1 June 2016 INSIDE Earn 2 CE Credits Written for dentists, hygienists and assistants Integrated Media Solutions Inc./DentalLearning.net is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the pro- vider or to ADA CERP at www.ada.org/cerp. Integrated Media Solutions Inc./DentalLearning. net designates this activity for 2 continuing education credits. Approved PACE Program Provider FAGD/MAGD credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. 2/1/2016 to 1/31/2020. Provider ID# 346890 AGD Subject Codes: 690, 691, 697 Dental Learning, LLC is a Dental Board of California CE Provider. The California Provider # is RP5062. All of the information contained on this certificate is truthful and accurate. Completion of this course does not constitute authorization for the attendee to perform any services that he or she is not legally authorized to perform based on his or her license or permit type. This course meets the Dental Board of California’s requirements for 2 units of continuing education. CA course code is 02-5062-16004. Knowledge for Clinical Practice WWW.DENTALLEARNING.NET A PEER-REVIEWED PUBLICATION D ENTAL L EARNING Stuart J. Froum, DDS, Sang-Choon Cho, DDS, Peter Michael Loomer, BSc, DDS, PhD, MRCD, Aikaterini Georgantza, DDS, Takanori Suzuki, DDS, PhD, Yung Cheng Paul Yu, DDS The Use of in Dental Implant Education 3D Printing

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1June 2016
INSIDEEarn 2
CECredits
Written fordentists, hygienists
and assistants
Integrated Media Solutions Inc./DentalLearning.net is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the pro-vider or to ADA CERP at www.ada.org/cerp. Integrated Media Solutions Inc./DentalLearning.net designates this activity for 2 continuing education credits.
Approved PACE Program Provider FAGD/MAGD credit.Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement.2/1/2016 to 1/31/2020. Provider ID# 346890AGD Subject Codes: 690, 691, 697
Dental Learning, LLC is a Dental Board of California CE Provider. The California Provider # is RP5062. All of the information contained on this certi� cate is truthful and accurate. Completion of this course does not constitute authorization for the attendee to perform any services that he or she is not legally authorized to perform based on his or her license or permit type. This course meets the Dental Board of California’s requirements for 2 units of continuing education. CA course code is 02-5062-16004.
Knowledge for Clinical Practice
WWW.DENTALLEARNING.NET
A PEER-REVIEWED PUBLICATIONA PEER-REVIEWED PUBLICATION
DENTAL LEARNING
Stuart J. Froum, DDS, Sang-Choon Cho, DDS, Peter Michael Loomer, BSc, DDS, PhD, MRCD,
Aikaterini Georgantza, DDS, Takanori Suzuki, DDS, PhD, Yung Cheng Paul Yu, DDS
The Use of
in Dental Implant
Education
3D Printing

DENTAL LEARNING www.dentallearning.net
EDUCATIONAL OBJECTIVES
The overall objective of this article is to discuss the basic principles and applications of three-dimensional printing for educational use in implant dentistry, and to review the integration and experience of this technology in a 2-year post-graduate implant training program. After completing this article, the reader will be able to:
1. Review the history and use of 3D models and techniques to create these;
2. List and describe advantages of 3D versus 2D models in implant dentistry;
3. Describe the use of 3D models for implant treatment planning and pre-operative practice; and,
4. Review the results of the student survey and implications for dental education.
Rapid prototyping techniques for complex three-dimensional model fabrication were introduced more than a decade ago; however they were not widely applied in the fi eld of dentistry because of their prohibitive cost. A survey to evaluate the use of three-dimensional models was completed by the 12 post-graduate students in the Department of Periodontology and Implant Dentistry at New York University College of Dentistry implant program. It was concluded that all aspects of implant training were improved using three-dimensional models. These models can be accurately and rapidly produced, based on Cone Beam Computed Tomography datasets and with the help of various rapid prototyping techniques. Using these models in implant dentistry training appears to be highly benefi cial for demonstrating complex anatomical situations, instructing students and treatment planning. Based on these fi ndings and the students’ experiences it is recommended that educators use these models in periodontal and prosthetic training in specialty programs as well as for undergraduate teaching.
ABSTRACT
ABOUT THE AUTHORS
The Use of 3D Printing in Dental Implant Education
EditorFIONA M. COLLINS
Creative DirectorMICHAEL HUBERT
Art DirectorMICHAEL MOLFETTO
Copyright 2016 by Dental Learning, LLC. No part of this publication may be reproduced or transmitted in any form without prewritten permission from the publisher.
