Dr. Paknahad

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr. Paknahad

CLASSIFICATION

(1) Size
(2) Number
(3) Shape/Form
(4) Defects of Enamel and Dentin
Developmental Disturbances

Microdontia
Macrodontia
Size
Microdontia
(1) Generalized Microdontia
(2) Localized Microdontia
Size

all teeth are smaller than normal
pituitary dawrfism
(1) Generalized Microdontia
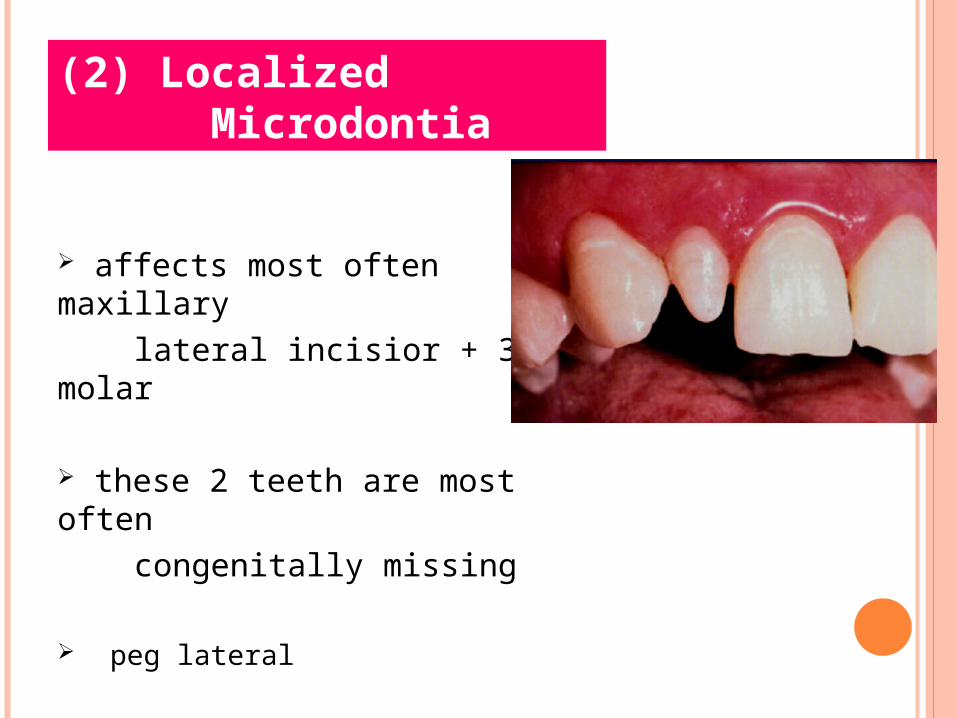
affects most often maxillary lateral incisior + 3rd molar
these 2 teeth are most often congenitally missing
peg lateral
(2) Localized Microdontia

Macrodontia
(1) Generalized Macrodontia
(2) Localized Macrodontia
Size
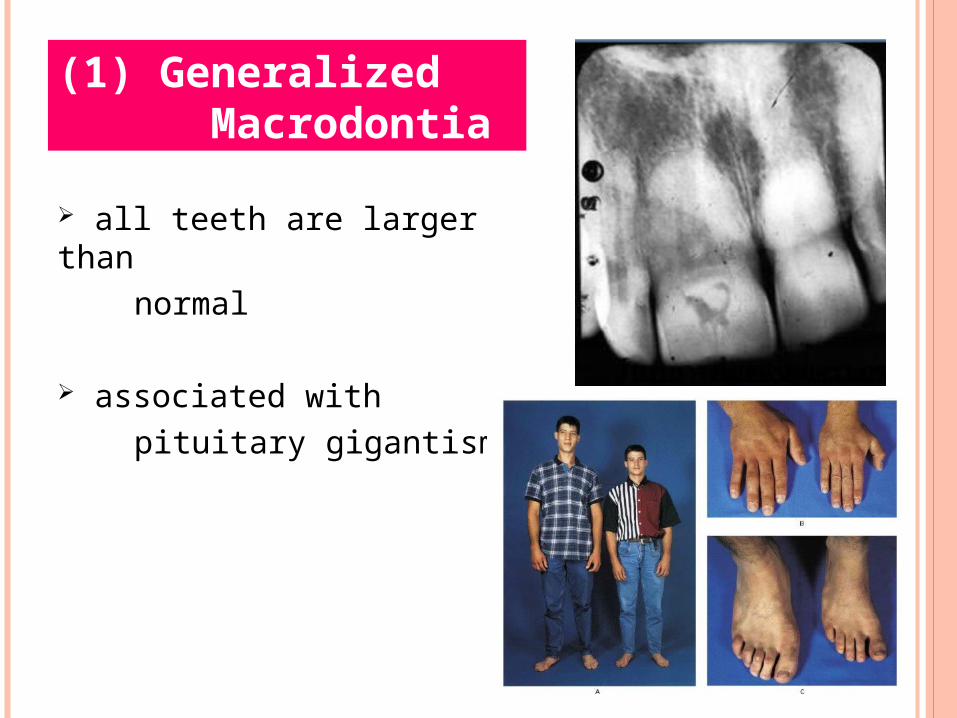
all teeth are larger than normal
associated with pituitary gigantism
(1) Generalized Macrodontia

