3/1/2014 1 Dennis Spence, PhD, CRNA http://www.bing.com/images/search?q=images+of+obstructive+sleep+apnea&qpvt=images+of+obstructive+sleep+apnea&FORM=IG RE Disclaimer The views expressed in this article are those of the author and do not reflect official policy or position of the Department of the Navy, the Department of Defense, the Uniformed Services University of the Health Sciences, or the United States Government. The author does not endorse, promote or advertise any products presented in this presentation. Disclosure Nothing to disclose

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

3/1/2014
1
Dennis Spence, PhD, CRNA
http://www.bing.com/images/search?q=images+of+obstructive+sleep+apnea&qpvt=images+of+obstructive+sleep+apnea&FORM=IGRE
Disclaimer The views expressed in this article are those of the
author and do not reflect official policy or position of the Department of the Navy, the Department of Defense, the Uniformed Services University of the Health Sciences, or the United States Government.
The author does not endorse, promote or advertise any products presented in this presentation.
Disclosure Nothing to disclose

3/1/2014
2
Objectives Review the stages of sleep
Describe types of sleep disordered breathing with focus on OSA
Compare and contrast the normal and OSA airway
Describe the pathophysiology and clinical consequences of OSA
Review evidence on OSA related to:
Opioid effects
Screening
Difficult airway
PACU & Postoperative Complications
List perioperative precautions that may reduce risks in OSA patients
Clinical Vignette 56 y/o male scheduled for ex lap for sigmoid resection
PMH-HTN, obesity (BMI 48), DM II, colon cancer
PSH- none
Meds- HCTZ, metoprolol, glyburide
EKG- NSR w/ LAD, LVH Labs- wnl BP- 160/85, HR- 58
Airway- MP III, 3FB MO, TM 2.5 FB, limited ROM, neck
50 cm
+snoring, +daytime somnolence, witnessed apnea by wife
Clinical Vignette What is the likelihood that this patient has
undiagnosed OSA?
If he has OSA, how severe is it?
What other comorbidities might he have secondary to his OSA?
Is he a potentially difficult airway?
Does having OSA increase his risks for perioperative complications?
What perioperative OSA precautions can I use to minimize his risks?

3/1/2014
3
Stages of Sleep Non-REM (non-rapid eye mvt)
3 stages
Stage 3 physically restorative sleep
Stage 3reduced muscle tone
REM
Most muscles paralyzed/relaxed
Potential collapse of upper airway
Lack of REM may impair ability to learn complex tasks
Sleep impairment
interferes w/ growth patterns, memory, healing, & immune response
http://www.bing.com/images/search?q=images+of+stages+of+sleep&go=&qs=bs&form=QBIR
Types of Sleep Disordered Breathing
Apnea
Cessation of airflow > 10 seconds
Hypopnea
Decreased airflow >30% for > 10 seconds associated with:
Oxyhemoglobin desaturation ≥4%
Arousals
Apnea Patterns Obstructive Mixed Central
Airflow
Respiratory
effort
American Academy of Sleep Medicine. Sleep Apnea: Diagnosis and Treatment Sleep Medicine Professional Education slides. 2006.

3/1/2014
4
OSA Definition
Characterized chronic, frequent events of airway obstruction during sleep Sxs: snoring, witnessed apnea, & daytime sleepiness
Secondary HTN
During sleep OSA patients experience: Frequent episodes of apnea and/or hypopnea
Frequent oxygen desaturation
Chronic hypercarbia and hypoxemia
Frequent Arousals
Reduced Non-REM Stage 3 & REM sleep
OSA Risk Factors
Male gender
Obesity (BMI>29) present in 60-90% of OSA pts
Non-obese craniofacial & orofacial abnormalities (i.e, enlarged
tonsils)
Family hx
Large neck circumference (>17 in male, >16 in female)
Smoking and alcohol use
Medications-sedatives, opioids
Measures of Sleep Apnea Frequency Polysomnography
Gold standard for diagnosis of OSA
Apnea Index
# apneas per hour of sleep
Apnea / Hypopnea Index (AHI)
# apneas + hypopneas per hour of sleep
Oxygen desaturation index (ODI)
Number of desaturations of ≥4% per hour of sleep
ODI of >5 high likelihood of OSA