500 Craig Road, Floor One, Manalapan, NJ 07726
DENTAL LEARNING
SPONSOR/PROVIDER: This is a Dental Learning, LLC continuing education activity. DESIGNATION STATEMENTS: Dental Learning, LLC is an ADA CERP recognized provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Den-tal Learning, LLC designates this activity for 2 CE credits. Dental Learning, LLC is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 2/1/2016 - 1/31/2020. Provider ID: # 346890. EDUCATIONAL METHODS: This course is a self-instructional journal and web activity. Information shared in this course is based on current information and evidence. REGISTRATION: The cost of this CE course is $29.00 for 2 CE credits. PUBLICATION DATE: June 2016. EXPIRATION DATE: May 2019. REQUIREMENTS FOR SUCCESSFUL COMPLETION: To obtain 2 CE credits for this educational activity, participants must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%. AUTHENTICITY STATEMENT: The images in this course have not been altered. SCIENTIFIC INTEGRITY STATEMENT: Information shared in this continuing education activity is developed from clinical research and represents the most current information available from evidence-based dentistry. KNOWN BENEFITS AND LIMITATIONS: Information in this continuing education activity is derived from data and information obtained from the reference section. EDUCATIONAL DISCLAIMER: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the fi eld related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. PROVIDER DISCLOSURE: Dental Learn-ing does not have a leadership position or a commercial interest in any products that are mentioned in this article. No manufacturer or third party has had any input into the development of course content. CE PLANNER DISCLOSURE: The planner of this course, Joseph Riley, does not have a leadership or commercial interest in any products or services discussed in this educational activity. He can be reached at [email protected]. TARGET AUDIENCE: This course was written for dentists, dental hygienists, and assistants, from novice to skilled. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfi ed with this course can request a full refund by contacting Dental Learning, LLC, in writing. Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. Go Green, Go Online to www.dentallearning.net take your course.
Stuart J. Froum, DDS is a Diplomate of the Ameri-
can Board of Periodontology. He earned his dental
doctorate from New York University College of
Dentistry after graduating with a BA from Brook-
lyn College. Dr. Froum then completed a general
dentistry internship at Brooklyn Veterans Administration Hospital
and a periodontal residency at New York Veterans Administration
Hospital and New York University Dental Center.
Currently, Dr. Froum is a Clinical Professor and Director of
Clinical Research in the Department of Periodontics and Implant
Dentistry at New York University Dental Center. He is also a
Diplomate of the International College of Implantology.
Dr. Froum is the past President of the American Academy of
Periodontology (2013-2014), past President of the Northeastern
Society of Periodontics (1995-1996) and sits on the editorial review
boards of Middle East Journal of Oral and Maxillofacial Surgery,
the International Journal of Periodontics and Implant Dentistry and
Journal of Periodontology. He is the recipient of The 2016 AAP
Master Clinician Award. He also received the AAP Gies Award and
the NESP Hirschfeld Award. Dr. Froum is the Editor and an Author

The Use of 3D Printing in Dental Implant Education
3June 2016
of Implant Complications Etiology, Prevention and Treatment
(Published: 2010 Wiley-Blackwell) and Dental Implant Complica-
tions Etiology, Prevention and Treatment 2nd Edition (Published:
2016 Wiley-Blackwell). He also Co-authored the Second Edition:
of Comprehensive Periodontics for the Dental Hygienist By Mea A.
Weinberg, DMD, MSD, RPh, Cheryl Westphal, RDH, MS, Milton
Palat, DDS, JD, Stuart J. Froum, DDS and Robert Schoor, DDS. He
contributed chapters to The Sinus Bone Graft 2nd edition edited
by Ole T. Jensen, DDS, MS and Carranza’s Clinical Periodontology
12th Edition, by Michael G. Newman, DDS, Henry Takei, DDS, MS,
Perry R. Klokkevold, DDS, MS and Fermin A. Carranza.
Sang-Choon Cho, DDS is a Clinical Assistant Professor and Direc-
tor of the Advanced Program for International Dentists in Implant
Dentistry and Co-director of Clinical Research in the Department
of Periodontology and Implant Dentistry at New York University
College of Dentistry. He currently holds a position as an ICOI
Ambassador and recognized as a Diplomate of ICOI. Dr. Cho
graduated from the College of Dentistry at Kyungpook National
University, Korea, and received his Bachelors of Dental Science in
1984. Dr. Cho continued his clinical practice in South Korea, until
coming to the United States in 1995 to further his studies. He then
received an Advanced Implantology Certificate from the New York
University, where he has been teaching hands-on implant surgery and
restorative courses since 1997. In 2003, Dr. Cho received his Doctorate
in Dental Surgery, from New York University.
Dr. Cho is part of the Editorial Board for Journal of Periodontal and
Implant Science; he is a Member of the Academy of Osseointegration
(AO), Greater New York Academy of Prosthodontics (GNYAP)
and OKU. He is a Chairman of the Implant Dentistry Research
& Education Foundation Scientific Advisory Board. He received
the Outstanding Teacher Award in 2013. Dr. Cho has published
over 30 articles in peer review journals and wrote chapters in four
textbooks. He delivers timely scientific presentations and continu-
ally publishes articles in prestigious dental journal. In addition
to teaching and lecturing, Dr. Cho maintains a private practice in
New York City, specializing in Implantology and Dental Aesthetics.