Hemangioma, Hemifacial hypertrophy
(2) Localized Macrodontia

(1) Size
(2) Number
(3) Shape/Form
(4) Defects of Enamel and Dentin
Developmental Disturbances

Supernumerary teeth
( Hyperdontia, Supplemental)
many are impacted
cleidocranial dysostosis, gardner syndrome
Number
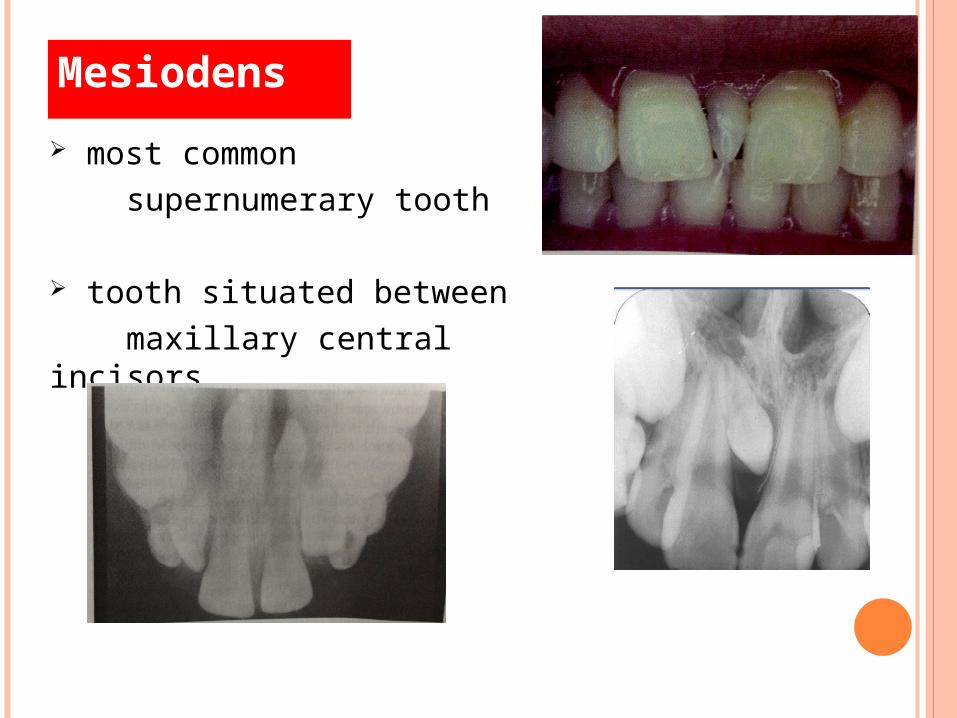
most common supernumerary tooth
tooth situated between maxillary central incisors
Mesiodens

situated bucally or lingually to one of the maxillary molars
Paramolar
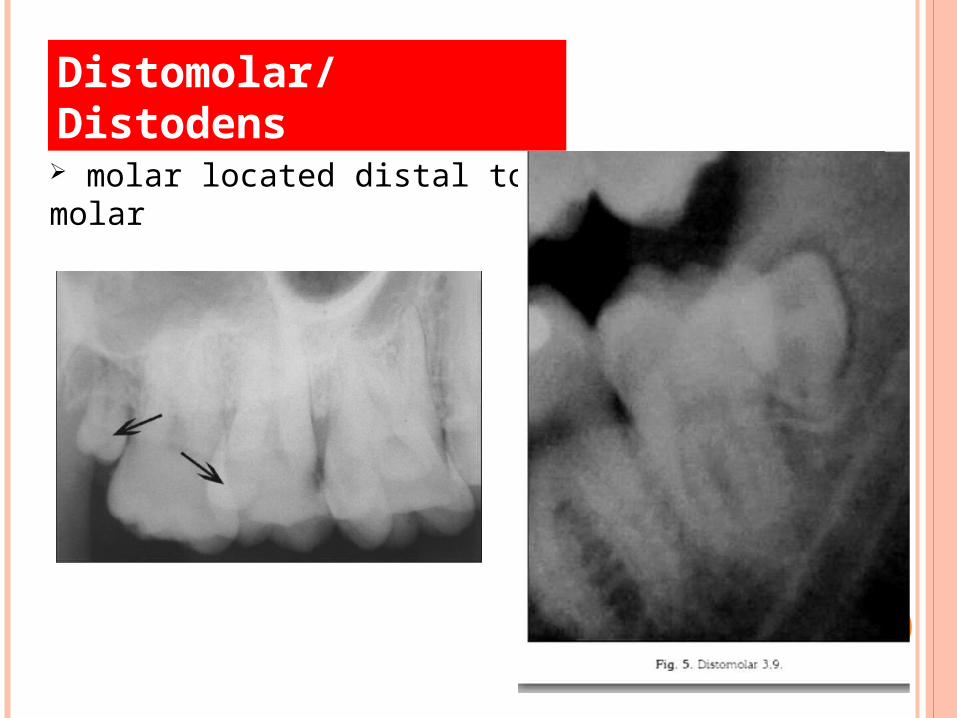
molar located distal to molar
Distomolar/Distodens

