http://dem.sagepub.com/ Dementia http://dem.sagepub.com/content/early/2011/11/01/1471301211421837 The online version of this article can be found at: DOI: 10.1177/1471301211421837 published online 7 November 2011 Dementia Lorraine Venturato, Wendy Moyle and Andrea Steel practice documents help bridge the great divide? Exploring the gap between rhetoric and reality in dementia care in Australia: Could Published by: http://www.sagepublications.com can be found at: Dementia Additional services and information for http://dem.sagepub.com/cgi/alerts Email Alerts: http://dem.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Nov 7, 2011 OnlineFirst Version of Record >> at Griffith University on February 21, 2013 dem.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://dem.sagepub.com/Dementia
http://dem.sagepub.com/content/early/2011/11/01/1471301211421837The online version of this article can be found at:
DOI: 10.1177/1471301211421837
published online 7 November 2011DementiaLorraine Venturato, Wendy Moyle and Andrea Steel
practice documents help bridge the great divide?Exploring the gap between rhetoric and reality in dementia care in Australia: Could
Published by:
http://www.sagepublications.com
can be found at:DementiaAdditional services and information for
http://dem.sagepub.com/cgi/alertsEmail Alerts:
http://dem.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Nov 7, 2011OnlineFirst Version of Record >>
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
Article
Exploring the gap betweenrhetoric and reality indementia care in Australia:Could practice documentshelp bridge the great divide?
Lorraine VenturatoGriffith University, Australia
Wendy MoyleGriffith University, Australia
Andrea SteelRSL Care, Queensland, Australia
Abstract
Quality of care, and indeed, quality of life, for people living with dementia in long-term care is often
underpinned by philosophies of care, such as person-centred care and relationship-centred care.
The translation of these philosophies into practice is influenced by a range of individual and
organizational features, including the context in which such care occurs. Within modern care
organizations, the context of care is evidenced through organizational documents.
This study sought to identify the key documents guiding dementia care within one large
Australian long-term care organization and to explore points of consistency and tension within
the documented system of care. Results highlight a lack of consistency and clarity in the philosophy
of dementia care and a disconnection between the key documents guiding practice. This
disconnection creates tension for clinicians and carers, and may contribute to the gap between
rhetoric and reality in dementia care.
This study suggests that a congruent documented dementia system can help bridge the gap
between espoused philosophies of care and everyday care practices.
Keywords
care documents, dementia, documentation analysis, hermeneutics, person-centred care
Corresponding author:
Dr Lorraine Venturato, Research Centre for Clinical and Community Practice Innovation, Griffith Health Institute, Griffith
University, Kessels Road, Nathan, QLD 4111, Australia
Email: [email protected]
Dementia
0(0) 1–17
! The Author(s) 2011
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/1471301211421837
dem.sagepub.com
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
Introduction
People are living longer than at any other time in the past. As a result, the incidence of chronicconditions associated with ageing and longevity is rising rapidly. This is especially truefor dementia, which is widely touted to be approaching epidemic proportions (AccessEconomics Pty. Limited, 2009; Nepal, Ranmuthugala, Brown, & Budge, 2008). Globalburden of disease estimates suggest that the disability weight or burden for dementia is high(World Health Organization, 2003). In Australia, dementia is estimated to be the leadingcause of burden of disease among people aged 75 years and over and it creates the fifthhighest burden across all ages (Australia Institute of Health and Welfare (AIHW), 2010).In part, this is because people with dementia tend to be heavy consumers of health services,particularly community and long-term care services (Ferri et al., 2005). Indeed, approximately60 per cent of people living in long-term care in Australia have a recorded diagnosis ofdementia (AIHW, 2010) and this figure is estimated to be much higher if those without aformal diagnosis are considered. Furthermore, cognitive impairment is frequently a cause ofadmission to long-term care (Andel, Hyer, & Slack, 2007; Bharucha, Pandav, Shen, Dodge, &Ganguli, 2004).
Although we can do little as yet to stop the onset or progressive decline associated withdementia, healthcare professionals in community and long-term care are well placed to affectquality of care and, by extension, quality of life (Courtney, O’Reilly, Edwards, & Hassall,2009). Since the late 1990s, notions of quality in dementia care have been associated withthe philosophies of person-centred care (based on the work of Kitwood, 1997) and, morerecently, relationship-centred care (based on the work of Nolan, Davies, Brown, Keady, &Nolan, 2004), and their tenets have become foundational to considerations of qualitydementia care. Some of these tenets include the recognition of the ethical aspects ofpersonhood, including interdependence and respect (Kitwood, 1997); recognition ofthe subjective experience of the person, regardless of cognitive ability (McCormack, 2004);the use of biographical knowledge (Kellett, Moyle, McAllister, King, & Gallagher, 2010); afocus on the person over tasks (Edvardsson, Fetherstonhaugh, & Nay, 2010); and arecognition of the importance of the relationship between the person with dementia, theirfamily and care staff (Nolan et al., 2008).
Rhetoric and reality
These tenets have spawned a number of models and frameworks for practice includingthe Senses Framework (Nolan et al., 2004), the VIPS Framework (Brooker, 2007) and theperson-centred care framework (McCormack & McCance, 2006). While there is debatesurrounding the theoretical and empirical rigour of such frameworks (Edvardsson et al.,2010), it is widely accepted that, despite the best intentions of these models andframeworks, practice remains largely rooted in traditional, task-focused care, bound by thethree Rs – routines, rules and regulations (Robinson & Gallagher, 2008). As a result, it isincreasingly obvious that there is a gap between the rhetoric surrounding accepted bestpractice and the realities of everyday practice in dementia care (Draper, Low, Withall,Vickland, & Ward, 2009; Hill, 2008; Moyle, 2010).
Consequently, researchers and service providers are increasingly focusing on ways tooperationalize person- and relationship-centred care in an attempt to bridge this gapbetween rhetoric and reality. One of the approaches to achieving this is through education.
2 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
This approach focuses on developing the knowledge and skills of individual care providersto enhance their understanding and uptake of philosophical tenets into practice. However,despite some benefits, it is increasingly recognized that education on its own is not sufficientto change practice (Edvardsson et al., 2010; Nolan et al., 2008; Vollmar, Butzlaff, Lefering, &Reiger, 2007).