Peter Michael Loomer, BSc, DDS, PhD, MRCD is the Chairman and
Clinical Professor of the Department of Periodontology and Implant
Dentistry at New York University College of Dentistry (NYUCD)
and the Director of Oral Health for Global Health Sciences, NYU
College of Global Public Health. He is a graduate of the University of
Toronto, where he obtained all of his academic and clinical specialty
training. He is a Diplomate of the American Board of Periodontol-
ogy, member of the Royal College of Dentists of Canada and a
Fellow of the New York Academy of Medicine and the OKU Dental
Honors Society. He serves as Associate Editor for the Journal Biomed
Central Oral Health, and as a reviewer for many other peer-reviewed
journals. Over the last 25 years, Professor Loomer has studied bone
and microbial aspects of periodontal diseases. His research has a
strong focus on global oral health, concentrating on improving oral
health of underserved populations in Africa and India. Professor
Loomer is the recipient of the Medical Research Council of Canada
Medical Sciences Fellowship, the AAP Young Investigator Fellowship
Award, Oral-B Dr. Robert Hutson Award for Dental Education, AAP
Outstanding Educator Award, Pierre Fauchard Society Faculty Award,
and New York Academy of Medicine Fellowship.
Aikaterini Georgantza, DDS obtained her dental degree from the
Aristotle University of Thessaloniki School of Dentistry in 2007.
She graduated from the Advanced Program in Implant Dentistry
for International Dentists at NYU in 2015. She is currently a resi-
dent of the Periodontology Post Graduate Program at NYUCD.
Takanori Suzuki, DDS, PhD graduated from the Nippon Dental
University College of Life Dentistry in Tokyo, Japan. He received
his DDS degree there in 2000, a doctorate of operative dentistry
in 2004, and then worked in the department of operative den-
tistry as an assistant professor from 2004 to 2008. He completed
a one-year Advanced Program for International Dentists in Com-
prehensive Dentistry at NYUCD in 2009, the two-year Advanced
Program for International Dentists in Implant dentistry in 2011
and a clinical fellowship in Implant dentistry in 2012. He is cur-
rently a Clinical Assistant Professor in the Ashman Department
of Periodontology and Implant Dentistry at NYUCD.
Yung Cheng Paul Yu, DDS graduated from Dental School in 1997 at
Universita’ Sapienza in Rome, before training in Advanced Orth-
odontic and Gnatology at Ospedale Nuovo Regina Margherita in
Rome and later completing his Advanced Implant Dentistry training
at NYU. Dr. Yu lectures nationally and internationally and has
published in several peer reviewed journals. Dr. Yu is currently a full
time faculty member in the Ashman Department of Periodontology
and Implant Dentistry at NYUCD.

DENTAL LEARNING www.dentallearning.net
4
Introduction
Numerous clinical reports have demonstrated the benefits of digital technology in the diagnosis, treatment and fabrication of implant-supported
dental prostheses.1,2 Digital diagnostic impressions, virtual planning, computer-guided implant surgery and custom abutments, fabricated using Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM), can be used to plan and complete implant placement and implant- supported dental prostheses.3,4
Recent advances in computed tomography (CT) technol-ogy have improved visualization of bone morphology when compared to standard two-dimensional (2D) radiographs.5,6 Use of this planning software has the potential to increase the predictability of implant treatment while avoiding
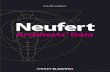
unwanted complications.7 Techniques have also been developed using new software and hardware to accurately represent data in three-dimensional (3D) format on a 2D screen. Given the visualization provided by sophisticated software packages, the fabrication of physical models may seem unnecessary; however, the display of 3D morphology on a 2D screen does not provide the surgeon with a complete representation of the patient’s anatomy (Fig. 1). Using 2D visualization, surgeons must learn to interpret the informa-tion in order to mentally reconstruct the 3D geometry. The utilization of 3D physical models is a significant advance-ment, whereby 3D information is seen in an accurate dupli-cation of the patient’s anatomy (Fig. 2).
Rapid prototyping (RP) refers to the fabrication of 3D physical models directly from a CAD model.8 3D printing was introduced more than a decade ago, but was not widely ap-plied in the field of dentistry at the time as early 3D printers were highly complex and expensive, suitable only for the larg-est manufacturers that could afford to pay several hundred thousand dollars for them.9,10 However, a series of advances, and cost reduction, has enabled the use of 3D printing in mainstream dentistry. Moreover, by providing visual and tac-tile information and documentation of the patient’s anatomy, 3D printing has enormous potential in changing the overall
4June 2016
Figure 1. CBCT view of the right maxillary site and simulation of implant placement
Figure 2. Translation of the CBCT data to a 3D printed model of the patient and implant site in Figure 1 with simulated sinus augmentation and implant placement

The Use of 3D Printing in Dental Implant Education
5June 2016
process of teaching, treatment planning, and successful place-ment and restoration in implant dentistry. Computer-directed RP techniques in dental education have begun to become more available. To date, however, there are few publications regarding the various uses of 3D models in combination with traditional training methods in the fields of restorative den-tistry and oral and maxillofacial surgery.11-14
Experience with the use of 3D Printed Models in the New York University College of Dentistry (NYUCD) Implant Program
Since 2012, 3D printed models have been successfully integrated and used in educating and training students in the International Implantology Program at NYUCD.