when all teeth are missing
ectodermal dysplasia
Complete Anodontia

lack of development of one or more teethPermanent: m3pm2max lateral mand central
Primary: max incisors
Hypodontia

lack of development of six or more teeth
Oligodontia

POSITION
Transposition

(1) Size
(2) Number
(3) Shape/Form
(4) Defects of Enamel and Dentin
Developmental Disturbances

joining of 2 developing tooth germs
resulting in a single large tooth structure
Fusion

Fusion

formation of 2 teeth from a single enamel organ
partial cleavage
Gemination(Twinning)

joined along the root surfaces
by cementum
more frequently in
posterior and maxillary regions
may occur before or after the
teeth have erupted
extraction of one may result in
extraction of the other
Concrescence

Taurodontism

angulation or a sharp
bend or curve in root
or crown of a formed tooth
trauma to a developing
tooth can cause root to form
at an angle to normal
axis of toothBull’s eye
Dilaceration

Dens Evaginatus(Leong’s Premolar
)

deep surface invagination of crown or root that is lined by enamel
2 forms:
coronal radicular
Dens Invaginatus (Dens in Dente)
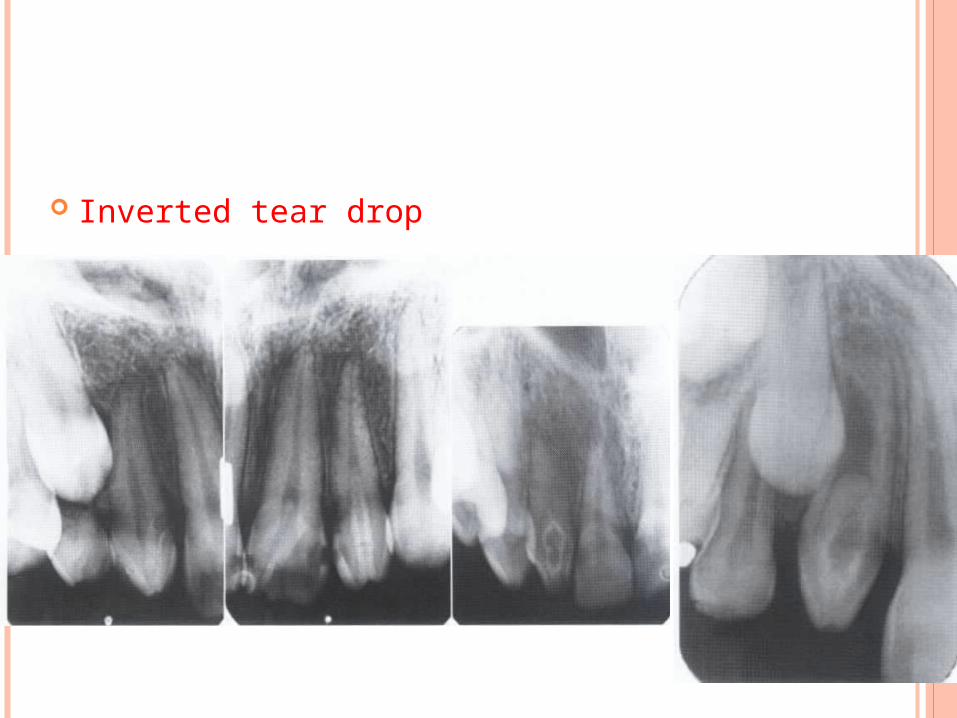
Inverted tear drop