Other attempts at bridging the gap have focused on the link between social and physicalenvironments, with space and design principles in the built environment increasingly beingconsidered from a person- and relationship-centred viewpoint (Alzheimer’s Australia, 2004;Davis, Byers, Nay, & Koch, 2009; Fleming & Purandare, 2010). Such approaches supportdementia-friendly built environments that encourage active participation and anunderstanding of the experience of life through a social model rather than an institutionalor medical model (Davis et al., 2009). Despite more aesthetic and dementia-friendlyenvironments, there is little evidence of widespread alteration in everyday practice andquality of care for people with dementia (Edvardsson et al., 2010).
Finally, an emerging area in bridging the gap between rhetoric and reality in dementia careincorporates insights from the field of knowledge transfer, knowledge translation andknowledge utilization (Moyle, 2010). These focus around processes to facilitate thedissemination and application of research findings and the subsequent use of thisknowledge in changing practice, and embedding ‘best’ practice in a systematic andconsistent manner (Greenhalgh, Robert, Macfarlane, Bate, & Kyriakidou, 2004; Quinlan,2009). Although this approach offers the promise of actual change and alignment ofprinciples and practice, it is also limited by the requirement for specialist staff,organizational commitment and appropriate resources (Moyle, 2010).
What is evident, despite this body of work, is that, while there are some examples ofquality dementia care in practice, in general, everyday dementia care remains deeply rootedin traditional, task-focused care. A number of reasons have been proposed for this includingthe transient nature and often limited education of the long-term care workforce, the volumeof research and speed of knowledge generation in dementia care (Draper et al., 2009),the historically slow integration of research into practice (Dearing & Kreuter, 2010), andsubtle differences between knowledge dissemination (which researchers may be experiencedat), knowledge diffusion and knowledge utilisation (making changes in practice based onnew knowledge) (Dearing & Kreuter, 2010). Such challenges in the linkage of knowledge,evidence and practice are not, however, specific to dementia care or to aged care ingeneral. Indeed, such gaps lie at the very core of the evidence-based practice movement(Dopson, FitzGerald, Ferlie, Gabbay, & Locock, 2010).
In dementia care, this gap is, in part, a reflection of the fact that quality of care and qualityof life are complex and multidimensional concepts (Brod, Stewart, Sands, & Walton, 1999)at both an individual and a social level. Such complexity is compounded in the context ofbroader organizational systems, competing demands and the regulatory nature ofcontemporary long-term care provision. Together these individual, organizational andsocial factors form the context of care for people with dementia living in long-term care.
Context of care: documentation
Within modern health and social care organizations, the context of care is manifested inorganizational documents (Prior, 2003). Modern organizations and social institutionsproduce massive volumes of documented material that are wide-ranging in scope and form.
Venturato et al. 3
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from
XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
They may be hard copy or electronic, text or image or both, and relate to policy, educationor practice, including written policies, processes, guidelines, educational and trainingmaterials, forms and audits, as well as assessment and care plans, progress notes,medication administration forms, and behaviour charts. Most importantly, for thepurposes of this study, documents may be organized into themes or systems associated withorganizational endeavour (Smith, 2005) or aspects of clinical practice. Thus, it is possible toidentify an organization’s system of dementia care through its documentation and to explorethe context of dementia care through document analysis.
This paper explores an organizational care environment for people with dementia (thecontext of dementia care) evident in a documented dementia care system. This documentedsystem analysis (based on Smith, 1988, 2005) was undertaken as part of a larger study onquality of life and moral worth of people with dementia living in long-term care (Moyle, Hsu,Lieff, & Vernooij-Dassen, 2010). Specifically, this documented system analysis sought to:
(1) identify the organizational documents that guide the care of people with dementia withinone care organization;
(2) consider the context of care identified through these documents; and(3) identify consistencies and tensions within the documented system of care for people with
dementia.
Research method
The analysis method presented in this paper is based on hermeneutics and institutionalethnography. In its broadest sense, hermeneutics refers to the interpretation of texts andthe study of meaning, while institutional ethnography is concerned with the ‘textualarchitecture of routine organisational action’ (Campbell & Gregor, 2004, p. 4). The methodused is underpinned by considerations of language and tensions (Gadamer, 2004; Smith, 1988;Townsend, Langille, & Ripley, 2003). Such tensions reflect discord between the ‘truth’ ofan experience and the dominant ideology (Habermas, 1972). Identifying these tensionsis an important mediator of understanding and the essence of the hermeneutic task. Suchan approach also recognizes the broader sociocultural context of dementia and the experienceof dementia care through a focus on organizational culture, defined here as the ‘material andideational’ aspects of an organization represented through its documented systems (O’Connoret al., 2007, p. 132).
Two analytical movements are used within this study to identify tensions anduncover points of dissonance within the documented system of dementia care. First, aquestion-and-answer dialectic is used, in which questions are posed and answers soughtfrom within documents, and secondly, a process of critical reflection, moving betweenthe whole and the parts at various levels within the process of analysis is used. Thus, eachdocument is analysed as both an individual document and as part of the broader documentedsystem of dementia care.
The innovative research design used the following three-step approach:
(1) Gathering and sorting of relevant documents into a document matrix;(2) Analysis within a single document category (across-level analysis); and(3) Analysis across all document categories (drill-down analysis).
4 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from
XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
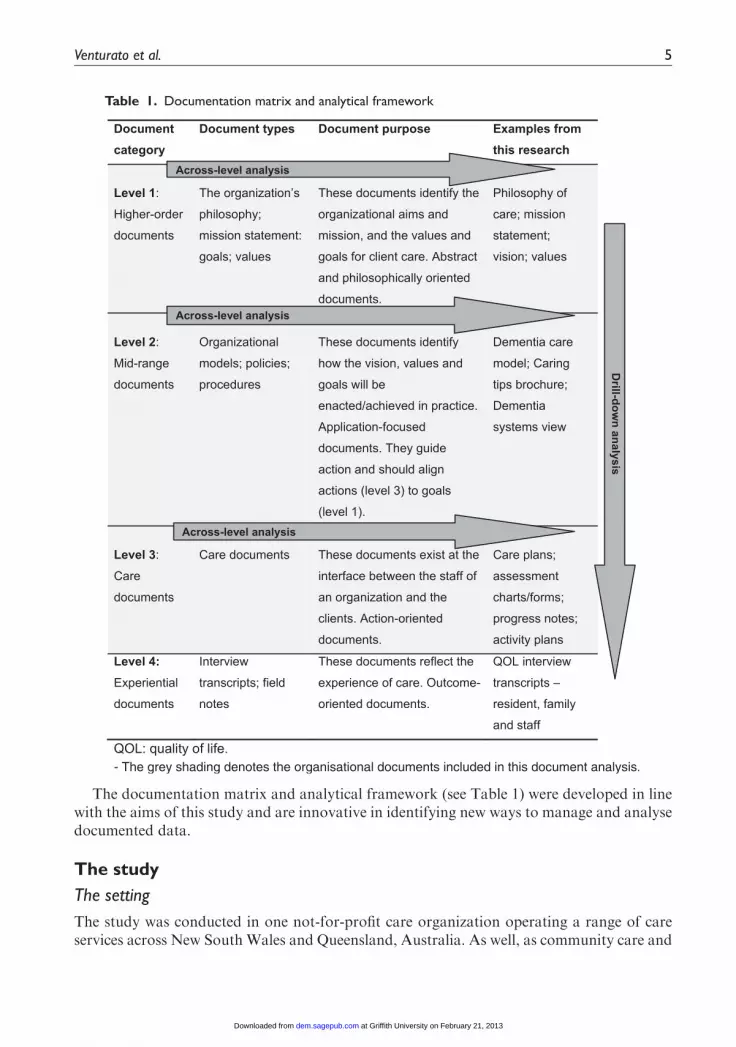
The documentation matrix and analytical framework (see Table 1) were developed in linewith the aims of this study and are innovative in identifying new ways to manage and analysedocumented data.
