Demographic Perspectives on Female Genital Mutilation

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Demographic Perspectives on Female Genital Mutilation

2

Table of contents
1. Introduction 6
2. ADemographicOverviewofFGMPrevalentCountries 10
2.1 YoungPopulationAgeStructures 12
2.2 HighLevelsofFertility 15
2.3 HighLevelsofMortality 18
2.4 UrbanizationandMigration 20
2.5 FGMandOtherFormsofViolenceagainstGirlsandWomen 22
3. LevelsandTrends 26
3.1 GlobalEstimatesandCountryPrevalence 27
3.2 Trends:IsthePracticeChanging? 30
3.3 CaseStudies:TrendsandDisparitiesinBurkinaFasoandGuinea 33
4. Projections 40
5. ConclusionandtheWayForward 50
3

Foreword
Femalegenitalmutilation(FGM)
isthepracticeofpartiallyortotally
removingtheexternalgenitalorgans
fornon-medicalreasons.Itviolatesthe
humanrightsofgirlsandwomen,and
causesseriousand,insomecases,
life-threateninghealthcomplications.
In2012,theUnitedNationsGeneralAssemblypassedresolution67/146onintensifyingglobaleffortsfortheeliminationoffemalegenitalmutilations,reaffirmedbyresolution69/150in2014.TheHumanRightsCouncilin2014passedresolution27/22onintensifyingglobaleffortsandsharinggoodpracticestoeffectivelyeliminatefemalegenitalmutilations.ThesecommitmentsbyUnitedNationsMemberStatesreflectanunprecedentedawarenessofthepracticeandgrowingeffortstostopit.Globalconsensusisclear;FGMmustend.
Accurateandcurrentdataareessentialforpolicymakersandadvocatestobuildoncurrentmomentum,developsuccessfulinterventionsandachievecommitmentsmadebyUNMemberStates.
DataoncurrentprevalencelevelsandprojectionsofFGMtrendsareimperative,asisaccurateandup-to-dateinformationonpopulationchanges,includingurbanizationandresultingshiftsinpractisingpopulations.Trackingratesofreductionandprogressofchangeisnecessarytoinformongoingandfutureinterventions,andtoidentifywhathasbeensuccessfulandwhere.
Thisreport,thefirstsuchpublishedbytheUnitedNationsPopulationFund(UNFPA),looksatFGMthroughthelensofpopulationdynamicsandthedemographicdividend,basedoncurrentevidenceanddata.Itoffersquantitativeinformationthatbothsupportsevidence-basedprogramming,andframesfinancialimplicationsforMemberStatesandinternationaldonors.Evidencetodefinethesizeofthetargetpopulationandorientactionsaroundareasofgreatestimpactisofhighvalueindevelopinginterventionsandformulatingpolicies.
UNFPAremainsstronglycommittedtoengagingwithMemberStates,civilsociety,UNagenciesandallotherstakeholderstoacceleratetheeliminationofFGMworldwide.Protectinggirlsupholdstheirsexualandreproductivehealthandrights,andenablesthemtorealizetheirfullpotential.
BenoitKalasaDirector,TechnicalDivision,UNFPA
4


1Introduction

TheresolutionreaffirmsthatFGMis“aharmfulpracticethatconstitutesaseriousthreattothehealthofwomenandgirls,includingtheirpsychological,sexualandreproductivehealth,whichcanincreasetheirvulnerabilitytoHIVandmayhaveadverseobstetricandprenataloutcomesaswellasfatalconsequencesforthemotherandthenewborn,andthattheabandonmentofthisharmfulpracticecanbeachievedasaresultofacomprehensivemovementthatinvolvesallpublicandprivatestakeholdersinsociety,includinggirlsandboys,womenandmen.”1
TheresolutiondemonstratesdeepconcernsaboutthepersistenceofFGM,indicatingincreasinginternationalcommitmenttoabandonmentofthepractice.Butsofar,afundingshortfallhaslimitedthescopeandpaceofprogrammestoachieveelimination.
FGMisadeeplyingrainedculturalpracticewithdevastatingmedical,social,emotional,legalandeconomicrepercussionsforyounggirlsandwomen.Itreferstoallproceduresinvolvingpartialortotalremovalofthefemaleexternalgenitaliaorotherinjurytothefemalegenitalorgansforculturalorothernon-medicalreasons.2Althoughprimarilyconcentratedin29countriesinAfricaandtheMiddleEast,FGMisauniversalproblem.ItispracticedinsomecountriesinAsia,includingIndia,Indonesia,IraqandPakistan,3aswellasinLatinAmerica,andamongimmigrantpopulationsinWesternEurope,NorthAmerica,AustraliaandNewZealand.TheEuropeanParliamentestimatedthat,in2009,about500,000womenlivedwiththeconsequencesofFGMintheEuropeanUnion,andapproximately180,000additionalwomenandgirlsareatriskofundergoingiteachyear.4
1UNGeneralAssemblyresolution67/146onintensifyingglobaleffortsfortheeliminationoffemalegenitalmutilations.5March2013.See:www.un.org/ga/search/view_doc.asp?symbol=A/RES/67/146(accessed24April2014).
2“FemaleGenitalMutilation:AjointWHO/UNICEF/UNFPAstatement.”1997,reiteratedin2008.Geneva:WorldHealthOrganization(WHO).
3“EndingFemaleGenitalMutilation/Cutting:Lessonsfromadecadeofprogress.”2013.Washington,DC:PopulationReferenceBureau.
4EuropeanParliamentresolutionof24March2009oncombatingfemalegenitalmutilationintheEuropeanUnion.
FGMhasbeeninternationallyrecognizedasanextremeformofviolationof
therights,healthandintegrityofwomenandgirls.In2012,theUnitedNations
GeneralAssemblyadoptedthefirst-everresolutionagainstFGM(67/146),
callingforintensifiedglobaleffortstoeliminateit.
7

CountrieswithFGMdatacollectedbyhouseholdsurveys
CountriesinwhichFGMhasbeenreported
CountriesinwhichFGMhasbeenreportedamongsomeimmigrantcommunities
Source:UNFPAanalysisbasedonDHSandMICS,2002-2014,andWHO,
“FemaleGenitalMutilation:AJointWHO/UNICEF/UNFPAStatement,”1997.
FGM can be found around the world
8

ThispublicationdocumentsthemostrelevantfeaturesofthepracticeofFGMin27African,2Arab,and1Asiacountries.Themainobjectiveistoprovideasimplepresentationofcurrentlevels;themaindifferences,accordingtobackgroundcharacteristics;andobservedtrendsinthelast10-15years.Consideringpast,currentandfuturedemographicdynamicshelpsidentifypossiblescenariosforelimination.
DataonFGMhavebeencollectedthroughDemographicHealthSurveys(DHS)5since1990,withabout50surveysconductedin25countrieswithprevalentFGM,andthroughMultipleIndicatorClusterSurveys(MICS)6since2000,withmorethan30surveysconductedin18countrieswithprevalentFGM.ReliabledataonthepracticearenowavailableforallAfricancountrieswherethepracticeisconcentrated,plusIraqandYemen.StatisticalinformationiscurrentlynotavailableforcountrieswhereFGMhasbeennewlyidentified,suchasColombiaandIndia.
5ICFInternationalimplementsDHSsurveys,fundedbytheUnitedStatesAgencyforInternationalDevelopment,withcontributionsfromotherdonorssuchasUNICEF,UNFPA,WHOandUNAIDS.Thesehouseholdsurveysprovidedataonawiderangeofindicatorsonpopulation,healthandnutrition.
6TheMICSarehouseholdsurveysrununderaUNICEFprogrammetoprovideinternationallycomparable,statisticallyrigorousdataonthesituationofchildrenandwomen.
ThefirstsectionofthispaperpresentsbackgroundinformationandadescriptionofeffortstoeliminateFGM.ThesecondsectionintroduceskeydemographiccharacteristicsofcountrieswithFGMconcentrations.Thethirdsectionfeaturescurrentlevels,trendsanddisparitiesbasedonthelatestFGMstatistics,focusingongapsinexistinganalyses.ThefourthsectionpresentscurrentprojectionsofeffortsrequiredtoeliminateFGM,providinganewperspectivebyfactoringindemographicdynamicsanalysis.
9


2A Demographic Overview
of FGM Prevalent Countries
11
SeveraldemographiccharacteristicsarecommontocountrieswhereFGMis
prevalent.Theyallhaveyoungpopulations,highfertilitylevels,andhighchild
andmaternalmortalityrates.Thesecharacteristicsdefinethecomplexityand
consequencesofthepractice,andmakeitseliminationmorechallenging.
2.1. Young PopulationsThetotalnumberofgirlsaffectedbyFGMisultimatelydeterminedbyitsprevalence/intensityandbythetotalnumberofgirlsatriskduringtheirlifespan—referring,inotherwords,totheagestructureofthepopulation.AsFGMmostlyhappenstogirlsbeforetheyreachage15,7agestructureisimportant.Populationsizeandstructurevaryduetopastandpresentpatternsoffertility,mortalityandmigration.ThemajorityofFGMaffectedcountries,22outof30,areleastdevelopedcountries,8exceptionsbeingCameroon,Côted’Ivoire,Egypt,Ghana,Indonesia,Iraq,KenyaandNigeria.Thesecountriesgrewatafastpacebetween1950and2010,andwillcontinuedoingsogiventheirpopulationmomentumandhighlevelsoffertility.Thepopulationoftheleastdevelopedcountriesisexpectedtoreachover1.8billionby2050.9
MostcountrieswithprevalentFGMhavelargeproportionsofyoungadolescentsandchildren(0-14yearsofage).All30FGMprevalentcountrieswithavailabledata,besidesIndonesia,areexperiencinghighpopulationgrowthandayoungagestructure,with30percentormoreoftheirfemalepopulationsunderage15.Incomparison,VietNam,anon-FGMprevalentcountry,hasonly22percentoffemalesunderage15.InChad,NigerandUganda,thepercentagewasalmosthalfthefemalepopulationin2015(seeTable2.1andFigure2.1).
7“FemaleGenitalMutilationFactsheetNo.241.”2014.Geneva:WHO.Seewww.who.int/mediacentre/factsheets/fs241/en/(accessedApril25,2014).
8TheleastdevelopedcountriesareclassifiedbytheUnitedNationsbasedontheirlowgrossnationalincome,weakhumanassetsandhighdegreeofeconomicvulnerability.
9UnitedNationsDepartmentofEconomicandSocialAffairs,PopulationDivision.2013. World Population Prospects: The 2012 Revision.
12