droplets of ectopic enamel
or so called enamel pearls
may occasionally be found on roots of teeth
uncommon, minor abnormalities, which are formed on normal teeth
Enamel Pearls
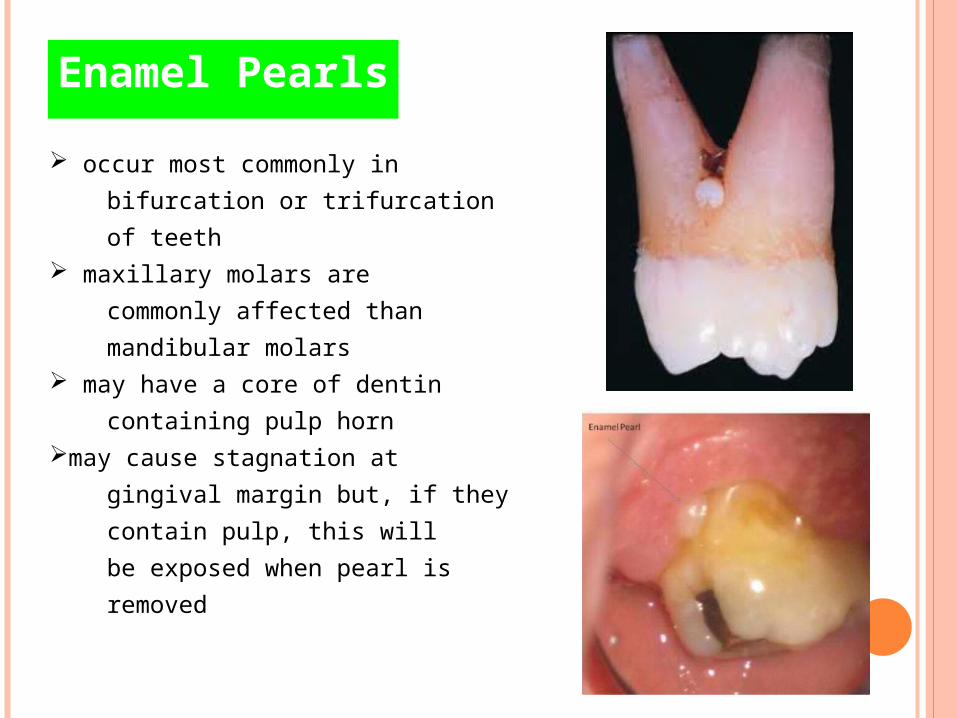
occur most commonly in
bifurcation or trifurcation
of teeth maxillary molars are
commonly affected than
mandibular molars may have a core of dentin
containing pulp horn may cause stagnation at
gingival margin but, if they
contain pulp, this will
be exposed when pearl is
removed
Enamel Pearls

D.D
Calculus/pulp stone

(1) Size
(2) Number and Eruption
(3) Shape/Form
(4) Defects of Enamel and Dentin
Developmental Disturbances

well-delineated additional cusp
located on the surface of an anterior tooth
Talon’s Cusp

TURNER’S HYPOPLASIA
Often Man. Pm ill defined radiolucency
D.D: anomalies in radiation therapy
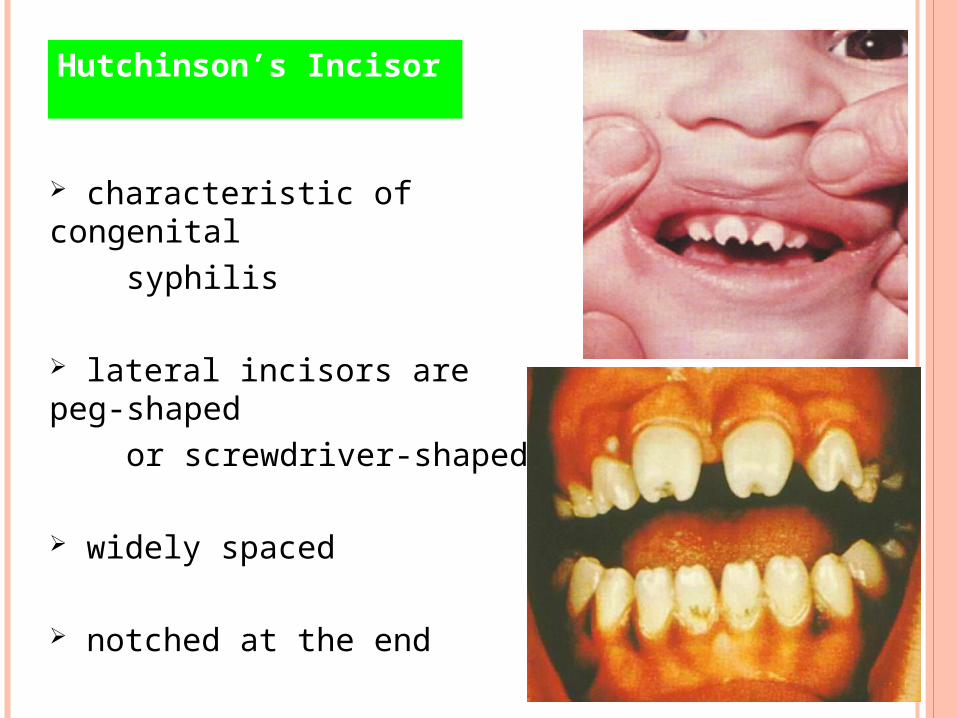
characteristic of congenital syphilis
lateral incisors are peg-shaped or screwdriver-shaped
widely spaced
notched at the end
Hutchinson’s Incisor

