DENTAL CONSIDERATION IN INFLAMMATORY BOWEL DISEASES Presented by: Jigyasha Timsina BPKIHS

dental consideration for inflammatory bowel disease
Aug 12, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DENTAL CONSIDERATION IN INFLAMMATORY BOWEL DISEASES
Presented by:Jigyasha
Timsina BPKIHS

Bowel and Bladder habit in history for dental checkup?!! ..,Well.. I will just skip through this and complete history taking faster…
INFLAMMATORY BOWEL DISEASE
General classification of
inflammatory processes that affects the large and small intestines.
Includes: 1)Crohn’s disease 2)Ulcerative colitis

Introduction Ulcerative colitis more prevalent 3.9 to 10 new cases of IBD per
100000 Shows three peak prevalance rates
. 1st peak- 20 to 24 years 2nd peak- 40 to 44 years 3rd peak- 60 to 64 years More commonly affects
Caucasians and Jews

Pathogenesis Considered to be idiopathic.
Increasingly believed to be a result interaction between environmental and genetic factors.
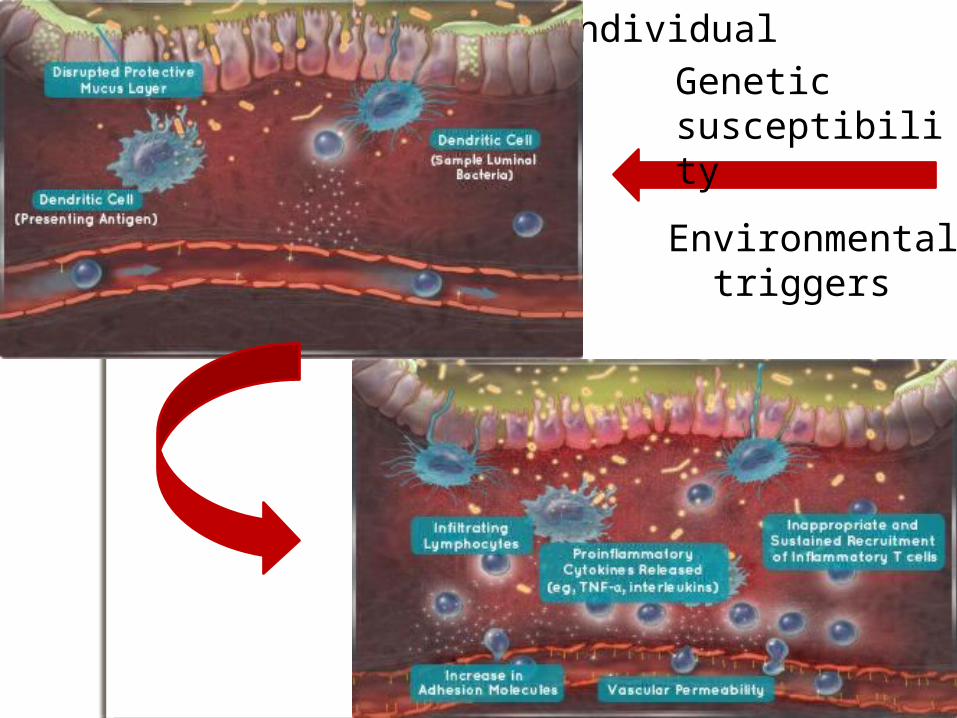
Genetically susceptible individual
Environmental triggers
Genetic susceptibility
Environmental triggers
Ulcerative Colitis a form of colitis, that includes
characteristic ulcers or open sores that attacks only the large intestine
Hallmark - rectal bleeding diarrhea
CROHN’S DISEASE (Crohn syndrome OR regional enteritis)
a type of inflammatory bowel disease (IBD) that may affect any part of the gastrointestinal tract from mouth to anus.
Types :1)Non-perforating 2)Perforating or aggressive
type
More commonly affects middle aged women from 20 to 39 years

Clinical features
• Skip lesions
• Granulomas
• All Layers
Differentiating features
ORAL MANIFESTATIONS
Can be catagorized as :1. Specific2. Non-specific3. Complications of malabsorption
caused by the bowel inflammation4. Side effects or complications of
medications prescribed to treat the bowel disease.

