Delivery Design Delivery Design “ “ an improvement model of diabetes care” an improvement model of diabetes care” a project funded by the Robert Wood Johnson a project funded by the Robert Wood Johnson Foundation Foundation East Carolina University/Bertie Memorial Hospital East Carolina Health-Bertie All-County Health Services Paul Bray, MA., Skip Cummings, Pharm.D., Jolynn Harrell, RN

Delivery Design “ an improvement model of diabetes care” a project funded by the Robert Wood Johnson Foundation East Carolina University/Bertie Memorial.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Delivery DesignDelivery Design““an improvement model of diabetes care”an improvement model of diabetes care”
a project funded by the Robert Wood a project funded by the Robert Wood Johnson FoundationJohnson Foundation
East Carolina University/Bertie Memorial HospitalEast Carolina Health-Bertie All-County Health Services
Paul Bray, MA., Skip Cummings, Pharm.D., Jolynn Harrell, RN
KeysKeys toto DeliveryDelivery DesignDesign Education with coaching (E-C) is the primary tool used to achieve
patient self-management
E-C is delivered by an advanced skilled non-physician clinical staff
E-C is delivered at the time of the (primary care provider) PCP visit
The physician’s and (Educator/coach) EC form a care team
The physician’s leadership is very important to the team’s success
Nurses and front desk support staff play important and expanded
roles
There are 6 Steps to the delivery design; 4 steps PCP visit
redesigned and 2 steps education-coaching
Step 1: Monthly QI (Quality Step 1: Monthly QI (Quality Improvement) Team MeetingsImprovement) Team Meetings
Team reviews 3-5 evidence-based clinic panel outcome indicators including A1C & BP,
Team initiates corrective PDSA (Plan, Do, Study, Act) cycles
Team reports outcomes quarterly to board of directors, or governing body

Clinical Measures Reviewed in QI Clinical Measures Reviewed in QI MeetingsMeetings
Phase I
NCQA= National CommitteeFor Quality Assurance
Targets: stretch goals for practices to work toward; -benchmark goals = NCQA
Quality Compass
Diabetes
Patient Count N/AHbA1C Management: Poor Control
greater than 9% < 5%Blood Pressure Management :
<130/80 > 70%LDL Cholesterol Management: <100
mg/dl > 70%
Diabetic Eye Exam > 80%
Medical Attention for Nephropathy > 90%
Influenza Vaccination > 75%
Aspirin for DM patients over 40 > 85%
Lipid Test Documentation > 90%
HbA1C Documentation > 90%
Statin for DM patients over 40 > 70%
Tobacco Use Assessment > 80%
Tobacco Cessation Intervention > 80%
Step 2: Nurse schedules Step 2: Nurse schedules all patients through all patients through
standing orders for E-C & standing orders for E-C & LabsLabs
Standing Orders1.E-C with initial Dx of DM2.E-C at minimum every 12 months3.E-C visit asap for A1c >84.A1c q 3 months5.Eye exam report every12 months6.Lipid panel q 12 months7.Shoes off every provider visit
•Nurse scheduling of education based on clinic calendar1.Same day if EC is on-site
2.Schedule EC for same day if follow-up PC visit is within 30 days
3.If follow-up is not within 30 days, schedule a brief PC visit and
EC same day
4.Empowerment of nurse to expedite urgent EC visits (A1c>8.0,
TRG >300, BP> 150/90, BS>200, open wound, or combination)
•Nurse linking EC, PCP & Doctor•Coordinates PCP introduction of EC to patient
•Coordinates PCP brief visit to E-C session
•Coordinates E-C during exam room waiting times
Step 3: Support staff Step 3: Support staff scheduling follow up and scheduling follow up and
trackingtrackingFollow-up appointments scheduled
as directed by PCP or EC1. New diagnosis, 3-4 visits focused on key self-
management objectives
2. Follow-up visit scheduled for key learning objectives (i.e. glucose testing, insulin management and bs goals)
3. New start insulin/medication or changes in insulin/medication dose follow up within 2 weeks
4. Visits follow-up <30 days apart with a1c > 8

•Support Staff ( front desk, etc.) calls and reminds all patients one day before visits1.Support staff calls and re-schedules all no-shows2.EC calls patient after two no-shows
•Educator-coach empowered to re-schedule

Step 4: Team consultations Step 4: Team consultations for most patients for most patients
Hall-way brief case conferencesBrief visit by PCP in educationBrief visit by EC in exam roomsPhysician will ask “what is the clinical
goal & SM goal?”Any team member is encouraged to
schedule case conference for difficult or puzzling patient at monthly QI meeting
Educator-coach empowered to recommend medication-insulin (depending on skill)
Step 5: Focused 1Step 5: Focused 1stst E-C E-C VisitVisit
1. Use short intake summary questionnaire form
2. Chart consulted: confirm diagnosis, medications, labs, A1C, consult progress notes
3. Seek quick understanding of issues & barriers; clarify why a medication may not be working, determine patient’s knowledge base, literacy, length of diabetes, ability to test blood sugars
4. Clarify blood sugar goals, basic nutrition knowledge, basic survival skill knowledge
5. Key inquiry: what did you eat in last 24 hours, how did it affect blood sugars?
6. Check office meter against patient’s meter: Do they have a glucometer and are they competent in its use, are supplies affordable, do they understand how to use results?
Step 5: 1st Visit (con’t)Step 5: 1st Visit (con’t)7. Standard 1st visit self-management goal: Check blood sugars as prescribed, return to next
scheduled DM visit with log and meter; Begin to understand how portions of carbohydrates and
activity impact bs results. Always have return visit in mind. Proceed to
check-out, for scheduling of next appointment --or add E-C visit to next physician appointment.
8. Encourage next visit to be with care-partner
9. At end of first visit: Patient should believe they can have control over their diabetes and they should have some definition of blood glucose – and how numbers impact health
10. Final words to patient ALWAYS, “what is your diabetes goal today?”