The study
The setting
The study was conducted in one not-for-profit care organization operating a range of careservices across New South Wales and Queensland, Australia. As well, as community care and
Table 1. Documentation matrix and analytical framework
Venturato et al. 5
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from
XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
retirement living services, the organization also operates 25 long-term care facilities, ranging insize from 60 to 160 beds. The documents involved in this study were those used across the 25long-term care facilities. Like many aged care organizations in Australia, this organization isundergoing a period of rapid growth, as smaller providers are subsumed within largerorganizations in search of ‘economies of scale’.
Ethical considerations
The study received approval from the human research ethics committee of Griffith Universityand had the support of the not-for-profit organization.While the organization was supportiveof this research, there was some concern over confidentiality and commercial sensitivitiesin relation to the reporting of organizational material. Thus, for ethical and commercialreasons the reporting of source material in this paper is limited.
Data collection
Data collection entailed an iterative and exploratory process to identify and review relevantdocuments within the organization. Documents were drawn from electronic and hard-copysources and identified:
(1) through a process of electronic searching of the organization’s document managementsystem using the terms ‘dementia’ and ‘behaviour’;
(2) through manual searches; and(3) through the organization’s dementia specialists and facility staff.
This process was aided somewhat by the organization’s document management system,which linked relevant documents, both internal and external to the organization, viahyperlinks or notation. As a result, a range of relevant documents were identified, includingbrochures, forms, policy and procedure documents, the mission statement, philosophy of caredocuments, dementia care educational resources for staff, assessment forms and care plans.
Documents underwent initial screening to ensure relevancy to the study and Table 2identifies the questions posed of each document during the initial screening. At this stage, itwas determined that documents assigned to category 1 (higher-order documents that seekto guide care) would, by necessity, include general organizational documents, that is, they didnot need to relate specifically to dementia care. This is because most care organizationsonly have one set of guiding documents; one philosophy of care document, one missionstatement and one set of organizational values. These would, therefore, be common driversfor any documented system within the organization. Category 2 (mid-range documents thatseek to operationalize aspects of care within a documented system of care, e.g. guidelines,practice models) and category 3 documents (documents used in practice at the client/staffinterface, e.g. care plans, assessment forms), however, are more specific and, in this study,dementia-specific documents were sought. Thus, documents were excluded if they related togeneral care (relevant to all clients with or without dementia). Due to the specific aims of thelarger study, it was determined that category 4 documents (those that reflect outcomes of care,e.g. interviews, observations, satisfaction surveys) would be dealt with solely from a researchfocus. Results of the category 4 analysis are published separately (Moyle et al., 2011a; Moyleet al., 2011b).
6 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
The above process resulted in a final set of organizational documents that were dementia-focused and covered policy, care, education, practice and regulation/standards. Thesedocuments were then catalogued into one of the three levels of the documentation matrixaccording to their category (see Table 1). Following this, the analysis occurred, first acrosseach of levels 1–3 followed by a drill-down analysis through each level within the matrix.Analysis considered language, context, history and culture, as well as temporal changesevident within the documents (Gadamer, 2004). This level of analysis aimed to develop anunderstanding of the key elements of each category, including congruent or shared featuresand those that reflect a disconnection or that created dissonance and, therefore, tension withinthe documented system. The final stage of analysis involved a drill-down analysis to considerdocuments across all four categories in order to consider congruency, disconnections andtensions between the categories.
Results
Two main themes emerged from the analysis of each category and of the system as a whole.The first of these themes is titled ‘Aspiring, delivering, doing’ in response to the purpose andfocus of each document category. The second theme is titled ‘The great divide’ in response tothe findings from the drill-down analysis. Each theme contains a number of sub-themes.
Aspiring, delivering, doing
Aspiring . . . What we want to do!. Category 1 documents are aspirational in nature, in thatthey identify the values and goals of the organization. Documents in this category serve as thephilosophical and theoretical drivers for the provision of care within the organization, andincluded the philosophy of care, mission, vision and value statements. Analysis of thiscategory, as a whole, reveals a focus on the individual and on responsiveness to individualneeds (both client and staff). The philosophy of care is referred to as the ‘lifestyle approach’and this reflects a focus on supporting the maintenance of individualized choice and lifelonggrowth and participation as key outcomes for clients. Values identified within thesedocuments included concepts such as honesty, integrity, trust, caring, respect and openness.In general, these documents identify with concerns about the individual’s health, well-being,choice, decision-making and complex relationships.
Despite a general consistency in the focus of most of these documents, there are alsosome inconsistencies within this category, and a point of dissonance. Inconsistencies areparticularly evident in the philosophy of care documents whereby a number of versions ofthese documents were evident and rather than old versions being archived as the documents
Table 2. General questions posed at the initial screening of each document
1. What is the key focus of the document?
2. Who is the intended audience? Who is the document aimed at?
3. What concepts and terms are used?
4. What values (if any) are outlined in the document?
5. What purpose does the document serve?
6. Is there anything you would expect to see in this type of document and don’t?
Venturato et al. 7
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
were revised, they remained active in the system. While this led to some inconsistency andconfusion, it did facilitate understanding of the development and evolution of this keydocument over time. For example, the addition of terminology associated with ‘evidence-based practice’ emerged in the most recent versions of the document, but was not evident inthe original versions.