SPECIFIC NON SPECIFIC
CROHNS Orofacial Crohn disease
•Angular chelitis•Apthous ulcers/ Apthous stomatitis•Dry mouth•Halitosis
ULCERATIVE COLITIS
Pyostomatitis vegetans
•Apthous ulcers/ Apthous stomatitis•Glossitis •Cheilitis•Halitosis

Complications of malabsorption caused by the bowel inflammation
Folic acid deficiency– red painful tongue (Acute)
shiny and smooth (chronic)
Glossitis and Cheilitis
Vitamin A deficiency- hyperkeratosis of oral
mucosa Vitamin B12 deficiency- beefy red
tongue, mouth ulcersVitamin k deficiency- gum bleedingVitamin C deficiency- ulceration of
gums and mucosa

Side effects of therapeutic drugs
Budesonide glossitis, dry mouth
Cyclosporine gum hyperplasia
Ciprofloxacin oral candidiasis, angioedema, Stevens-Johnson syndrome / toxic epidermal necrolysis
Loperamide dry mouth, SJS/TEN, angioedema
Metronidazole unpleasant metallic taste, furry tongue, glossitis, stomatitis, oral candidiasis, dry mouth
Prednisolone oral candidiasis (thrush)
Sulfasalazine altered taste, stomatitis, oral candidiasis
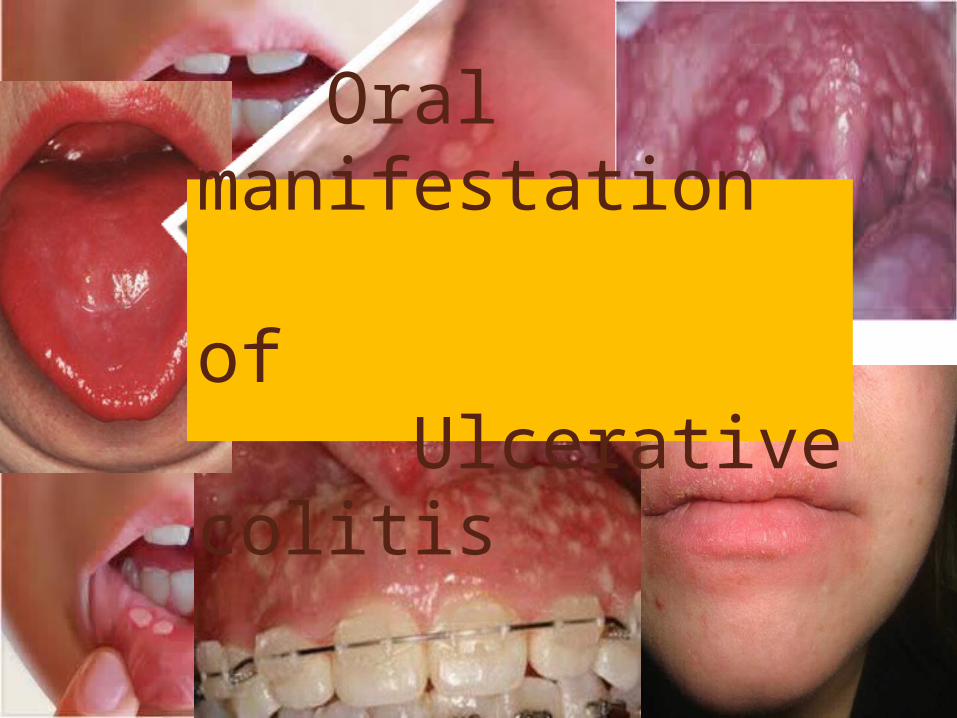
Oral manifestation of Ulcerative colitis

