DENTAL CONSIDERATIONS AND DRUGS IN PREGNANT AND LACTATING MOTHER -SUNAYANA SHRESTHA 4 TH YEAR, ROLL: 44 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
DENTAL CONSIDERATIONS AND DRUGS IN PREGNANT AND LACTATING MOTHER
-SUNAYANA SHRESTHA
4TH YEAR, ROLL: 44

2
CONTENTS:
• INTRODUCTION• MAJOR ORAL CHANGES• MINOR ORAL CHANGES• SYSTEMIC CHANGES DUE TO ORAL CONDITIONS• DENTAL TREATMENT DURING PREGNANCY• DENTAL TREATMENT GUIDELINE• DRUGS DURING PREGNANCY AND LACTATION PERIOD
• FDA CLASSIFICATION• ANALGESICS• ANTIBIOTICS• SEDETIVES AND ANXIOLYTICS• ANESTHETICS• EMERGENCY MEDICATION
• CONCLUSION• REFERENCES
3
INTRODUCTION• Physiological condition starting from conception till delivery
of fetus.• Characterized by various changes in female body• Divided into 3 trimesters1st Trimester (1-12 weeks)Fetal organ formation and differentiation.Most susceptible to adverse effects of teratogens.•2nd Trimester (13-24 weeks) Fetal growth and maturation•3rd Trimester (25-40 weeks) Fetal growth continues with final weight gain

4
• Changes evident in oral cavity as well.• Few major and minor changes are seen.considered an impediment to dental treatment• with some treatment modifications and initial planning; preventive, emergency, and routine dental procedures are all suitable during various phases of a pregnancy.1ST TRIMESTER: Avoid all elective care but provide care as needed.2ND TRIMESTER: Safest period to provide dental care.
3RD TRIMESTER: Focus of concern is risk to upcoming birth process and safety and comfort of the pregnant woman.
5
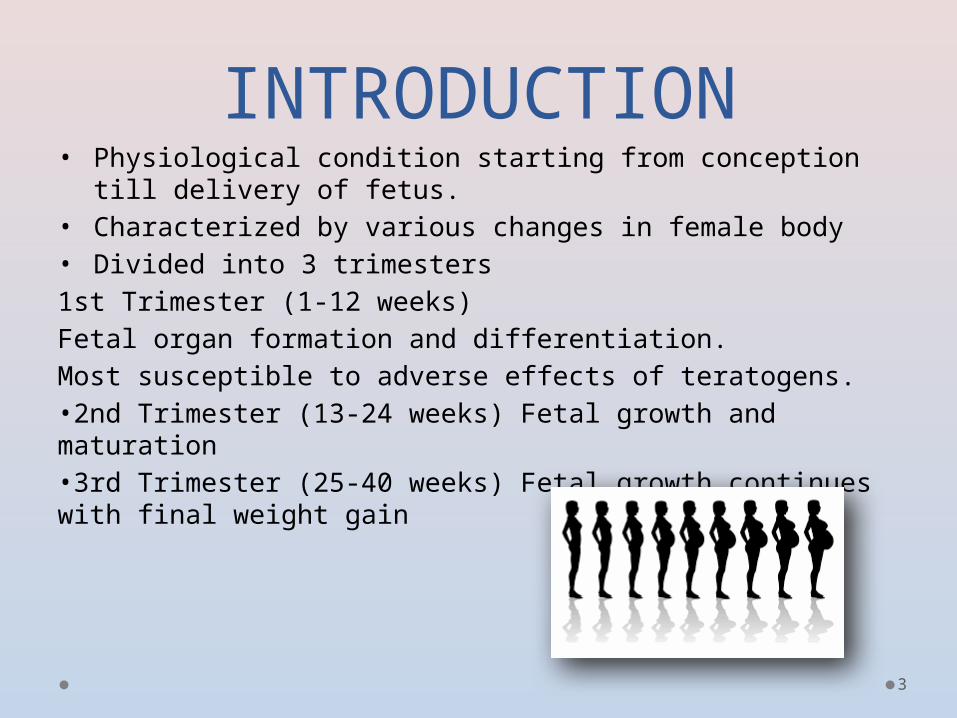
MAJOR ORAL CHANGES• PREGNANCY TUMOR:Also known as ‘pyogenic granuloma’ due to its high vascular nature.• Occurs in up to 5% of women.• Most common in buccal maxillary anterior areas.• Usually starts in an area of gingivitis• Rapid growth up to 2 cm.• Single tumor-like growth• usually in interdental papillae• Purplish to bluish in color, may be ulcerated- bleeds easily• HISTOLOGICAL: Atrophic stratified squamous epithelium
with edematous connective tissue and thin walled vascular channels.