3/1/2014
5
Severity of OSA AHI
None 0-5
Mild 6-15
Moderate 16-30
Severe >30
Obstructive Apnea EEG
10 sec
Arousal
Airflow
Effort (Pes)
SaO2
Effort (Abdomen)
Effort (Rib Cage)
American Academy of Sleep Medicine. Sleep Apnea: Diagnosis and Treatment Sleep Medicine Professional Education slides. 2006.
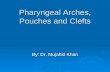
Normal Airway
Retropalatal (RP)
from the level of the hard palate to the caudal margin of the soft palate
Retroglossal (RG)
from the caudal margin of the soft palate to the base of the epiglottis
Schwab et al. Am J Respir Crit Care Med. 2003 168; 522–530.

3/1/2014
6
OSA Airway Decreased pharyngeal area 2nd excess adipose tissue
Uvula, tonsillar pillars, tongue, lateral pharyngeal walls
MRI study- Large tongue and increased volume of lateral pharyngeal walls risk factors for OSA
Increased extramural pressure compresses airway (i.e., large neck)
Schwab et al. Am J Respir Crit Care Med. 2003 168; 522–530.
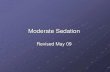
OSA Airway OSA Normal
Schwab et al. Am J Respir Crit Care Med. 2003 168; 522–530.
Normal vs. OSA Airway
Larger
smaller
airway
Schwab et al. Am J Respir Crit Care Med. 2003 168; 522–530.

3/1/2014
7
OSA = airway smaller & lateral pharyngeal walls larger
OSA Airway
Schwab et al. Am J Respir Crit Care Med. 2003 168; 522–530.
http://www.bing.com/images/search?q=images+of+obstructive+sleep+apnea&qpvt=images+of+obstructive+sleep+apnea&FORM=IGRE
OSA Airway During Sleep
Spence DL. Anesthesia for Uvulipharyngopalatoplasty. In Clinical Cases in Nurse Anesthesia, Ed.: Elisha, S. Jones and Bartlett; Sudbury, MA. 2010: pp. 53-61.

3/1/2014
8
Vicious Cycle of OSA
Loss of neuromuscular
compensation
+ Decreased pharyngeal
muscle activity
Sleep Onset
Hyperventilate: correct
hypoxia & hypercapnia
Airway opens
Airway collapses
Pharyngeal muscle
activity restored
Apnea Arousal from sleep
Hypoxia &
Hypercapnia
Increased ventilatory
effort
American Academy of Sleep Medicine. Sleep Apnea: Diagnosis and Treatment Sleep Medicine Professional Education slides. 2006.
Clinical Consequences
Moos DD, Prasch M, Cantral DE, Huls B, Cuddeford JD. Are patients with obstructive sleep apnea syndrome appropriate candidates for the ambulatory surgical center? AANA J. 2005;73(3):197-205.
Co-existing diseases/symptoms associated with OSA
Cardiovascular Neuropsychological Endocrine/Other
Hypertension
Arrhythmias:
o Atrial
Fibrillation
o Bradycardia
o A-V Block
CAD
Nocturnal angina
MI
CHF
CVD
Pulmonary HTN
Daytime
somnolence
Cognitive
Impairment
Accident proneness
Anxiety
Depression
Glucose Intolerance and
Diabetes
Obesity
Gastroesphogeal Reflux
Disease
Difficult airway
Adapted from Spence DL. Anesthesia for Uvulipharyngopalatoplasty. In Clinical Cases in Nurse Anesthesia, Ed.: Elisha, S. Jones and Bartlett; Sudbury, MA. 2010: pp. 53-61.