Pyostomatitis vegetansLarge number of broad
based tiny abscess developing in area of intense erythema
Most commonly affects gingiva and hard palate
Tongue least commonly affected
Histologicaly 1. Hyperplastic
stratified squamous epithelium
2. Intraepithelial or sub epithelial micro abscess
Diagnosis: Biopsy of perilesional tissue with histopathological and immunostaining examinations.
Treatment :1. Topical corticosteroids eg
clobetasol, flucinolone2. Treat the underlying disease.3. Some patient report benefit from
zinc supplementation >1yrs- 10mg OD daily <1yrs – 5mg OD daily4. Antibiotic therapy usually not
beneficial as lesion is refractory.
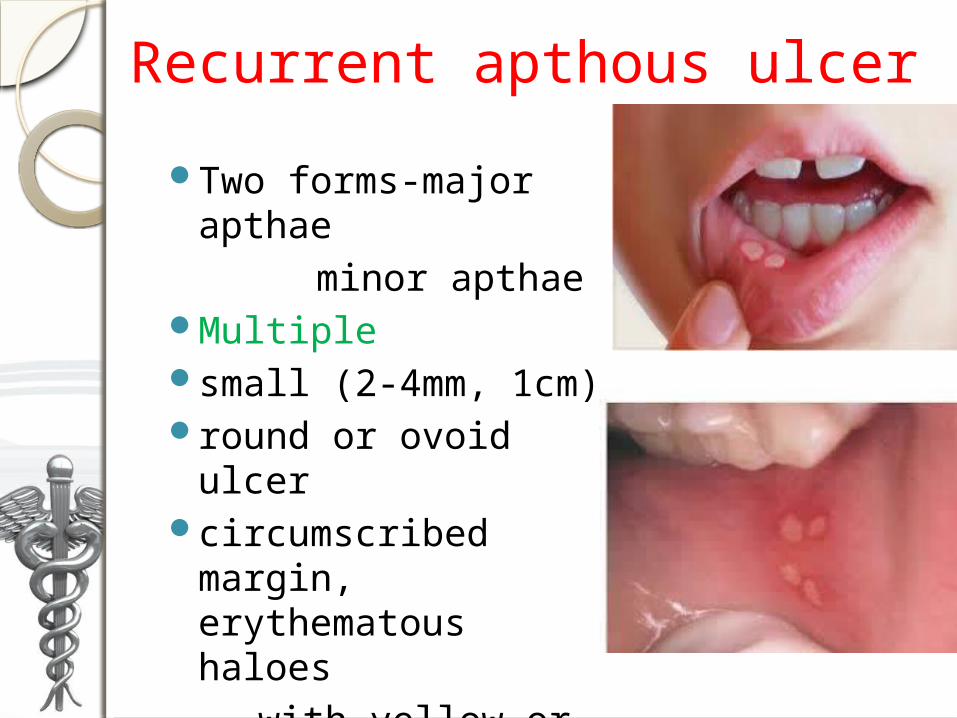
Recurrent apthous ulcer
Two forms-major apthae
minor apthae
Multiple small (2-4mm, 1cm)round or ovoid ulcer circumscribed
margin, erythematous haloes
with yellow or grey floor
Management Topical , intralesional , systemic
corticosteroids Topical and systemic analgesics eg:
2%lidocaine gel orabaseThalidomide , an immune modulating
and angiogenesis inhibiting drug is effective for refractory cases.-300 mg daily
Colchicines- 0.6mg tds for 2 weeksPentoxyphylline (TRENTAL 400mg) - in
cases where topical steroid do not respond.

CATEGORY THERAPEUTIC DOSE
Antimicrobials: Chlorhexidine Tetracycline Penicillin-G
0.2% mouthrinse or 1% gel5% tetracycline used as mouthwash50mg penicillin-G 4 times a day for 4 days
STEROID Topical : Flucinonide
Triamcinolone acetonideSystemic: Prednisolone
0.05% gel applied 2-4 times a day until healing 0.1% gel applied 2-4 times a day until healing
1-2 mg /kg/ day
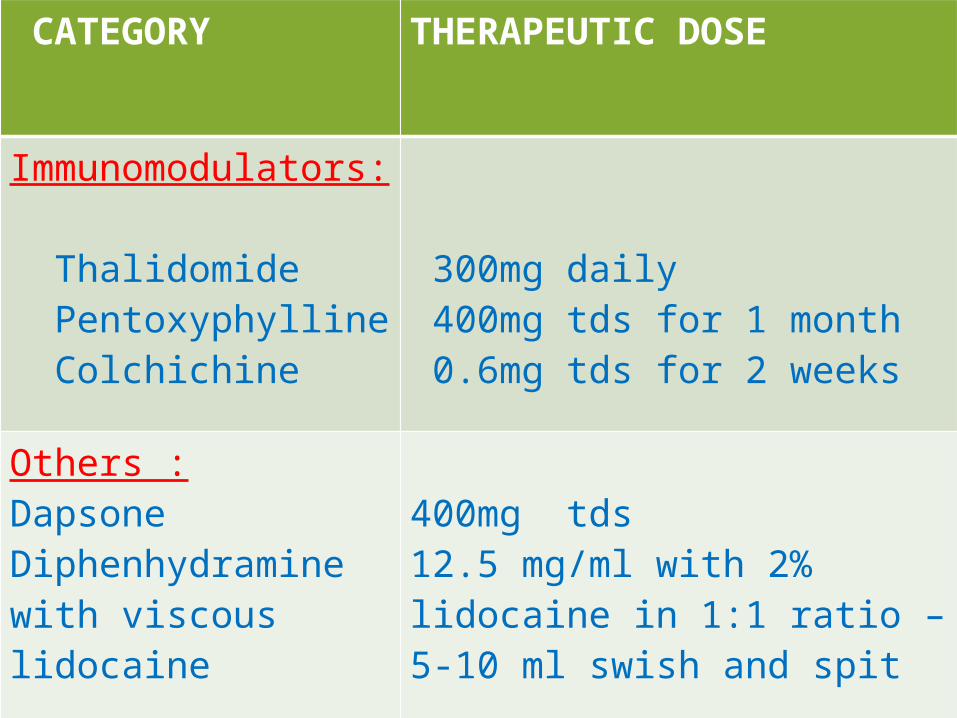
CATEGORY THERAPEUTIC DOSE
Immunomodulators: Thalidomide Pentoxyphylline Colchichine
300mg daily 400mg tds for 1 month 0.6mg tds for 2 weeks
Others :Dapsone Diphenhydramine with viscous lidocaine
400mg tds 12.5 mg/ml with 2% lidocaine in 1:1 ratio – 5-10 ml swish and spit

