Dementia with Lewy Bodies Leonard Griffiths Thursday 22 nd Nov 07

Dementia with Lewy Bodies Leonard Griffiths Thursday 22 nd Nov 07.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dementia with Lewy Bodies
Leonard Griffiths
Thursday 22nd Nov 07
Case: Mrs ME
86♀ Admitted 2/10/07 with 2/12 Hx worsening
mobility• Leg weakness
• No altered sensation of pain
Fall noted 6/52 prior to admission• ‘mechanical sounding’
• No LOC/HI/CP/palpitations/SOB
• Recalled incident
Case: Mrs ME
Intermittent confusion for 5/52 prior to admission• Treated for UTI (although no urinary signs or
symptoms)
Case: Mrs ME
PMH• ‘Registered blind’
• Osteoporosis
• Angina
• Hypertension
• Asthma
• Episode of jaundice 40 yrs ago
PTWR
Diagnosed ‘weakness of legs’• ?musuloskeletal
• ?UTI
Abnormal results
WBC 11.5; Neut 8.2 Na+ 128
• U Osmo 566
• U Na+ <20
• P Osmo 282
• P Na+ 132 not SIADH
Abnormal results
Urine dip• Blood +
• Leuk +++
• Protein +
• Nitrites +
Lab +ve for nitrites and leukocytes• Culture ‘mixed growth suggesting contam.’
Abnormal results
AMSE• 8/10
• MMSE 20/28
• GDS 3/15• i.e. not depressed
CT brain• Moderate small vessel disease
• Small L occipital infarct
SHO WR 6/10/07
Thought pt had low mood d/w consultant ref to Ψ liaison• Felt that ‘new environment and poor eyesight
a significant factor in agitation’
Consultant WR 9/10/07
Cogwheeling Tremor Short shuffling gait ‘Leans backwards’
• Impression: Parkinsonism
• 1/52 domperidone commenced
• Ref. to PD consultant
SHO WR 11/10/07
Hallucinating• “Horse woman of the year”
• Believed someone gave her eye drops (not prescribed)
PD consultant review “Tricky mixed picture which is difficult to
disentangle”• Hallucinations
• Although ?Charles Bonnet in relation to reduced eyesight
• Some reduced memory• ?DLB but has cerebrovascular disease
• Parkinsonism – but not typical PD• ‘tremor rather fine’• ‘balance back’
Try madopar, ‘but suspect little to be gained from medication’
SHO WR 15/10/07
Hallucinating• Relatives
• Monkey
Progress…
18/10/07 madopar commenced
22/10/07 more confused and hallucinations worsening madopar stopped & rivastigmine commenced
30/10/07 – paranoia and aggressive

Progress…
6/11/07 – hallucinations worse at night quetiapine added
16/11/07 – mood even lower venlafaxine added
Now awaiting community hospital bed
Diagnosis
Clinical features reflect anatomical distribution of pathology rather than its nature
Therefore subtle clinical features not helpful
What is Dementia? ICD-10 definition
1. A decline in memory to an extent that it interferes with everyday activities, or makes independent living either difficult or impossible.
2. A decline in thinking, planning and organizing day-to-day things, again to the above extent.
3. Initially, preserved awareness of the environment, including orientation in space and time.
4. A decline in emotional control or motivation, or a change in social behaviour, as shown in one or more of the following: emotional lability, irritability, apathy or coarsening of social behaviour, as in eating, dressing and interacting with others.