3/1/2014
9
OSA Prevalence
Prevale
nce
AHI >
5
Mod-S
ev Undx O
SA
0
20
40
60
80
100Men
Women
pe
rce
nta
ge
of
pa
tie
nts
(%
)
Adapted from Young T et al. N Engl J Med 1993;328.
Wisconsin Sleep Cohort Study
4% 2%
24%
9%
82%
93%
How Well Do We Do?
Screening Surgical Patients for OSA
Polysomnography considered gold standard Problem- difficult to obtain; expensive
Allows for initiation of CPAP therapy
Questionnaire screening tools ASA OSA checklist
Berlin Questionnaire
STOP-BANG
Combination of questionnaire + home sleep study

3/1/2014
10
ASA Checklist Screens & estimates risk (12 items)
High-risk = (+) ≥2 more categories
Invasiveness of surgery
Postop opioid requirements
AHI ≥ 5
Sensitivity = 72%
Specificity = 38%
AHI ≥ 15
Sensitivity = 79%
Specificity = 37%
Abrishami et al. A systematic review of screening questionnaires for obstructive sleep apnea Can J Anesth (2010) 57:423–438
Berlin Questionnaire Most widely used in primary care
11 questions in 3 categories Obstructive sxs
Daytime sleepiness
HTN hx
AHI ≥ 5 Sensitivity = 69%
Specificity = 56%
AHI ≥ 15 Sensitivity = 79%
Specificity = 51%
Abrishami et al. A systematic review of screening questionnaires for obstructive sleep apnea Can J Anesth (2010) 57:423–438
STOP-BANG Questionnaire
8 item screening tool for surgical patients
≥3 high risk OSA
AHI ≥ 5
Sensitivity = 84%
Specificity = 56%
AHI ≥ 15
Sensitivity = 93%
Specificity = 43%
Chung et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008;108:812-821

3/1/2014
11
STOP-BANG Does a higher score predict more severe OSA?
Table 1. Odds of OSA based on STOP-Bang Score
STOP-Bang score All OSA (AHI>5) Mod/Sev OSA (AHI>15) Severe OSA (AHI >30)
5 3.98 (2.38-6.66) 4.75 (2.81-8.03) 10.39 (4.45-24.26)
6 4.52 (2.34-8.74) 6.29 (3.39-11.66) 11.55 (4.64-28.71)
7 or 8 7.04 (2.82-17.55) 6.88 (3.32-14.25) 14.86 (5.58-39.56)
N = 746
STOP-BANG = 5 were 10x more likely to have Sev OSA vs. score <3
Score of 5 = Specificity 74% for Sev OSA
Chung et al. High STOP-BANG score indicates a high probability of obstructive sleep apnea Br J Anaesth 2012;108:768-75
Does STOP-BANG Predict Postop Complications? Vasu et al 2010 N = 135 surgical patients
STOP-BANG score ≥ 3 vs. ≤ 3
Outcomes = composite postop complications
Afib, hypotension, MI, hypoxemia, PE, pneumonia
Results for STOP-BANG ≥ 3
Odds: 11.4x more postoperative complications (P = 0.03)
Vasu TS et al Arch Otolarynglol Head Neck Surg; 2010;136(10):1020-4
How Common is OSA in Surgical Patients? Finkel et al (2008)
N = 2778 surgical pts
OSA screening questionnaire
High-risk pts sleep study
Compared high vs. low risk
Results
OSA prevalence = 22%
82% never diagnosed
High-risk = >BMI, >Neck circ., >HTN, >DM
Finkel et al. Sleep Medicine. 2009;10:753-58 Spence DL. Anesthesia Abstracts 2011;(5)9: 19-22.
Home Sleep Study Results (n = 207)