Which of the following antihelminthic drug shows immunomodulating
property??1) Albendazole2) Suramin3) Levamisole4) Ivermectin
• Levamisole -Sharada N, Shashikant MC,
Priyanka kant,Manika jain
Case study source :pubmed
Fifty RAS subjects were enrolled in the single-blind randomized placebo-controlled trial. Study medications were administered thrice daily for 3 consecutive days/week for 3 consecutive weeks. Patients in Group 1 received placebo, Group 2 received levamisole (150 mg) and Group 3 received levamisole (150 mg) and low-dose prednisolone (5 mg). Patients were followed up for 60 days after treatment
Result:Levamisole alone or in combination with
low dose prednisolone produced similar results
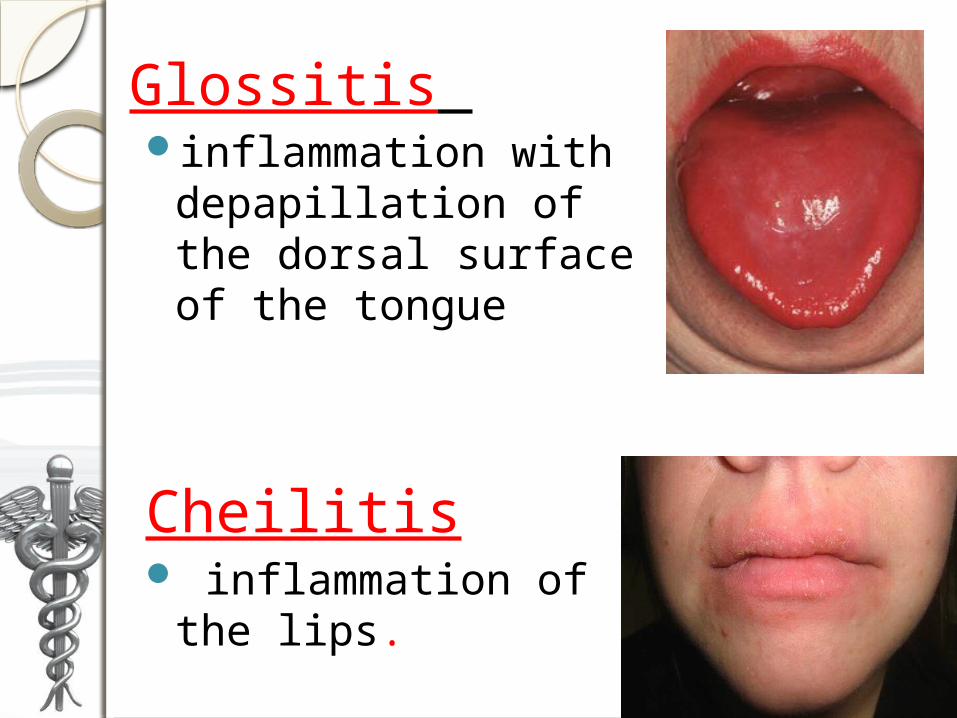
Glossitis inflammation with
depapillation of the dorsal surface of the tongue
Cheilitis inflammation of
the lips.
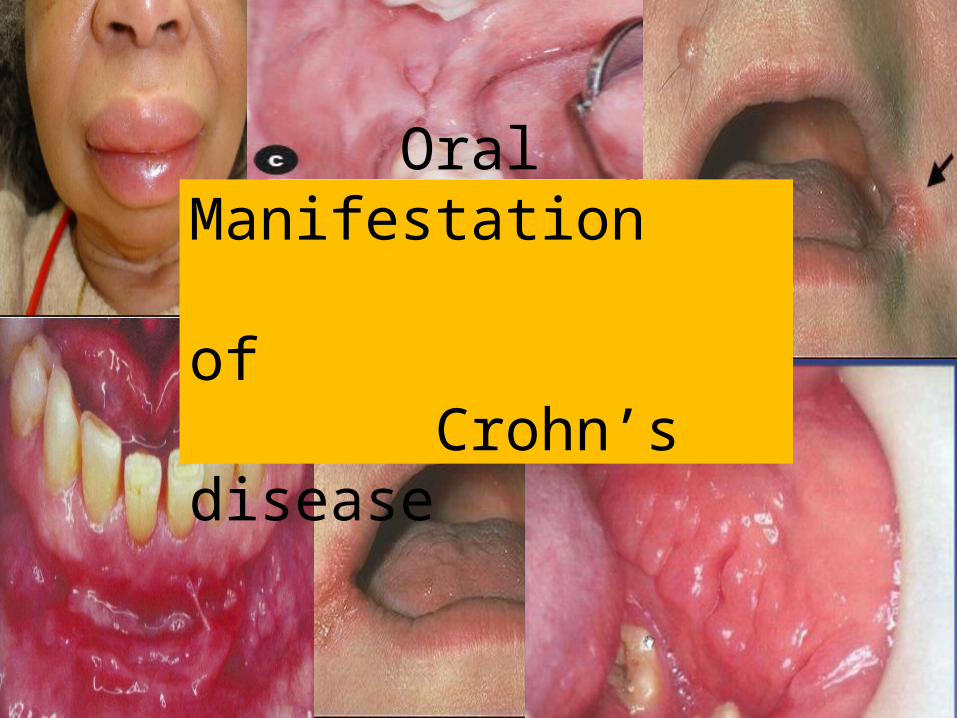
Oral Manifestation of Crohn’s disease

