Delirium as a Palliative Care Emergency Shirley H. Bush Contents 1 Introduction ....................................................................... 2 2 Epidemiology ...................................................................... 3 3 Clinical Features of Delirium ..................................................... 3 4 Screening for Delirium ............................................................ 4 5 Making a Diagnosis of Delirium ................................................. 5 5.1 Potential Diagnostic Challenges ................................................... 5 6 Risk Factors for Delirium ........................................................ 6 7 Decision-Making in the Management Approach ............................... 6 8 Clinical Assessment ............................................................... 8 8.1 Detailed History .................................................................... 8 8.2 Physical Assessment ................................................................ 8 8.3 Investigations ....................................................................... 8 8.4 Management of Potentially Reversible Delirium Participants ..................... 9 9 Management of Delirium Symptoms in Palliative Care Patients ............. 9 9.1 Nonpharmacological Management ................................................. 9 9.2 Pharmacological Management ..................................................... 12 10 The Delirium Experience and Support .......................................... 14 11 Refractory Delirium at the End of Life .......................................... 15 S. H. Bush (*) Department of Medicine, Division of Palliative Care, University of Ottawa, Ottawa, ON, Canada Bruyère Research Institute, Ottawa, ON, Canada Ottawa Hospital Research Institute, Ottawa, ON, Canada Bruyère Continuing Care, Ottawa, ON, Canada e-mail: [email protected] # Springer Nature Switzerland AG 2019 R. D. MacLeod, L. Block (eds.), Textbook of Palliative Care, https://doi.org/10.1007/978-3-319-31738-0_87-2 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Delirium as a Palliative CareEmergency
Shirley H. Bush
Contents1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2 Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
3 Clinical Features of Delirium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
4 Screening for Delirium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
5 Making a Diagnosis of Delirium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.1 Potential Diagnostic Challenges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
6 Risk Factors for Delirium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
7 Decision-Making in the Management Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
8 Clinical Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88.1 Detailed History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88.2 Physical Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88.3 Investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88.4 Management of Potentially Reversible Delirium Participants . . . . . . . . . . . . . . . . . . . . . 9
9 Management of Delirium Symptoms in Palliative Care Patients . . . . . . . . . . . . . 99.1 Nonpharmacological Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 99.2 Pharmacological Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
10 The Delirium Experience and Support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
11 Refractory Delirium at the End of Life . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
S. H. Bush (*)Department of Medicine, Division of Palliative Care,University of Ottawa, Ottawa, ON, Canada
Bruyère Research Institute, Ottawa, ON, Canada
Ottawa Hospital Research Institute, Ottawa, ON, Canada
Bruyère Continuing Care, Ottawa, ON, Canadae-mail: [email protected]
# Springer Nature Switzerland AG 2019R. D. MacLeod, L. Block (eds.), Textbook of Palliative Care,https://doi.org/10.1007/978-3-319-31738-0_87-2
1

12 Palliative Sedation for Refractory Agitated Delirium at the End of Life . . . . . 15
13 Conclusion and Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
AbstractThis chapter considers delirium in the contextof a palliative care emergency. It reviewsscreening for delirium, tools to confirm theclinical diagnosis of delirium, and diagnosticchallenges. It describes both the non-pharmacological and pharmacological man-agement of delirium. It also reviews thedelirium experience and associated distress. Itconcludes with a brief discussion of the role ofpalliative sedation for refractory delirium at theend of life.
1 Introduction
Delirium is a complex and often distressingneurocognitive syndrome which commonly occursin patients with advanced life-threatening illness.Delirium is an index of a serious change reflectingmajor underlying pathology and homeostaticdestabilization, such as acute worsening of anexisting or acute emergence of a new medical con-dition, medication, toxic substance, etc. (AmericanPsychiatric Association [APA] 2000).
Delirium is often considered a medical orclinical emergency. Its sudden onset requires theclinical healthcare team to take urgent action inorder to not only minimize many potentially seri-ous negative outcomes including increased risk offalls and risk of harm to patients themselves, theirfamilies, and staff due to aggressive behavior,but also because untreated delirium is life-threatening. There is a need to identify andpromptly treat reversible delirium precipitants ifconsistent with a patient’s goals of care.
The online English Oxford dictionary definesmedical emergency as “a serious and unexpectedsituation involving illness or injury and requiringimmediate action” (Oxford University Press2017). However, delirium can often be antici-pated as it is known that certain people are at
higher risk of developing delirium. This includespeople with pre-existing dementia or advancedillness such as cancer, a past history of a previousdelirium episode, and who are over the age of65 years. Patients with a pre-existing “vulnerable”brain only require a comparatively small precipi-tating insult to develop full syndromal delirium(Inouye et al. 2014a).