6
Treatment
• Scaling and root planing• Excision in 2nd trimester if it is too large or bleeds
too easily• May regress spontaneously after pregnancy
7
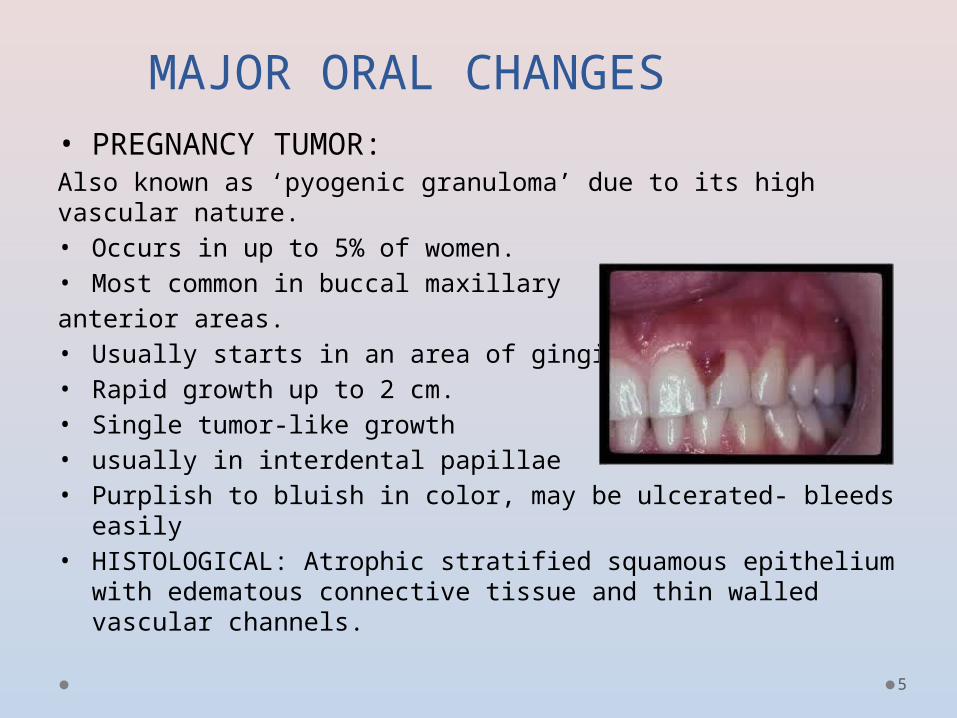
PREGNANCY INDUCED GINGIVITIS AND PERIODONTITIS:
• Occurs in about 50% of pregnant women• Caused by hormonal and vascular changes of pregnancy• Elevated circulating estrogen increases capillary permeability.• Preexisting gingivitis may predispose to
pregnancy gingivitis• Occurs commonly in the 2nd to 8th months
8
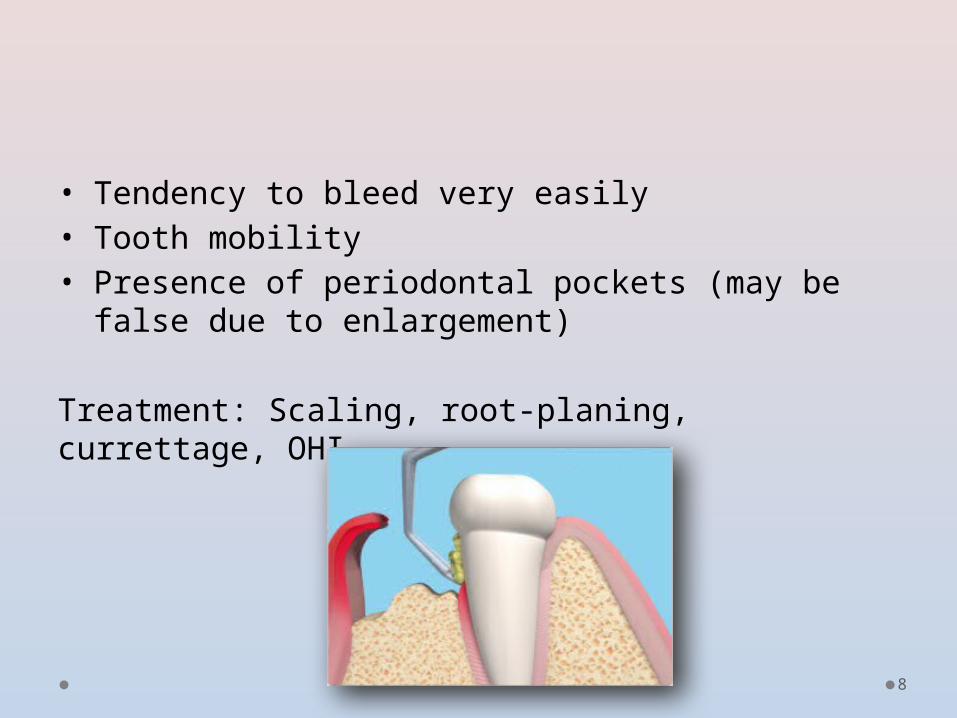
• Tendency to bleed very easily• Tooth mobility• Presence of periodontal pockets (may be false
due to enlargement)
Treatment: Scaling, root-planing, currettage, OHI