dental condition usually
associated with congenital
syphilis
characterized by multiple
rounded rudimentary enamel
cusps on permanent 1st molars
dwarfed molars with cusps
covered with globular enamel
growths
giving the appearance of a
mulberry
Mulberry Molar

Amelogenesis Imperfecta
group of conditions caused by
defects in the genes encoding
enamel matrix proteins
affects both dentition
deciduous permanent
classified based on pattern of
inheritance:
hypoplasia hypomaturation hypocalcified

inadequate formation of matrix
reduced enamel thickness
abnormal contour absent interproximal
contact points
dentin + pulp chambers
appear normal
Hypoplastic Amelogenesis Imperfecta
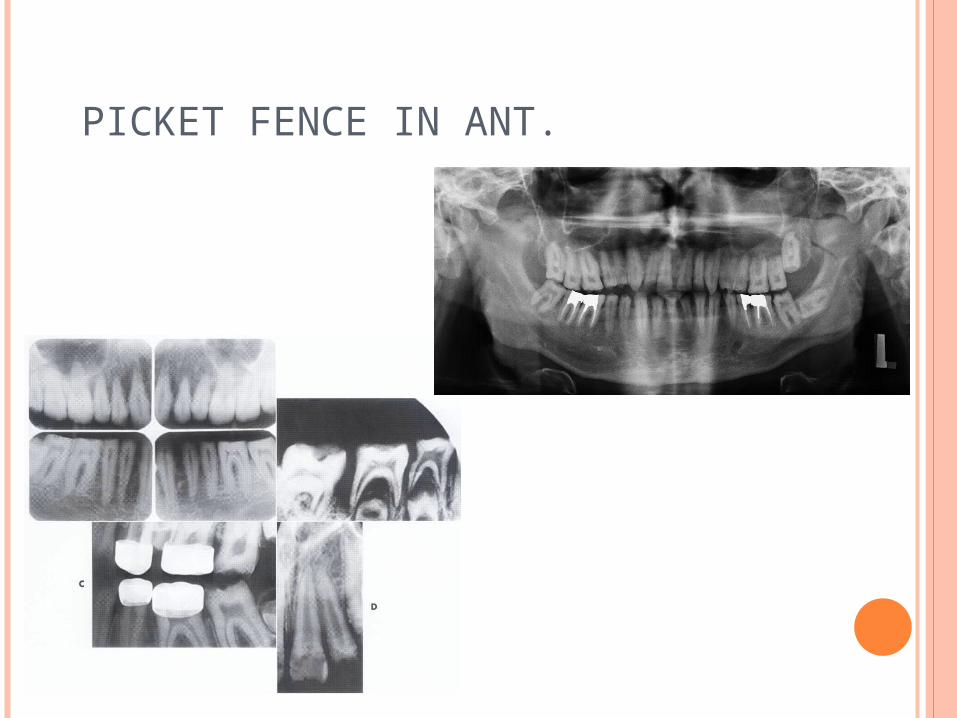
PICKET FENCE IN ANT.

enamel is normal in form on
eruption but:
softer than normal tends to chip from
underlying
dentin snow-capped" teeth
Radiographically:
affected enamel exhibits
radiodensity similar to
dentin
Hypomaturation Amelogenesis Imperfecta

enamel matrix is formed in normal quantity
poorly calcified
when newly erupted:
enamel is normal in thickness normal form but weak opaque or chalky in appearance
Hypocalcified Amelogenesis Imperfecta

with years of function:
coronal enamel is removedeven less than dentin
abrasion to gingiva
Radiographically:
density of enamel is less than dentin
Hypocalcified Amelogenesis Imperfecta

affects both primary + permanent
dentition
have blue to gray
discoloration(a result of the obliteration the pulp chamber, which normally gives a pinkish coloration to the dentin)
Dentinogenesis Imperfecta