Both patients and families can becomeextremely distressed during an episode of delir-ium, requiring urgent intervention, support, andeducation. Patients may experience psychologicaldistress due to vivid perceptual and delusionaldisturbances (Partridge et al. 2013). Familiesmay continue to have ongoing distress in theirbereavement. Delirium challenges the clinicalassessment of other symptoms, and often leadsto patients being unable to participate indecision-making and goals of care discussion,thus potentially adding to family burden. A delir-ious patient can be particularly challenging tomanage in the home setting, even with the avail-ability of an “emergency kit” of medications.Family members are often exhausted due tosleep deprivation if the delirious patient is notsleeping at night. While extra homecare supportwill often be required, potential referral for urgentinpatient care may be needed.
The aim of this chapter is to highlight theimportance of considering delirium as a clinicalemergency, requiring planning for its occurrence,and immediate action at its onset to reduce mor-bidity and mortality. It outlines the impact andpotentially ominous outcomes of this very com-mon neurocognitive syndrome. An overview ofdelirium screening and diagnostic tools to assist inthe clinical diagnosis of delirium is presented,as well as diagnostic challenges. A patient- andfamily-centered approach to delirium managementwhich incorporates the patient’s goals of care,while avoiding an inappropriately pessimisticapproach to investigation and management, is
2 S. H. Bush

discussed. Nonpharmacological strategies used inthe prevention and management of delirium areemphasized. Pharmacological management forsymptom relief is reviewed in the context ofrecent research. Finally, the chapter discusses theimportance of providing emotional and practicalsupport to patients experiencing delirium andtheir families, including when a patient requirespalliative sedation for refractory delirium at theend of life. The interested reader is also referred tochapter ▶ “Delirium and Terminal Agitation”which provides a comprehensive description ofdelirium in palliative care patients, includingpathophysiology.
2 Epidemiology
Delirium affects 20% of patients admitted to acutegeneral medical care settings (Pendlebury et al.2015), with delirium incidence increasing up toalmost 29% in older patients (� 65 years old)(Bellelli et al. 2016), 35% if >80 years (Ryanet al. 2013), and 56% in patients with dementia(Inouye et al. 2014a). Up to 20% of older personspresenting to the emergency department havedelirium (Inouye et al. 2014a). Delirium is alsocommon in palliative care patients. The preva-lence of delirium on admission to a specialistpalliative care inpatient setting ranges from13.3–42.3% and increases to 88% in the lasthours to weeks of life (Hosie et al. 2013). Mostsignificantly for palliative care patients, delirium
is a poor prognostic feature with an associationwith increase in mortality (Caraceni et al. 2000;Hui et al. 2015). In fact, delirium has even beencalled “a harbinger of death” in terminally illpatients, with death occurring within days toweeks of its onset (Breitbart and Alici 2008).
Delirium also causes an increase in patientmorbidity, with a heightened risk of falls, longerhospital stays and associated increase in healthcare costs, and significant patient and family dis-tress (see Fig. 1). In the increasingly recognizedsyndrome of “persistent delirium,” deliriumsymptoms frequently continue and recoveryrates are often poor in the elderly (Dasgupta andHillier 2010). Cognitive decline after an episodeof delirium is common. Delirium appears toworsen pre-existing dementia as well as increas-ing the risk of new-onset dementia (Fong et al.2015). Functional decline and permanent institu-tionalization are also common outcomes afterdelirium.
3 Clinical Features of Delirium
The essential clinical feature of a delirium syn-drome is impaired attention, with a change havingoccurred in a patient’s baseline attention andawareness over a short period of time (APA2013). Delirium usually fluctuates in severitywithin a 24-h period. Patients also develop distur-bances in cognition, including perceptual distur-bances such as misinterpretations, illusions, and
Fig. 1 Impact and potential outcomes of delirium
Delirium as a Palliative Care Emergency 3
hallucinations. Other clinical features which mayoccur (but are not required features for a deliriumdiagnosis) include sleep-wake cycle disturbance,emotional lability, disorganized thinking, incoher-ent speech, and altered psychomotor activity(Breitbart and Alici 2012). Although notperformed routinely, generalized slowing on anelectroencephalogram (EEG) is a characteristicfeature of delirium (Engel and Romano 1959).