The organization’s mission statement was also identified as a point of dissonance as thisstatement took a completely different focus to other documents in this category, by identifyingthe organization’s mission in business terms (‘industry leader’; ‘first choice provider’), ratherthan in service terms, such as care. This dissonance creates a subtle tension in organizationalidentity and focus within the documents and this tension between business and care ishighlighted further by the organization’s listing as a not-for-profit setting.
Delivering . . . How we are going to achieve this!. Category 2 documents specifically serveto guide and direct the care of the person with dementia. Documents in this category includethe organization’s Dementia Approach (care model), dementia system views, brochuresand process documents relating to the care of people with dementia and staff training andeducational materials associated with dementia care. These documents draw heavily on thework of Kitwood (1997) and are based, to a greater or lesser degree, on a person-centred carephilosophy that recognizes the uniqueness of each individual. The key document in thiscategory is the Dementia Approach (referred to as the Dementia Management Model),which is aligned to the National Framework for Action on Dementia (2006–2010)(Australian Health Ministers’ Conference (AHMC), 2006) and includes value statementsassociated with inclusion, respect, personhood, sustaining and flexibility.
There are two sub-themes evident in the documents in this category. Firstly, the personwith dementia is recognized as an individual whose personhood is to be valued and respected,and secondly, staff knowledge, skill and specialist support is considered to be a vitalcomponent of dementia care. Documents across this category display a high degreeof congruency and indeed, most of them were authored by the same small group ofspecialist staff.
Doing . . . What we do when staff and residents come together!. Category 3 documentsare those used in the practice domain, where staff and clients come together in the processof assessing, planning and documenting care of the person with dementia. Across-levelanalysis suggests that this category of documents is also reasonably consistent in its focus.While there are no stated values inherent in these documents, they do reflect a fairlytraditional, biomedical focus, with an emphasis on physical care and identifying clientdeficits and limitations, with relatively less emphasis on psychosocial care and capacity.
Documents within this category frequently paid homage to category 1 documents(particularly in their title), without necessarily embracing the values and concepts espousedin category 1 documents. For example, the ‘Lifestyle support needs’ document includesmedication and pain management without mentioning client choice or holistic care, whilethe ‘Lifestyle issues’ document covers skin integrity, eating and drinking, toileting, mobilityand safety management.
While there were some exceptions, these documents largely reflected a biomedicalapproach to assessment and care planning, although there was some limited evidence ofpsychosocial data capture (primarily around terminal care beliefs, funeral arrangements,alcohol and smoking preferences, and aspects of life which are important to the individual).
8 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
While well-being and communication needs were identified within the documents, they wereagain largely conceptualized from a biomedical perspective. For example, well-being for theperson with dementia was measured using a combination of the Psychogeriatric AssessmentScale (PAS) and Cognitive Impairment Scale (CIS), as well as various behaviour anddepression scales. While the organizational documentation includes a form titled ‘Myprofile’, which aims to assist staff in ‘identifying and rekindling past pleasurable activitiesthat might be still within the resident’s capabilities’ and ‘to get to know the residents better’,there is little evidence that this form, which is used by the diversional therapists in planningactivities, is actually linked to individual activity plans. Thus, even where assessmentdocuments do offer some support for individualized care, this is rarely carried through inaction-oriented (planning) documentation.
Table 3 highlights the findings from the analysis of each document category.
The great divide
Not surprisingly, given the above results, the drill-down analysis of the document system as awhole highlighted a significant tension. This tension occurred between category 1 and 2documents, which were reasonably compatible, and those in category 3. In many ways, thisis a reflection of the broader tension between rhetoric and reality discussed earlier in thispaper.
This tension sees a marked shift in purpose, function and focus of documents withincategory 3 and breaks the focus on the individual. This shift to a biomedical structure andfocus is evident in the assessment documents in particular, and includes a shift tomeasurementand losses/limitations, as opposed to capacity and holistic considerations. By applying abiomedical view, category 3 documents promote a standardized view of people withdementia, and residents in general, with little capacity for individualization. Category 3documents are found at the interface between clients and staff and are essentially action-oriented documents, that is, they have effects (Prior, 2003), and this change in focus servesto redirect practice and action away from the individual needs. As Smith (1988) suggests,everyday experience is regulated by organizational practices and policies (throughdocumented systems), and these shape both the experience of care (for clients) and thepractice of care (for staff).
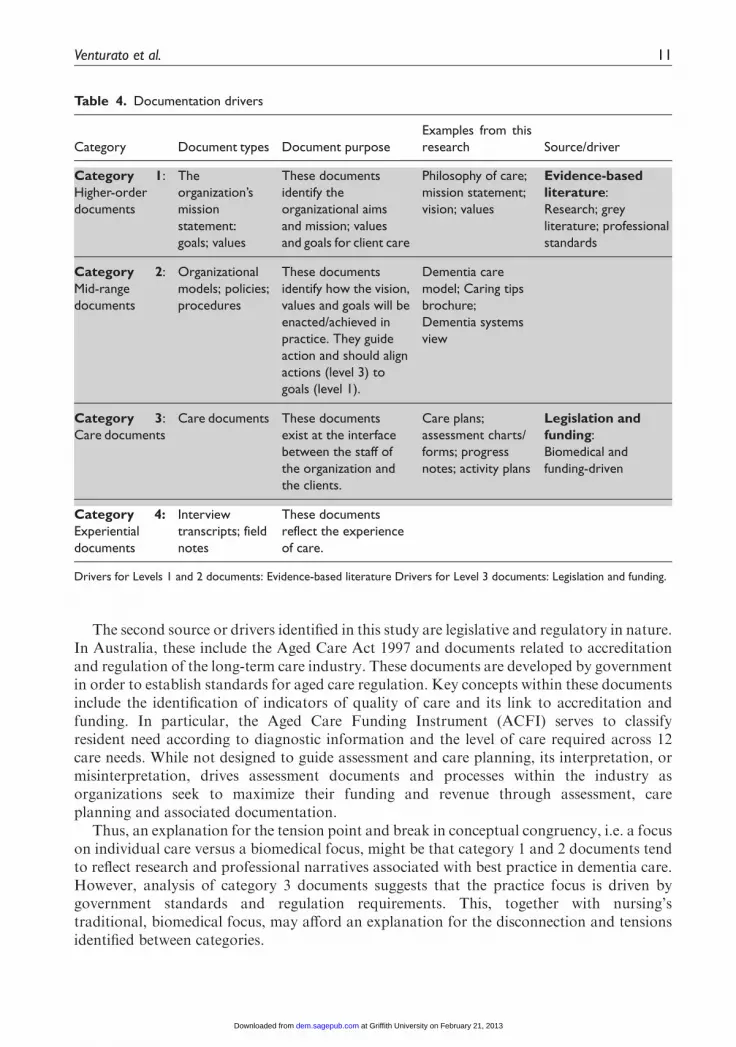
One possible explanation for this disconnection between category 1/2 and category 3documents is the document drivers. In this study, two principal sources or drivers areidentified:
(1) Professional discourses and evidence-based literature; and(2) Legislation and regulation-based documents (see Table 4).