RP technologies and 3D model fabrication in dentistryA physical model was manufactured using data from
Cone Beam Computed Tomography (CBCT) and Mag-netic Resonance Imaging (MRI).15-17 Methods employed to fabricate a physical prototype fall into two categories: subtractive and additive. The subtractive technique employs conventional numerically controlled (NC) machining, gener-ally milling, and the shape of the model is created from a block of polyurethane or other foam. However, this method has limitations – complex geometries are difficult to program, and reproduction of anatomical undercuts is almost impos-sible. In addition, the quality of milled models is limited because polyurethane foam is brittle, soft, cannot be steril-ized, and significant excess material waste is generated. On the other hand, RP models are created by the additive technique and can include undercuts, voids and complex internal geometries such as neurovascular canals and sinuses. These models can also be translucent, allowing the internal anatomy to be easily seen. Therefore, additive methods are advantageous in fabricating physical models with anatomical details. In addition they are cost-effective, as the materials used are in powder or liquid forms, and then hardened by external power sources before being layered into the final model. The most common additive technologies in dentistry are Selective Laser Sintering, Fused Deposition Modeling,
Multi-Jet Modeling and Stereolithography.8
Prior to 3D printing, highly complex data had to be pre-processed to provide a format that a RP system could recog-nize. The current process for data utilization is divided into the following steps: 1. Data acquisition; 2. Image processing; and, 3. Model fabrication. The digital imaging and communications in medicine (DICOM)-based CBCT data can now quickly be exported into the standard tessellation language format used in RP.11 This has greatly facilitated the printing of 3D models derived from radiographic images. As part of the workflow fol-lowing acquisition of CBCT scan data, CT slices are created as 2D layers during the printing process and these layers are then assembled into a solid mass. The result is the easy production of CBCT data-based, tactile models for educational purposes. The 3D models serve as identical physical representations of the patient's oral anatomy derived from CT data sets. By accurately simulating the hard tissue, they provide both visual and tactile information and documentation for visualization, diagnostic, therapeutic and educational purposes.
Use of 3D Models in Dental Implant EducationThe use of 3D models (Formlab Inc., Somerville, MA)
in the NYUCD dental implant education program can be divided into 4 major areas: 1. Patient education and informed consent; 2. Student visualization of anatomical structures related to implant dentistry; 3. Treatment planning and pre-operative practic-ing; and, 4. Evaluation of prosthetic options using provi-sionals created to simulate the final prostheses.
1. Patient education and informed consent3D models help patients understand the treatment plan
prior to signing an informed consent form and allow them to feel more comfortable about the proposed treatment. For many patients, observing the procedure on a 3D model decreases fear of the unknown and allows them to “see” the procedure in a non-threatening way (Figs. 3,4).
2. Dental implant education to teach anatomical structuresUnlike traditional models (Fig. 5), 3D models can replicate

DENTAL LEARNING www.dentallearning.net
6
the exact maxillary and mandibular anatomy, which allows the student to view the external and internal structures that will be encountered during surgical intervention, thereby aiding treat-ment planning (Fig. 2, page 3). The most common maxillary anatomical landmarks that are significant in implant dentistry are: the sinus floor and sinus anatomy including the septa, the posterior superior alveolar artery, the greater palatine foramen and the incisive canal (IC). In the mandible, they are: the pathway of the inferior alveolar nerve (IAN) and the mental foramen.
For both the maxilla and mandible, visualization of the residual ridge width and height is also of great importance, and provides a method for measurement and implant planning.
3. Utilizing 3D models for treatment planning and pre-operative practice
3D models have been used to assist students in develop-ing a pre-surgical treatment plan for routine and complex procedures, including selection of the surgical technique and materials, and simulation of the planned surgical procedure.12 The benefits of planning and practicing implant procedures on these models with the implant faculty instructors are numerous (Fig. 5):• Students encounter the exact bone anatomy that they will
find under the soft tissue at the time of the actual surgery and can rehearse the procedure, correct any errors during the rehearsal, and become familiar with the proper tech-nique (Figs. 6,7, page 6).