Delirium is categorized into three subtypesaccording to the level of psychomotor activity:hyperactive, hypoactive, and mixed (with alter-nating features of both hyperactive and hypo-active subtypes). In a study of 100 palliative careunit inpatients with delirium whose motor activitywas assessed with the Delirium Motor SubtypeScale (DMSS), almost a quarter of assessmentswere categorized as “no-subtype,” as they did notmeet criteria for the other defined subtypes(Meagher et al. 2012). The hypoactive andmixed subtypes are the most common in palliativecare populations. Motor agitation is a feature ofthe hyperactive subtype and purposeless repeti-tive movements (such as plucking at bed sheetsor pulling off clothes) may be observed. A patientwith hyperactive delirium may be deemed to be inneed of more urgent attention by the healthcareteam due to visible motor agitation, but in factpatients with the hypoactive delirium subtypehave a poorer overall prognosis with increasedmortality (Kim et al. 2015).
After a positive result for possible delirium fromroutine screening or the onset of clinical signs, thediagnosis needs to be formally confirmed. Defineddiagnostic criteria for delirium are codified in theDiagnostic and Statistical Manual of Mental Dis-orders (DSM-5) (APA 2013), and in the Interna-tional Classification of Diseases (ICD-10) (WorldHealth Organization 1992). The earlier that delir-ium is recognized, the sooner proactive manage-ment strategies can be put in place if previouslyimplemented nonpharmacological strategies didnot prevent its onset (see also chapter▶ “Delirium”).
4 Screening for Delirium
Back in 1959, Engel and Romano declared that:“Most delirious patients are considered eitherdull, stupid, ignorant, or uncooperative. It isonly when their behaviour and content of thoughtare grossly deviant that an abnormal mental stateis recognized, although [ids] not always correctlyidentified as delirium” (Engel and Romano 1959).Unfortunately, delirium remains under-recognizedand is repeatedly missed or misdiagnosed (Clegget al. 2011; Inouye et al. 2014a; de la Cruz et al.2015a). Routine screening for delirium by allmembers of the health care team may improveits detection.
The Confusion Assessment Method (CAM) isa widely used instrument (Inouye et al. 1990). Therating of the CAM requires the co-administrationof a brief cognitive assessment tool. The CAMhasbeen validated in palliative care patients and ratersrequire a moderate level of training to ensurereliability. Two nursing observational deliriumscreening tools rated at the end of each shift arethe Nursing Delirium Screening Scale (Nu-DESC) and Delirium Observational Screening(DOS) Scale (Gaudreau et al. 2005; Schuurmanset al. 2003). The recently developed brief 4ATest(4AT) (available at: www.the4at.com) is designedto be used by a healthcare professional when firstmeeting a patient, or when delirium is suspected,as opposed to daily monitoring. It assesses forboth cognitive impairment and delirium and hasbeen validated in older hospitalized patients(Bellelli et al. 2014).
The prodromal features of delirium may pro-vide an early warning to the healthcare team of theimpending onset of a delirium episode. Theseearly features include disruption of the sleep-wake cycle with reduced sleep at night, increasedsomnolence in the daytime, and also irritability,anxiety, and motor restlessness (Kerr et al. 2013).These features may occur before cognitivechanges or perceptual disturbances such as hallu-cinations are observed. As part of the circle ofcare, the patient’s family is also uniquely placedto identify the occurrence of subtle changes in apatient’s behavior and/or cognition and should beencouraged to report this immediately to any
4 S. H. Bush

member of the healthcare team. The Single Ques-tion in Delirium (SQiD) asks a family member orfriend “Do you think [name of patient] has beenmore confused lately?” (Sands et al. 2010).
5 Making a Diagnosis of Delirium
Delirium is listed as a “neurocognitive disorder”in the Diagnostic and Statistical Manual of Men-tal Disorders (DSM-5) which lists formal diag-nostic criteria for delirium (APA 2013). It is acomplex syndrome with varying clinical featuresand deleterious effects. As per the DSM-5 criteria,an essential feature for the diagnosis of delirium isa disturbance in attention and awareness, accom-panied by a change in baseline cognition whichcannot be better explained by a preexisting,established, or evolving neurocognitive disorder.Delirium usually develops over hours to days, andits severity tends to fluctuate within a 24-h period.Patients may also be classified as having sub-syndromal delirium (SSD) if they meet some butnot all the criteria for full syndromal delirium(Leonard et al. 2014).
Although the CAM was designed as a screen-ing tool, in clinical practice the CAM diagnosticalgorithm is often utilized as a “diagnostic” tool.The recent 3D–CAM, which operationalizes theCAM using a 3-min assessment, was validated in201 general medicine inpatients (� 75 years) in asingle center (Marcantonio et al. 2014). Morelengthy delirium-specific assessment toolsinclude the Delirium Rating Scale-revised-98(DRS-R-98) (Trzepacz et al. 2001) and MemorialDelirium Assessment Scale (MDAS) (Breitbartet al. 1997).