Professional and research-based literature reflects the professional knowledge base andprofessional standards for practice. These are reflected in professional guidelines, research,evidence-based practice information and professional discussions. The key conceptsembedded in contemporary, professional literature related to dementia care include notionsof personhood, person and relationship-centred care, and quality of life (Venturato, 2010).These are evident in, and consistent with, the key themes identified in category 1 and 2documents.
Venturato et al. 9
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
Tab
le3.
Docu
menta
tion
mat
rix
and
acro
ss-lev
elan
alys
is
Docu
mentc
atego
ryD
ocu
ment
types
Docu
ment
purp
ose
Exam
ple
sfr
om
this
rese
arch
Acr
oss
-leve
lan
alys
is
Cate
go
ry
1:
Hig
her-
ord
er
docu
ments
Philo
sophy
ofth
e
org
aniz
atio
n;m
issi
on
stat
em
ent;
goal
s;va
lues
These
docu
ments
identify
the
org
aniz
atio
nal
philo
sophy;
aim
san
d
mis
sion;va
lues
and
goal
s
for
clie
nt
care
.T
hese
are
theore
tica
lly,ab
stra
ctan
d
philo
sophic
ally
ori
ente
ddocu
ments
.
Philo
sophy
ofca
re;m
issi
on
stat
em
ent;
pro
duct
know
ledge
guid
e;vi
sion;
valu
es
Pu
rpo
se:A
spir
atio
nal
docu
ments
;bas
ed
on
the
resp
onsi
veness
toin
div
idual
needs
Co
reele
men
ts:In
div
idual
atth
ece
ntr
e
Valu
es:
Honest
y,in
tegr
ity,
trust
,ca
ring,
resp
ect
and
openness
Mess
age:R
elat
ionsh
ips,
care
,etc
.are
des
igned
toenhan
cech
oic
e,h
ealth,w
ellb
ein
g,par
tici
pat
ion
and
life-
long
grow
th.
Cate
go
ry
2:
Mid
-ran
ge
docu
ments
Org
aniz
atio
nal
models
;
polic
ies;
pro
cedure
s
These
docu
ments
identify
how
the
visi
on,va
lues
and
goal
sw
ill
be
enac
ted/a
chie
ved
inpra
ctic
e.
These
are
applic
atio
n-f
ocu
sed
docu
ments
.T
hey
guid
eac
tion
and
should
alig
nac
tions
(lev
el3)
togo
als
(lev
el1).
Dem
entia
care
model;
Par
tners
hip
sin
dem
entia
care
;C
arin
gtips
bro
chure
;
Dem
entia
syst
em
svi
ew
;D
em
entia
educa
tion
and
trai
nin
gm
ateri
als
Pu
rpo
se:To
guid
eth
eca
reofth
ePW
D;st
aff
educa
tion
and
trai
nin
g
Co
reele
men
ts:B
ased
on
pers
on-c
entr
ed
care
;
uniq
ueness
ofeac
hin
div
idual
.A
ligned
toth
e
Nat
ional
Fram
ework
for
Act
ion
on
Dem
entia
(2006–2010)
Valu
es:
Incl
usi
on,re
spect
,pers
onhood,
sust
ainin
g,fle
xib
ility
Mess
age:
1.T
he
PW
Dis
anin
div
idual
whose
per
sonhood
is
tobe
valu
edan
dre
spec
ted.
2.S
taff
know
ledge
,ski
llsan
dsp
ecia
listsu
pport
isa
vita
lco
mponen
tofdem
entia
care
.
Cate
go
ry
3:
Car
edocu
ments
Car
eD
ocu
ments
These
docu
ments
exis
tat
the
inte
rfac
e
betw
een
the
staf
fofan
org
aniz
atio
n
and
the
clie
nts
.T
hese
are
action-
ori
ente
ddocu
ments
.
Car
epla
ns;
asse
ssm
ent
char
ts/form
s;pro
gress
note
s;ac
tivi
typla
ns
Pu
rpo
se:A
ssess
ing,
pla
nnin
gan
ddocu
menting
care
;au
ditin
gan
dac
creditat
ion
Co
reele
men
ts:B
io-p
sych
o-s
oci
aldat
a
Valu
es:
(Im
plie
d)
bio
medic
alin
nat
ure
,
pre
scri
ptive
.
Mess
age:St
rong
em
phas
ison
phy
sica
l
care
and
limitat
ions;
less
em
phas
ison
psy
choso
cial
care
and
capac
ity.
Cate
go
ry
4:
Experi
ential
docu
ments
a
Resi
dent
satisf
action
surv
eys;
com
pla
ints
;
rese
arch
docu
ments
These
docu
ments
refle
ctth
e
experi
ence
ofca
re.T
hese
are
outc
om
e-o
riente
ddocu
ments
.
Report
ed
els
ewhere
Report
ed
els
ew
here
PW
D:pers
on
with
dem
entia.
aD
ocu
ments
inth
isca
tego
ryin
clude
rese
arch
(inte
rvie
wtr
ansc
ripts
;surv
eys;
obse
rvat
ions;
and
field
note
s)an
dorg
aniz
atio
nal
docu
ments
(resi
dent
satisf
action
surv
eyre
port
s;re
sident
and
fam
ilyco
mpla
ints
,etc
.).T
hese
docu
ments
are
not
incl
uded
inth
isdocu
ment
anal
ysis
.T
he
grey
shad
ing
denote
sth
eorg
aniz
atio
nal
docu
ments
incl
uded
inth
isdocu
ment
anal
ysis
.
10 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from
XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
The second source or drivers identified in this study are legislative and regulatory in nature.In Australia, these include the Aged Care Act 1997 and documents related to accreditationand regulation of the long-term care industry. These documents are developed by governmentin order to establish standards for aged care regulation. Key concepts within these documentsinclude the identification of indicators of quality of care and its link to accreditation andfunding. In particular, the Aged Care Funding Instrument (ACFI) serves to classifyresident need according to diagnostic information and the level of care required across 12care needs. While not designed to guide assessment and care planning, its interpretation, ormisinterpretation, drives assessment documents and processes within the industry asorganizations seek to maximize their funding and revenue through assessment, careplanning and associated documentation.