Oro-facial Crohn’s Disease
Signs of orofacial Chrohn disease include:
mucogingivitis
deep linear ulcers in the vestibule
-hyperplastic margins-rolled edge -shows presence of non
caseating granulomas
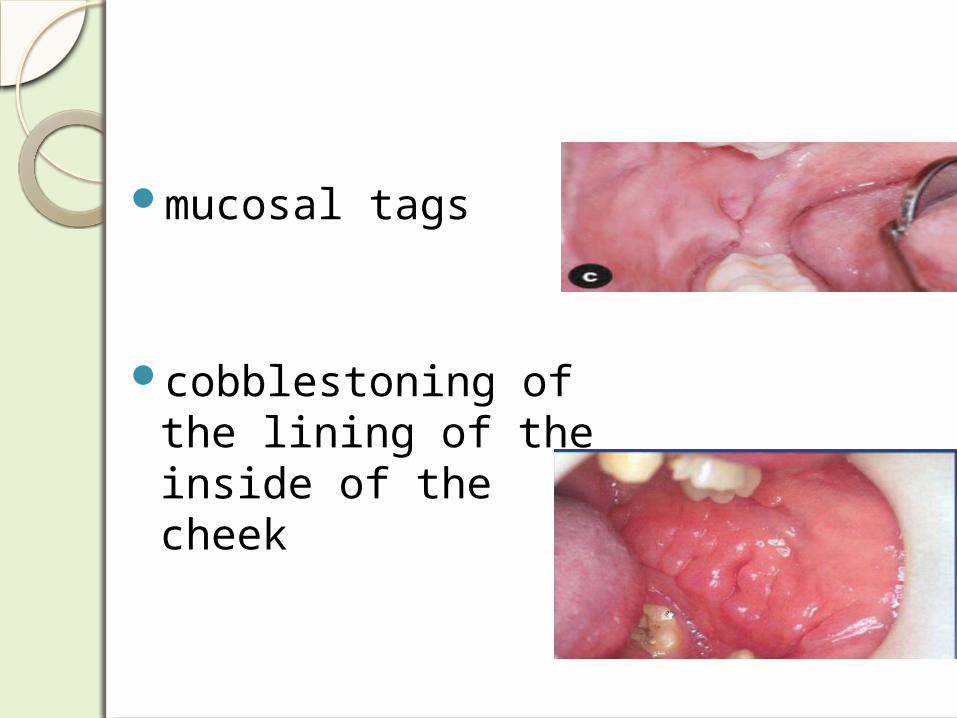
mucosal tags
cobblestoning of the lining of the inside of the cheek
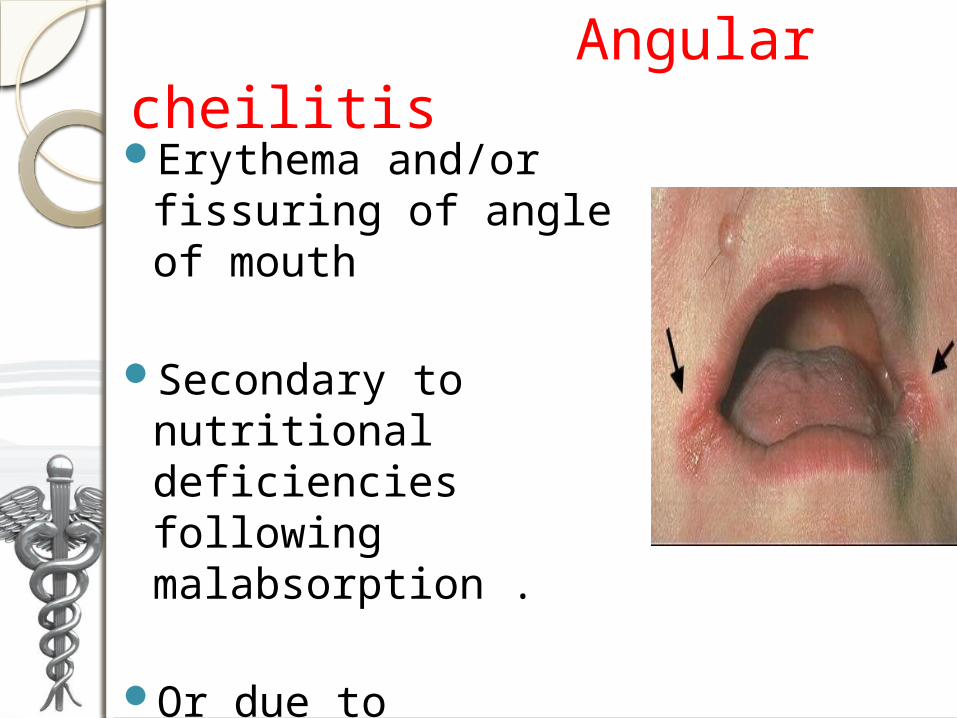
Angular cheilitisErythema and/or
fissuring of angle of mouth
Secondary to nutritional deficiencies following malabsorption .
Or due to concommitant infections