9
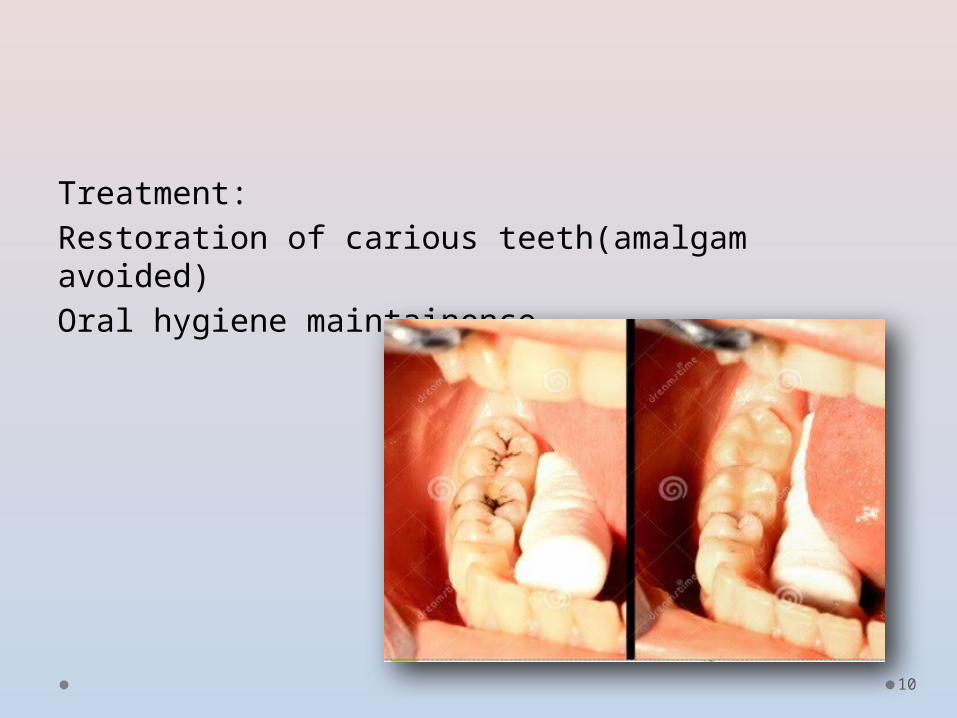
DENTAL CARIES:• Usually seen in women with poor oral hygiene
and preexisting carious status• Mainly due to myths like to avoid brushing and
dental treatment• Accelerated due to decreased salivary flow and
change in diet
10
Treatment:Restoration of carious teeth(amalgam avoided)Oral hygiene maintainence
11
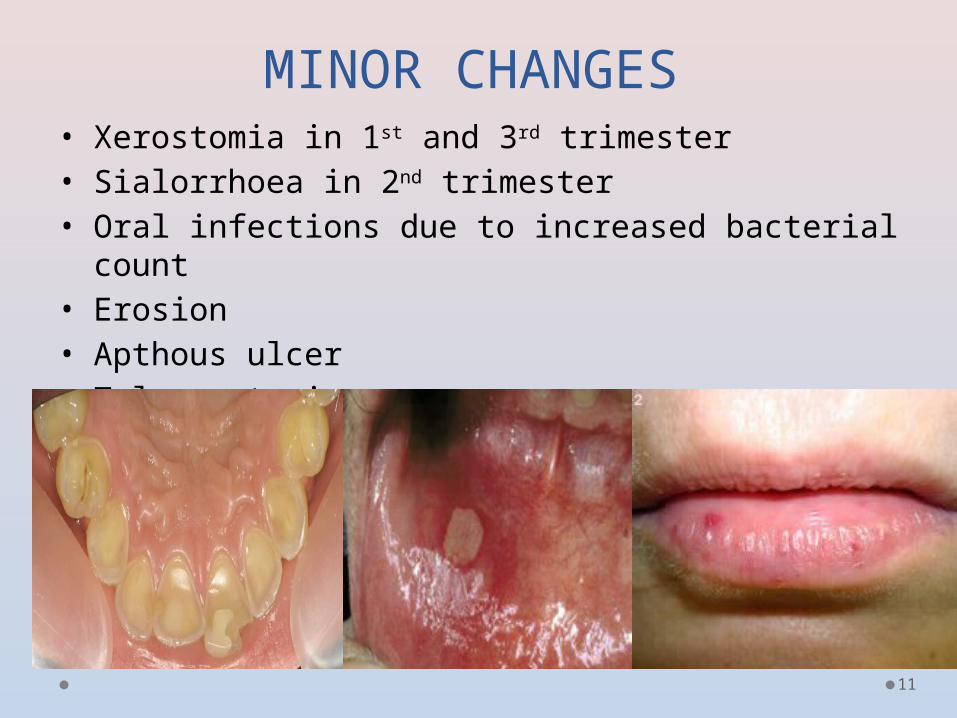
MINOR CHANGES• Xerostomia in 1st and 3rd trimester• Sialorrhoea in 2nd trimester• Oral infections due to increased bacterial count• Erosion• Apthous ulcer• Telangectasia
12
Systemic changes due to oral disease in pregnancy
• Low birth weight (LBW)
• Pre term labor and pre term birth: Inflammatory response stimulates prostaglandin and cytokine production to stimulate labor Thorough calculus (tartar) removal in pregnant women with periodontitis may reduce pre-term births
• Pre eclapsia :Periodontal infection leads to inflammatory vascular damage Triggers cell damage in placenta