5.1 Potential Diagnostic Challenges
Delirium impairs patient communication. It isoften challenging to diagnose delirium in a patientwith reduced communication or a reduced level ofconsciousness, due to delirium itself or the dyingphase as a result of disease progression,employing many of the currently available delir-ium assessment tools. Differentiating dementia,
depression, and hypoactive delirium can be prob-lematic for healthcare providers. Dementia, wherea change in cognition occurs with little or noclouding of consciousness, has an insidiousonset over months. Notably, patients with demen-tia with Lewy bodies have fluctuating cognitiveimpairment with variations in attention and alert-ness, complex visual hallucinations, and parkin-sonism. Delusions may also be a feature (Pealingand Iliffe 2011). Delirium is also commonlysuperimposed on dementia, making clinical eval-uation more problematic compounded by a cur-rent lack of suitable assessment tools (Morandiet al. 2017). Hypoactive delirium may present asdepression or fatigue.
Hyperactive delirium may be misdiagnosed asanxiety, akathisia, or mania. With akathisia, thesubjective symptoms of feeling nervous or restlessand the observed movements of the body may bemisinterpreted as increasing agitation due to delir-ium, hence the necessity that health care providersshould monitor for potential medication-inducedakathisia and other adverse extrapyramidal sideeffects (EPS) of antipsychotic medications admin-istered to a distressed delirious patient. Agitationis not specific to delirium, so possible other causesfor a patient’s agitation should be considered.Urinary retention, severe constipation, or fecalimpaction may aggravate patient agitation, espe-cially in the elderly. This is often overlooked andmay require urgent intervention, e.g., insertion ofa urinary catheter, or rectal suppositories/micro-enema. Uncontrolled pain may also cause patientagitation. Valid, reliable tools to assess pain inolder cancer patients with delirium are needed(Gagliese et al. 2016).
Agitation may also be the presenting feature oftwo distinct syndromes, neuroleptic (antipsy-chotic) malignant syndrome (NMS) and serotoninsyndrome, where it is a more typical clinical fea-ture in the latter (Buckley et al. 2014; Katus andFrucht 2016). Timely recognition of these poten-tially life-threatening syndromes is critical asurgent management is required. NMS is an infre-quent, idiosyncratic, and potentially fatal syn-drome which develops over days to weeks and isprecipitated by dopamine antagonists. Some fea-tures of NMS are similar to serotonin syndrome
Delirium as a Palliative Care Emergency 5

which is precipitated by serotonin agonists with amore rapid onset of less than 24 h (see Table 1).
In palliative care settings, any sudden changein patient behavior, such as anxiety and psycho-logical distress, should be used as a trigger forpatient reevaluation to exclude delirium. A delir-ious patient may show signs of moaning,groaning, and facial grimacing as a result of delir-ium, not pain. In addition, a delirious patient mayhave an increased expression of pain as a result ofdisinhibition. If these signs in a delirious patientare misinterpreted as an increase in pain produc-tion due to activation of nociceptors, the resultingadministration of extra unnecessary doses of opi-oids may potentially increase the deliriumseverity.
6 Risk Factors for Delirium
Delirium is usually multifactorial and risk factorscan be broadly divided into predisposing (baselinevulnerability) and acute precipitating factors witheach delirium episode having a range of 1–6superimposed precipitants (median 3) (Lawloret al. 2000). The development of delirium arisesfrom the interplay of these factors: patients with apre-existing “vulnerable” or “fragile” brain need asmaller noxious precipitating insult in order totrigger full syndromal delirium, as compared tothose with a “healthy” brain (Inouye et al. 2014a).(See chapter ▶ “Delirium”, Fig. 1: “Model of thecumulative effects of predisposing and precipitat-ing factors on development of delirium”.)
The most common predisposing factors fordelirium are advanced age (>70 years) and pre-existing dementia or cognitive impairment.
Others include: history of delirium, depressionor alcohol abuse, reduced mobility, visual andauditory impairment, fracture or trauma, malnu-trition, multiple co-morbidities, and advancedlife-threatening illness (Laurila et al. 2008; Inouyeet al. 2014a). Studies in palliative care patientshave reported the elucidation of risk factors inaround 50% of delirium episodes, with rates ofup to 90% also reported (Lawlor et al. 2000;Morita et al. 2001). Multiple causes for a deliriumepisode frequently occur at the same time (forexample, opioid-induced neurotoxicity, dehydra-tion, and hypercalcemia), so a detailed clinicalassessment is fundamental, provided it is in keep-ing with the established goals of care.