Table 2.1. Number and percentage of girls under age 15 in FGM prevalent countries, 2015
FGM PREVALENT COUNTRIES NUMBER OF GIRLS UNDER AGE 15 in thousands
PERCENTAGE OF GIRLS UNDER AGE 15 as of total female population
VERY YOUNG AGE STRUCTURE (MORE THAN 45% OF WOMEN UNDER AGE 15)
Niger
Uganda
Chad
Mali
Somalia
4,723
9,557
3,230
3,790
2,581
49.5
47.7
47.6
47
46.2
YOUNG AGE STRUCTURE (BETWEEN 35% AND 45% OF WOMEN UNDER AGE 15)
Gambia
UnitedRepublicofTanzania
Nigeria
BurkinaFaso
Cameroon
Eritrea
Senegal
Liberia
Benin
Côted’lvoire
Guinea
Kenya
Ethiopia
Togo
Guinea-Bissau
SierraLeone
Sudan
Mauritania
CentralAfricanRepublic
Yemen
Iraq
Ghana
446
11,593
39,730
3,961
4,939
1,419
3,202
933
2,270
4,338
2,560
9,714
20,259
1,489
367
1,292
7,905
796
945
4,891
6,819
5,022
44.8
44.4
44.1
44
42.2
42.1
42
41.8
41.6
41.5
41.5
41.5
41
41
40.8
40.6
40
39.3
38.7
38.6
38.5
37
RELATIVELY YOUNG AGE STRUCTURE (LESS THAN 35% OF WOMEN UNDER AGE 15)
Djibouti
Egypt
Indonesia
149
12,770
34,935
33.3
30.3
27.5
Source:UnitedNationsDepartmentofEconomicandSocialAffairs,PopulationDivision.2013.World Population Prospects: The 2012 Revision.
13

0-45-9
10-1415-19
20-2425-2930-3435-39
40-4445-4950-5455-5960-6465-6970-7475-79
80+
25 20 15 10 5 0 5 10 15 2020 25
0-45-9
10-1415-19
20-2425-2930-3435-39
40-4445-4950-5455-5960-6465-6970-7475-79
80+
25 20 15 10 5 0 5 10 15 2020 25
0-45-9
10-1415-19
20-2425-2930-3435-39
40-4445-4950-5455-5960-6465-6970-7475-79
80+
25 20 15 10 5 0 5 10 15 2020 25
Male Female
Male Female
Male Female
Figure 2.1. Population pyramids for FGM countries compared to a non-FGM prevalent country, 2015
A. Very young age structure example, Niger
B. Young/relatively young age structureexample, Burkina Faso
C. Non-FGM prevalent developing country example, Viet Nam
Source:UnitedNationsDepartmentofEconomicandSocialAffairs,PopulationDivision,2013,World Population Prospects: The 2012 Revision.
14

2.2. High Levels of Fertility
Inadditiontohavingyoungpopulations,FGMprevalentcountrieshavehighfertility.Globally,thetotalfertilityratefrom2010to2015was2.5childrenperwoman15-49yearsofage,andtheadolescentbirthratewas49livebirthsper1,000women15-19yearsofage.10Amongthe30FGMprevalentcountries,allhavetotalfertilityratesgreaterthan4childrenperwomanaged15-49(exceptforEgypt
with3andIndonesiawith2.3),andadolescentbirthratesthatexceed70per1,000womenaged15-19(exceptforDjibouti,Egypt,GhanaandIndonesia).Nigerpresentsthehighesttotalfertilityrateat7.6childrenperwomenaged15-49,whiletheCentralAfricanRepublichasthehighestadolescentbirthrateat229livebirthsper1,000womenaged15-19.
Figure 2.2. Prevalence of FGM among girls aged 15-19 according to adolescent birth rate and total fertility rate, 2002-2014
Globalaverage
Slowgrowthcountries
Rapidgrowthcountries
Veryrapidgrowthcountries
2 3 4 5 6 7 8
0
40
80
120
Adolescentbirth rate
160
200
240
Total fertility rate
Global average
Egypt
Djibouti
Ghana
EritreaEthiopia Yemen
Nigeria
Sudan
Gambia
Somalia
UgandaBurkina Faso
Guinea
Guinea-Bissau
CameroonCôte d’Ivoire
Tanzania
Sierra Leone
Kenya Benin Senegal
TogoMauritania
Iraq
Liberia
Mali
ChadNiger
Central African Republic
Indonesia
Source:DHS,MICSandothernationalsurveys
Bubble size:prevalence
ofFGM/Camonggirls
aged15-19,besidesglobal
average
10UnitedNationsDepartmentofEconomicandSocialAffairs,PopulationDivision.2013.World Fertility Patterns 2013.
15

VariationsintheprevalenceofFGMamonggirlsaged15-19areshownaccordingtothecorrespondinglevelsoffertilityinthecountry(adolescentbirthrateandtotalfertilityrate,Figure2.2).Italsorevealsthatcountrieswithveryrapidgrowthgenerallyhaveaveryhightotalfertilityrate(approximately5.6-7.6childrenperwomanaged15-49)andveryhighadolescentbirthrates(88-206per1,000womenaged15-19).AlthoughtheFGMprevalentcountrieshavesignificantlyhighertotalfertilityratesandadolescentbirthratesthantheglobalaverage,thereisnosignificantpositivecorrelationbetweenlevelsofFGMandtotalfertilityrates/adolescentbirthrates.Thisfindingindicatesthatthepracticeisnotlinkeddirectlytotheserates,buttootherfactors.
AmongFGMaffectedcountries,highlevelsoffertilityareassociatedwithrelativelyyoungpopulations(populationmomentum,Figure2.3).Thesecountrieshavegreaterpopulationgrowthgiventheirveryyoungagestructure.InSenegal,forexample,ayoungagestructurecontributesto56percentoffuturepopulationgrowth,andtogetherwiththeeffectofhighfertility,67percent.Thesetwofeaturesaccountfornearlyallfuturegrowth.Incontrast,inThailandandtheUnitedStates,wherefertilitylevelsareatorbelowreplacementlevel,agestructureswillonlycontributeto8percentoffuturepopulationgrowth.
Itispossibletocounteracttheimpactofpopulationmomentumcausedbyayoungagestructure.Forexample,additionalreductioninpopulationgrowthcanbeachievedbyraisingtheaverageageatwhichwomenbeginbearingchildren,andbylengtheningtheintervalbetweenbirths.MostwomenaffectedbyFGM,however,donothavetheoptiontodecideonwhetherornottohavesexualrelations,whentohavesexualrelations,whenorwhomtomarry,andwhethertodeferchildbearing.Similarly,thesewomentendtohaveshortintervalsbetweenbirthsasaresultofsocialpressureandasameansofobtainingsocialacceptanceandeconomicsecurity.Sincedelayingthestartofchildbearingcontributestofertilityreductionandpopulationgrowth,andtotheimprovementofwomen’swell-beingandqualityoffamilylife,itisimportanttodevelopcomprehensivepoliciesandinterventionsthataddressnotonlythepracticeofFGM,butalsochildandearlymarriage,earlychildbearingandbirthspacing.
16

1 2 3 4 5 6 70
10
20
30
Young age structure contribution to
population growth up to 2050
40
50
60
Total fertility rate
FGM prevalent countries
Other countries
Source:UNFPADecompositionofFuturePopulationGrowthTool.See:www.dataforall.org/dashboard/unfpa/decomposition.
Figure 2.3. Distribution of countries according to current levels of fertility (2010-2015) and the contribution of a young age structure to population growth up to 2050
17

