1 Department of Medicine Morbidity and Mortality Conference February 13, 2018 “54 year old female presents with shortness of breath and encephalopathy” Presenter: Burton Shen, MD Internal Medicine-Pediatrics Resident, PGY2 Prepared by Seth Clark, MD/MPH 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Department of Medicine
Morbidity and Mortality Conference
February 13, 2018
“54 year old female presents with shortness of breath
and encephalopathy”
Presenter:
Burton Shen, MDInternal Medicine-Pediatrics Resident, PGY2
Prepared by Seth Clark, MD/MPH
1

Panel Discussants
Joann Jannitto, RNClinical Manager Jane Brown 4N
Barbara George, CPHRM, CPPSLifespan Risk Management Coordinator
Mary Jane Pizza, MSW, LICSW, LCDPSubstance Abuse Coordinator
Alexander Chirkov, MDMedical Examiner
2
2

Disclosures
Our presenters have no financial interest in or
affiliation with any commercial supporter to
disclose.
3
3

4
Presents via friend in severe respiratory distress, stabilized in critical care
bay with supplemental O2 and able to provide following history.
Chief Complaint: Shortness of breath
History of Present Illness:
• 54 YOF with AIDS on HAART (VL undetectable) , HCV,
polysubstance use, and asthma presents to ED with 2 days of worsening
shortness of breath. Reports 2 weeks of generalized fatigue and dry
cough with progressive SOB that began the day prior and acutely
worsened 1 hour prior to arrival while at rest. Denies DOE, fevers,
chills, sputum production, chest pain, recent travel, prolonged
immobility, or sick contacts.
Case Presentation
4

5
Past Medical History:
•AIDS (CD4 count 616, VL
undetectable)
•HCV untreated (VL 7.4 million
IU/ml)
•Schizophrenia
•Anxiety
•Depression
•Substance use DO (crack cocaine)
•? Asthma
Past Surgical History: None
Allergies: None
Family History:
•CAD in father
History (Continued)
Medications:
•Atazanavir/Cobicistat – 300/150mg daily
•Emtricitabine / Tenofovir – 200/300mg daily
•Paliperidone palmitate – 156mg Qmonth
•Respiridone – 1mg daily
•Trazodone – 50mg HS
•Gabapentin – 100mg BID
•Trihexyphenidyl – 2mg BID
•Ventolin – 90mcg inhaler PRN
Social History:
•Current smoker, 40 pack year hx
•Denies active illicit drug use
•Remote hx IVDU, last reported 2004
•Hx crack cocaine use, last reported 2012
5

6
Physical ExaminationVital Signs: T 98.9 HR 144 BP 92/42 RR 33 O2 sat: 99% venti mask
General Medical Exam: Distressed, using accessory muscles for breathing.
HEENT: Normocephalic and atraumatic. Oropharynx is clear and moist. Airway patent. Conjunctivae and EOM are normal.
Cardiovascular: Regular rhythm and normal heart sounds. Tachycardia present.
Pulmonary/Chest: Tachypnea noted. She is in respiratory distress. She has decreased breath sounds and mild expiratory wheezes throughout all lung fields. Speaking in 3-4 word sentence. Frequent dry cough.
Abdominal: Soft. There is no tenderness.
Musculoskeletal: She exhibits no edema or tenderness. No obvious signs of injury or deformity.
Neurological: Lethargic, requiring frequent stimuli. Moves all four extremities.
Skin: Skin is warm and dry.
6

7
Laboratory Results
11.414.7
148 137 103
25
15
1.25187
44.3 3.4
VBG 7.30/60 Utox + Cocaine
Lactate 2.2 - Opiates
- Benzodiazepines
Trop 0.018
BNP 64.2 RPP + Rhino/Enterovirus
Urine toxicology testing was otherwise negative at this time.
Dr. Garland, from the audience, had seen the patient intermittently
in his outpatient office but noted that she kept her appointments
inconsistently and had not been seen in the office for a long period
of time
7

8
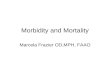
CXR
No acute cardiopulmonary process was observed on the admission chest x-ray
8

9
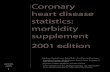
CTPE
Official Reading: No pulmonary embolism. Patchy tree and bud airspace opacities
bilaterally, likely infectious or inflammatory in etiology
9

10
Hospital Course
• Assessment: asthma exacerbation precipitated by URI
• Plan: admit for inpatient care of bronchospasm in light of respiratory distress
10

11
Hospital Course (HD 1-2)
• Remained somnolent in ED on BiPAP, intermittently attempting to leave AMA
• Treated with repeated doses of duonebs, IV steroids, 2L NS, and ativan
• Weaned off of BiPAP at 0600, remained tachycardic, admitted to the floor
• Arrived to the floor at 0730 and noted to be minimally responsive to sternal rub with significant wheeze, placed on non-rebreather
• No response to narcan
• ABG: 7.32/53/169 on 4L NRB
• Transferred to MICU
There was no clear reason for this patient’s somnolence upon admission. The patient
was initially triaged to the Medical ICU due to her dyspnea.
The patient had initial treatment for presumed asthma flare with solumedrol 125mg x2
doses, as well as bronchodilators for presumed asthma exacerbation
The patient had received Ativan which could have worsened hypoventilation, though not
enough to explain encephalopathy.
11