• If simultaneous bone augmentation will be required at the time of implant placement, the student can be prepared with the materials and techniques needed. The actual sur-gical procedure may then require less time, with accuracy improved and the student becoming more confident. Figure 3. 3D printed radiographic and surgical
template for sinus augmentation procedure rep-resenting the patient’s actual maxillary anatomy
Figure 4. 3D model used for patient education and informed consent
Figure 5. Conventional prefabricated model for implant education – the model does not dupli-cate actual patient anatomy

The Use of 3D Printing in Dental Implant Education
7June 2016
• Improved communication and trust, not only between the student and the Faculty/Instructor but also between the student and patient.
• Accurate selection of the required materials, e.g., in the case of ridge augmentation, using a 3D model, enables the student and faculty to visualize the defect, measure it and consequently select the appropriate materials. The type of implant and material can be accurately selected, and in some cases membrane barriers can be specifically contoured, prior to surgery.
• Lastly, second-year students are able to practice advanced and more complex procedures hands-on with 3D models, e.g., immediate implant placement and immediate pro-visionalization, implant placement lateral to the IAN, ridge split techniques and sinus augmentation procedures
Figure 6. 3D model used for surgical simulation prior to actual surgery
Figure 7. Implant placed on 3D model according to ideal mesio-distal and bucco-lingual dimensions with resulting fenestration, lateral and occlusal view. Surgical “practice” increases successful placement during the actual surgery and demonstrates implant position placement changes to avoid fenestration
Figure 8. Modified implant position with no resulting fenestration

DENTAL LEARNING www.dentallearning.net
8
with or without simultaneous implant placement. This planning is aided by individually prefabricated 3D guides that allow accurate window design on the models and are then used on the patient, thereby increasing accuracy while reducing surgical time (Fig. 8). The innovative application of 3D technology has helped
in optimizing treatment outcomes, and in reducing operating time and intra-operative complications.10
4. Utilizing 3D models for prostheses and for implant maintenance education
RP techniques are becoming more attractive in dental prosthodontics and can be used to design, develop and man-ufacture dental prostheses such as provisional restorations, copings, crowns, and fixed partial dentures.18,19 Prosthetic applications can be reviewed using 3D models, with par-ticular focus on fabrication of the wax pattern of the actual
prostheses, surgical templates, custom trays, bite registration jigs, provisional restorations and night guards (Fig. 5, page 5). Data is acquired using 3D scanning devices and CAD for the prosthesis. Unlike with traditional methods, dental prostheses can now be fabricated layer by layer directly from a computer model, without part-specific tooling or human intervention. Labor costs are substantially reduced and better dental restorations can be delivered in less time. In addition, the models can be used to demonstrate maintenance of the implant-restoration complex to patients.
To evaluate experiences and opinions regarding the use of 3D models in their training, a 12-question visual analog scale (VAS) survey with a scale from 1 to 10 (1: of little help, 10: very helpful) was completed anonymously by each first- and second-year post-graduate student (n=12). These two classes of students had been exposed to the 3D printing models to a different extent. First-year students had limited or no experi-
TABLE 1. Survey questions asked regarding 3D printing models
Item Question: The use of 3D printing models improved the following procedures or understanding.
1 Rapport with the patient
2 Obtaining informed consent from the patient regarding their treatment plan
3 Treatment planning skills
4 Knowledge of the patient’s anatomy
5 Ordering of materials
6 Understanding the surgical procedure
7 Practicing the surgical procedure and becoming more proficient with the 3D models
8 Decreased time of the surgery
9 Smoother post-op course
10 Planning and placing of provisional restorations with the use of 3D models
11 Planning of auxiliary restorations with the use of 3D models
12 Planning and final production of the implant supported restoration with the use of 3D models
Note: Results were quantified on a scale of 1 to 10.

The Use of 3D Printing in Dental Implant Education
9June 2016
ence restoring implant-supported prostheses in general and with the help of 3D models in particular. Therefore, only the students who had experience with the 3D models in plan-ning and placing provisional, auxiliary and final restorations were asked to answer questions 10,11 and 12 in the survey. Survey questions are shown in Table 1.
ResultsIn the students’ opinion, all aspects of implant training –
from planning to knowledge of the patient’s surgical anat-omy to production of the provisional and final restorations – were improved using 3D models. Patient understanding of the procedures, and confidence in giving informed consent, were also improved as evidenced by ratings in the 8-9 range. The areas rated as providing the least improvement were “decreased time of the procedure” and “smooth post-operative course,” although improvements were still reported (scores >7.0) (Table 2).
DiscussionRP technologies were originally developed in the 1980s
to build a prototype of a new product based on a computed file, and have been a very valuable method over the last decade. This technique is widely used in product design in other industries, especially in the automobile industry and in engineering.8 The successful use of RP technology for clinical applications in dentistry has been documented in the literature.12,13 In addition, as CT slice thickness is reduced, 3D model resolution will continue to improve. For a single model the printing process takes up to 1-2 hours depending on the layer thickness used. The benefit of this process is that one group of 20 mandibles can be finished in 5-10 hours. With the help of various RP techniques, 3D model fabrica-tion can be completed accurately and rapidly.