Type Ioccurs in families with
Osteogenesis Imperfecta
Type IIonly have dentin abnormalities
and no bone disease
Dentinogenesis Imperfecta
OSTEOGENESIS IMPERFECTA
Progressive osteopenia Bone fractures Blue sclera Wormain bone Dentinogenesis imperfecta Cl III Impaction of m1, m2

Radiographically:
bulbous crowns cervical constriction thin roots early obliteration of roots canals + pulp chambers
periapical lesion with no evidence of Caries
Dentinogenesis Imperfecta

rare disturbance of dentin formation
normal enamel
atypical dentin formation
abnormal pulpal morphology
Dentin Dysplasia

Classification:
Type I (Radicular Type)
Type II (Coronal Type)
Dentin Dysplasia

short roots(shallow w)
exfuliation with little trauma
pulp obliteration before eruption
periapical lesion with no evidence of Caries
Type I (Radicular Type)
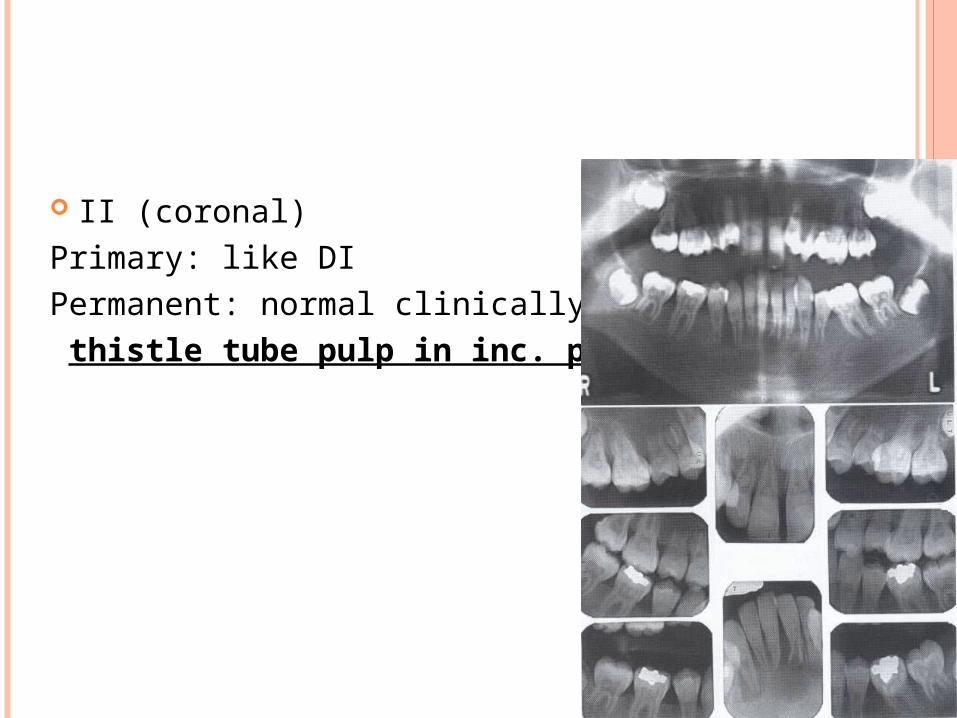
II (coronal)Primary: like DIPermanent: normal clinically thistle tube pulp in inc. pm.

coronal pulps are usually large (thistle tube appearance)
filled with globules of abnormal dentin
Type II (Coronal Type)

DIFFERENTIAL DIAGNOSIS
Thistle tube in one-root tooth ?
Tooth with out roots?
Rarefying osteitis with no caries?
Bulbus crown with cervical constriction?

Odontogenesis Imperfecta Ghost Teeth
etiology is unknown(Developmental) one or several teeth in a
localized area are affected
maxillary teeth are involved
more frequently than
mandibular area
teeth affected may exhibit
a delay or total failure in
eruption
Regional Odontodysplasia

Radiographically:
marked reduction in
radiodensity teeth assume a “ghost”
appearance both enamel + dentin appear
very thin pulp chamber is exceedingly
largeDelayed eruption
Susceptible to caries
DD: D.I.
Regional Odontodysplasia