11ProducedbytheInter-agencyGrouponMaternalMortalityEstimation,comprisingWHO,UNFPA,UNICEF,WorldBankandUnitedNationsPopulationDivision.
12Thematernalmortalityratioisthenumberofwomenwhodieduringpregnancyandchildbirthper100,000livebirths.
13EgyptandDjiboutihavevaluesbelowtheglobalaverage.WHO,UNICEF,UNFPA,WorldBankandUnitedNationsPopulationDivision.2014.Trends in maternal mortality: 1990 to 2013. Geneva: WHO.
14Theinfantmortalityrateisthenumberofinfantsdyingbeforereachingoneyearofage,per1,000livebirthsinagivenyear.
15UNICEF,WHO,WorldBankandUnitedNationsPopulationDivision.2013.Levels and Trends in Child Mortality Report 2013. New York: UNICEF.
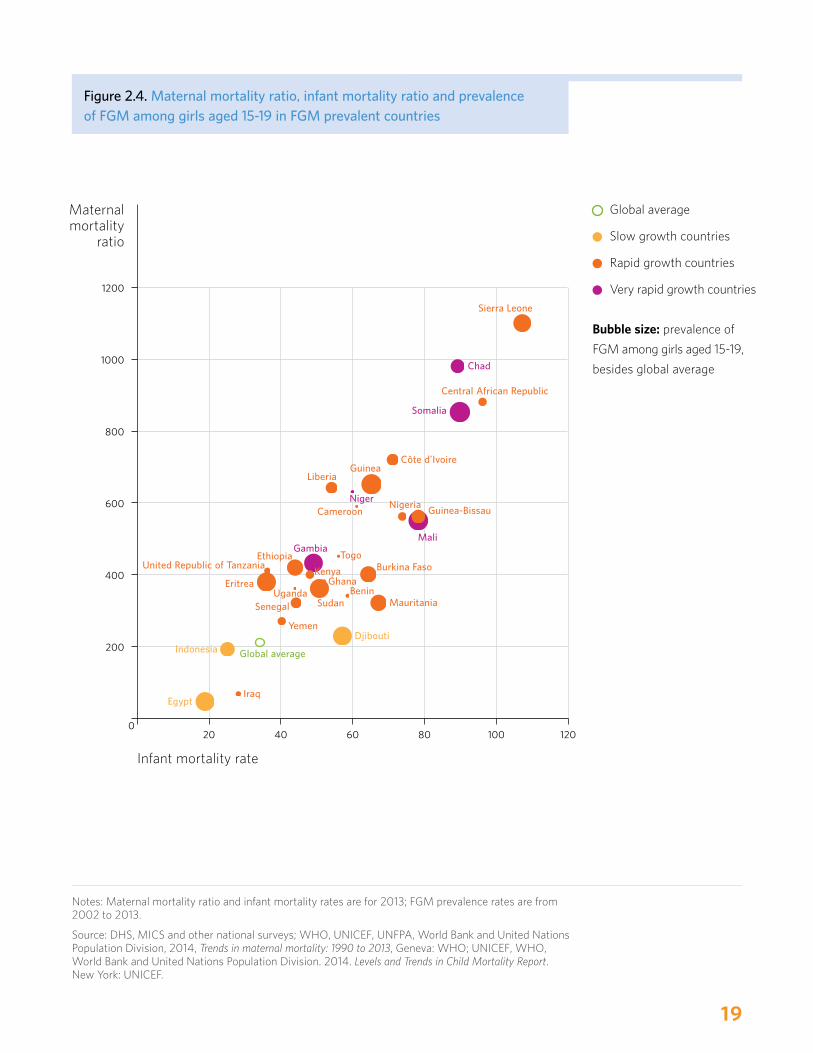
2.3. High Levels of Mortality
HighlevelsofmortalityarethethirddemographiccharacteristicobservedamongFGMprevalentcountries.Accordingto2013UnitedNationsestimates,11theaverageglobalmaternalmortalityratio12is210maternaldeathsper100,000livebirths;theratioin27ofthe30FGMprevalentcountriesishigherthanthis.13Infantmortalityrates14followasimilarpattern.Accordingto2013estimatesproducedbytheUnitedNationsInter-agencyGroupforChildMortalityEstimation,15theinfantmortalityrateinFGMprevalentcountriesconsiderablyexceededtheglobalaverage,exceptinEgypt,IndonesiaandIraq.Figure2.4showsthedistributionofFGMprevalentcountriesaccordingtotheirprevailinglevelsofbothmaternalandinfantmortality,underliningthatthemajorityofFGMaffectedcountriesareaffectedbyrapidpopulationgrowthandhighmortality.
18
20 40 60 80 100 1200
200
400
600
Maternal mortality
ratio
800
1000
1200
Infant mortality rate
Global average
Egypt
Somalia
Central African Republic
Chad
Sierra Leone
Côte d’Ivoire
Mali
Guinea-BissauNigeria
Guinea
NigerCameroon
Liberia
Iraq
Djibouti
Gambia
KenyaGhana
TogoBurkina Faso
MauritaniaSudanBenin
Ethiopia
UgandaEritrea
Senegal
Yemen
Indonesia
United Republic of Tanzania
Figure 2.4. Maternal mortality ratio, infant mortality ratio and prevalence of FGM among girls aged 15-19 in FGM prevalent countries
Globalaverage
Slowgrowthcountries
Rapidgrowthcountries
Veryrapidgrowthcountries
Bubble size:prevalenceof
FGMamonggirlsaged15-19,
besidesglobalaverage
Notes:Maternalmortalityratioandinfantmortalityratesarefor2013;FGMprevalenceratesarefrom2002to2013.
Source:DHS,MICSandothernationalsurveys;WHO,UNICEF,UNFPA,WorldBankandUnitedNationsPopulationDivision,2014,Trends in maternal mortality: 1990 to 2013,Geneva:WHO;UNICEF,WHO,WorldBankandUnitedNationsPopulationDivision.2014. Levels and Trends in Child Mortality Report.NewYork:UNICEF.
19

2.4. Urbanization and Migration
In2015,morethanhalfoftheworld’spopulationlivesinurbanareas.By2050,theUnitedNationsPopulationDivisionprojectsthatthisfigurewillreach66percentoftheworld’spopulation.16Althoughurbanizationisauniversalphenomenon,ithasregionaldifferences,withLatinAmericabeinghighlyurbanized,Asiaalmosthalfurbanandsub-SaharanAfricaaboutone-thirdurban.Amongcountrieswithlowurbanizationlevels,therateofurbangrowthcanstillbeveryhigh;lowcurrentlevelscanchangeintofast-pacedurbanizationinthefuture.
MostFGMaffectedcountriesarelessurbanizedthanothersintheirregions;22ofthe30FGMaffectedcountrieshavelessthanhalfoftheirpopulationsinurbanareas(seeFigure2.5).ThisfeatureisimportantasFGMismoreprevalentinruralareas.OneexceptionisNigeria,whereFGMoccursathighratesamongurbanresidents.Thismaybeexplainedbyethnicity.17
Figure 2.5. Percentage of people living in urban areas in FGM prevalent countries, 2010 and 2050
2010
Source:UnitedNationsDepartmentofEconomicandSocialAffairs,PopulationDivision.2014.World Urbanization Prospects: The 2014 Revision.
0 10 20 30 40 50 60 70 80 90
Indonesia
Côte d’Ivoire
Ghana
Cameroon
Nigeria
Liberia
Guinea-Bissau
Benin
Senegal
Mali
Togo
Somalia
Sierra Leone
Central AfricanRepublic
Egypt
Guinea
Yemen
United Republicof Tanzania
Burkina Faso
Sudan
Kenya
Eritrea
Ethiopia
Chad
Niger
Uganda
71
71
71
70
70
67
65
65
61
60
60
58
42
42
36
38
58
57
57
57
56
54
53
52
50
44
33
24
42
38
37
35
32
21
17
22
18
14
35
32
28
26
37
38
39
43
52
43
48
45
77 83
69 78
Djibouti
Iraq
Mauritania 7457
50
Gambia 56
51
51
2050
20

UrbanizationworldwidebutparticularlyinAfricaisfuelledbyaconstantflowofruraltourbanmigrants.Greaterandbetteropportunitiesarethemainreasons,aspeopleseekexpandedaccesstobasicservicessuchaswaterandsanitation,education,health,employmentandincome.ThepositiveeffectsofurbanizationincludetheabandonmentofFGM,asfamiliesandwomeninparticularbenefitfrombettereducationandaccesstoservicesthatencouragechangesinnormsandbehavioursthatpreviouslysupportedFGM.ThechallengebecomeshowtoreapthebenefitsofurbanizationinadvancingtheeliminationofFGM.Withinthespecificcontextofurbanandruraldynamics,policiesandinterventionstoeliminateFGMcanacquiremaximumrelevance,effectiveness,efficiencyandimpact.
Between2010and2050,thepercentageofpeopleinurbanareasinFGMaffectedcountrieswillincreasebyalmost60percent.Ineightcountries,theincreaseisexpectedtobe70percentorhigher:Yemen(70percent),Kenya(86percent),theUnitedRepublicofTanzania(89percent),Niger(101percent),BurkinaFaso(103percent),Eritrea(104percent),Ethiopia(117percent)andUganda(121percent).SomechangesfromruraltourbanmigrationcouldincludeincreasedprevalenceinurbanareasduetothemovementsofethnicgroupswhopracticeFGM,ashasbeennotedinSenegal.
Thereisgrowingrecognitionoftheprecarioussituationfacedbytheworld’s232millionmigrants,18andtheimperativeoffulfillingandprotectingtheirhumanrights.InternationalmigrationhasincreasedthenumberofgirlsandwomeninWesterncountrieswhohaveundergoneFGMorwhomaybeatrisk.ItisthroughmigrationthatthisonceremotepracticeanditsharmfulconsequenceshavebecomearealityinEurope,NorthernAmerica,AustraliaandNewZealand.Often,thereiscontinuingsupportforthepracticeamongcommunitiesoriginatingfromFGMcountries,suggestingthatthissocialconventionisstronglyrooted.BecauseFGMiscloselytiedtoculture,itbecomesanintegrationissue,inadditiontobeingahealthandhumanrightsissue.DataonFGMprevalenceamongmigrantsindestinationcountriesarerare,however.Mostofthetime,extrapolationsfromknowncasesareusedtomeasuretheextentofthepractice.StrategiesaddressingFGMmustbeadaptedtothespecificitiesofmigration.19
16UnitedNationsDepartmentofEconomicandSocialAffairs,PopulationDivision.2014.World Urbanization Prospects: The 2014 Revision.
17A.A.Abiodun,B.A.OyejolaandO.Job.2011.“Female Circumcision in Nigeria, Prevalence and Attitudes.”CENTREPOINTJOURNAL(scienceedition)17(2).
18StatementbytheUnitedNationsSecretary-Generalon15December2014.
19InternationalOrganizationforMigration“Supporting the Abandonment of Female Genital Mutilation in the Context of Migration.”
21

2.5. FGM and Other Forms of Violence against Girls and Women
FGMandchildmarriageareformsofviolencethatcausenegativeconsequencesforgirlsandwomen,includingthroughtheperpetuationofgenderinequality.Thesepracticeshappentogirlsandwomenatdifferenttimesoftheirlives,exposingthemtovariouslevelsofvulnerabilitiesandmultiplehumanrightsviolations.ThissectionexplorestheevidencetodetermineifwomenwhohaveexperiencedotherformsofviolencearemorelikelytosubjecttheirdaughterstoFGM.Thisisdonewithdataonwomenwithdaughtersaged10-14inninecountrieswherethemajorityofFGMtakesplacebeforeage10.
Byanalysingdataforwomenaged15-49whohaveatleastonedaughteraged10-14,Figure2.6showsapositiverelationshipbetweenchildmarriageandtheprobabilityofcuttingthedaughtersforselectedcountries.Inotherwords,womenmarriedaschildrentendtopracticeFGMontheirdaughters.ThisismoreevidentwhencomparingGhanawithSenegal,orGhanaorTogowithNigeria.InGuineaandNigeria,weobservethatahigherpercentageofmothersmarriedbeforeage18resultedinahigherprevalenceofmotherscuttingatleastoneoftheirdaughters.
25 50 75 1000
25
50
75
100
Percentage of women 15-49 who have at least one daughter aged 10-14 and who married before age 18
Ghana
NigeriaBurkina Faso
Sierra Leone
Guinea
Percentage of women 15-49 who
have at least one daughter aged 10-14 who
has experienced FGM
Senegal
Central Africa Republic
Figure 2.6. Among mothers who have at least one daughter aged 10-14, the percentage of whom have at least one daughter who has experienced FGM, and the percentage of whom married before age 18
22