12
Hospital Course (HD 2)
• In MICU continued on IV steroids, albuterol nebs Q4H
• Family reports the patient occasionally smokes crack cocaine, unclear last use
• O2 weaned from BiPAP to 3.5L NC, family notes baseline mental status
• Remained in sinus tachycardia (HR 90-130)
• Treated as asthma exacerbation secondary to rhinovirus, tachycardia believed due to albuterol and anxiety
• Transferred back to medicine service
• Remains alert, asking to leave AMA, but redirectable
Ms. Jannitto (Clinical Manager on Jane Brown 4N) noted that when the floor nurses
receive word of a complex patient being transferred to their floor from the Ed or MICU,
they prepare by locating the patient near to the nursing station, observe for fall risk. On
occasion, patients are placed in the hallway for closer observation, particularly at night.
Dr. Fagan, from the audience, noted that the patient demonstrated a high degree of
acuity, including abnormal vital signs and a lack of explanation for her altered mental
status or respiratory illness. Were this his patient, he would prioritize the patient to be
seen early on rounds and often thereafter while an aggressive investigation was carried
out..
Dr. Bayliss noted that the patient had a negative troponin, normal BNP and an ECG
showing only sinus tachycardia, prompting a search for an alternative explanation of her
tachycardia. Note that thyroid studies were normal.
12

13
Hospital Course (HD 3)
• Stable overnight
• Remained in sinus tach to 130, on 3L NC
• 1700 – Patient signed out by primary team to crosscover as intermittently confused and does not have capacity to signoutagainst medical advice
• Also advised to hold benzodiazepines given encephalopathy
An audience member noted that the standard toxicology screen will not detect all drugs
of abuse , such as bath salts. Opiate withdrawal is also possible and there is often
fentanyl cut into cocaine.
Dr. Tammaro, from the audience, noted that her persistent and documented
encephalopathy would prompt him to consider other causes of altered mental status than
hypercarbia, including drug intoxication or withdrawal. Some of this work up had
already been done without identification of a cause.
Dr. Shen noted that the daytime team signed the patient out upon their departure to an
on-call intern who was also admitting patients. The patient’s resident would also sign the
patient over to a covering resident should the patient have active medical issues. While
this usually goes well, the handoff time is often very busy and followed by another
handoff later that evening to the overnight team.
Barbara George, from the Lifespan Risk Management office, noted that the patient’s
capacity for decision-making is best documented in the record.
13

14
Hospital Course (HD 3)
• 1520 – Patient alone with visitor for roughly 30 min
• Nursing notes increasing agitation following visit
• 1800 – Agitation continues to escalate, patient removing O2 and tele leads. Desatting to 70s without O2, HR 140s.
• Cross cover paged, attempted to redirect, placed on venti mask
• 1815 – Patient placed in non-violent restraints after continuing to remove O2 and tele leads, notes “security may be needed”.
• 1845 – Nursing paged cross cover for persistent agitation and HR in 160s.
• Team reviewed CT with radiology and confirmed no PE
• HR and agitation transiently improved with verbal engagement and reassurance
Ms. Jannitto noted that this patient, due to her behaviors, was under constant
observation. A nursing assistant from the unit was in the room as a constant observer but
would likely have had difficulty holding a mask on the patient or preventing her from
removing telemetry leads.
Mr. Scott Hemingway from RIH Security explained that the need for extra supervision
is real, but that clinical staff on the med/surg floors at times expect security to provide
an ongoing presence beyond their staffing and ability. Security staff are best equipped to
provide safety oversight regarding visitors but cannot offer physical restraint efforts for
patients on a prolonged basis.
Despite the constant observation in the room, the patient continued to remove telemetry
leads and oxygen mask, resulting in transient episodes of hypoxia.
14

15
Hospital Course (HD 3)
• 1920 – HR noted to be in 30s on tele, patient unresponsive, pulseless, code blue called
• PEA arrest ROSC with CPR + epi intubated (midazolam and morphine administered) PEA arrest, code called after 9 rounds CPR
15

16
Alexander Chirkov, MD –
Medical Examiner
The patient had elevated levels of cocaine in her blood – although this could reflect
cocaine ingested before or after hospitalization. The ME examination suggested that this
might be pre-hospital ingestion of cocaine. Acute ingestion can be detected in urine for
up to 70 hours. The autopsy did not suggest acute lung injury from inhaled cocaine use.
16

17
ME Report
17

18
ME Report
• Benzoylecgonine – cocaine degradation product
• Halflife – 6-10 hrs
• Average blood concentration in patients admitted to ED for cocaine related medical complaints – 1280 ng/mL
• Average blood concentration in cocaine related fatalities –7900 ng/mL (700-31,000 ng/mL)
18

19
Visitation Policy – Inpatient Adult
The working diagnosis for this patient was death from asthma exacerbation. The ME
exam raised issue of cocaine ingestion as potential cause or trigger of flare.
Dr. Garland noted that the patient had been seen in the clinic off and on for 15 year and
had sustained periods of sobriety from drug use.
Barbara George from Risk Management noted that HIPAA protects medical records for
50 years after death. The death certificate is a public document and so, even if a patient
expressed wishes that their condition not be shared with others, anyone in the public
could request this document after a patient expires. HIPAA also holds the clinicians
involved in the care of the patient to the privacy rules as long as the physician is aware
of the patient’s wishes.
19

20
Body and Belonging Search Policy
If contraband or harmful substances are suspected, patients can be searched. Clinicians
and nurses should confer and reach a consensus on whether or not there is sufficient
cause to initiate a search. Such discussion should be documented in the record and be
based on team discussions.
There are three levels of search: Room -> Body -> Body Cavity. When a search is
initiated, the patient is informed in a respectful manner first and then, after the patient
and any companions are escorted from the room, the search is carried out., even despite
patient protest.
Note that a hospital policy on caring for patients who are prescribed medical marijuana
is being drafted.
20

21
Body and Belonging Search Policy
Mr. Hemingway noted that hospitals with procedures for vetting and registering visitors
have decreased episodes of patient compromise by harmful ingestions in hospital.
21

22
Thank you!
22

23
Questions?
23
Related Documents