3/1/2014
12
How Common is OSA is Surgical Patients?
STOP-BANG study
N = 2721 surgical patients
STOP-BANG + sleep study
Results
High-risk (≥3)= 28%
OSA In
cidence
(AH
I >5)
Mild
OSA (A
HI >
5)
Modera
te O
SA (AH
I >15
)
Severe O
SA (AH
I >30
)
0
20
40
60
80
100
Sleep Study Results
N = 122
pe
rce
nta
ge
of
pa
tie
nts
(%
)
Chung et al. Anesthesiology 2008;108:812-821 Spence DL. Anesthesia Abstracts 2011;(5)9: 12-15.
How Common is OSA is GI Patients?
ERCP OSA Study
N = 231 ERCP patients
Used STOP-BANG
Results
High-risk (≥3)= 43%
>MP score, >ASA class, >age, >BMI, >male gender
Coté GA et al. Clin Gastroenterol Hepatol 2010;8:660-665
EBP STOP-BANG Projects Does incorporation of the STOP-BANG increase our ability to
identify patients at high risk for OSA?
Method
Baseline: measure incidence of high risk OSA
Educated nurses & implemented STOP-BANG
Post: measured incidence of high risk OSA (score ≥3)
Before
After
Before
After
0
10
20
30
Williams et al (2012)
Lakdawala (2011)
High-risk for OSA
pe
rce
nta
ge
of
pa
tie
nts
(%
)
Lakdawala L. J Perianesthesia Nurs. 2011. 26(1): 15-24 Williams et al. 2012. Presented at AANA State of Science Aug 2012.

3/1/2014
13
Challenges with Screening Incorporated into EMR &
preop workflow
Auto-calculated score
Score 5 to flag as high risk
8 months = 12,500 necks measured
Implementing auto-sleep study referral not possible
“Altering medical assistant and nurse practitioner workflows in the clinic was straightforward…. …but changing our anesthesia providers’ workflow has not yet been successful. While some of the variables can be derived from demographics and patient history, ... …obtaining neck circumference measurements and asking the additional screening questions adds extra time …..”
Robert Stoelting, MD, President, Anesthesia Patient Safety Foundation: “Clinically significant drug-induced respiratory depression (oxygenation and/or ventilation) in the postoperative period remains a serious patient safety risk that continues to be associated with significant morbidity and mortality.”
•JC Screen patients for respiratory depression risk factors (see sidebar).
Preoperative Implications OSA prevalence 22-43%
>80% of patients have OSA and don’t know it
Have high index of suspicion for coexisting diseases HTN, CAD, DM, atrial fibrillation
Difficult airway
Should develop screening process for undiagnosed OSA Polysomnography & initiation of CPAP when possible
Use the STOP-BANG
Requires multidisciplinary team, buy-in & support at all levels

3/1/2014
14
“Anesthesia Providers could potentially impact a significant public health burden and reduce the percentage of undiagnosed OSA patients in major ways: proper implementation of screening guidelines, optimization of interventional therapy (e.g., CPAP) perioperatively and ensuring follow up by sleep physician postoperatively” “Our Role does not stop within the confines of the operating room or the PACU. “ “Specialist sleep physician referral and appropriate therapy are crucial in long term cardiac and cerebrovascular outcomes”….
Society of Anesthesia & Sleep Medicine , Volume 3, Issue 1 w 2014
Opioids & OSA OSA sleep study (N = 19 moderate OSA, AHI>15-30)
Continuous remifentanil infusion in sleep lab
Results
Only 20% experienced REM sleep (P < 0.05)
Increased # arousals vs. baseline study
AHI increased (44 ± 29 vs. 24 ± 5, P = NS)
#obstructive apneas lower(4 ± 6 vs. 8 ± 5, P = NS)
#hypopneas increased (22 ± 16 vs. 15 ± 6, P = NS)
#Central apneas increased (17 ± 29 vs., 0.4 ± 1 P < 0.05)
Bernards CM et al. Anesthesiology 2009;110: 41-49
Opioids & OSA
Lowest SaO2= Baseline = 87 ± 4% Remifentanil = 80 ± 5% P< 0.05
Bernards CM et al. Anesthesiology 2009;110: 41-49 Spence DL. Anesthesia Abstracts 2011;(5)9: 7-12.

