER2 mutant lung cancer responses
Confirmed PR SD/PD
Time since treatment start (months)
Prob
abili
ty o
f PFS
0
1.0
0.8
0.6
0.4
0.2
0 10 8 6 4 2
Time on treatment (months)
HER
2 m
utan
t pat
ient
s re
ceiv
ing
ado-
tras
tuzu
mab
em
tans
ine
1
1
2
3
3
3
4
4
4
4
4
5
5
6
6
8
9
11
Treatment ongoing Response Response and treatment ongoing

• Oncogene addiction – ~ 25% of ADC – almost no squamous cell carcinoma
• Oncogene expedience – most ADC – vast majority of squamous cell
carcinomas
How about squamous cell lung cancer?

Potential therapeutic targets in squamous NSCLC
Perez-Moreno P, et al. Clin Cancer Res. 2012;18:2443-51.
FGFR1 amplification 22%
DDR2 mutation 4%
PIK3CA amplification 33%
MET amplification 5%
MET mutation 1%
BRAF mutation 2%
Others
Unknown

FGFR1 amplifications in SCC of the lung: from discovery to clinical evaluation
SCC, squamous cell carcinoma; SQLC, squamous lung cancer.
1. Weiss J, et al. Sci Transl Med. 2010;2:62ra93. 2. Heucamp LC, et al. Sci Transl Med. 2012;4:141ra91. 3. Malchers F, et al. Cancer Discov. 2014;4:246-57.Nogova L, et al. Presented at ASCO 2014. Abstract 8034.
Chromosome 8p geography
FIM trial BGJ398 in FGFR1-ampl. SQLC
Genomic discovery1 Pre-clinical validation1 FISH diagnostics2
Clinical evaluation
Understanding response on the molecular level3
n = 153

BGJ398 has clinical activity at doses ≥ 100 mg/day
HNSCC, head and neck squamous cell carcinoma. Sequist L, et al. Presented at AACR 2014. Abstract CT326.
RR FGFR1 amplified lung: 16% (RR FGFR-altered bladder: 40%)
Bes
t % c
hang
e fr
om b
asel
ine
(sum
of l
onge
st d
iam
eter
s of
targ
et le
sion
s)
0
80 60 40 20
−20 − 40 − 60
Bladder Breast Lung Cholangiocarcinoma HNSCC Other

Conclusion
• Targeted therapies extend survival over conventional chemotherapy (with improved QoL) in NSCLC
• Identification of patients for targeted therapies is key
• This can only be done by proper sequencing techniques – no clinical factor predicts reliably
• Calls for close cooperation between pathologists and treating physicians

Thank you for your attention!

Thermo Fisher Scientific and its affiliates are not endorsing, recommending, or promoting any use or application of Thermo Fisher Scientific products presented by third parties during this seminar. Information and materials presented or provided by third parties are provided as-is and without warranty of any kind, including regarding intellectual property rights and reported results. Parties presenting images, text and material represent they have the rights to do so.
Related Documents