13
DENTAL TREATMENT IN PREGNANCY1st TRIMESTER:Plaque controlOral hygiene instructionScaling, polishing, curettageAvoid elective treatment; urgent care only
2ND TRIMESTER:Plaque controlOral hygiene instructionScaling, polishing, curettageRoutine dental care
3RD TRIMESTER:Plaque controlOral hygiene instructionScaling, polishing, curettageRoutine dental care (after middle of third trimester, elective care should be avoided)

14
DENTAL MANAGEMET GUIDELINES
• Developing rapport with patient reduces anxiety• Detailed medical history with medical
consultation.• Monitoring of vital signs and blood examination
anemia and folate deficiency• Proper preventive programs can reduce caries
incidence in child• Prenatal fluoride 2.2mg/day• Short appointments• Patient advised to change position frequently
15
CHAIR POSITION IN PREGNANCY
• SUPINE POSITION CONTRAINDICATED increased size of uterus can obstruct vena cava and aortasemi reclined position adviced
return to the heart reduced perfusion of uterus fetal hypoxiaSupine hypotension Syndrome:• Obstruction of inferior vena cava and aorta from pressure
of the large fetus. Symptoms: Sweating Nausea Weakness Sense of lack of air

16
PREVENTION:•Elevate right hip 10-12 cm Use of soft pillow on right side•Weight is taken off the major vessels
TREATMENT:Roll patient onto her left side.
17
RADIOGRAPHS DURING
PREGNANCY
• Take as needed with optimal methods for reducing secondary radiation and exposure time.• Always use a lead apron.• Exposure to fetus (with apron use) is • .00001 centiGray.(rad)• Exposure can be limited by:
o Lead apron shielding o Modern fast film o Avoiding retakes
• X-ray only if necessary (i.e. root canal therapy, trauma)

Use of Radiation on Pregnant Patient• Dose given and time of gestation are important• doses < 5-10 rads (cGy) not teratogenic• fetus is most susceptible to radiation between the
2nd and 6th week of gestation• single dental x-ray exposes patient to 0.01 millirads
of radiation. In relative terms, this amount is 40 times less than daily dose acquired from cosmic radiation. Therefore, important diagnostic radiation should not be withheld during pregnancy

19
TREATMENTS TO BE AVOIDED
• Radiographs requiring high dose of radiation eg. CBCT
• Stressful procedures requiring prolonged chair time
• Major surgical procedures• Amalgam restorations
20
MEASURES TO PREVENT ORAL
CONSEQUENCES• Proper diet• Avoid smoking and drinking• Use of oral hygiene measures like brushing, flossing and Chlorhexidine mouth wash• Timely and occasional visit to dental clinic

21
• Always safe to avoid drug during pregnancy esp in 1st trimester.
• Drugs may cross placental barrier and may be toxic to the child
• Considering drugs for group of patient like pregnant, trying to conceive and in patient with unknown pregnancy status limited group of mediations used.o Analgesics and anti inflammatoryo Antibiotico Local anesthesiao Sedativeso Emergency medication
DRUGS DURING PREGNANCY AND
LACTATION PERIOD

22
FDA classification system based on potential for causing birth defects:• A = Controlled Studies in women fail to demonstrate a risk
to the fetus in the first trimester and the possibility of fetal harm appears remote
• B = Animal studies show no risk, or if risk shown in animals, controlled trials in women showed no risk
• C = Studies in animals with adverse effects and no human studies,
OR no animal or human studies, but benefits of use may outweigh potential harms
• D = There is evidence of human fetal risk, but benefits may outweigh risks
• X = Contraindicated
23
COMMONLY USED ANALGESICS
• Paracetamol (B)• Ibuprofen (B/D*) • Oxycodone (B/D*) • Hydrocodone and codeine (C/D*)• Aspirin(C/D*)
*avoid in third trimester
24
Paracetamol • analgesic of choice for all stages of gestation• treat mild to moderate pain and fevers• avoid chronic and large doses • Maternal anemia and fetal renal disease Aspirinnonteratogenic but may cause maternal and fetal hemorrhage• large and chronic doses during last trimester may result
in premature closure of ductus arteriosus, fetal hypertension, anemia, and low birth weight
ibuprofen • Avoid in 3rd trimester• adverse circulatory effectscodiene• avoid codeine in late • fetal respiratory depression and withdrawal symptoms