Management
Treatment of underlying pathology
Maintenance of proper hygiene
Topical antifungal medication as clotrimazole (0.1% )
amphotericin B, ketoconazole
Topical corticosteroids can help with the inflammation .

AngioedemaAlso called lip swelling
It may be allergic or drug induced.
Mild presentation but require immediate management if risk of airway blockage
MANAGEMENTAvoid any known allergen or trigger that
causes the symptoms Antihistamines -Cetrizine (Alerva 10mg)
OD Fexofanadine(Allegra 120
or 180 mg) Anti-inflammatory medicines
(Corticosteroids) Epinephrine shot
Lets just check if u had
been sleeping or not???
Specific oral manifestation of Ulcerative colitis is:
A. Angioedema B. Pyostomatitis
vegetansC. Angular cheilitesD. Glossitis
Crohn’s disease differs from Ulcerative colitis in that it doesnot show:
A. GranulomasB. Skip lesionsC. Fistula formationD. All layers involvementE. None (fistula formation requires
involvement of all layers of intestine)
Which of the following is a pustular lesion?
A. Recurrent Apthous UlcersB. Pyostomatitis VegetansC. AngioedemaD. Angular cheilitis
Management of IBD Detailed history, physical examination ,
gastrointestinal radiography and endoscopy.
Medical management First line drug
Sulfasalazine- initiate and maintain remission
Sazone 500mg 1-2g 3 to 4 times a day
Corticosteroid –Initiation dose 40 to 60 mg
prednisolone oral daily (Emsolone 5,10,20,40 mg tab)
Maintenance dose- 10 to 20 mg prednisolone oral daily

Second line drug - Antibiotic agents - Immunosuppresive drugs
Azathioprine -Azoran 5omg 1.5 to2.5 mg/kg body weight
Surgical management : in 15 to 20 % cases
proctocolectomy combined with ileostomy
Suppotive therapy bed rest , dietary manipulation ,
and nutritional supplementation.
Management of oral lesions
Chlorhexidine gluconate 0.2% used as swish and expectorate
Moderate potency topical steroid (eg 0.01% fluocinolone FLUCORT-H oint) or ultra potency preparation (eg clobetasol 0.05% LOBATE cream ) can be applied topically – 4 times a day
But should not exceed 2 continuous week
If lesions are disseminated , Dexamethasone 0.5mg/5ml
(DEXONA) used as rinse for 1 min – 4 times a day and expectorated

Dental evaluation of patient with IBDDetermine medications used , with special attention to steroid therapy in the past.
Evaluate the diagnosis of the type of IBD

Treatment planning modification schedule appointments during remission
Minimize stress by shorter appointments and adjunctive sedation techniques.
Evaluation of hypothalamic/pituitary/adrenal cortical
function to determine the patient’s ability to
undergo extensive dental procedures.