3/1/2014
15
Opioids & OSA Opioids reduce REM sleep
decreases # of obstructive apneas REM sleep is when airway most relaxed # central apneas may increase (no stimulus to breathe) REM rebounds in 48-72hrsworsening of OSA sxs*
Hypoxemia & hypercarbia may have triggered increased # arousals & reduced obstructions
Hypoxemia incidence and severity worse on remifentanil
Implication Be cautious when administering opioids to OSA patients
*Lao P, Sun F, Amirshahi B, Islam S, Vairavanathan S, Shapiro C, Chung F. A significant exacerbation of sleep breathing is OSA patients
undergoing surgery with general anesthesia. Sleep 2009;32: A223.
OSA & Difficult Airway
http://www.bing.com/images/search?q=images+of+obstructive+sleep+apnea&qpvt=images+of+obstructive+sleep+apnea&FORM=IGRE
Are Patients with OSA more Difficult to Ventilate?
Kheterpal S et al Prediction and Outcomes of Impossible Mask Ventilation: A Review of 50,000 Anesthetics. Anesthesiology. 110(4):891-897, April 2009
Predictors of Impossible Mask Ventilation
Odds ratio
Neck radiation changes 7.1
Male sex 3.3
Sleep apnea 2.4
MP III or IV 2
Beard 2
Patients with ≥ 3 of these risk factors were 8.9x more likely to be impossible to mask ventilate

3/1/2014
16
Are Patients with OSA more Difficult to Intubate?
Palatal muscle resection for OSA (N = 115) (Lee et al 2011)
20% difficult intubation (DI) rate
Predictors Large neck ≥ 40 cm
AHI≥50
UPPP (N = 180) (Kim et al 2006)
OSA vs. no OSA
DI rate: 16.6% vs. 3.3%
Spence DL. Anesthesia Abstracts 2011;(5)9: 30-33.
OSA & Difficult Intubations Bariatric Surgery observational study (N = 180)
78% female, BMI = 49.4 ± 7.6, median OSA severity = mild
Median MP score = MP 2, neck circumference = 43.8 ± 5.4 cm
Results
DI rate = 3.3%
No relationship between OSA dx and difficult intubation in bariatric pts(P = NS)
Predictors of DI = >MP 2 & male gender
Larger neck = poorer glottic view
Meligan et al Anesth Analg 2009;109: 1182-1186
Implications Men with severe OSA & large necks at greatest risk
Airway surgery for OSA may be risk
Be prepared for difficult mask and intubation!
Ramp obese pts & optimize sniffing position
Backup device (indirect video laryngoscopy, LMA)
Call for help early!
Consider AFOB

3/1/2014
17
Sedation & OSA Cohort study N = 231
ERCP/EUS
High vs. Low risk OSA (STOP-BANG)
CRNA = propofol +/- opioid/midazolam
Outcomes = Airway maneuvers
sedation related complications
High-risk OSA 1.6x more likely to experience SAO2<90%
Coté GA et al Clin Gastroenterol Hepatol 2010;8:660-665 Spence DL. Anesthesia Abstracts 2011;(5)9: 22-26.
PACU & Suspected OSA Cohort study N = 693 surgical Non-OSA dx patients
High vs. Low-Risk OSA
Outcome = recurrent PACU respiratory complications <90% with nasal cannula; 3 episodes needed for yes
Results 32% high-risk for OSA
>1 event of SaO2 <90% = 28% vs. 11%, P < 0.001
High-risk OSA = 3.5x more likely postop resp. event
21x more likely experience recurrent PACU events
2.7x more likely experience postop complication
Unplanned ICU admission = 27% vs. 8%
Gali et al. Anesthesiology 2009;110:869-876
PACU & Suspected OSA
High-risk OSA = more likely to experience recurrent desaturation Gali et al. Anesthesiology 2009;110:869-876 Spence DL. Anesthesia Abstracts 2011;(5)9: 39-44.

3/1/2014
18
Implications- PACU Desaturation most common complication
What about hypercarbia?
Points to need to have plan for high-risk OSA pts ICU vs. Step-down unit
Question: Should OSA pts have continuous ETCO2 & SaO2
monitoring?
Severity?
Gali et al. Anesthesiology 2009;110:869-876
OSA & Postop Complications Case-control study of TKA surgery pts
clinically suspected or diagnosed OSA pts vs. control (N = 202)
Respiratory complications = 28% vs. 10%, P = 0.019
Note. Serious complications were defined as complications necessitating transfer to the
ICU for cardiac events or urgent respiratory support with need for intubation or CPAP. undx OSA vs. dx OSA =
Total complications = 32% vs. 3%, P <0.05 Gupta et al. Mayo Clin Proc 2001;76:897-905 Spence DL. Anesthesia Abstracts 2011;(5)9:.
OSA & Postop Complications
Liao P et al. Postoperative complications in patients with obstructive sleep apnea: a retrospective matched cohort study. Can J Anesth 2009;56:819-828
Spence DL. Anesthesia Abstracts 2011;(5)9.
N = 240
N = 240