Thus, an explanation for the tension point and break in conceptual congruency, i.e. a focuson individual care versus a biomedical focus, might be that category 1 and 2 documents tendto reflect research and professional narratives associated with best practice in dementia care.However, analysis of category 3 documents suggests that the practice focus is driven bygovernment standards and regulation requirements. This, together with nursing’straditional, biomedical focus, may afford an explanation for the disconnection and tensionsidentified between categories.
Table 4. Documentation drivers
Category Document types Document purpose
Examples from this
research Source/driver
Category 1:
Higher-order
documents
The
organization’s
mission
statement:
goals; values
These documents
identify the
organizational aims
and mission; values
and goals for client care
Philosophy of care;
mission statement;
vision; values
Evidence-based
literature:
Research; grey
literature; professional
standards
Category 2:
Mid-range
documents
Organizational
models; policies;
procedures
These documents
identify how the vision,
values and goals will be
enacted/achieved in
practice. They guide
action and should align
actions (level 3) to
goals (level 1).
Dementia care
model; Caring tips
brochure;
Dementia systems
view
Category 3:
Care documents
Care documents These documents
exist at the interface
between the staff of
the organization and
the clients.
Care plans;
assessment charts/
forms; progress
notes; activity plans
Legislation and
funding:
Biomedical and
funding-driven
Category 4:
Experiential
documents
Interview
transcripts; field
notes
These documents
reflect the experience
of care.
Drivers for Levels 1 and 2 documents: Evidence-based literature Drivers for Level 3 documents: Legislation and funding.
Venturato et al. 11
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from
XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
Implications and discussion
Two issues associated with the delivery of quality care for people with dementia havebecome apparent in recent times. The first of these is the challenge of operationalizingperson-centred care and relationship-centred care concepts in everyday practice. Thischallenge is evident in the recognition of a gap between practice and theory commonlybeing referred to as the gap between rhetoric and reality in dementia care (Moyle, 2010).This gap is generally considered in one of two ways: as an individual practitioner issue,usually related to knowledge or attitude (Moyle et al., 2010); or as a function of the workenvironment, associated with workload and time constraints, which are seen to limitopportunities for individualized care and interaction (Edvardsson, Sandman, Nay, &Karlsson, 2009).
This study suggests a third possibility: that documented systems of care withinorganizations serve to maintain this gap through directing action (and interaction) towardsstandardized, biomedical and task-focused practices. This may be because ‘people routinelyconduct their work through texts, forms and reports’ (Campbell & Gregor, 2004, p. 33).Indeed, it is recognized that organizational culture (including values and beliefs, resourceallocation, textual systems and even architecture) contributes to ‘shaping the nature ofservices and the manner in which they are delivered’ (O’Connor et al., 2007, p. 132).
This has a number of implications for people with dementia, the staff caring for themand the organizations providing care services. For people with dementia, the implicationsinclude a sense of being devalued (Moyle et al., 2010), limitations to the quality ofindividualized care, and ultimately, limitations to their quality of life. For staff, the tensionbetween aspiring/delivering (what they should do) and doing (what they actually do) can leadto role strain and burnout (Edvardsson et al., 2009). For organizations, the developmentof effective systems and efficient processes is essential to the delivery of quality care, as wellas their sustainability in themarketplace. Tensions within documented systemsmay impact onstaff engagement and retention (Venturato, Kellett, & Windsor, 2007), as well as theirability to deliver quality care. It also limits the efficiency and effectiveness of organizationalprocesses.
This study suggests that organizations, and in particular those within organizationswho write policy, procedure and practice documents should consider their documentedsystems as a whole, rather than focusing on individual documents as single entities. Suchconsideration would seek to align practice documents with aspirational documents in orderto minimize tensions within the system. Furthermore, a congruent documented dementiacare system may help bridge the gap between espoused philosophies of care and everydaycare practices.
The second issue associated with the delivery of quality care for people with dementiacentres on processes for changing practice. This has become particularly evident inconsideration of knowledge transfer and utilization and the evidence-based practice (EBP)movement (Moyle, 2010; Masso & McCarthy, 2009). While EBP has largely focused onchange at the individual level, quality improvement processes have often focused onsystems and processes (Masso & McCarthy, 2009). While it is not the intent of this paper toengage in a lengthy discussion relating to developing EBP processes, this study does suggeststhat consideration of documented systems of care may offer an approach to bridge this gapbetween EBP and quality improvement processes and link individual action and practice withsystem and process issues.
12 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
For example, current literature suggests that care planning in long-term care shouldincorporate resident involvement and procedures for ongoing consent (Butterworth, 2005;Worden & Challis, 2008), as well as narrative approaches (Heliker, 1999). It is also recognizedthat biographical, as well as biological data needs to be captured, particularly in care planningin chronic conditions (Kellett et al., 2010). Traditional EBP approaches focused on theindividual practitioner would support education and skill development to reframe careplanning processes. However, findings from this study suggests that changing care planningpractices within the organization also requires changes to the documented system – in bothclinical documents (assessments and care plans) and policy and process documents. Given thattexts shape actions (Prior, 2003), changing practice needs to consider both the individualpractitioner and the systemic issues that shape their practice.
A third issue associated with the delivery of quality care for people with dementia hasbecome apparent in this study: the issue of different drivers that shape organizationalsystems. Within aged care in Australia, organizational systems are shaped by researchand profession discourses, as well as by legislative and regulatory structures. While researchand professional discourse focus on best practice and quality of care issues, in general,regulatory and legislative structures focus on industry control and the policing of minimumstandards, and quality is conceptualized as a measure of economic efficiency. Thus, thesedrivers serve very different purposes.
O’Connor et al. (2007, p. 132) suggest that:
‘. . . at any given time, there are multiple and competing discourses, or storylines, available through
which one can make sense of the world . . . [and] to develop a contextualized account ofpersonhood in dementia, it is necessary to identify and interrogate the different storylines thatare being used to construct the dementia experience in relation to their social, historical and
political contexts’.
They also note that research that considers these varied contexts is only just beginningto emerge.
This study supports the need for further research and ‘interrogation’ of the politicalcontext as a contributor to the broader social discourse and as a shaper of organizationalstructures and systems. In this respect, this study supports that of Downs (2000) who called fora comprehensive and multidimensional vision of care for people with dementia that includesthe personal (subjective), the organizational and the broader social and political storylines.