Dental management Frequent preventive and
routine dental care to prevent destruction of hard and soft tissue.
If patient under corticosteroid therapy
obtaining blood pressure and blood glucose measurement prior dental treatment highly recommended

Routine dental treatment like oral prophylaxis and simple restorations carried out as normal.
Surgical treatment contraindicated due to collective effect of risk associated with anemia like delayed wound healing , increased risk of infection depression of respiration
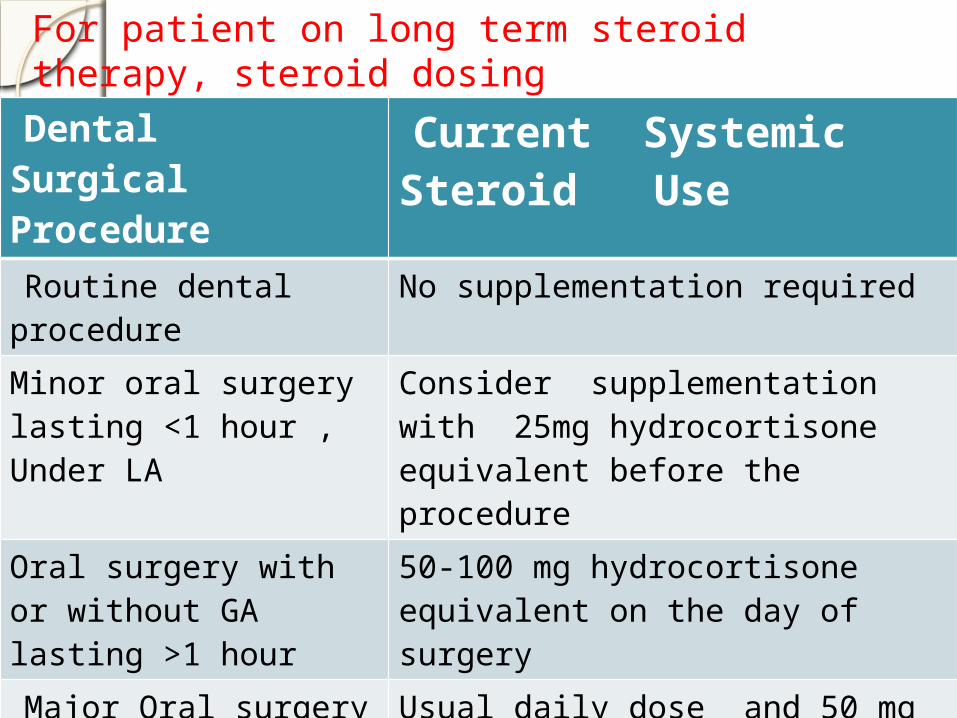
Dental Surgical Procedure
Current Systemic Steroid Use
Routine dental procedure
No supplementation required
Minor oral surgery lasting <1 hour , Under LA
Consider supplementation with 25mg hydrocortisone equivalent before the procedure
Oral surgery with or without GA lasting >1 hour
50-100 mg hydrocortisone equivalent on the day of surgery
Major Oral surgery done under GA lasting >1hour with significant blood loss
Usual daily dose and 50 mg hydrocortisone equivalent IV, repeat hydrocortisone equivqlent every 8 hour after initial dose upto 72 hours
For patient on long term steroid therapy, steroid dosing
In patient with history of immunosuppresive agents intake, liver function test recommended
complete blood studies including hemoglobin, hematocrit, red cell count and protrombin time and partial thromboplastin time necessary
Topical steroids should be short termed and monitored because of the side effects of mucosal atrophy and systemic absorption.
NSAIDS should be avoided.
Antibiotics that could aggravate diarrhea should be avoided.
These include :- amoxicillin-clavulanate (AMOXICLAB) and clindamycin

Pain and anxiety control measures
Patient are advised to obtain proper rest the night before treatment.benzodiazepine sedative can be prescribed to be taken the night before treatment.
Appointments are tolerated best when they are scheduled in the morning and in limited in duration.