RP techniques are now regarded as a promising option for dental prosthesis production and have been a valuable addition to implant training at NYUCD. However, few studies have addressed its use as a teaching resource and none for dental implant education. With reference to the dental literature, this is the first time applications of 3D printing have specifically been used for educational and didactic purposes in implant dentistry.
The use of 3D models in the education of implant den-tistry appears to be highly beneficial to demonstrate com-plex anatomical situations, for instructing students and for treatment planning. The survey results demonstrated that students believe that 3D models improved the educational experience in treatment planning, patient anatomy, practice in implant placement as well as the fabrication of provisional and final implant-supported restorations. Based on these findings, it would follow that educators can use 3D models in periodontal and prosthetic training in various specialty programs and undergraduate teaching. Surgical education with models, using data from cone beam computed tomog-raphy (CBCT) patients, provides a method of teaching and has a long tradition in conservative operative dentistry.
In conclusion, generating 3D models based on CBCT datasets has promising potential for implant education, for understanding, planning and surgical practice. Mass
TABLE 2. Survey results from students
Item Number of students Average score
1 n=12 8.5
2 n=12 8.2
3 n=12 9.1
4 n=12 8.9
5 n=12 8.2
6 n=12 8.7
7 n=12 8.9
8 n=12 7.8
9 n=12 7.2
10 n=8 9.0
11 n=6 8.4
12 n=11 8.8

DENTAL LEARNING www.dentallearning.net
10
production of these models also makes it feasible to use 3D models in all implant-training programs. Further teaching options and uses of the 3D printer may be revealed in the future, and their applicability in various education settings remains to be determined in future studies.
References1. Stapleton BM, Lin WS, Ntounis A, Harris BT, Morton D. Ap-plication of digital diagnostic impression, virtual planning, and computer-guided implant surgery for a CAD/CAM – fabricated, implant supported fixed dental prosthesis: A clinical report. J Prosthet Dent 2014;112(3):402-8.2. Cassett M, Di Mambro A, Giansanti M, Stefanelli LV, Cavallini C. The intrinsic error of a stereolithographic surgical template in implant guided surgery. Int J Oral Maxillofac Surg 2013;42: 264–75. 3. Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: A systemat-ic review. Int J Oral Maxillofacial Implants 2014;29(Suppl):25-42.4. Kapos T, Evans C. CAD/CAM technology for implant abut-ments, crowns, superstructures. Int J Oral Maxillofacial Implants 2014;29(Suppl):117-36.5. Cavalcanti M. Cone beam computed tomographic imaging: Perspective, challenges, and the impact of near-trend future applications. J Craniofac Surg 2012;23:279-82.6. Benjamin LS. The evolution of multiplanar diagnostic imag-ing: predictable transfer of preoperative analysis to the surgical site. J Oral Implantol 2002;28(3):135-44.7. Orentlicher G, Goldsmith D, Horowitz A. Applications of 3- dimensional virtual computerized tomography technology in oral and maxillofacial surgery: current therapy. J Oral Maxillofac Surg 2010;68:1933-59.8. Liu Q, Leu M, Schmitt S. Rapid prototyping in dentistry: tech-nology and application. Int J Adv Manuf Technol 2006;29: 317-35.9. The History of 3D Printing: redOrbit Press – A publication of Science Matters Media LLC.10. Cohen A, Laviv A, Berman P, Nashef R, Abu-Tair J. Mandibu-lar reconstruction using stereolithographic 3-dimensional print-ing modeling technology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:661-6.11. Esses S, Berman P, Bloom A, Sosna J. Clinical applications of physical 3D models derived from MDCT data and created by rapid prototyping. AJR Am J Roentgenol 2011;196(6):W683-8.12. Lambrecht JTH, Berndt DC, Christensen AM, Zehender M. Haptic model fabrication for undergraduate and postgraduate teaching. Int J Oral Maxillofac Surg 2010;39:1226-9.
13. Soares PV, de Almeida Milito G, Pereira FA, Reis BR, Soares CJ, de Sousa Menezes M, de Freitas Santos-Filho PC.. Rapid prototyping and 3D-Virtual models for operative dentistry edu-cation in Brazil. J Dent Educ 2013;77(3):358-63.14. Chan DCN, Frazier KB, Tse L, Rosen D. Application of rapid prototyping to operative dentistry curriculum. J Dent Educ 2004;68(1):64-70.15. Lambrecht JTH, Berndt DC, Schumacher R, Zehender M. Generation of three-dimensional prototype models based on cone beam computed tomography. Int J CARS 2009;4:175-80.16. Kaeppler G. Applications of cone beam computed to-mography in dental and oral medicine. Int J Comput Dent 2010;13:203-19.17. Petzold R, Zeilhofer HF, Kalender WA. Rapid prototyping technology in medicine-basics and applications. Comp Med Imag Graphics 1999;23:277-84.18. Sun J, Zhang F. The application of rapid prototyping in prosthodontics. J Prosthodont 2012;21:641-44.19. Torabi K, Farjood E, Hamedani S. Rapid protoyping tech-nologies and their applications in prosthodontics, a review of literature. J Dent (Shiraz) 2015;16(1):1-9.