Limitations of the study
It should be noted that the findings are drawn from one research study and one long-termcare organization. Other organizations may have a different structure in their documentsystems, for example, a three-level document system. There may also be a place within thisapproach for broader policy and external document review as drivers and as a source ofanalysis. A comprehensive system analysis, incorporating category 4 documents (outcomesof care) may also be useful, particularly if considering broader documented systems of care(e.g. beyond one organization). It is also outside the scope of this study to establish howpractice (category 3) documents may be modified to incorporate philosophical concepts ofcare and whether this would indeed enhance quality of care and quality of life for people livingwith dementia in long-term care.
Venturato et al. 13
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from
XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
Conclusions
This study of a documented system of dementia care offers further insights into both thecontext of care for people with dementia living in long-term care and the tensions inherentwithin such systems. These tensions within the system go some way towards explainingthe complex web of issues associated with grounding philosophical notions of bestpractice, such as person-centred care, in everyday practice. In this way, this study adds afurther dimension to understanding the gap between rhetoric and reality in dementia care andmoves such understanding beyond the individual practitioner to include broader system andcontextual challenges. Furthermore, the findings from this study suggest that documentedsystem analysis is a useful methodological approach to understanding organizational andcontextual issues associated with quality of care within long-term care organizations.
Funding
This study was funded by the Australian Research Council (LPO775127; Moyle, W., McAllister, M.,
Venturato, L., & Oxlade, D.) under the Linkage Project Scheme for 2007–2010 and collaborating
industry partner RSL Care, Queensland, Australia.
Acknowledgments
We would like to acknowledge the management, staff and residents who participated in this research.
Notes
1. The VIPS definition of person-centred care, as defined by Brooker (2007), encompasses four majorelements:
V: Valuing people with dementia and those who care for them.I: Individualized care.P: The perspective of the person.
S: Supportive social psychology.
References
Access Economics Pty. Limited (2009) Keeping dementia front of mind: incidence and prevalence 2009–2050. Final report for Alzheimer’s Australia. Canberra: from http://www.alzheimers.org.au/research-
publications/access-economics-reports.aspx.Alzheimer’s Australia (2004) Dementia Care and the Built Environment. Position Paper Number 3 (June
2004). Canberra: Alzheimer’s Australia. Retrieved August 24, 2011, from http://www
.alzheimers.org.au/research-publications/alzheimers-australia-numbered-publications.aspx.Andel, R., Hyer, K., & Slack, A. (2007). Risk factors for nursing home placement in older adults with
and without dementia. Journal of Aging and Health, 19(2), 213–228.Australian Health Ministers’ Conference (AHMC) (2006) National Framework for Action on Dementia
2006–2010 (pp. 2–7). Sydney: New South Wales Department of Health. Retrieved August 24, 2011,from http://www.alz.co.uk/sites/default/files/australia_plan.pdf.
Australian Institute of Health and Welfare (AIHW) (2010) Australia’s Health 2010. Canberra: AIHW.
Retrieved August 24, 2011, from http://www.aihw.gov.au/publication-detail/?id¼6442468376&tab¼2.
Bharucha, A. J., Pandav, R., Shen, C., Dodge, H.H., &Ganguli,M. (2004). Predictors of nursing facility
admission: a 12-year epidemiological study in the United States. Journal of the American GeriatricsSociety, 52(3), 434–439.
14 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
Brod, M., Stewart, A. L., Sands, L., & Walton, P. (1999). Conceptualization and measurement of
quality of life in dementia: the dementia quality of life instrument (DQoL). Gerontologist, 39(1),25–35.
Brooker, D. (2007). Person-centred dementia care. Making services better (Bradford Dementia Group
Good Practice Guides). London: Jessica Kingsley Publishers.Butterworth, C. (2005). Ongoing consent to care for older people in care homes. Nursing Standard,
19(20), 40–45.Campbell, M., & Gregor, F. (2004).Mapping social relations: a primer in doing institutional ethnography.
Walnut Creek, CA: AltaMira Press.Courtney, M., O’Reilly, M., Edwards, H., & Hassall, S. (2009). The relationship between clinical
outcomes and quality of life for residents of aged care facilities. The Australian Journal of
Advanced Nursing, Vol. 26(4), 49–57 (Retrieved August 24, 2011, from http://www.ajan.com.au/Vol26/26-4_O’Reilly.pdf.
Davis, S., Byers, S., Nay, R., & Koch, S. (2009). Guiding design of dementia friendly environments
in residential care settings: Considering the living experiences. Dementia, 8(2), 185–203.Dearing, J. W., & Kreuter, M. W. (2010). Designing for diffusion: how can we increase uptake of
cancer communication innovations. Patient Education and Counseling, 81(Suppl), S100–S110.Dopson, S., FitzGerald, L., Ferlie, E., Gabbay, J., & Locock, L. (2010). No magic targets!
Changing clinical practice to become more evidence based. Health Care Management Review,35(1), 2–12.
Downs, M. (2000). Dementia in a socio-cultural context: An idea whose time has come. Ageing and
Society, 20(3), 369–375.Draper, B., Low, L. F.,Withall, A., Vickland, V., &Ward, T. (2009). Translating dementia research into
practice. International Psychogeriatrics / IPA, 21(Suppl 1), S72–S80.
Edvardsson, D., Fetherstonhaugh, D., & Nay, R. (2010). Promoting a continuation of self andnormality: person-centred care as described by people with dementia, their family members andaged care staff. Journal of Clinical Nursing, 19(17–18), 2611–2618.
Edvardsson, D., Sandman, P. O., Nay, R., & Karlsson, S. (2009). Predictors of job strain in residentialdementia care nursing staff. Journal of Nursing Management, 17(1), 59–65.
Ferri, C. P., Prince, M., Brayne, C., Brodaty, H., Fratiglioni, L., Ganguli, M., et al. (2005). Globalprevalence of dementia: a Delphi consensus study. Lancet, 366(9503), 2112–2117.
Fleming, R., & Purandare, N. (2010). Long-term care for people with dementia: environmental designguidelines. International Psychogeriatrics / IPA, 22(7), 1084–1096.
Gadamer, H. G. (2004). Truth and method (2nd Rev. ed.). Translation revised by Weinsheimer, J. &
Marshall, D. G. New York: The Continuum International Publishing Group.Greenhalgh, T., Robert, G., Macfarlane, F., Bate, P., &Kyriakidou, O. (2004). Diffusion of innovations
in service organizations: systematic review and recommendations. The Milbank Quarterly, 82(4),
581–629.Habermas, J. (1972). Knowledge and human interests. Translated by Shapiro, J. Boston, MA: Beacon
Press.