The identification of precipitating risk factorsis dependent on the extent of possible laboratoryand radiological investigations which in turn isinfluenced by a patient’s location, as well asgoals of care. The precipitating factors identifiedin observational studies in palliative carepopulations depend on the clinical setting andcase mix with a few consistently identified riskfactors, i.e., infection, organ failure, psychoactivemedication, electrolyte abnormalities, and acuteillness.
Figure 2 shows common causes of deliriumand Table 2 shows etiologies that are less commonor potentially missed by the healthcare team.
7 Decision-Making in theManagement Approach
For palliative care patients, the management ofdelirium should be guided by the agreed goals ofcare. Goals of care can be defined as “the intended
Table 1 Comparing clinical features of neuroleptic malignant syndrome (NMS) and serotonin syndrome (Buckley et al.2014; Katus and Frucht 2016)
Neuroleptic (antipsychotic) malignant syndrome Serotonin syndrome
Precipitated by dopamine antagonistsClinical features:Severe rigidityHyperthermiaAltered mental statusAutonomic dysfunction
Develops over days to weeks, and includeshyporeflexia
Precipitated by serotonin agonistsClassically a triad of:(i) Altered mental status, e.g., confusion, agitation(ii) Neuromuscular excitation, e.g., clonus, rigidity,
hyperreflexia(iii) Autonomic excitation, e.g., tachycardia, hyperthermia
Rapid in onset, <24 h
6 S. H. Bush

purposes of healthcare interventions and supportas recognized by both a patient or substitutedecision-maker and the healthcare team” (Winnipeg
Regional Health Authority 2011). Discussinggoals of care requires clear and sensitive commu-nication with the substitute decision-maker
Fig. 2 Common causes of delirium
Table 2 Potentially missed and less common etiologies of delirium
Etiology
HypercalcemiaReported calcium level within normal range, but hypoalbuminemiaAbout 40% of the total serum calcium is bound to plasma proteins, mainly albumin“Total” calcium is reported by laboratories, and a “correction” is needed for the albumin levelMeasure ionized calcium if specific value needed
HyperglycemiaNew finding in person with no preexisting history of diabetes mellitusMonitor glucose level of patients on high dose corticosteroids
Hypoglycemia
Hypoxia
Hypercapnia
Medication or substance withdrawal
Post-ictal phase
Nonconvulsive status epilepticus
Cerebrovascular accident (CVA)
Reversible posterior leukoencephalopathy syndrome (RPLS)
Paraneoplastic syndromes, e.g., paraneoplastic encephalomyelitis
Hematological, e.g., anemia, disseminated intravascular coagulation
Cytotoxic chemotherapy
Acute cerebral edema after brain irradiation
Cognitive deficits/impairment after radiation treatment/chemotherapy?
Delirium as a Palliative Care Emergency 7

(which is usually a family member) as the deliri-ous patient usually lacks decisional capacity, aswell as an individualized approach. There is a riskof being unduly fatalistic by assuming that a pal-liative care patient has an irreversible delirium andsubsequently failing not to investigate clinically,thereby missing potentially reversible precipi-tants. In such cases, death becomes a self-fulfilling prophecy and the opportunity for aperiod of meaningful communication between apatient and their family is lost.
It is advantageous to clarify what the patient’sillness trajectory and functional status was likebefore the onset of delirium, to help confirmwhether the patient has had a sudden precipitouschange in condition, or if their condition has beensteadily declining and they are in actual factapproaching the dying phase. Discussions shouldinclude the probable or suspected delirium pre-cipitants, the potential for reversal or likelihood ofnonreversal, in conjunction with ascertaining thepatient’s prior expressed goals of care and theirpossible desire to proceed or not proceed withfurther investigations and treatment. The burdenand possible risk of inappropriate investigationand treatment should be taken into account. Theconclusion of an informed decision-making pro-cess should reach an agreed management plan. Assuch, a timed trial of antibiotics for infection maybe considered, for example. If the managementplan does not aim for both delirium reversal (byway of investigation and treatment of precipitants)and symptom treatment, then symptom-directedtreatment (nonpharmacological and potentiallypharmacological) solely to control delirium symp-toms should continue with the aim of ensuringcomfort.
8 Clinical Assessment
Even with a detailed clinical assessment, deliriumetiology in palliative care patients may remainunclear in approximately 50% of episodes.