ThishypothesisbecomesmoreapparentfromdatainFigure2.7,whichshowsFGMratios20amongwomenmarriedbefore,andatorafterage18.Inallninecountriesmotherswhoexperiencedchildmarriagearemorelikelytocutatleastoneoftheirdaughters,comparedtothemotherswhomarriedatorafterage18(aratiogreaterthanone).
0.5 1.0 1.5 2.0 2.5 3.00
Senegal
Ghana
Central African Republic
Nigeria
Burkina Faso
Sierra Leone
Mauritania
Guinea
Mali
Mothers who married before age 18 are more likely to cut their girls.
20Aratiogreaterthanoneindicatesthatbeingintheselected/exposedgroupincreasestheoddsorriskofexperiencingtheoutcome.
Figure 2.7. Ratio of the percentage of mothers who have at least one daughter who has experienced FGM, by mothers married before age 18 over mothers married at age 18 or later
Source:UNFPAanalysisbasedonDHSandMICS.
23

Domesticviolenceisprevalentacrossallsocietiesandalllevelswithinthem,amanifestationofgenderinequalityandagravehumanrightsviolation.Figures2.8and2.9showtherelationshipbetweenwomen’sattitudestowardsdomesticviolence(wifebeatingacceptance)andthepercentageofthemwithatleastonedaughterwhohasexperiencedFGM.
Figure2.8indicatesapositiverelationship,withwomenwhobelievethatdomesticviolenceisjustifiedunderatleastonecircumstancemorelikelytosubjecttheirdaughterstoFGMthanthosewhoconsideritnotacceptableatall.Thisisparticularlyevidentwhencomparing,forinstance,BurkinaFasowithGuinea,orcomparingGhanawithSenegal,wherehigherpercentagesofmotherswhothinkdomesticviolencecanbejustifiedunderatleastoneconditionresultedinhigherpercentagesofmotherswhohaveatleastonedaughterwhohasexperiencedFGM,asreportedbythemothers.
Figure 2.8. Among mothers who have at least one daughter aged 10-14, the percentage of whom have at least one daughter who has experienced FGM, and the percentage of whom think domestic violence can be justified under at least one condition
25 50 75 1000
25
50
75
100
Ghana
NigeriaBurkina Faso
Sierra Leone
Guinea
Percentage of women 15-49 who have at least one daughter aged 10-14, and who think wife beating can be justified under at least one condition
Percentage of women 15-49 who
have at least one daughter aged 10-14 who
has experienced FGM
Central Africa Republic
Senegal
Figure2.9presentstheratiosofFGMprevalencetowomenjustifyingdomesticviolenceversusthosewhorejectthenotioncompletely.WomeninBurkinaFaso,Mauritania,Nigeria,SenegalandSierraLeonewhotendtojustifydomesticviolencearemorelikelytosubjecttheirdaughterstoFGMbyaratioexceedingonecomparedtothosewhorejectit.21CentralAfricanRepublichasaratiooflessthanone,andGhanahasahighratio,butcalculationswereinfluencedbyuncertaintyaroundFGMestimates.GhanahasarelativelylowlevelofFGM,below2percent,asshowninthenextsection.
Girlswhomarrybeforeage18arelesslikelytocompletetheireducation,andmorelikelytoexperiencedomesticviolenceandcomplicationsinchildbirth,inequalitiesthatstandinthewayofdevelopment.Empoweredwomen,bycontrast,contributetothehealthandproductivityofwholefamiliesandcommunities,andimproveprospectsforthenextgeneration.
24

21Aratiogreaterthanoneindicatesthatbeingintheselected/exposedgroupincreasestheoddsorriskofexperiencingtheoutcome.
Figure 2.9. Ratio of the percentage of mothers who have at least one daughter who has experienced FGM, by mothers who think domestic violence can be justified under at least one condition over mothers who think it cannot be justified under any condition
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.00
Senegal
Ghana
Central African Republic
Nigeria
Burkina Faso
Sierra Leone
Mauritania
Guinea
Mali
Source:UNFPAanalysisbasedonDHSandMICS.
Mothers who think domestic violence can be justified under at least one condition are more likely to cut their girls.
Developmentpoliciesmustaddresspersistentdiscriminationandinequalitiestobeeffective.EffortstoaddressFGMmustoccurwithinawiderframeworkofpoliciesandinterventionsthatholisticallyaddressallharmfulpracticesandformsofviolenceagainstgirlsandwomen.
Thisoverviewofseveralsocio-demographiccharacteristics—fertility,mortality,migrationandgender-basedviolence—impliesthatanyattempttofurtherconceptualizeandcontextualizethepracticeofFGMneedstobedoneinlightofthese,takingonboardthespecificpatternsinanygivencountry.GirlsandwomensubjectedtoFGMfindthemselveshavingmanychildren,havingahigherriskofdyinginchildbirthalongwiththeirchildrenalsodying,andbeingvictimsofdomesticabuse—allfactorswithimportantimplications,directlyorindirectly,forwork
toaddressFGM.UnderstandingthedemographicbackgroundofacountryisusefulindevelopingaholisticcomprehensionofthecontextinwhichFGMoccursanddrawingrelevantconclusionstoguideprogramming.
Foradvocacyandprogrammaticpurposes,itcanbeimportanttostressthatinterventionstargetingFGMabandonmentcouldhelpimprovedemographiccharacteristics.Forexample,effectivelyaddressingFGMentailsthebetteroverallwell-beingandstatusofgirlsandwomenatthefamilyandcommunitylevels.Itcanhelpredressgenderinequalityandencourageastrong,holistic,sustainablesocialchangeprocess.Programmesprimarilydesignedaroundothertypesofviolenceandgenderinequality,suchaschildmarriage,alsoneedtosystematicallyincorporateFGMasawayofbroadeningopportunitiestoadvancechange.
25

3Levels and Trends

3.1. Global Estimates and Country Prevalence
Today,bysomeestimates,130milliongirlsandwomenhaveundergoneFGMinthe29countrieswithFGMdatacollectedbyhouseholdsurveys.22Otherestimatesindicatethatalmost87millionwomenandgirlsaged15yearsandolderhavebeensubjectedtoitin27AfricancountriesandYemen,23orabout100millionto140milliongirlsandwomenworldwide.24Theactualnumberremainsunknown,mainlyduetoalackofreliabledataongirlsyoungerthanage15,onwomenandgirlsintheArabStates,AsiaandLatinAmerica,andonimmigrantcommunitiescontinuingthepracticeinEurope,NorthAmericaandAustralia.
ThemainindicatortomeasureFGMprevalenceisthepercentageofgirlsaged15-19experiencinganyformofFGM,asselfreported.Thisindicatorisusedforthreereasons.First,itislikelytoreflectmorecompleteFGMstatus,sincealmostallgirlsarecutbeforeage15.Afterthatage,theirriskofFGMismuchlower.Indicatorsthatmeasuregirlsyoungerthanage15onlyreflectthecurrentFGMstatusofthesegirls.This,therefore,canresultinunder-reportingoftheactualprevalenceofFGMbecausethegirlsarestillatriskofundergoingthispractice.Second,thisindicatoristheclosesttoFGMincidence(newFGMcases),anditfocusesongirlsmostrecentlycut.
Thewidelyusedindicatoronthepercentageofgirlsandwomenofreproductiveage(15-49)whohaveexperiencedanyformofFGM,althoughshowingabiggerpicture,doesnotcapturerecentchanges.Thatisbecausewomenages20-24yearshavealreadyundergoneFGMatleastfiveyearspriortothesurvey,dependingontheageofcutting.Thepracticemayhavehappenedmuchearlierforwomenaged25andbeyond.Thereforetheprogrammestargetingtheabandonmentofthispracticewillnothaveanyinfluenceontheolderwomen.Athirdreasonisdataavailability.AllhouseholdsurveysallowthecalculationofFGMprevalenceamongthegroupaged15-19.
ThereiswidevariationinFGMprevalenceacrosscountries,asindicatedbythemostrecentdata(seeTable3.1andMap3.1).ThehighestprevalencewasinSomaliaat97percent,followedbyGuineaat94percentandMaliat90percent.ThelowestprevalencewasinCameroonat0.4percent,afterwhichcomeNigerandUgandaat1percent.CountriesaredividedintothreegroupsbasedonFGMprevalence:high,mediumandlow.Subnationalvariationdiffers,beinglessinhigh-prevalencecountriesandgreaterinlow-prevalencecountries.
22UNICEF.2014.“Female Genital Mutilation/Cutting: What might the future hold?”NewYork.
23P.S.Yoder,S.WangandE.Johansen.2013.“Estimates of Female Genital Mutilation/Cutting in 27 African Countries and Yemen.” StudiesinFamilyPlanning44(2):189-204.
24PopulationReferenceBureau.2014.“Female Genital Mutilation/Cutting: Data and Trends.”
27