3/1/2014
19
OSA & Postop Complications
Liao P et al. Postoperative complications in patients with obstructive sleep apnea: a retrospective matched cohort study. Can J Anesth 2009;56:819-828
OSA group (N = 240) • 2x increased risk of postop complication • 27% require CPAP 2nd hypoxemia • Complications occurred more often after
transfer to ward • CV & neuro complications same • 2 vs. 1 cardiac arrests in OSA pts
• 2 for difficult intubation/reintubation
OSA & Postop Complications
• National Inpatient Sample OSA Study N = 3,441,262
21. Memtsoudis S et al. Perioperative pulmonary outcomes in patients with sleep apnea after noncardiac surgery. Anesth Analg 2011;112: 113-121.
OSA & Postop Complications • National Inpatient Sample OSA Study N = 3,441,262
Table 1. Odds of Postoperative pulmonary complications in OSA patients
General surgery
Aspiration pneumonia
ARDS
PE
Intubation/mechanical ventilation
1.37 (1.33-1.41)
1.58 (1.54-1.62)
0.90 (0.84-0.97)
1.95 (1.91-1.98)
Orthopedic
Aspiration pneumonia
ARDS
PE
Intubation/mechanical ventilation
1.41 (1.35-1.47)
2.39 (2.28-2.51)
1.22 (1.15-1.29)
5.20 (5.05-5.37)
Note. Results are odds ratio (95% confidence interval). All are significant (P < 0.05).
21. Memtsoudis S et al. Perioperative pulmonary outcomes in patients with sleep apnea after noncardiac surgery. Anesth Analg 2011;112: 113-121.

3/1/2014
20
Non-SDB group • Higher Hospital charges,
• $39,977 vs. $37,934, P < 0.001 • Slightly higher mortality
• 0.3% vs. 0.1%, P 0.001 • Longer LOS
• 7.1 days vs. 5.8 days, P < 0.01
Why???? • Higher vigilance in those dx w/ OSA?
• Some Non-SDB group could have had
undiagnosed OSA?
Does Technique Matter?
• Neuraxial anesthesia +/- GA associated with improved outcomes
• Reduced odds of major complications, requirement for critical care admission (especially for neuraxial anesthesia alone), or mechanical ventilation
• Associated with reduced hospital length of stay and costs.
• Randomized N = 177 OSA patients (AHI>15) to auto-titrated CPAP • started 3 days prior to surgery or routine care
• CPAP significantly reduced postoperative AHI • Low compliance
• <48% of patients used the CPAP >4h per night

3/1/2014
21
CPAP adherence in patients with newly diagnosed obstructive sleep apnea prior to elective surgery. Guralnick AS, Pant M, Minhaj M, Sweitzer BJ, Mokhlesi B. Methods: Pre-surgical patients who screened positive for OSA on the STOP-Bang questionnaire and underwent PSG before surgery. CPAP was offered to patients with moderate or severe OSA. Results: Median Adherence only 2.5 h/n Conclusion: Adherence to prescribed CPAP therapy during the perioperative period was extremely low.
J Clin Sleep Med. 2012 Oct 15;8(5):501-6
Postoperative Implications Known or suspected OSA patients increased risk for
postoperative pulmonary/respiratory complications
Hypoxemia
Need for higher level of care
CPAP improves postop AHI, but compliance poor
Neuraxial improved outcomes reduced costs
Mod-Sev OSA may need continuous ETCO2 +/- SPO2
Smart Pump Technology
Patient Surveillance systems
OSA During Pregnancy Home sleep study
N = 161 obese parturients @21 w
BMI > 30 kg/m2
AHI >5 vs. AHI <5
Outcomes
Perinatal outcomes
Predictors of preeclampsia
controlled for BMI, age, diabetes
Results
OSA incidence = 15%
Age
30±6 vs. 27±6 (P = 0.04)
Prepregnancy BMI
48±11 vs. 39±6 (P <0.001)
CHTN
58% vs. 33% (P = 0.02)
Asthma
50% vs. 31% (P = 0.005)
Louis J et al. Perinatal Outcomes Associated With Obstructive Sleep Apnea in Obese Pregnant Women. Obstet Gynecol 2012;120:1085–92