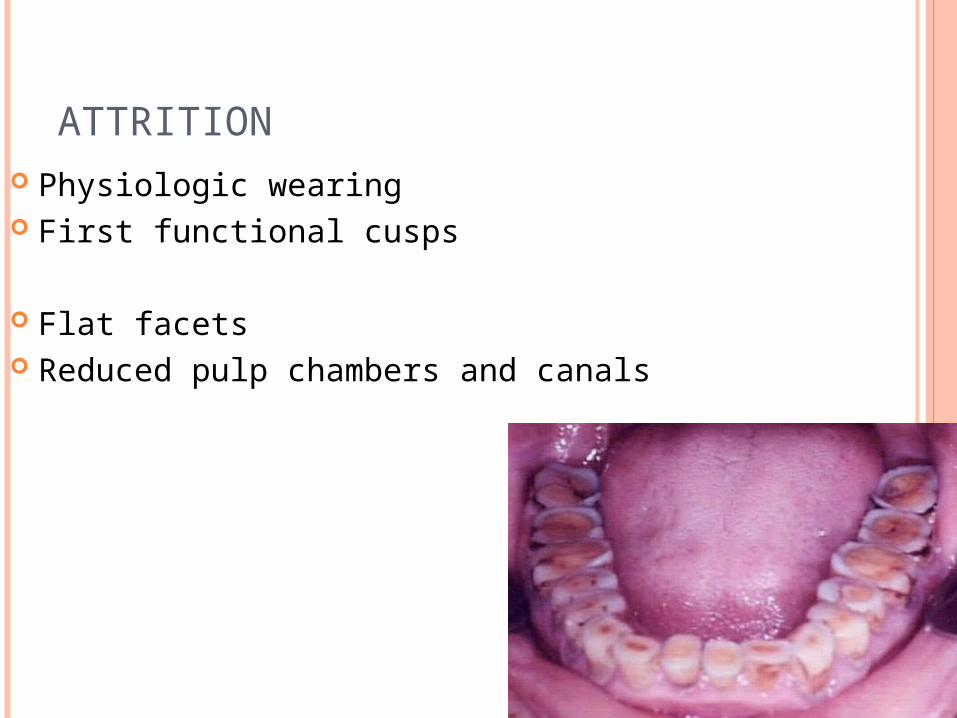
ATTRITION Physiologic wearing First functional cusps
Flat facets Reduced pulp chambers and canals

ABRASION
Brushing pm>can>inc
Dental floss deeper in dis.
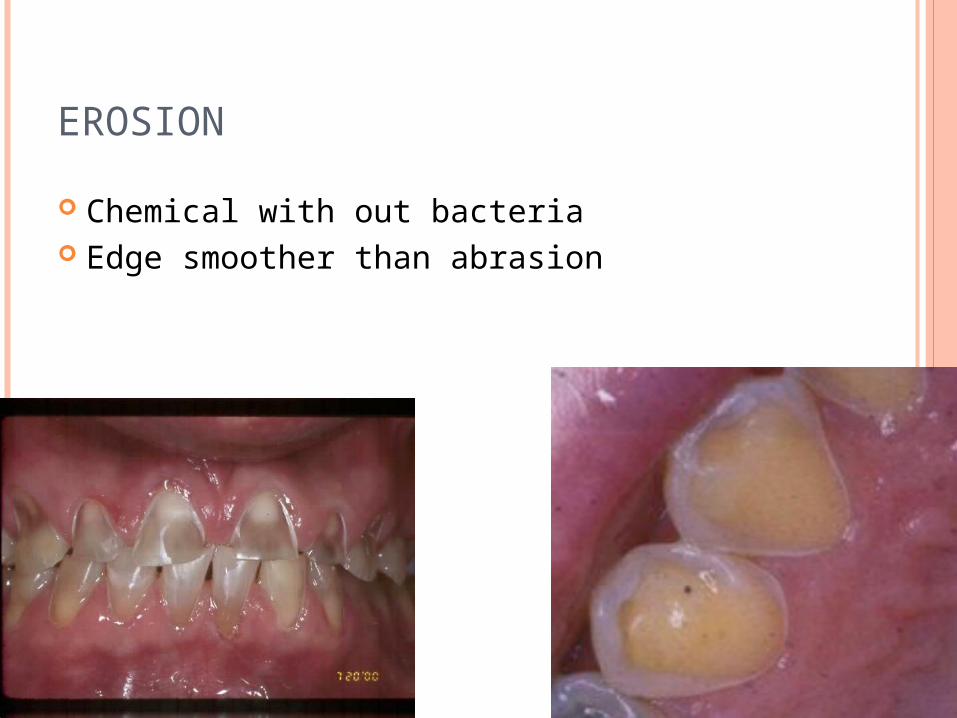
EROSION
Chemical with out bacteria Edge smoother than abrasion