Table 3.1. Percentage of girls aged 15-19 experiencing any form of FGM, by country, most recent data, 2002-2014
FGM PREVALENT COUNTRIES PERCENTAGE OF GIRLS AGED 15-19 EXPERIENCING ANY FORM OF FGM
DATA SOURCE
HIGH PREVALENCE COUNTRIES (MORE THAN 60%)
Somalia
Guinea
Mali
Djibouti
Sudan
Egypt
Eritrea
Gambia
SierraLeone
Mauritania
Ethiopia
96.7
94
90.3
89.5
84
81
78.3
76.3
74.3
65.9
62.1
2006MICS
2012DHS
2013DHS
2006MICS
2010SHHS
2008DHS
2002DHS
2013DHS
2013DHS
2011MICS
2005DHS
MEDIUM PREVALENCE COUNTRIES (20-60%)
BurkinaFaso
Indonesia*
Guinea-Bissau
Chad
Coted’lvoire
Liberia**
Senegal
58
51
48.4
41
31
26.4
21.1
2010DHS
2013RISKESDAS
2010MICS
2010MICS
2011-12DHS
2013DHS
2014DHS
LOW PREVALENCE COUNTRIES (LESS THAN 20%)
CentralAfricanRepublic
Yemen
Nigeria
Kenya
UnitedRepublicofTanzania
Iraq
Benin
Togo
Ghana
Niger
Uganda
Cameroon
18
16.4
15.3
11.4
7
4.9
2
1.8
1.5
1.4
1
0.4
2010MICS
2013DHS
2013DHS
2014DHS
2010DHS
2011MICS
2011-12DHS
2014DHS
2011MICS
2012DHS
2011DHS
2004DHS
*Percentageofgirlsaged0-11yearswhohaveundergoneanyformofFGM/C
**Percentageofgirlsaged15-19yearswhoaremembersoftheSandesociety.MembershipintheSandesocietyisaproxyforFGM.
28

Highprevalencecountries(morethan60%)
Mediumprevalencecountries(20%-60%)
Lowprevalencecountries(lessthan20%)
FGMisnotprevalentinthesecountries
Map 3.1. FGM prevalent countries where data are available, latest data
Egypt
Sudan
EritreaChad
Iraq
Yemen
Somalia
Ethiopia
Kenya
United Republic of Tanzania
Uganda
Central African RepublicCameroon
Nigeria
NigerMaliMauritania
SenegalGambia
Guinea-Bissau
Sierra LeoneLiberia
Côte d’Ivoire
Burkina Faso
Ghana
Togo
Benin
Guinea Djibouti
ItisevidentthattheprevalenceofFGMvariesfromlessthan1percentincertaincountriestobeingalmostuniversalinothers.ThepatternofsubnationalvariationinFGMprevalentcountriesdiffers.
Ingeneral,subnationalvariationsinprevalenceinhighFGMcountriestendtobeminor,whilelowFGMprevalencecountriestendtoshowmoresignificantvariations.
Source:DHSandMICS,2002-2014.
Indonesia
29

3.2. Trends: Is the Practice Changing?
AnincreasingnumberofcountrieshaveconductedoneormorehouseholdsurveyswithanFGMmodule,therebymakingtrendanalysismorefeasible.Trendanalysiscanbeconductedfrommultipleperspectives.Oneofthemostcommonmethodsistotakemorethanonesurveyforthesamecountry,andcomparetheprevalenceofFGMforoneagegroup.ItisalsopossibletocomparetheprevalenceofFGMacrossfive-yearagecohortsfromthesamesurvey.Forexample,acomparisonofprevalenceamonggirlsaged15-19andamongwomenaged45-49mayindicateadecreasingorincreasingtrend.Dependingontheageatcutting,thetrendmayalsobeanalysedbycomparingtheprevalenceamonggirlsaged15-19yearsandamonggirlsunderage15(aged0-4,aged5-9andaged10-14)fromthesamesurvey.Whenmakingthistypeofcomparison,itisimportanttoadjusttheprevalenceamonggirlsunder15.SincetheyarestillsubjectedtoFGM,prevalenceislikelytobeunderestimated.
Thisreportanalysestrendsbycomparingtheprevalenceamonggirlsaged15-19fromtwopointsintimeforthesamecountry(around2007andaround2012).Figure3.1showsthatofthe23countrieswithtwoconsecutivehouseholdsurveys,16have
seenadeclineinprevalenceamonggirlsaged15-19.Amongthehighprevalencecountries,thefastestreductionhastakenplaceinEgypt,from96percentin2005to81percentin2008,a16percentdecline.Surprisingly,twohighprevalencecountriesshowedanincrease,GuineaandMali.InGuinea,prevalenceclimbedfrom89percentin2005to94percentin2012.
ThechangeinFGMinmediumprevalencecountriesandinlowprevalencecountriesvaried.ThelargestdeclinewasinLiberia,droppingfrom36percentin2007to26percentin2013,a26percentdecline,followedbySenegal,witha12percentdecreasefrom24percentin2010to21percentin2014.InCôted’lvoire,thereportedprevalenceroseslightlybetween2006and2012,from28percentto31percent.InGuinea-Bissau,theprevalencewentfrom44percentto48percent,an11percentincrease.
ThemostdramaticdeclineinlowprevalencecountrieswasinBenin,from8percentin2006to2percentin2012,areductionof75percent.InKenya,prevalencefellby28percent,from20percentin2003to15percentin2008.
30

Table 3.2. Data on FGM are available for 30 FGM prevalent countries, after 2000
Egypt
Nigeria
Mali
Senegal
SierraLeone
Benin
BurkinaFaso
CentralAfricanRepublic
Chad
Gambia
Ghana
Kenya
Mauritania
Sudan
Togo
Côted’lvoire
Ethiopia
Guinea
Guinea-Bissau
Liberia
Niger
UnitedRepublicofTanzania
Uganda
Cameroon
Djibouti
Eritrea
Indonesia
Iraq
Somalia
Yemen
2014DHS
2013DHS
2013DHS
2014DHS
2013DHS
2012DHS
2010DHS
2010MICS
2010MICS
2013DHS
2011MICS
2014DHS
2011MICS
2010SHHS
2014DHS
2012DHS
2005DHS
2012DHS
2010MICS
2013DHS
2012DHS
2010DHS
2011DHS
2004DHS
2006MICS
2002DHS
2013RISKESDAS
2011MICS
2006MICS
2013DHS
2008DHS
2011MICS
2010MICS
2012DHS
2010MICS
2006DHS
2006MICS
2006MICS
2004DHS
2010MICS
2006MICS
2008DHS
2007MICS
2006SHHS
2010MICS
2006MICS
2000DHS
2005DHS
2006MICS
2007DHS
2006DHS
2004DHS
2006DHS
2005DHS
2008DHS
2006DHS
2010DHS
2008DHS
2001DHS
2003DHS
2000MICS
2000MICS
2005MICS
2003DHS
2003DHS
2000DHS
2000MICS
2006MICS
2003DHS
2007MICS
2001DHS
2005DHS
2005MICS
2000DHS
2003DHS
Source:UNFPAanalysisbasedonDHSandMICS.
31

0 10 20 30 40 50 60 70 80 90 100
Guinea
Mali
Sudan
Egypt
Gambia
Sierra Leone
Mauritania
Ethiopia
Burkina Faso
Guinea-Bissau
Côte d’Ivoire
Chad
Liberia
Nigeria
Kenya
United Republic of Tanzania
Benin
Ghana
Niger
Uganda 11
Togo 20
12
21
28
79
1115
1522
1819
2636
Senegal 2124
3128
4143
4844
5860
6271
6668
7476
7680
8196
8487
9085
9489
Central AfricanRepublic
Figure 3.1. Reductions and increases in FGM according to the percentage of girls aged 15-19 who have experienced any form, 2007-2012
Aroundyear2007
Aroundyear2012
Notes:DataforEthiopiaaretakenfromDHS2000and2005asDHS2010didnotcollectdataonFGM.
Source:DHS,MICSandothernationalsurveys.
32

3.3. Case Studies: Trends and Disparities in Burkina Faso and Guinea
ThissectionlooksatspecifictrendsinBurkinaFasoandGuinea.
TocapturethemostrecentchangesinGuinea,theprevalenceofFGMamongyounggirlsunderage15,asreportedbytheirmothers,wasanalysed,adjustingforthefactthatgirlsunderage15arestillatriskofbeingcut.Thegroupofgirlsaged10-14wasselectedbecauseestimatesforthemarelesssensitivetocensoring,comparedtoestimatesforyoungergirls,andbecausetheirstatusismorelikelytobetheirfinalone.
CalculatingtheadjustedprevalencerequiresexaminingpatternsofageatthetimeFGMwasperformedandrelatedtrend.InGuinea,nosignificanttrendwasfoundforageatcutting.Table3.2presentstheprevalenceofFGMamonggirlsandwomenaged5-49byfive-year
agegroups,accordingtoageattimeofcutting.Amonggirlsaged15-19,23percentwerecutunderage5,44percentbetweenages5-9,27percentbetweenages10-14,and1percentatage15yearsorlater,addinguptoatotalprevalenceof94percent.Thiscomparisonismadewithgirlsaged10-14,where12percentwerecutbeforeage5,54percentbetweenages5-9,and14percentbetweenages10-14.Bytakingtheratiosofgirlscutatages0-4correspondingtogirlsaged15-19and10-14,andthosecutatages5-9correspondingtogirlsaged15-19and10-14,itcanbeestimatedthatapproximately6percentofgirlsaged10to14areexpectedtobecutbeforeage15.AccordingtoTable3.2,oncegirlsreachage15,approximately1percentwhohavenotyetundergoneFGMarestillatriskofbeingcut.Thisaddsuptoanadjustedprevalenceof86percentamonggirlsaged10-14.
Source:DHS,MICSandothernationalsurveys.
*Prevalenceratesamonggirlsaged10-14needtobeadjustedbecausetheyarestillatriskofbeingcutbeforetheyreachage15(valueforbeingcutat10-14isunderestimated),andevenaftertheyreachage15(valueforbeingcutat15andbeyondismissing).
Table 3.2. Percentage of girls and women in Guinea who have undergone FGM by five-year age group, by age at cutting
AGE GROUP CUT AT 0-4 CUT AT 5-9 CUT AT 10-14 CUT AT 15+
PREVALENCE OF GIRLS AND WOMEN WHO HAVE NOT UNDERGONE FGM
PREVALENCE OF FGM
5-9
10-1410-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
17.9
11.6
11.6
22.5
24.2
25.9
25.3
23.0
22.4
23.8
32.6
54.3
54.3
43.5
41.8
40.3
36.5
35.4
38.7
37.3
14.1
19.6
26.8
26.5
29.4
34.6
38.0
34.7
33.6
0.8
1.1
2.4
2.4
1.9
2.4
3.0
4.9
49.4
19.9
13.7
6
5.1
2.1
1.7
1.2
1.2
0.4
50.6
80.1
86.3
94
94.9
97.9
98.3
98.8
98.8
99.6
adjustedprevalence*
33