WebliographyChoi JW, Kim N. Clinical application of three-dimensional print-ing technology in craniofacial plastic surgery. Arch Plast Surg 2015;42(3):267-77. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4439584/.
Gerstle TL, Ibrahim AM, Kim PS, Lee BT, Lin SJ. A plastic surgery application in evolution: three-dimensional printing. Plast Recon-str Surg 2014;133(2):446-51. Abstract available at: http://www.ncbi.nlm.nih.gov/pubmed/24469175.
Lambrecht JT, Berndt D, Christensen AM, Zehnder M. Haptic model fabrication for undergraduate and postgraduate teaching. Int J Oral Maxillofac Surg 2010;39(12):1226-9. Abstract avail-able at: http://www.ncbi.nlm.nih.gov/pubmed/20851573
McMenamin PG, Quayle MR, McHenry CR, Adams JW. The production of anatomical teaching resources using three-dimen-sional (3D) printing technology. Anat Sci Educ 2014;7(6):479-86. Abstract available at: http://www.ncbi.nlm.nih.gov/pubmed/?term=The+production+of+anatomical+teaching+resources+using+three-dimensional+(3D)+printing+technology.
Qi S, Yan Y, Li R, Hu J. The impact of active versus passive use of 3D technology: a study of dental students at Wuhan University, China. J Dent Educ 2013;77(11):1536-42. Available at: http://www.jdentaled.org/content/77/11/1536.long.

The Use of 3D Printing in Dental Implant Education
11June 2016
1. Rapid prototyping technology was originally developed in the __________________.
a. 1970s b. 1980s c. 1990s d. 2000s
2. 3D printed models were not widely used in the field of dentistry until recently as __________________.
a. they were highly complex b. their cost was prohibitive c. only large manufacturers could accommodate their
large size d. a and b
3. Displaying 3D morphology on a 2D screen provides the surgeon with __________________ representation of the patient’s anatomy.
a. a high resolution b. a complete c. an incomplete d. a and b
4. Using the subtractive technique to create physical prototypes, one limitation is that __________________.
a. reproduction of anatomical undercuts is almost impossible
b. the relatively poor quality of milled models c. polyurethane foam is brittle, soft, cannot be sterilized d. all of the above
5. Prior to 3D printing, highly complex data had to be pre-processed to provide a format that a RP system could recognize.
a. True b. False
6. The additive method to create physical prototypes results in __________________.
a. translucent models whereby the internal anatomy can be observed
b. models that can include undercuts, voids and complex internal geometries
c. cost-effective models d. all of the above
7. By accurately simulating the hard tissue, 3D models provide __________________.
a. visual information b. tactile information c. documentation for visualization, diagnostic, therapeutic
and educational purposes d. all of the above
8. For many patients, observing the procedure on a 3D model __________________.
a. decreases visualization of the procedure b. decreases fear of the unknown c. increases resistance to the proposed treatment d. decreases compliance
9. The __________________ is/are one of the most common maxillary anatomical landmarks that is/are significant in implant dentistry.
a. the sinus floor and sinus anatomy b. the posterior superior alveolar artery c. the greater palatine foramen and the incisive canal d. all of the above
10. The pathway of the inferior alveolar nerve (IAN) and the mental foramen are significant landmarks for implant dentistry.
a. True b. False
CEQuizTo complete this quiz online and immediately download your CE verification document, visit www.dentallearning.net/3DP-ce, then log into your account (or register to create an account). Upon completion and passing of the exam, you can immediately download your CE verification document. We accept Visa, MasterCard, Discover, and American Express.

DENTAL LEARNING www.dentallearning.net
12
11. When using 3D models, the student can __________________. a. remove any possibility of implant failure b. accurately treatment plan and practice the procedure
ahead of the patient visit c. avoid patients being noncompliant with maintenance d. all of the above
12. Using 3D models helps __________________. a. to improve team communication and trust b. with accurate selection of the required materials c. to improve accuracy and may reduce treatment time d. all of the above
13. Implant students are able to practice __________________ using 3D models.
a. Immediate implant placement and immediate provisionalization
b. implant placement lateral to the IAN c. sinus augmentation procedures d. all of the above
14. RP techniques are becoming more attractive and can be used to design, develop and manufacture __________________.
a. dental prostheses b. bone grafts c. temporary anchorage devices d. luting cements
15. According to the responses of the students at the NYU Implant Program, the biggest improvement in their educational experience by incorporating the use of 3D models was __________________.