• Maj, M.. 2002., Dementia, Second Edition [online]. 2nd Edition. Wiley. Available from: http://mil.ingramdigital.com/Browse/open.asp?ID=10147&loc=Cover 15 November 2007
Wikipedia definition
Dementia is the progressive decline in cognitive function due to damage or disease in the brain beyond what might be expected from normal ageing.• http://en.wikipedia.org/wiki/Dementia
Dementia Alzheimer's Vascular Lewy body Alcohol Pure vascular Frontotemporal lobar degenerations Creutzfeldt-Jakob disease Dementia pugilistica Moyamoya disease
Nomenclature
Diffuse Lewy body Disease Cortical Lewy body Disease Lewy Body Dementia Senile Dementia Of Lewy Type Lewy Body Variant of Alzheimer's
Disease Dementia with Lewy Bodies (preferred)
Dementia with Lewy Bodies
Describes several common disorders causing dementia
The main features of these conditions are:• development of dementia with features overlapping
with those of Alzheimer's disease
• development of features of Parkinson's disease
• fluctuation in severity of condition on a day-to-day basis
• early development of hallucinations
Neuropathology
Degeneration of substantia nigra
Degeneration of the cortical areas of the brain with many or all of the features seen in Alzheimer's disease
Remaining nerve cells contain abnormal structures called ‘Lewy bodies’
Lewy Bodies
Abnormal aggregation of proteins, including• alpha-synuclein, neurofilament and ubiquitin
• PD
• Dementia with Lewy bodies
• MSA
• Amyotrophic lateral sclerosis
• Hallervorden-Spatz syndrome
Core, body, halo Variations in shape
SynucleopathiesSynucleopathies
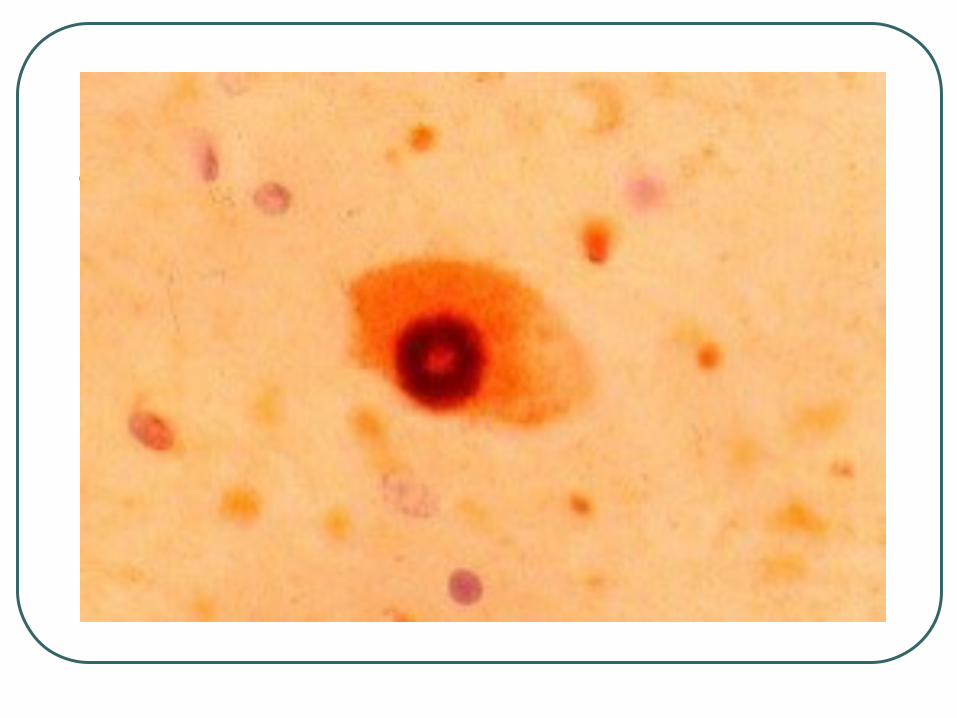
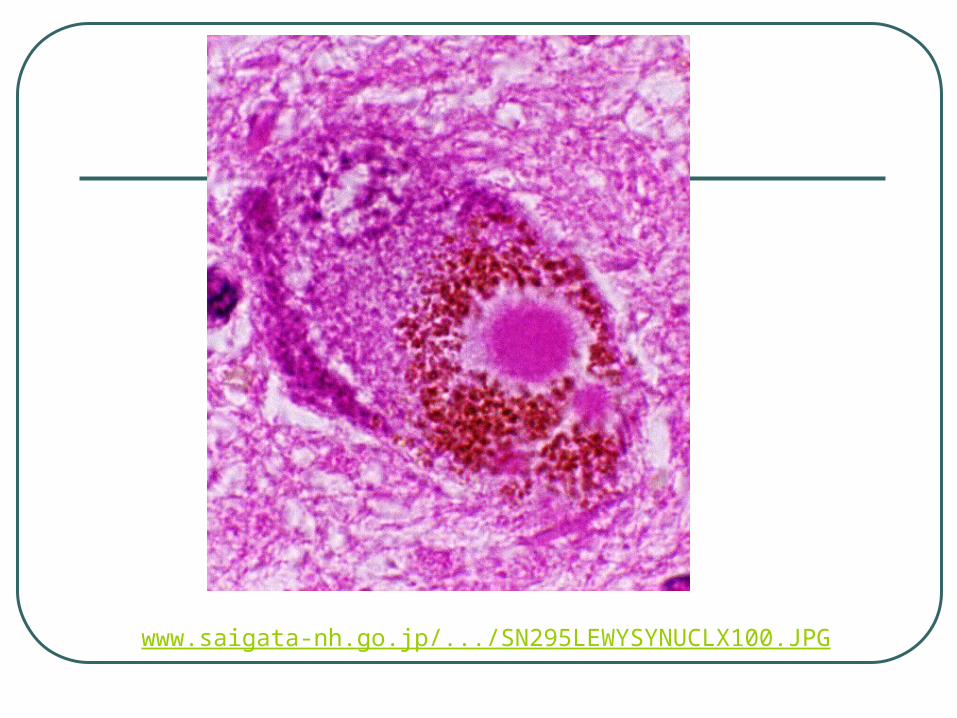
www.saigata-nh.go.jp/.../SN295LEWYSYNUCLX100.JPG
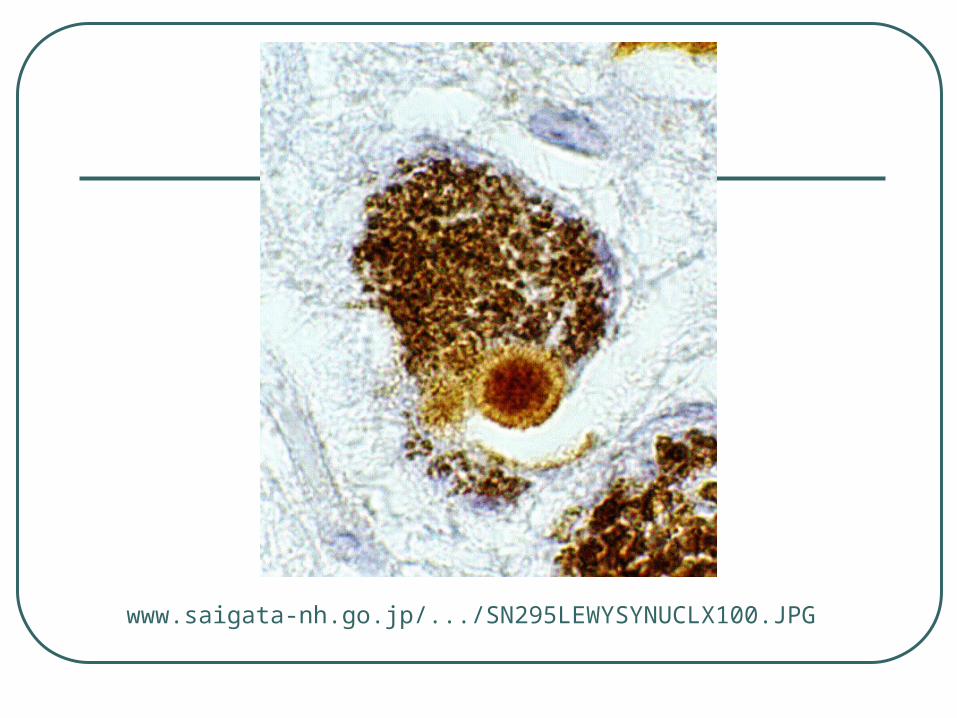
www.saigata-nh.go.jp/.../SN295LEWYSYNUCLX100.JPG
Tonus und Bewegund (Muscle Tone and Movement)
Frederich Heinrich Lewy
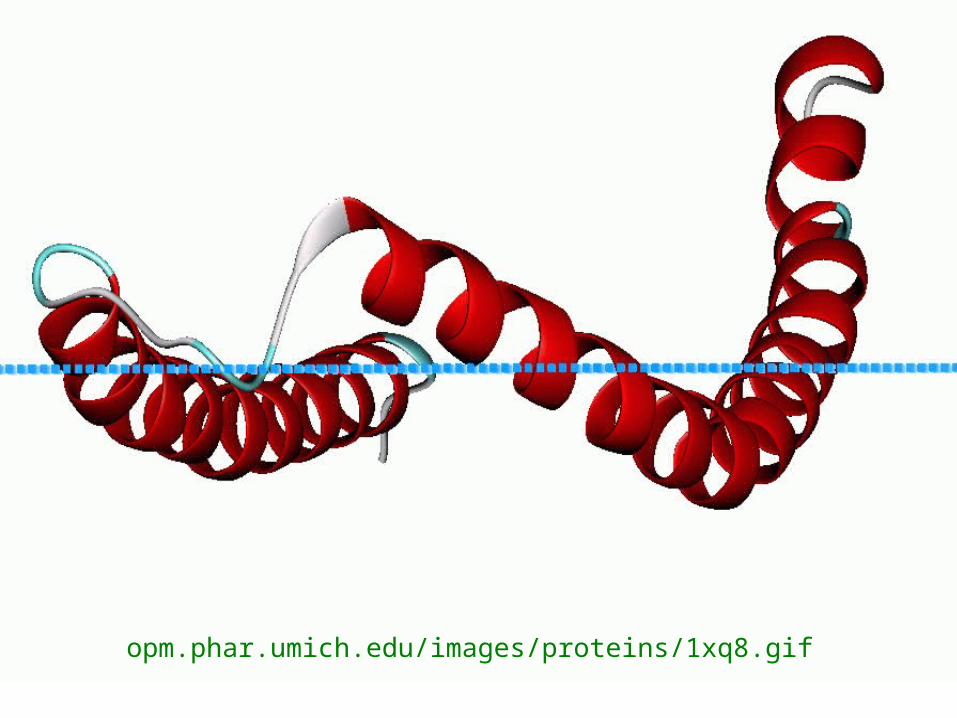
opm.phar.umich.edu/images/proteins/1xq8.gif
Alpha-synuclein
Abundant CNS protein Composed of 140 amino acids Alpha form of synuclein is the only form
capable of aggregating into fibrillar structures in vitro
Beta-synuclein is not localized in Lewy bodies, it may have a role in regulating alpha-synuclein metabolism or aggregation
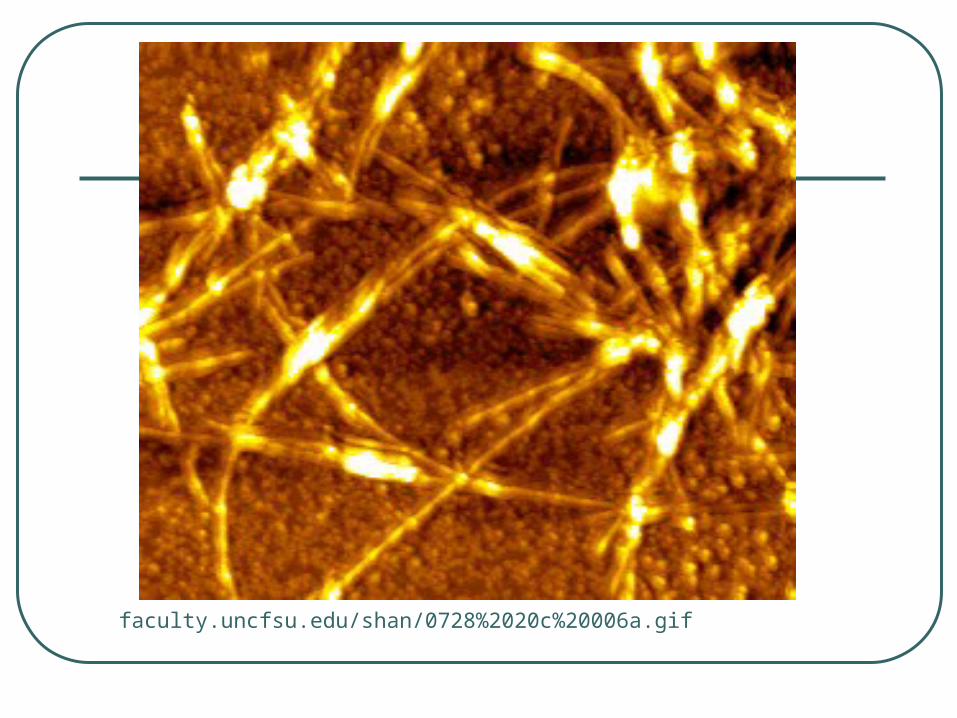
faculty.uncfsu.edu/shan/0728%2020c%20006a.gif