INTERNAL RESORBTION
Causes: Acute trauma/direct and indirect pulp cap/pulpotomy/enamel invagination
Pink mottleD.D: Bacc/ling caries External root resorbtion
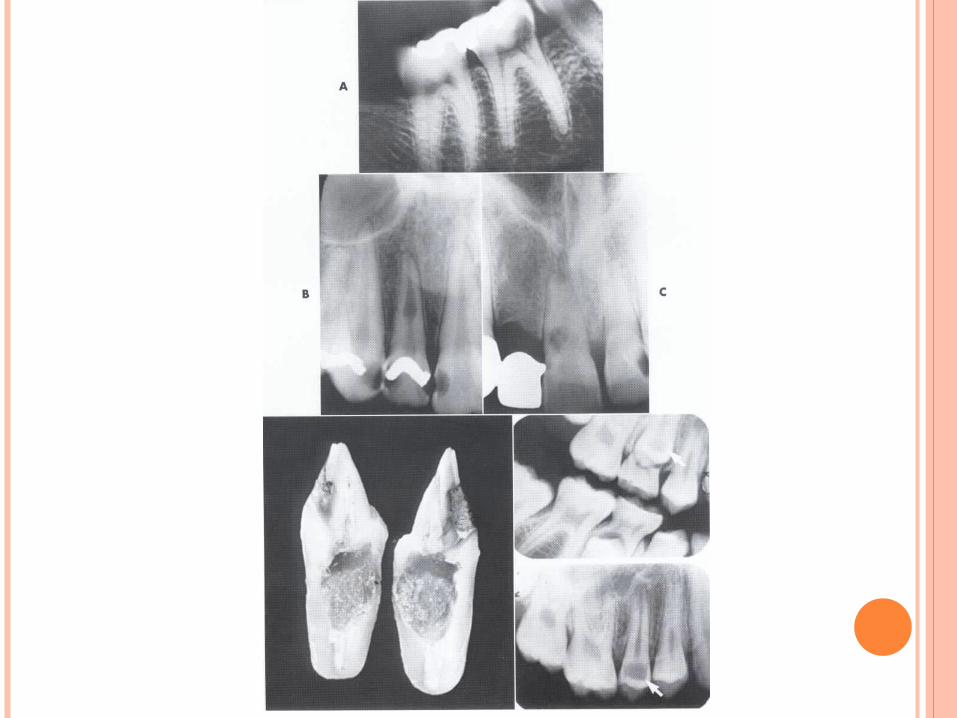

EXTERNAL ROOT RESORBTION
Tooth root Unerupted tooth crownCause: Reimplantation, local inflammation, too much
mechanical forcesFeatures:
AP Blunting Normal supporting structures
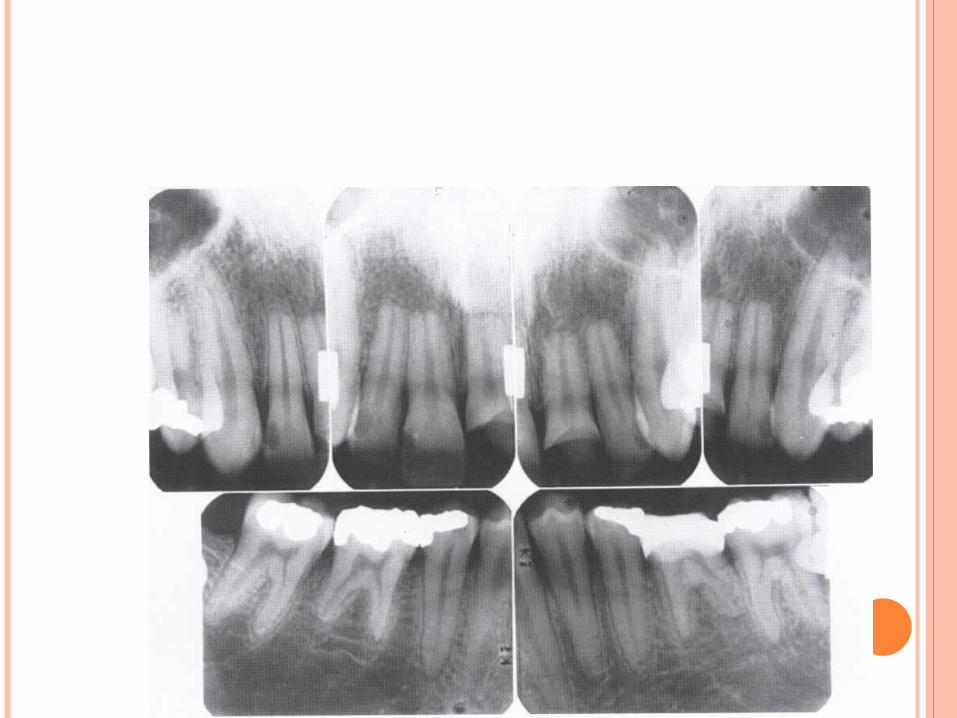

HYPERCEMENTOSISCause:Super eruption
Too much occ forces
Inflammation
Paget/gigantism and acromegaly
Related Documents