8.1 Detailed History
The patient may be aware of feeling confused andreport perceptual disturbances (visual or tactilehallucinations and illusions), or delusions. Aspart of a comprehensive past medical historyassessment, an alcohol and substance abuse his-tory should be obtained to identify delirium asso-ciated with withdrawal. A collateral history maybe required from a family member or friend toconfirm the fluctuating nature and recent onset ofdelirium symptoms, as well as baseline mentalstatus. Medication lists should be reviewed, notonly for new medications, but also for long-stand-ing medications and recent increases in doses.Opioid-induced neurotoxicity (OIN) is a syn-drome of neuropsychiatric side effects that mayoccur with opioid therapy, especially if the opioidis administered in a large or rapidly increasingdose. OIN is exacerbated by dehydration.
8.2 Physical Assessment
In addition to a formal cognitive assessment andevaluation of attention, a physical examinationshould be conducted to look for potential under-lying causes of delirium, such as infection, dehy-dration, and OIN. In addition to delirium andcognitive impairment, the clinical features ofOIN are severe sedation, hallucinations, myoclo-nus, seizures, allodynia, and hyperalgesia. Apatient may exhibit increased or decreased psy-chomotor activity. A further neurological exami-nation of the patient may reveal abnormalmovements such as asterixis, or cranial nervedeficits. In diffuse encephalopathies, signs ofbifrontal dysfunction may be elicited, e.g.,palmomental, snout, and grasp reflexes.
8.3 Investigations
It is less appropriate to extensively investigate forunderlying causes of delirium in patients in thelast hours of life. Laboratory investigations shouldbe aimed at identifying potentially reversiblecauses and may include complete blood count,
8 S. H. Bush

sodium, potassium, urea, creatinine, calcium,albumin, magnesium, random blood glucose, bil-irubin, liver enzymes, ammonia levels (if severeliver impairment suspected), urinalysis, and urineculture. If suspected, tests for vitamin deficienciessuch as Vitamin B1 (thiamine), B12 (cobalamin),and folate may be indicated. The patient’s level ofoxygen saturation should be assessed. A chest X-ray may confirm the presence of pneumonia. If inkeeping with a patient’s goals of care, radiologicalcerebral imaging may be appropriate, such as acomputed tomography (CT) or magnetic reso-nance imaging (MRI) scan of the brain.
8.4 Management of PotentiallyReversible DeliriumParticipants
Approximately, 50% of delirium episodes inadvanced cancer patients are reversible (Lawloret al. 2000). The decision to investigate for poten-tially reversible precipitants will depend on apatient’s goals of care and assessment of burdenof investigation and treatment, in addition to thetype of care setting and availability of resourceslocally.
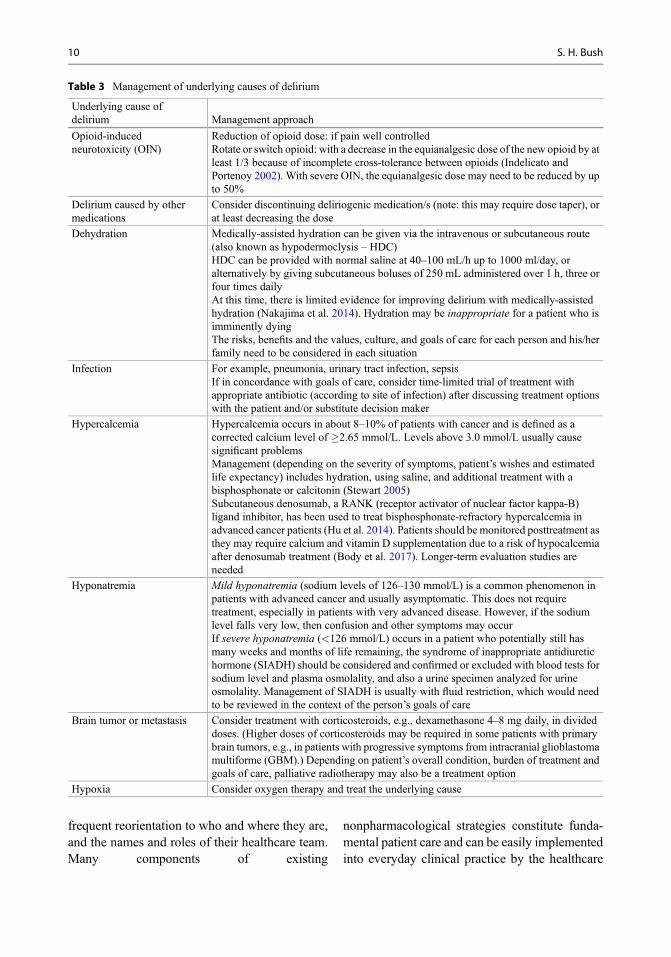
Delirium in palliative care patients is signifi-cantly more reversible if the precipitating factor isopioids and other psychoactive drugs, infection,and hypercalcemia (Lawlor et al. 2000; Morita etal. 2001). See Table 3 for the management ofunderlying causes of delirium. As part of good“deprescribing” practice to reduce polypharmacy,all patients’ medication lists should undergo asystematic review, with a drug profile review bya pharmacist if possible, to reduce or discontinuemedications, especially psychoactive drugs. Opi-oid rotation and discontinuation of other medica-tions results in resolution of approximately75–80% of episodes of drug-induced delirium.Reversal of delirium takes 2–7 days to occur.Conversely, delirium is less likely to improve inpatients with an underlying dementia (Inouye etal. 2006), or if the delirium is related to hypoxic orglobal metabolic encephalopathy, or disseminatedintravascular coagulation (Lawlor et al. 2000;Morita et al. 2001).