Heliker, D. (1999). Transformation of story to practice: an innovative approach to long-term care. Issuesin Mental Health Nursing, 20(6), 513–525.
Hill, H. (2008). Talk but no walk: barriers to person-centred care. Journal of Dementia Care, 16(4),21–24.
Kellett, U., Moyle, W., McAllister, M., King, C., & Gallagher, F. (2010). Life stories and biography: ameans of connecting family and staff to people with dementia. Journal of Clinical Nursing, 19(11–12),1707–1715.
Kitwood, T. (1997). Dementia reconsidered: the person comes first. Maidenhead: Open University Press.Masso,M., &McCarthy, G. (2009). Literature review to identify factors that support implementation of
evidence-based practice in residential aged care. International Journal of Evidence-Based Healthcare,
7(2), 145–156.
Venturato et al. 15
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
McCormack, B. (2004). Person-centredness in gerontological nursing: an overview of the literature.
Journal of Clinical Nursing, 13(3a), 31–38.McCormack, B., & McCance, T. V. (2006). Development of a framework for person-centred nursing.
Journal of Advanced Nursing, 56(5), 472–479.
Moyle, W. (2010). Is quality of life being compromised in people with dementia in long-term care?International Journal of Older People Nursing, 5(3), 245–252.
Moyle, W., Hsu, M. C., Lieff, S., & Vernooij-Dassen, M. (2010). Recommendations for staff educationand training for older people withmental illness in long-term aged care. International Psychogeriatrics
/ IPA, 22(7), 1097–1106.Moyle, W., Venturato, L., Griffiths, S., Grimbeek, P., McAllister, M., Oxlade, D., et al. (2011a). Factors
influencing quality of life for people with dementia: a qualitative perspective.Aging &Mental Health,
0(0), 1–8. Retrieved August 24, 2011, from http://www.tandfonline.com/doi/abs/10.1080/13607863.2011.583620.
Moyle, W., Murfield, J., Griffiths, S. & Venturato, L. (2011b). Care staff attitudes and experiences of
working with older people with dementia. Australiasian Journal on Ageing, DOI: 10.1111/j.1741-6612.2010.00470.x.
Nepal, B., Ranmuthugala, G., Brown, L., & Budge,M. (2008).Modelling costs of dementia in Australia:evidence, gaps, and needs. Australian Health Review, 32(3), 479–487.
Nolan, M. R., Davies, S., Brown, J., Keady, J., & Nolan, J. (2004). Beyond person centred-care: a newvision for gerontological nursing. Journal of Clinical Nursing, 13(3a), 45–53.
Nolan, M., Davies, S., Brown, J., Wilkinson, A., Warnes, T., McKee, K., et al. (2008). The role of
education and training in achieving change in care homes: a literature review. Journal of Research inNursing, 13(5), 411–433.
O’Connor, D., Phinney, A., Smith, A., Small, J., Purves, B., Perry, J., Drance, E., et al. (2007).
Personhood in dementia care: Developing a research agenda for broadening the vision. Dementia,6(1), 121–142.
Prior, L. (2003). Using documents in social research. London: Sage Publications Ltd.
Quinlan, E. (2009). The ‘actualities’ of knowledge work: an institutional ethnography of multi-disciplinary primary health care teams. Sociology of Health & Illness, 31(5), 625–641.
Robinson, G. E., & Gallagher, A. (2008). Culture change impacts quality of life for nursing homeresidents. Topics in Clinical Nutrition, 23(2), 120–130.
Smith, D. E. (1988). The everyday world as problematic: A feminist sociology. Toronto, Canada:University of Toronto Press.
Smith, D. E. (2005). Institutional ethnography: a sociology for people (Gender Lens series). Walnut
Creek, CA: AltaMira Press.Townsend, E., Langille, L., & Ripley, D. (2003). Professional tensions in client-centered practice: using
an institutional ethnography to generate understanding and transformation. The American Journal of
Occupational Therapy, 57(1), 17–28.Venturato, L. (2010). Dignity, dining and dialogue: reviewing the literature on quality of life for people
with dementia. International Journal of Older People Nursing, 5(3), 228–234.
Venturato, L., Kellett, U., &Windsor, C. (2007). Nurses’ experiences of practice and political reform inlong-term aged care in Australia: implications for the retention of nursing personnel. Journal ofNursing Management, 15(1), 4–11.
Vollmar, H. C., Butzlaff, M. E., Lefering, R., & Rieger, M. A. (2007). Knowledge translation on
dementia: a cluster randomized trial to compare a blended learning approach with a ‘‘classical’’advanced training in GP quality circles. BMC Health Services Research, 7, 92.
Worden, A., & Challis, D. (2008). Care planning systems in care homes for older people. Quality in
Ageing, 9(2), 28–38.WorldHealth Organisation (2003)TheWorld Health Report 2003: Shaping the Future. Retrieved August
24, 2011, from http://www.who.int/whr/2003/en/whr03_en.pdf.
16 Dementia 0(0)
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from

XML Template (2011) [21.10.2011–2:57pm] [1–17]K:/DEM/DEM 421837.3d (DEM) [PREPRINTER stage]
Lorraine Venturato is a Research Fellow in the School of Nursing and Midwifery and theResearch Centre for Clinical and Community Practice Innovation at Griffith University. Sheholds a joint appointment with RSL Care. Her research focus is on the organizationalelements of service delivery for older people, aged care workforce and models of care, andsystemic influences on dementia care.
WendyMoyle is a Professor and Director of the Research Centre for Clinical and CommunityPractice Innovation at GriffithUniversity. Her research focus has been on finding evidence formanaging agitated behaviours in people with dementia using controlled trials andpsychosocial and complementary and alternative medicine interventions, quality of life forpeople with dementia and their carers and the development of a capabilities model of care.
Andrea Steel holds a Bachelor of Behavioural Science (Psychology) from QueenslandUniversity of Technology completed in 2007. She currently works for RSL Care in theService Development Team working across areas of research, practice development andstrategy. She has worked in the aged care industry for 14 years and has a passionateinterest in positive outcomes for this group. Her areas of interest are dementia, telehealth,health and well-being.
Venturato et al. 17
at Griffith University on February 21, 2013dem.sagepub.comDownloaded from
Related Documents