Figure 3.2. Percentage of girls and women who have undergone FGM, by age group, cut at any age, cut before age 15 only and cut before age 10 only
A. Cut at any age
B. Cut beforeage 15 only
C. Cut before age 10 only
Source:UNFPAanalysisbasedonDHS.BurkinaFasoDHS2010andGuineaDHS2012.
45-49 40-44 35-39 30-34 25-29 20-24 15-19 Adjusted10-14
0
25
50
75
100100
89 8885 83
78
70
58
27
99 99 98 9895 94
86
45-49 40-44 35-39 30-34 25-29 20-24 15-19 Adjusted10-14
0
25
50
75
100
95 9696 96 9692 93
8586 85 8481
76
69
57
27
45-49 40-44 35-39 30-34 25-29 20-24 15-19 Adjusted10-14
0
25
50
75
100
75 76 75 7470
63
53
25
61 6158
6266 66 66
66
Guinea
BurkinaFaso
34

Figures3.2a-cshowthepercentagesofgirlsandwomenwhohaveundergoneFGMbyfive-yearagegroupsinBurkinaFasoandGuinea.Figure3.2asummarizestheprevalenceofFGMatanytimeinthegirls’lives.Figure3.2bincludescutsdonebeforeage15,andFigure3.2conlycutsbeforeage10.Together,thefiguresprovideanalternativeoverviewofthelatesttrendsinFGMprevalenceinthetwocountries.WhilethetrendinGuinearemainsalmostconstant,andalthoughFGMisalmostuniversalamongwomenaged45-49years,asmallpercentageofgirlsaged15-19remainuncut.InBurkinaFaso,theprevalenceofFGMhasdeclinedinthepastdecade.
Althoughtheadjustedprevalencehelpsminimizetheriskofunderestimationduetocensoring,therearestilluncertaintiesduetorisksthatincludemisreportingonageatcutting,andunwillingnessamongmotherstodisclosetheirortheirdaughters’realFGMstatusbecauseoftheirknowledgeofcampaignsonFGMabandonmentandlegalbansonthepractice.
TheprevalenceofFGMcanvarysignificantlyacrossdifferentethnicandreligiousgroups,eveniftrendsinoverallprevalenceareconstantforsomecountries.Figure3.3showstrendsamonggirlsaged15-19byethnicityandreligion,inBurkinaFasoandGuinea,basedonthreeconsecutiveDHSsurveys.25
InGuinea,althoughtheprevalenceofFGMamongPeulh,Soussou,Kissi,andMalinkewomenremainedover90percentbetween2000and2012,theprevalenceamongGuerzewomendeclinedinthesameperiodfrom70percentto38percent.InBurkinaFaso,prevalenceamongthreeethnicgroups(Bobo/Dioula/Sénoufo,Mossi,andother)outoffivegroupsdeclinedbetween1999and2010.ReductionamongBobo/Dioula/Sénoufowomenwasthefastest,from78percentto58percent.Fulfuldé/Peulwomenhaveexperiencedacontinuousincreaseinprevalence,from60percentin1999,to64percentin2003,to78percentin2010.Groupslikethisdeserveparticularattentionfromprogrammemanagersandpolicymakers,asprevalenceishigherthanamongothergroupsandhasincreasedovertime.
PrevalenceinbothcountriesismuchhigheramongMuslimwomencomparedtootherreligiousgroups(Christian,Catholic,animistandnoreligion).AlmostnochangeshavebeenobservedinprevalenceamongMuslimwomeninthepastdecade.Incontrast,prevalenceinChristian/Catholicwomenhasdeclined.
25Someoftheseestimatesarebasedonareducednumberofobservationsandthereforemaybeaffectedbysamplingerrorsthat,togetherwithnon-samplingerrors,maycompromisethesignificanceofdescribeddifferencesbetweengroups.Differencesshouldbeusedcarefullytofurtheridentifyunderlyingculturalpractices.
35

DHS 2000 DHS 2005 DHS 2012
50
30
70
90
110
Prevalence of FGM/C among
girls 15-19, by ethnicity group
Peulh
Kissi
Guerze
Soussou
Malinke
A. Guinea, by ethnic group B. Burkina Faso, by ethnic group
DHS 1999 DHS 2003 DHS 2010
40
20
60
80
100
Prevalence of FGM/C among
girls 15-19, by ethnicity group
Bobo/Dioula/Sénoufo
Other
Gourmantché
Fulfuldé/Peul
Mossi
Figure 3.3. Trends in prevalence of FGM among girls aged 15-19, by ethnic group and religion
36

Notes:Traditional,animistandnoreligioncategorieswereexcludedduetolimitednumberofcases.
Source:UNFPAanalysisbasedonDHS.
B. Burkina Faso, by ethnic group C. Guinea, by religion D. Burkina Faso, by religion
DHS 2000 DHS 2005 DHS 2012
50
30
70
90
110
Prevalence of FGM/C among
girls 15-19, by religion
Muslim
Christian
DHS 1999 DHS 2003 DHS 2010
40
20
60
80
100
Prevalence of FGM/C among
girls 15-19, by religion
Muslim
Catholic
Protestant
37

Amorecomprehensivepictureofdisparitiesacrossdifferentsocio-demographiccharacteristicscomesfromanalysingFGMprevalenceamongyounggirlsaged10-14,basedondatadisaggregatedby13socio-demographiccharacteristicsoftheirmothersorhouseholds.Theseinclude:1)whethermotherunderwentFGM,2)wealthindex,3)highesteducationallevelofmother,4)husband/partner’seducationlevel,5)motherworksforfamily,othersorself,6)placeofresidence,7)religion,8)ethnicity,9)literacy,10)mothereverheardoffistula,11)adolescentpregnancy,12)beliefthatFGMrequiredbyreligion,and13)opinionthatFGMshouldbecontinuedorbestopped.Aftercomparingthelevelsacrossgroupsforeachcharacteristic,themostrelevantcharacteristicswereidentified(seeFigure3.4):
1)WhethermotherunderwentFGM
2)Highesteducationallevelofmother
3)Religion
4)Ethnicity
TheFGMstatusofmothershashighinfluenceonthestatusofthedaughters.InGuinea,motherswhounderwentFGMare10timesmorelikelytosubjecttheirdaughterstothepractice,apatternalsofoundinBurkinaFaso.Amother’seducationisalsoakeyfactor.InBurkinaFaso,27percentofgirlswhosemothershavenoeducationhaveexperiencedFGM,comparedto0percentofgirlswhosemothershaveahighereducationallevel.
ThetwocasestudiesprovidefurtherevidencethatapracticesuchasFGMoccurswithinverydefinedsocio-culturalparameters.ThesedisparitieswithinandamongcountrieshighlighttheneedtopayattentiontodifferentfactorsthatmaycauseFGMandcouldbethebasisofmoretargetedinterventions.
38

10
0
20
30
40
50
60
70
80
90
100
Guinea Burkina Faso
81
8
81
58
85
45
91
19
29
1
27
0
30
11
42
4
Prevalence of FGM among
girls aged 10-14
MotherunderwentFGM
MotherdidnotundergoFGM
Motherhasnoeducation
Motherhashighereducation
Religionwiththehighestprevalence
Religionwiththelowestprevalence
Ethnicitywiththehighestprevalence
Ethnicitywiththelowestprevalence
Source:UNFPAanalysisbasedonDHS.GuineaDHS2012andBurkinaFasoDHS2010.
Figure 3.4. Prevalence of FGM among girls aged 10-14, by selected socio-demographic characteristics
39


4Projections
41

Overthelast20years,significanteffortshavebeenmadeatthelocal,regional
andinternationallevelstoeliminateFGM.Nonetheless,in2012,in17countries26
implementingintensiveFGMprogrammes,itwasperformedonabout12milliongirls
aged15-19.27Ifprevalenceremainsunchangedinthesecountries,by2020,
15milliongirlsbornbetween2000and2005willundergoFGM.
Figure4.1presentsprevalenceestimatesamonggirlsaged15-19basedonthemostrecentdata,andtheannualrateofreductionbasedonconsecutivesurveysin24countrieswithavailabletrenddata.Inreviewinghistoricaltrends,itispossibletogeneratetheannualrateofreduction(ARR)28for2007to2012.ThecountrieswiththehighestARRareBeninwith23percent,Nigeriawith7percentandEgyptwith6percent.Ontheotherextremearenegativeratesindicatinganincreaseinprevalence.TheseincludeGuinea-Bissauat-2.1percent,Maliat-0.9percent,andGuineaat-0.7percent.Confirmationofanincrease,however,wouldrequirefurtherexaminationofmethodologicalmatterssuchassampling.29
CountrieslikeNiger,withanARRof5percent,Kenyawith4percent,Senegalwith3percent,andBurkinaFasowith1percent,haveimplementedspecificprogrammaticinterventionsthatmayhavehadanimpactonbehaviourchangeandreductionofFGM.TheseincludeacommunityempowermentprogrammehighlightingFGMasahumanrightsviolationinSenegal,politicalwillandenforcementoflegislationbanningFGMinBurkinaFaso,andeducationonthenegativeaspectsofFGMbychurchesinKenya.CivilsocietyorganizationsandthemediahavebeenactiveinallthreecountriesinensuringthattheharmfuleffectsofFGMarewidelyknown.
26The17countriesarecoveredbythesecondphaseoftheUNFPA-UNICEFJointProgrammeonFGM/C.
27Thesecondphaseisfrom2014-2017.These17countrieswereselectedbecausemoreinformationonpolicyandprogrammaticinterventionswasavailable.
28Changeinprevalenceisassumedtotakeanexponentialfunctionsimilartotheonecalculatedas“compoundinterestrate”infinancialterms.Foranygivenyeart,iftheprevalenceisknown
tobeXt,andtheannualrateofreductionisconstantlyr%,thentheprevalenceofthenextyear,denotedasXt+1,canbecalculatedas:Xt+1=Xt*(1-r%).
29PossiblemethodologicalmattersmayalsoincludetheplacementofthequestionabouttheFGMstatusoftherespondent.P.S.Yoder,N.AbderrahimandA.Zhuzhuni.2004.Female Genital Cutting in the Demographic and Health Surveys: A Critical and Comparative Analysis.DHSComparativeReportsNo7.Calverton,Maryland:ORCMacro.
42