As delirium is often less reversible at the end oflife, the challenge is discerning when attempts toreverse it are appropriate. Healthcare professionalsare often inaccurate in their predictions oflife expectancy, either under- or over-estimatingthe time left. Thus, it is important to try andidentify if the person is imminently dying inorder to establish the appropriateness of treatingthe precipitating causes of the delirium episode.However, diagnosing when a patient is enteringthe terminal phase can be especially challengingwhen viewed through the lens of fluctuating delir-ium signs and symptoms. Further developmentand research on predictive models of deliriumreversibility in palliative care would assist in clin-ical decision-making.
9 Management of DeliriumSymptoms in Palliative CarePatients
Delirium should be viewed as an acute clinicalemergency requiring urgent evaluation by theinterprofessional health care team. The serious-ness and urgency of management to minimize itsadverse effects is perhaps more pronounced if it isconsidered as a type of “acute brain dysfunction”(Morandi et al. 2008). The interprofessional teamshould work collaboratively to proactively man-age patients with delirium, reduce its harmfuleffects, and support family members. As part ofthis endeavor, clear and consistent communica-tion from the healthcare team with patients, fam-ilies, and other team members is paramount.Consultation with Psychiatry or Psychogeriatricsis recommended for cases that are challenging tomanage.
9.1 NonpharmacologicalManagement
Nonpharmacological strategies play a key role inthe management of delirium, potentially pre-venting about 30% of delirium episodes in acutecare settings (Siddiqi et al. 2016) (see Table 4).Delirious patients should be supported by
Delirium as a Palliative Care Emergency 9
frequent reorientation to who and where they are,and the names and roles of their healthcare team.Many components of existing
nonpharmacological strategies constitute funda-mental patient care and can be easily implementedinto everyday clinical practice by the healthcare
Table 3 Management of underlying causes of delirium
Underlying cause ofdelirium Management approach
Opioid-inducedneurotoxicity (OIN)
Reduction of opioid dose: if pain well controlledRotate or switch opioid: with a decrease in the equianalgesic dose of the new opioid by atleast 1/3 because of incomplete cross-tolerance between opioids (Indelicato andPortenoy 2002). With severe OIN, the equianalgesic dose may need to be reduced by upto 50%
Delirium caused by othermedications
Consider discontinuing deliriogenic medication/s (note: this may require dose taper), orat least decreasing the dose
Dehydration Medically-assisted hydration can be given via the intravenous or subcutaneous route(also known as hypodermoclysis – HDC)HDC can be provided with normal saline at 40–100 mL/h up to 1000 ml/day, oralternatively by giving subcutaneous boluses of 250 mL administered over 1 h, three orfour times dailyAt this time, there is limited evidence for improving delirium with medically-assistedhydration (Nakajima et al. 2014). Hydration may be inappropriate for a patient who isimminently dyingThe risks, benefits and the values, culture, and goals of care for each person and his/herfamily need to be considered in each situation
Infection For example, pneumonia, urinary tract infection, sepsisIf in concordance with goals of care, consider time-limited trial of treatment withappropriate antibiotic (according to site of infection) after discussing treatment optionswith the patient and/or substitute decision maker
Hypercalcemia Hypercalcemia occurs in about 8–10% of patients with cancer and is defined as acorrected calcium level of �2.65 mmol/L. Levels above 3.0 mmol/L usually causesignificant problemsManagement (depending on the severity of symptoms, patient’s wishes and estimatedlife expectancy) includes hydration, using saline, and additional treatment with abisphosphonate or calcitonin (Stewart 2005)Subcutaneous denosumab, a RANK (receptor activator of nuclear factor kappa-Β)ligand inhibitor, has been used to treat bisphosphonate-refractory hypercalcemia inadvanced cancer patients (Hu et al. 2014). Patients should be monitored posttreatment asthey may require calcium and vitamin D supplementation due to a risk of hypocalcemiaafter denosumab treatment (Body et al. 2017). Longer-term evaluation studies areneeded