25
SEDATIVES/ANXIOLYTICS
rated D and can cause oral clefts with prolonged exposure.• Nitrous oxide should not be used in 1st trimester
(If used in 2nd and 3rd, do not go below 50% O2)• SHORT TERM exposure do not cause birth defects
or spontaneous abortion• CHRONIC exposure may result in fetal loss and
infertility
26
ANTIBIOTICS• penicillin V and amoxicillin is preferred drug for mild to moderate infections• no studies show penicillin to be teratogenic• amoxicillin extensively used without harming the
fetus• Drug classes: B: penicillin, cephalosporins, erythromycin, clindamycin, Azithromycin D: Tetracycline

27
TO USE:• Amoxicillin• Penicillin V• Erythromycin (base
form)• cephalosporin• Clindamycin• Metronidazole
TO AVOID:• Doxycycline•
Tetracycline•
Erythromycin (estolate form)
• Vancomycin

28
OTHER ANTIMICROBIAL
to use:• Nystatin (B)• Chlorhexidine rinse (B)Use with caution:• Clotrimazole (C)• Ketoconazole (C)• Fluconazole (C)Do not use:• Doxycycline (D)

29
Local Anesthetic Use in PregnancyClass B:• Lidocaine (Xylocaine)• Etidocaine• Prilocaine Class C:• Procaine• Bupivicaine• Mepivicaine • LidocaineWidely use without obvious sideeffectintravascular injections of lidocaine pass through the placenta but the concentrations are too low to harm fetus• prilocaine might cause methemoglobinemia
30
TOPICAL AGENTS
• Fluoride
• Toothpaste & mouthrinse
• Xylitol chewing gum
• Chlorhexidine
• No over the counter mouthrinses with alcohol
31
EMERGENCY MEDICATION
• ALBUTEROLcategory C, safe during pregnancy• EpinephrineCategory c, use with caution• Naloxone Category c, use with caution• NitroglycerinCategory c, use with caution

32
MEDICATION DURING LACTATION
• Same drug dose as in pregnancy• Amount of drug excerted in breast milk is 2- 4%
of maternal dose.• Take drug just after breastfeeding and avoid
nursing for 4 hours.
33
CONCLUSION• Hence all the oral change regress spontaneously in post
partum period after balance of hormonal level.• Only severe conditions require medical interventions. But it is
always better adopt preventive measures• Also dental radiography poses little, if any risk to fetus
provided use of filter, collimation, fast speed film and lead aprons.
• Finally, considering drugs , if the benefits to the mother exceed the risk to the fetus and a medication is required, it always be administered regardless of FDA’s pregnancy factor definitions.
• Thus even though with proper planning and treatment modifications most of dental procedures can be carried out without fear of complication, prevention of such condition is safest treatment option in pregnancy.

34
REFERENCES:• BURKET’S ORAL MEDICINE
• MICHAEL GLICK, 12TH EDITION
• TEXTBOOK OF ORAL MEDICINE ORAL DIAGNOSIS AND ORAL RADIOLOGY
• RAVIKIRAN ONGOLE• PRAVEEN B N, 2ND EDITION
• CARRANZA’S CLINICAL PERIODONTOLOGY• 12TH EDITION
• Wasylko L, Matsui D, Dykxhoorn SM, Reider MJ. Weinberg S. A review of common dental treatments during pregnancy: implications for patients and dental personnel. J Can Dent Assoc 1998;64:434-9

35
Related Documents