Normal role of alpha-synuclein
Synaptic plasticity Negative regulation of dopamine
neurotransmission Protection at nerve terminals during
injury Trafficking of cargo in the ER/Golgi
complex
Alpha-synuclein in disease
‘Ubiquitinated’ with no loss of proteasome function, suggesting there is an excessive accumulation of alpha-synuclein that overwhelms the proteolytic machinery (Tofaris, et al. 2003). This may promote the formation of Lewy bodies
Presenting Features DLB
Dementia normally presenting feature
Minority present with parkinsonism
Some with psychiatric disorder without dementia
Others with orthostatic hypotension, falls or transient disturbances of consciousness
Sporadic (rarely familial)
Common Features
Fluctuation in cognitive performance and functional ability
Variations in attention and level of consciousness
Visual hallucinations in two-thirds
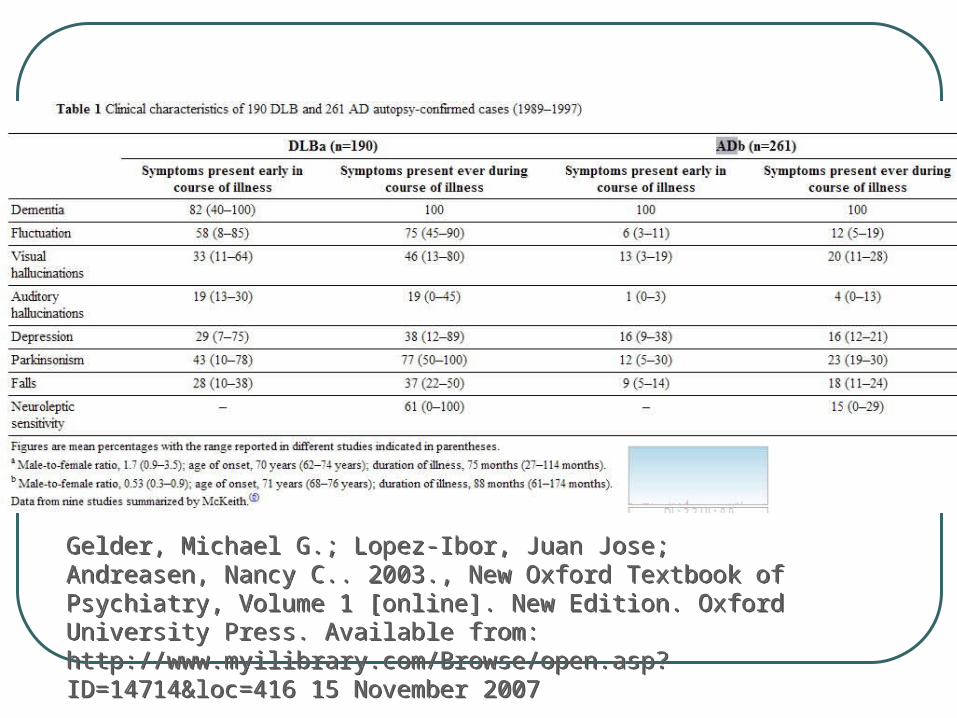
Gelder, Michael G.; Lopez-Ibor, Juan Jose; Andreasen, Nancy C.. 2003., New Oxford Textbook of Psychiatry, Volume 1 [online]. New Edition. Oxford University Press. Available from: http://www.myilibrary.com/Browse/open.asp?ID=14714&loc=416 15 November 2007
Gelder, Michael G.; Lopez-Ibor, Juan Jose; Andreasen, Nancy C.. 2003., New Oxford Textbook of Psychiatry, Volume 1 [online]. New Edition. Oxford University Press. Available from: http://www.myilibrary.com/Browse/open.asp?ID=14714&loc=416 15 November 2007
Sensitive signs for ‘bedside’ diagnosis
Psychiatric vs. cognitive symptoms• Hallucinations
• Delusions
Fluctuant cognitive state
Hallucinations
Repeated visual hallucinations are present in about two-thirds of patients• vivid, colourful, and sometimes fragmented
figures of people and animals
• often complex, detailed and rapidly moving
• can involve scenes and bizarre situations
• can start with misinterpretations and are usually short
• often occur at night
• usually not distressing to the patient
Treatment
No cure
Cognitive symptoms acetylcholinesterase inhibitors, such as donepezil and rivastigmine• May reduce psychiatric and motor symptoms
Rigidity levodopa
Summary
Third most common dementia Central feature is progressive cognitive
decline• Pronounced fluctuations
• Recurrent visual hallucinations
• Parkinsonism Symptoms caused by Lewy Bodies
comprised of bits of alpha-synuclein
Related Documents