Patients are advised to reduce business and social obligations the day of the appointment.
Analgesics (COX-2 inhibitor , acetaminophen) alone or in combination with opioid should be provided during postoperative phase when needed.
Conclusion In dental treatment of patients with
IBD, it is important that they undergo frequent dental revisions and preventive care to avoid oral infections and hard and soft tissue destruction.
We should be aware of the risk of infection, drug actions and interactions, the patient’s ability to withstand the stress and trauma of dental procedures and proper medical referral when necessary.
AND FINALLY An Twenty eight-year-old girl presented
with a four-month history of painful mouth ulcers, resulting in decreased oral intake and weight loss, history of intermittent abdominal pain and irregular bowel movements. On examination, she had redness and swelling of the lips as well as tenderness of the right lower quadrant of abdomen.
. Colonoscopy with multiple biopsies revealed multiple areas of the cobblestoning with sharply demarcated areas in-between and invovement of all the layers.
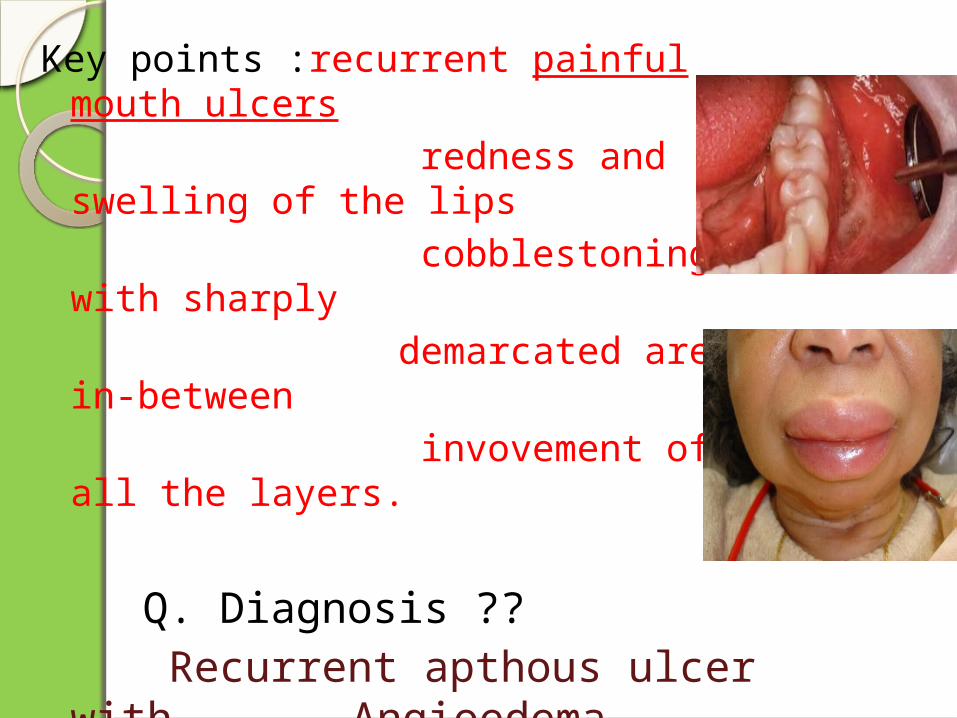
Key points :recurrent painful mouth ulcers
redness and swelling of the lips
cobblestoning with sharply demarcated areas in-
between invovement of all the
layers.
Q. Diagnosis ?? Recurrent apthous ulcer with
Angioedema secondary to Crohn’s disease

Points to be noted in history?? A. History of similar illness in other
family members?
B. Frequency of altered bowel movements ?
C. Medications used with special attention to steroid therapy in the past?

What investigations would you like to conduct before oral procedure??
A. Blood pressure and Blood glucose measurement
B. Complete blood studies including hemoglobin, hematocrit, red cell count and protrombin time and partial thromboplastin time
C. Liver function test
Which of the following drugs are not avoided in patients with IBD?
A. NSAIDsB. COX-2 inhibitorsC. Amoxicillin – ClavulanateD. Clindamycin
Which of the following dental modifications for IBD is false
A. Topical steroids should be short termed and monitored
B. Antibiotics that could aggravate diarrhea should be avoided
C. Aspirin should be givenD. None of the above

REFERENCESMedical problems in dentistry Crispian ScullyBURKET’S oral medicine Greenberg, Glick, ShipShafer’s textbook of Oral
pathologyNational handbook of medicineWikipedia Clinical Journals by clinics in
North America
THANK YOU

Related Documents