3/1/2014
22
OSA during Pregnancy Predictors of preeclampsia
3.5x more likely w/ OSA
2.8x more likely w/ previous preeclampsia
4.3x more likely w/CHTN
OSA No OSA0
20
40
60
80
100Cesarean Delivery
Preeclampsia
Wound Complications
NICU Admission
Hyperbilirubinemia
All P < 0.05
per
cen
tag
e o
f p
ati
ents
(%
)
Perioperative OSA Precautions • Need to ID those with known or suspected OSA (especially moderate-severe)
• Minimize preoperative sedation
• Prepare for possible difficult airway
• Minimize use of long acting opioids. Consider utilizing multimodal analgesic techniques
and regional anesthesia when possible
• Utilize short acting inhaled or intravenous anesthetics intraoperatively
• Utilize capnography during monitored anesthetic care
• Ensure patient is full reversal of neuromuscular blockade. Ensure patient is fully
conscious and cooperative prior to extubation
• Utilize non-supine posture for extubation and recovery
• Resume or consider use of CPAP therapy in patients with OSA
• Have plan for postop monitoring. Consider continuous ETCO2 +/- SPO2
Seet E, Chung F. Management of sleep apnea in adults- functional algorithms for the perioperative period: continuing professional development. Can J Anesth. 2010;57: 849-65.
Society of Ambulatory Anesthesia Consensus Guidelines 2012
• Recommend screening with STOP-BANG & presume patient has OSA based on sxs
• Literature unclear of benefit of sleep study or CPAP on postop outcomes
• Non-optimzed patients may not be suitable for ambulatory surgery
• Optimal duration of CPAP therapy prior to surgery unknown
• Recommend nonopioid analgesic/multimodal techniques especially for painful ambulatory surgery
• Encourage patients w/ OSA to use CPAP postop whenever sleep
• Educate surgeons, patient and family on minimizing opioids, use of CPAP, and sleeping in lateral position
• Patients should f/u with primary care MD for sleep study postop if identified as high risk
for OSA based on STOP-BANG
Joshi et al. Anesthesia & Analgesia. 115(5):1060-1068, November 2012.

3/1/2014
23
Joshi et al. Anesthesia & Analgesia. 115(5):1060-1068, November 2012.
References 1. American Academy of Sleep Medicine. Sleep Apnea: Diagnosis and Treatment Sleep Medicine Professional Education slides. 2006. 2. Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth Analg. 2008;107(5):1543-1563. 3. Spence DL. Anesthesia for Uvulipharyngopalatoplasty. In Clinical Cases in Nurse Anesthesia, Ed.: Elisha, S. Jones and Bartlett; Sudbury, MA. 2010: pp. 53-61. 4. Schwab et al. Identification of upper airway anatomic risk factors for obstructive sleep apnea with volumetric magnetic resonance imaging. Am J Respir Crit Care Med. 2003 168; 522–530. 5. Horner RL. Respiratory motor activity: influence of neuromodulators and implications for sleep disordered breathing. Can J Physiol Pharmacol 2007;85: 155-165. 6. Metzner J, Posner KL, Domino KB. The risk and safety of anesthesia at remote locations: the US closed claims analysis. Curr Opin Anesthesiol 2009;22: 502-508. 7. Chung F, Yegnesaran B, Liao P et al. Validation of the Berlin Questionnaire and American Society of Anesthesiologists Checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology 2008;108:822-830. 8. Chung F et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008;108: 812-821. 9. Lakdawala L. Creating a safer perioperative environment with an obstructive sleep apnea screening tool. J Perianesthesia Nurs. 2011. 26(1): 15-24.