Figure 4.1. Percentage of girls aged 15-19 who have experienced any form of FGM, according to the most recent data, and observed annual rate of reduction in prevalence between 2007 and 2012
Notes:ARRsforcountriesthathavenothadrepeatsurveys(Cameroon,Djibouti,Iraq,LiberiaandSomalia)wereassignedavalueof0.TheratesforTogoandUgandawerealsoassignedavalueof0asprevalenceinthetwocountriesisextremelylow,andchangesmaybeinsignificant.TherateforEritreawasassignedbyusingtheaverageoftherateinneighbouringcountries(EthiopiaandSudan).AstheprevalenceinUgandaisextremelylowandthechangemaybeinsignificant,dataforitarenotpresented.
Source:UNFPAanalysisbasedonDHS,MICSandothernationalsurveys.
0-5 5 10 15 30
0
20
40
60
Prevalence of FGM/C among girls 15-19,
2012 (per cent)
80
100
Observed ARR 2007-2012
GhanaUnited Republic of Tanzania
Niger
NigeriaCARYemen
Iraq
Cameroon
Senegal
Côte d’Ivoire
Chad
Liberia
Guinea-Bissau
Burkina Faso
EthiopiaMauritania
Sierra Leone GambiaEritrea
SudanEgypt
Somalia
DjiboutiMaliGuinea
BeninTogo
Kenya
Indonesia
43

SeveralcountriesstartedtoaddresstheeliminationofFGMmorethanadecadeago.Overtheyears,theyhavebeenabletocreateafavourablepoliticalenvironment,aninstitutionalresponse,acoordinatedmultisectoralapproachandlegislationbanningFGM,whilecivilsocietyorganizationshaveimplementedwell-structuredcommunityinterventions.TheseelementsarekeyfactorstoachieveFGMabandonmentfairlyrapidly.30
Amongthe17countries,aboutsevencountriesmayaccelerateelimination,withsufficientresources.Fiveofthesevencountries—BurkinaFaso,Ethiopia,Kenya,SenegalandSudan—showapositiveannualrateofreduction,rangingfrom4.1percentto0.8percent.Forall17countries,projectionsbasedonthemostrecentprevalenceestimatesineachwereusedasbaselinestocalculatecountry-specifictargetsby2020.Areductionof40percentisenvisagedforsevencountrieswithcapacitiestoacceleratetheeliminationofFGMbetween2012and2020;areductionof15percentinDjibouti,Egypt,Guinea-Bissau,MauritaniaandMali;areductionof10percentinGambia,Guinea,NigeriaandSomalia;andareductionof5percentinYemen(Table4.1).31InNigeriaandYemen,effortstargetingFGMhavemostlycome fromcivilsocietyorganizations,althougheliminationneedstobeaddressedinacomprehensiveandorganizedmanner.32
30“UNFPA-UNICEFJointProgrammeonFGM/CSummaryReportofPhaseI2008-2013,”2014.
31ThesecondphaseoftheUNFPA-UNICEFJointProgrammeonFGM/C(2014-2017)usesaclusterapproachbasedonafewcriteriaandpossiblescenarios.OnescenarioisthatFGMabandonmentwillaccelerateatdifferentpacesintheseclusters.“UNFPA-UNICEFJointProgrammeontheAbandonmentofFemaleGenitalMutilation/Cutting:AcceleratingChange,FundingProposalforaPhaseII,2014.”
32WHO,OHCHR,UNAIDS,UNDP,UNECA,UNESCO,UNFPAandothers.“EliminatingFemaleGenitalMutilation.Aninteragencystatement.”2008.
33BaselinesurveysarethelatestDHSandMICSconductedaround2012.
Table 4.1. FGM abandonment targets in specific countries by 2020
CLUSTER OF COUNTRY
TARGET REDUCTION BETWEEN AROUND 201033
AND 2020, %
GROUP 1
BurkinaFaso
Eritrea
Ethiopia
Kenya
Senegal
Sudan
Uganda
40
40
40
40
40
40
40
GROUP 1
BurkinaFaso
Eritrea
Ethiopia
Kenya
Senegal
Sudan
Uganda
40
40
40
40
40
40
40
GROUP 2
Djibouti
Egypt
Gambia
Guinea
Guinea-Bissau
Mali
Mauritania
Somalia
15
15
10
10
15
15
15
10
GROUP 3
Nigeria
Yemen
10
5
44

OneoftheuniqueaspectsoftheanalysispresentedhereisthecalculationofthehistoricalARRforthe17targetcountriesanditscomparisonwiththeARRrequiredifthesecountriesaretomeetthereductiontargetsby2020.Figure4.2comparesthehistoricalARRbetween2007and2012andtherequiredARRbetween2012and2020foreachcountry.Countriesintheshadedareaareinabetterpositiontoachievethetargets,ashistoricalratesinthesecountriesshowafasterreductioncomparedtotherequiredrates.
Figure 4.2. Observed ARR 2007-2012, and required ARR 2012-2020, based on country targets
0 5 10-5
-5
0
Requ
ired
AR
R 2
012
-20
20
5
10
Observed ARR 2007-2012
Burkina Faso
Sudan
Ethiopia
SenegalEritea
MauritaniaEgypt
Nigeria
Kenya
Gambia
DjiboutiMali
Guinea-BissauGuinea
SomaliaYemen
ThesecountriesincludeEgypt(Group2),Nigeria(Group3)andYemen(Group3).MostcountriesclassifiedunderGroup1haveahistoricalratemuchlowerthantherequiredrate.Assuch,theyneedtoaccelerateefforts.Thisrequires,inpart,carryingoutananalysisofcurrentstrategiesandinterventions,anddeterminingwhichareasshouldbegivenmorefocus.Itmayalsorequirebalancingthefocusofprogrammaticinterventions,particularlybetweennationaladvocacywithmoreemphasisonpolicyandlegalaspects,andcommunityleveloutreachfocusedonchangingsocialnorms.
Notes:AstheprevalenceinUgandaisextremelylowandthechangemaybeinsignificant,dataforitarenotpresented.
Group1countries
Group2countries
Group3countries
Bubble size:prevalenceof
FGM/Camonggirlsaged15-19
45

Datalimitationsrequiredusingestimatesintheprojection.Assuch,thenumberofgirlsundergoingFGMbetween2010and2020wasdeterminedbyestimatingthetotalnumberofgirlsaged15-19in2020whowouldhaveundergoneFGM.Thiscohortofgirls,bornbetween2000and2005,andaged15-19in2020,willexperienceFGMatdifferentagesaccordingtotheratesobservedinthemostrecenthouseholdsurveys.AnassumptionwasmadethatthecurrentFGMprevalenceratewillremainatthesamelevelatyear2020.ThenumberofgirlsprotectedfromFGMcouldbeoverestimatedinthe“nochange”scenarioin2020(Figure4.3)ifprevalenceatthattimeisdifferentfromthecurrentrateobservedinthehouseholdsurveys.
Assumingallcountriesreachthetargetsby2020,thenumberofgirlsbornbetween2000and2005subjectedtoFGMwouldfallto11million.Thatmeansprotectingatotalof4milliongirlsfromFGM(Figure4.3).
Theprojectionsprovidestrong,compellingevidenceforthecontinuedintensiveefforttoacceleratetheeliminationofFGM,andofferaquantitativebasisforcurrentandfutureprogrammaticandfinancialinvestments.Forexample,Ethiopia,withapotentialforprotecting1.6milliongirls,mayneedmoreintensivesupportthanacountrylikeDjibouti,withatargetof6,000girls.
Basedonpopulationsize,currentlevelofFGMandcountrytargets,theprojectednumberofgirlsaged15-19whowillexperienceFGMin2020ifcurrenttrendscontinue,andtheprojectednumberifcountriesreachtheirtargetswerecalculated.ThetwoprojectionsshowthenumberofgirlswhocouldpotentiallybeprotectedfromFGM(Table4.2).Morethan70percentwouldbeinthreecountries:Ethiopiawith1.6million,Sudanwith0.8millionandEgyptwith0.5million.
InhighlypopulatedcountriessuchasEgypt,EthiopiaandNigeria,FGMprevalenceamonggirlsaged15-19is80.7percent,62.1percentand15.3percent,respectively.ThehistoricalARRare5.9percentforEgypt,2.6percentforEthiopiaandahighof7percentforNigeria.Ifthesecountriesattainthetargetsofa40percentreductionforEthiopia,15percentforEgyptand5percentforNigeria—calculatedthroughtheannualreductionrateof6.4percentforEthiopia,2percentforEgyptand1.3percentforNigeria—thenthenumberofgirlsprotectedfromFGMwouldbe1.6milliongirlsinEthiopia,0.5millioninEgyptand165,000inNigeria.InlesspopulatedcountriessuchasGuinea-Bissau,thesametypeofanalysisrevealsanFGMprevalenceamonggirlsaged15-19of48.4percent.ThehistoricalARRis-2.1percent,indicatingincreasedprevalenceinrecentyears.Guinea-Bissauhasagoalof15percent,whichcorrespondstoanannualrateofreductionof2percentforthecountry.IfGuinea-Bissaureachesthistarget,then8,000girlswouldbeprotectedfromFGMby2020.
46

Figure 4.3. Projected numbers of girls aged 15-19 who will experience FGM, under a scenario of no change and a scenario based on country targets, year 2020
2010 2020
10
12
Millions
14
16
11
12
15
4 million girls will be saved
Nochange
Scenariobasedontargets
for2020
47