a. knowledge of the patient’s anatomy b. treatment planning skills c. practicing the surgical procedure and becoming more proficient d. Planning and placing of provisional restorations
16. RP techniques can be used to design, develop and manufacture dental prostheses.
a. True b. False
17. On the 1 – 10 scale used in the survey, the average score students gave when asked to rank how much 3D printing models helped in the planning and placement of provisional restorations was __________________.
a. 8 b. 8.4 c. 9 d. 9.5
18. According to the student survey responses, the area providing the least improvement with incorporating the use of 3D models was __________________.
a. patient understanding of the procedures b. treatment planning skills c. decreased time of the procedure d. confidence in treating the patient
19. Using 3D scanning devices and CAD for the prosthesis, __________________.
a. dental prostheses can now be fabricated layer by layer directly from a computer model
b. labor costs are substantially reduced c. the models can be used to demonstrate implant maintenance
to patients d. all of the above
20. Generating 3D models based on CBCT datasets has promising potential for implant education, for understanding, planning and surgical practice.
a. True b. False
CEQuiz

www.dentallearning.net/3DP-ceCE ANSWER FORM (E-mail address required for processing)
*Name: Title: Speciality
*Address: NPI No.
*City: *State: *Zip: AGD Identification No.
*E-mail:
*Telephone: License Renewal Date:
Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. COURSE EVALUATION and PARTICIPANT FEEDBACK: We encourage participant feedback pertaining to all courses. Please be sure to complete the evaluation included with the course. INSTRUCTIONS: All questions have only one answer. Participants will receive confirmation of passing by receipt of a verification certificate. Verification certificates will be processed within two weeks after submitting a completed examination. EDUCATIONAL DISCLAIMER: The content in this course is derived from current information and research based evidence. Any opinions of efficacy or perceived value of any products mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of Dental Learning. Completing a single continuing education course does not provide enough information to make the participant an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. COURSE CREDITS/COST: All participants scoring at least 70% on the examination will receive a CE verification certificate. Dental Learning, LLC is an ADA CERP recognized provider. Dental Learning, LLC is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Please contact Dental Learning, LLC for current terms of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. Dental Learning, LLC is a California Provider. The California Provider number is RP5062. The cost for courses ranges from $19.00 to $90.00. RECORD KEEPING: Dental Learning, LLC maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of request. Dental Learning, LLC maintains verification records for a minimum of seven years. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfied with this course can request a full refund by contacting Dental Learning, LLC in writing or by calling 1-888-724-5230. Go Green, Go Online to www.dentallearning.net to take this course. © 2016
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
QUIZ ANSWERSFill in the circle of the appropriate answer that corresponds to the question on previous pages.
EDUCATIONAL OBJECTIVES1. Review the history and use of 3D models and techniques to create these;2. List and describe advantages of 3D versus 2D models in implant dentistry;3. Describe the use of 3D models for implant treatment planning and pre-operative practice; and 4. Review the results of the student survey and implications for dental education.
If you have any questions, please email Dental Learning at [email protected] or call 888-724-5230.
COURSE SUBMISSION: 1. Read the entire course.2. Complete this entire answer sheet in
either pen or pencil.3. Mark only one answer for each question.4. Mail answer form or fax to 732-303-0555. For immediate results:1. Read the entire course.2. Go to www.dentallearning.net/3DP-ce.3. Log in to your account or register to create an
account.4. Complete course and submit for grading to
receive your CE verification certificate.
A score of 70% will earn your credits.
Dental Learning, LLC500 Craig Road, First FloorManalapan, NJ 07726
*If paying by credit card, please note:MasterCard | Visa | AmEx | Discover
*Account Number
______________________________________________
*Expiration Date
______________________________________________
The charge will appear as Dental Learning, LLC.
If paying by check, make check payable to Dental Learning, LLC.
ALL FIELDS MARKED WITH AN ASTERISK (*) ARE REQUIRED
AGD Codes: 690, 691, 697
Price: $29 CE Credits: 2Save time and the environment by taking this course online.
COURSE EVALUATIONPlease evaluate this course using a scale of 3 to 1, where 3 is excellent and 1 is poor.
1. Clarity of objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
2. Usefulness of content . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
3. Benefit to your clinical practice . . . . . . . . . . . . . . . . . . . . 3 2 1
4. Usefulness of the references . . . . . . . . . . . . . . . . . . . . . . 3 2 1
5. Quality of written presentation . . . . . . . . . . . . . . . . . . . . 3 2 1
6. Quality of illustrations . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
7. Clarity of quiz questions . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
8. Relevance of quiz questions . . . . . . . . . . . . . . . . . . . . . . 3 2 1
9. Rate your overall satisfaction with this course . . . . . . . . 3 2 1
10. Did this lesson achieve its educational objectives? Yes No
11. Are there any other topics you would like to see presented in the future? __________________________________________________________________________
_______________________________________________________________________________________
The Use of 3D Printing in Dental Implant Education
Related Documents