3/1/2014
24
References 10. Bernards CM, Knowlton SL, Schmidt DF, DePaso WJ, Lee MK, McDonald SB, Bains OS. Respiratory and sleep effects of remifentanil in volunteers with moderate obstructive sleep apnea. Anesthesiology 2009;110: 41-49.
11. Chung et al. High STOP-BANG score indicates a high probability of obstructive sleep apnea Br J Anaesth 2012;108:768-75.
12. Finkel et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Medicine. 2009;10:753-58.
13. Gross et al. Practice guidelines for the perioperative management of patients with obstructive sleep apnea: a report by the American Society of Anesthesiologists Task Force on Perioperative Management of patients with obstructive sleep apnea. Anesthesiology 2006;104: 1081-93.
14. Coté GA, Hovis CE, Waldbaum L et al. A screening instrument for sleep apnea predicts airway maneuvers in patients undergoing advanced endoscopic procedures. Clin Gastroenterol Hepatol 2010;8:660-665.
15. Kheterpal S, Martin L, Shanks AM, Tremper KK. Prediction and outcomes of impossible mask ventilation: review of 50,000 anesthetics. Anesthesiology 2009;110:891-897.
16. Lee SJ, Lee JM, Kim TS, Park YC. The relationship between the predictors of obstructive sleep apnea and difficult intubation. Korean J Anesthesiol 2011;60: 173-178.
References 17. Kim JA, Lee JJ. Preoperative predictors of difficult intubation in patients with obstructive sleep apnea syndrome. Can J Anesth 2006;53: 393-397. 18. Meligan PJ, Porter S, Max B, Malhotra G, Greenblatt EP, Ochroch EA. Obstructive sleep apnea is not a risk factor for difficult intubation in morbidly obese patients. Anesth Analg 2009;109: 1182-1186. 19. Moos DD, Prasch M, Cantral DE, Huls B, Cuddeford JD. Are patients with obstructive sleep apnea syndrome appropriate candidates for the ambulatory surgical center? AANA J. 2005;73(3):197-205. 20. Rao SL, Kunselman AR, Schuler GH, DesHarnais S. Laryngoscopy and tracheal intubation in the head-elevated position in obese patients: a randomized, controlled, equivalence trial. Anesth Analg 2008;107: 1912-1918. 21. Memtsoudis S et al. Perioperative pulmonary outcomes in patients with sleep apnea after noncardiac surgery. Anesth Analg 2011;112: 113-121. 22.Vasu TS, Dogharmji K, Cavallazzi R et al. Obstructive sleep apnea syndrome and postoperative complications: clinical use of the STOP-BANG questionnaire. Arch Otolaryngol Head Neck Surg 2010;136: 1020-1024. 23. Gali B, Whalen FX, Schroeder DR, Gay PC, Plevak DJ. Identification of patients at risk for postoperative respiratory complications using a preoperative obstructive sleep apnea screening tool and postanesthesia assessment. Anesthesiology 2009;110:869-876. 24. Gupta RM, Parvizi J, Hanssen AD, Gay P. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement: a case-control study. Mayo Clin Proc 2001;76:897-905. 25. Seet E, Chung F. Management of sleep apnea in adults- functional algorithms for the perioperative period: continuing professional development. Can J Anesth. 2010;57: 849-65.
References 26. Lao P, Sun F, Amirshahi B, Islam S, Vairavanathan S, Shapiro C, Chung F. A significant exacerbation of sleep breathing is OSA patients undergoing surgery with general anesthesia. Sleep 2009;32: A223.
27. Liao P et al. Postoperative complications in patients with obstructive sleep apnea: a retrospective matched cohort study. Can J Anesth 2009;56:819-828
28. Joshi et al. Society for Ambulatory Anesthesia Consensus Statement on Preoperative Selection of Adult Patients with Obstructive Sleep Apnea Scheduled for Ambulatory Surgery. Anesth Analg. 2012. 115(5):1060-106.
29. Louis J et al. Perinatal Outcomes Associated With Obstructive Sleep Apnea in Obese Pregnant Women. Obstet Gynecol 2012;120:1085–92
Related Documents