Table 4.2. Projected prevalence of FGM among girls aged 15-19 and number of girls protected, and country targets, 2020
COUNTRY/FGM JOINT PROGRAMME CLUSTER
YEAR/SOURCE
PREVALENCE AMONG GIRLS AGED 15-19, MOST RECENT DATA (per cent)
HISTORICAL ARR2007-2012
GROUP 1
BurkinaFaso
Ethiopia
Kenya
Senegal
Sudan*
Uganda
Eritrea
2010DHS
2005DHS
2014DHS
2014DHS
2010SHHS
2011DHS
2002DHS
58
62
11
21
84
1
78
0.9
2.6
4.1
3.2
0.8
-
1.7
GROUP 2
Egypt
Gambia
Guinea
Guinea-Bissau
Mali
Mauritania
Djibouti
Somalia
2008DHS
2013DHS
2012DHS
2010MICS
2013DHS
2011MICS
2006MICS
2006MICS
81
76
94
48
90
66
90
97
5.9
0.6
-0.7
-2.1
-0.9
0.8
0
0
GROUP 3
Nigeria
Yemen
2013DHS
2013DHS
15
16
7.0
1.0
TOTAL
48

NUMBER OF GIRLS 15-19 EXPERIENCINGFGM, 2012 (000)
480
3019
245
149
1573
19
238
645
3930
323
191
1993
26
314
35
37
7
13
50
1
47
387
2358
194
115
1196
16
188
258
1572
129
76
797
11
125
2974
68
543
41
642
122
42
488
3141
94
693
51
906
154
39
676
69
69
85
41
77
56
76
87
2670
85
624
43
770
131
33
608
471
9
69
8
136
23
6
68
1222
231
1645
252
14
16
1481
240
165
13
Notes:Djibouti,Eritrea,SomaliaandYemenhaveonlyonedatapoint,thustheAARcannotbecalculated.TheARRforEthiopiawasassignedbyusingtheaverageoftheARRinneighbouringcountries(EthiopiaandSudan);ARRsforDjibouti,SomaliaandYemenwereassumedtobe0.
Source:UNFPAanalysisbasedonDHSandMICS.
12,096 15,073 11,138 3,935
Scenario:areductionof40percentinaccelerationcountries;areductionof15percentinDjibouti,Egypt,Guinea-Bissau,Mauritania,Mali;areductionof10percentinotheremergentcountriesplusNigeria;nochangeinothernewcountries(Yemen),byyear2020
PROJECTED NUMBER OF GIRLS 15-19 EXPERIENCING FGM IF CURRENT TREND CONTINUES, 2020 (000)
PROJECTED PREVALENCE AMONG GIRLS 15-19, 2020 (per cent)
PROJECTED NUMBER OF GIRLS 15-19 EXPERIENCING FGM, 2020 (000)
PROJECTED NUMBER OF GIRLS 15-19 PROTECTED, 2020 (000)
49

5Conclusion and
the Way Forward
51

Humanrightsviolationsagainstwomenandgirlsincludeharmfulpractices,suchaschild,earlyandforcedmarriage,andFGM;lackofreproductiverightsandreproductivehealthcare;andwomen’sandgirls’unequalaccesstoeducation,employment,leadershipanddecision-making.Thepost-2015internationalsustainabledevelopmentagendarecognizesthekeyimportanceofgenderequality,bothinitsownrightandinachievingallsustainabledevelopmentgoals.34Amajorbarriertoequalityiswomen’sandgirls’lackofcontrolovertheirbodies,andviolationsofsexualandreproductivehealthandrights.
ThereiscompellinginformationfortheneedtocontinueacceleratingandscalinguptheabandonmentofharmfulpracticessuchasFGM.Ifprogrammaticinterventionsandfinancialresourcesremainthesameordecline,over15.2milliongirlswillbesubjecttoFGMby2020.Thisnumberisstaggering.Howeverifthe17targetcountriesachievetheirtargets,4milliongirlswillbeprotectedfromFGM.
Thedataprovidedinthisreportofferreliablequantitativeinformationtodefineprogrammaticandfinancialsupport,andcanguideindividualgovernmentsandinternationaldonors.FormulatinginterventionstopreventandeventuallyeliminateFGMwillbenefitfromhavingtheevidencetodefinethesizeofthetargetpopulation,andtoorientactionaroundareasofgreatestimpact.
Anaddedbenefitofquantitativetargetsisbeingabletodeterminethecost-effectivenessofinterventions.
FGMcannotbeaddressedinisolation.Whensocietalpressurespreventwomenfrommakingdecisionsabouttheirreproductivehealthandrights,theywillalsofeelcompelledtosubjecttheirdaughterstoadeeplyingrainedpracticewithstrongculturalandritualrelevance.DemographicanalysisofFGMdemonstratesthatitisapracticethatoccurswithinspecificsocio-culturalparameters,suchasplaceofresidence,andreproductivehealthandstatus.Interventionsfocusingonabandonmenthavetotakeintoconsiderationexistinggenderinequalitiesandhowthesemanifest,includinginexacerbatinghighfertilityandperpetuatingveryyoungpopulations.
ThecasestudiesfocusingonBurkinaFasoandGuineashowthatcharacteristicssuchasthemother’seducationallevelandwhetherornotsheexperiencedFGM,religiousbackgroundandethnicityprovidevaluableinformationindeterminingwhoissubjecttoFGManddefiningthemilieuinwhichtheylive.Thisinformationcorroboratesotherstudiesfindingthatethnicandreligiousbackgroundarestrongdeterminants.
AnalysispresentedherealsostronglyhighlightstheimportanceofdatainunderstandingthecontextwithinwhichFGMprogrammesoperate,especiallythosethattargetlocalcommunities.
34“SustainableDevelopmentKnowledgePlatform—TechnicalSupportTeamIssuesBrief:GenderEqualityandWomen’sEmpowerment.”See:http://sustainabledevelopment.un.org/content/documents/2396TST%20Issues%20Brief%20GEWE_FINAL.pdf.
Genderequality,women’sempowermentandtherealizationofwomen’srights
arefundamentaltotheirwell-being,andthatoftheirfamiliesandcommunities,
andtoachievingsustainabledevelopment.
52

Forexample,Djibouti,witharapidlygrowingurbanpopulation,shouldfocusonpreventionprogrammesincities.AhighlyruralcountrysuchasGuinea-Bissauwilltakeadifferentapproach,asonlyafewethnicgroupspracticeFGM.EffortstherecouldfocusmoreonpromotingthelawagainstFGMandcommunityeducation.
Approximately130milliongirlsandwomenhaveundergoneFGMincountrieswherewehavedata.Overthepastfiveyears,prevalencehasdecreasedduetotargetedefforts,encompassingstrengthenednationalownership,capacityandleadershipforabandonment;partnershipsandcoordinationamongnationalandcommunitylevelactors;andtheintegrationofprogrammaticapproaches,strategiesandinitiativesintonationalinterventions.Theseeffortsarerootedinacomprehensive,humanrightsbased,culturallysensitiveapproach,withconsistentfocusonchangingvalueattributedtogirlsandwomenaffectedbyFGM.
Theybuildonmanycoreelementsofachievinggenderequality.Reproductivehealthprogrammescontributetoimprovementsinthestatusofwomen.Increasedschoolingforgirlsproducesmanybenefits,includingreducedfertilitylaterinlife.Legalprotectionsforwomenupholdtheirrights,backedbyadvocacyatthecommunitylevel.Communityinitiativesonreproductivehealthandgenderhaveincreasedknowledgeandgeneratedsolutionstoreduceviolenceagainstwomen,includingFGM.
Genderequalityhasacatalyticeffect
ontheachievementofinclusiveand
progressivehumandevelopment,
goodgovernance,sustainedpeace,
andharmoniousdynamicsbetween
environmentsandhumanpopulations—
allofwhichareatthecentreof
sustainabledevelopmentandhuman
rights.35
35Ibid.
53

Acknowledgements
ThisreportwasproducedbyUNFPA’sTechnicalDivision.ItwaswrittenbyMengjiaLiang(MonitoringandEvaluationAnalyst),EdilbertoLoaiza(SeniorMonitoringandEvaluationAdviser),NafissatouJ.Diop(SeniorAdviserandCoordinator,UNFPA-UNICEFJointProgrammeonFGM/C)andBerhanuLegesse(AssistantRepresentativeGender,Ethiopia).ThereportwaseditedbyGretchenLuchsingeranddesignedbyMaryMarques.
UNFPAwouldliketoacknowledgetheworkoftheGlobalAllianceAgainstFemaleGenitalMutilationforitscontributiontoprojectdataonFGM.WeextendspecialthankstocolleaguesworkingontheUNFPA-UNICEFJointProgrammeonFGM/C,theworld’slargestprogrammetoeliminatethepractice,andtoGretchenKail(ResearchAssistant)andKatherineRadke(ProgrammeAnalyst)forvaluableinputsandcomments.UNFPAwouldfurtherliketorecognizethemanygovernments,ministries,regionalbodiesandcivilsocietyorganizationsthathavecontributedvaluablesupport,expertiseanddata.
AnoteofappreciationgoestoLuisMora(ChiefoftheGender,HumanRightsandCultureBranch)andAnnPawliczko(SeniorAdviserandOfficer-in-ChargeofthePopulationandDevelopmentBranch)fortheirleadershipandsupport.
SpecialthankstoBenoitKalasa(DirectoroftheTechnicalDivision),BruceB.Campbell(GlobalCoordinatoroftheDataforDevelopmentPlatform)andMonaKaidbey(DeputyDirectoroftheTechnicalDivision)fortheirsupportinproducingthispublication.
.Photo Credits
Cover:©JeromeSessini/MagnumPhotosPage5:©NancyDurrellMcKennaPage10:©UNFPA/SvenTorfinnPage18:©NancyDurrellMcKennanPage36:©NancyDurrellMcKennaPage40:©SheilaMcKinnonPage50:©SheilaMcKinnon
Delivering a world where every pregnancy is wanted every childbirth is safe and every young person’s potential is fulfilled
UNFPA
54


United Nations Population Fund605 Third AvenueNew York, NY 10158www.unfpa.org
Egypt
Kenya
Chad1573 girls
Related Documents