Step 5: 1Step 5: 1stst visit (con’t) visit (con’t)11. Seek out physician for 2 minute hall-way
consultation
12. Provide “introduction to diabetes” hand-out, provide score sheet to record bs
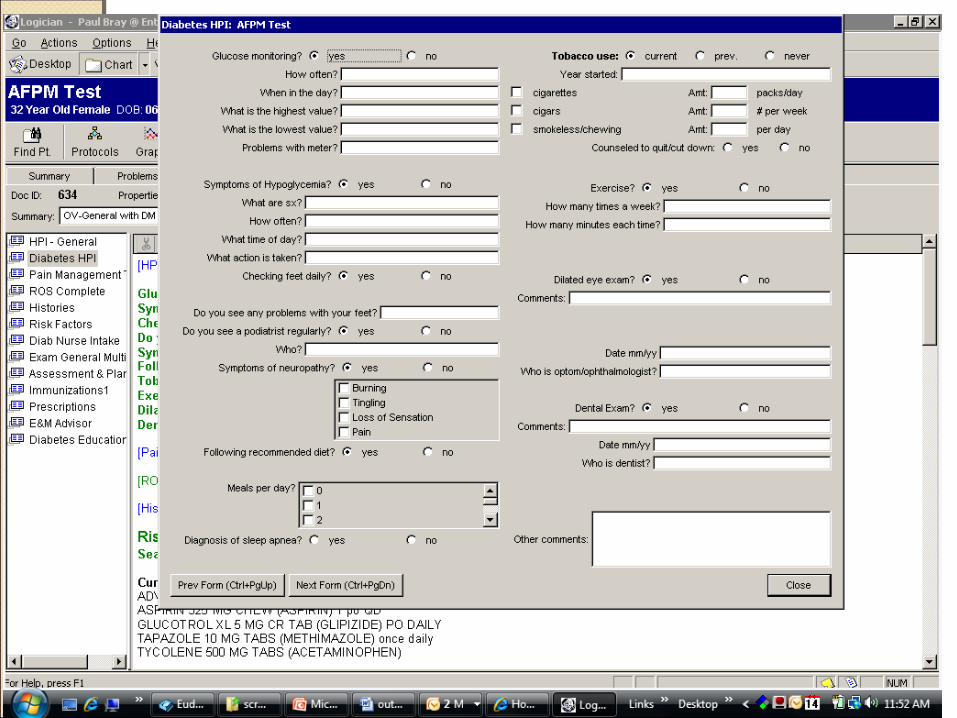
Information gathered in the 1st visit is entered into EMR forms. These forms can then report the progress a patient is making in diabetes management both to the patient and the health care team. The following two screen shot slides are reproductions of the clinic’s EMR diabetes forms (in Centricity EMR).


Step 6: Follow-up 2Step 6: Follow-up 2ndnd to 4 to 4thth to to ongoing visitsongoing visits
At least monthly visit until blood sugars stable
Prioritize key ADA (American Diabetes Association) curriculum issues that are preventing diabetes management
Order of modules – based on intake assessment – most problematic or crucial to least problematic.
Step 6: 2Step 6: 2ndnd visit and on visit and on (con’t)(con’t)Work towards education in each
ADA curriculum module1. Disease of DM, A1C, BS goals, Basic meal planning
2. Nutrition and Carbohydrate Counting
3. Nutrition and Heart Disease
4. Weight loss
5. Exercise
6. Dealing with diabetes, living with life style changes, psychological impact
7. Self management and complications of diabetes
8. Medications and monitoring
9. Problem Solving
Step 6: 2Step 6: 2ndnd visit and on visit and on (con’t)(con’t)
End each session with self-management goal (SMG), begin each session with review of SMG, review of blood sugars, challenges faced in self management.
Implement Motivational Interviewing model to enable self-confidence in ability to make healthy change.
Screen for DepressionProblem solve Eye Exam
Step 6: 2Step 6: 2ndnd visit and on visit and on (con’t)(con’t)
The following PDF files detail the diabetes curriculum used by the EC
http://nc-e-care.com/Teaching_points_Overview_Class.pdf
http://nc-e-care.com/Teaching_points_Intro_class_1-4.pdf
http://nc-e-care.com/Teaching_points_Nutrition_Class.pdf
http://nc-e-care.com/Teaching_points_Nutrition_and_Cholesterol.pdf
http://nc-e-care.com/Teaching_points_Medication_Class.pdf
Related Documents