Hyponatremia Mild hyponatremia (sodium levels of 126–130 mmol/L) is a common phenomenon inpatients with advanced cancer and usually asymptomatic. This does not requiretreatment, especially in patients with very advanced disease. However, if the sodiumlevel falls very low, then confusion and other symptoms may occurIf severe hyponatremia (<126 mmol/L) occurs in a patient who potentially still hasmany weeks and months of life remaining, the syndrome of inappropriate antidiuretichormone (SIADH) should be considered and confirmed or excluded with blood tests forsodium level and plasma osmolality, and also a urine specimen analyzed for urineosmolality. Management of SIADH is usually with fluid restriction, which would needto be reviewed in the context of the person’s goals of care
Brain tumor or metastasis Consider treatment with corticosteroids, e.g., dexamethasone 4–8 mg daily, in divideddoses. (Higher doses of corticosteroids may be required in some patients with primarybrain tumors, e.g., in patients with progressive symptoms from intracranial glioblastomamultiforme (GBM).) Depending on patient’s overall condition, burden of treatment andgoals of care, palliative radiotherapy may also be a treatment option
Hypoxia Consider oxygen therapy and treat the underlying cause
10 S. H. Bush

Table 4 Nonpharmacological strategies used in the management of delirium (Zimberg and Berenson 1990; CanadianCoalition for Seniors’ Mental Health 2010; NICE 2010; Breitbart and Alici 2012; Inouye et al. 2014b)
Delirium management strategies Details
Orientation: Environment
Devices, e.g., visible clock, calendar, orientationboard with name/date/location of setting
Simplify and organize patient’s environment (call bell, water,telephone, and other essential items within sight and reach)
Familiar objects from home, photographs inpatients rooms
Familiar staff (continuity of care)
Avoid frequent room changes Single room if possible
Orientation: Verbal
Reminders of time, day, place, who they are, whoyou are
Identify self every time, e.g., “I’m your nurse” – visible namebadge
Family/close friends may be able to assist Instruct family to interact in a simple, clear, and concise mannerwith patient
Communication:
Face-to-face with patientMaintain a calm and supportive approachEvaluate need for language interpreters
Communication should be clear, slow-paced, short, simple, andrepeated as necessaryPresent one task or stimulus at a timeIf delusional beliefs, use distraction to shift attention to
another topicExplain each clinical intervention prior to instituting care oradministering medication: avoid rapid movements or touching/grabbing that might be misinterpreted as aggressive
Ensure visual/hearing aids are accessible andused, and dentures where needed
Exclude and resolve impacted wax
Sleep Hygiene:
Facilitate a normal sleep-wake pattern For example, relaxation music at bedtime, warm noncaffeinateddrinks, familiar sleepwear, minimize disruptions through thenightEncourage exposure to bright natural light during the dayDiscourage napping during day, where possible
Environment: Avoid sensory deprivation
Ensure appropriate lighting For example, windowless room, excessive darknessDay-time: Shades/curtains open as much as possible during dayhoursNight-time: Utilize night light
Provide eyeglasses, magnifying lenses, hearingaids
Environment: Avoid sensory overload
Avoid excessive noise For example, excess noise and activityImplement unit-widenoise reduction strategies, especially at night
Avoid patient over-stimulation (by staff andfamily)
Educate family regarding use of simple explanations andinteractions with patient
Mobility: Mobilize as patient’s energy and performance status allowsIf unable to walk, encourage active range-of-motion exercises
as toleratedSit out of bed for meals whenever possibleMinimize use of immobilizing urinary catheters, intravenouslines
Patient/staff safety:Restraint-free care as standard of care
Remove potentially harmful objectsImplement a fall prevention protocolDesignated sitter may be requiredUse of physical restraints should be avoided
(continued)
Delirium as a Palliative Care Emergency 11

team, as well as family members with the supportof the team. While evidence-based multi-component nonpharmacological approacheshave been shown to be effective in reducing delir-ium incidence and preventing falls in older per-sons �65 years (Hshieh et al. 2015), the efficacyof these approaches in palliative care populationsacross the illness trajectory is not known at thistime (Gagnon et al. 2012).
It is important to be aware that an agitatedpatient with delirium is probably extremelyscared. They may be experiencing frighteningdelusional beliefs, such as that the health careteam is trying to harm them. Patients who haverecovered from delirium commonly report thatthey feel they are not being listened to or under-stood, in addition to not being able to understandwhat staff are wanting (Partridge et al. 2013;Lawlor and Bush 2015). The healthcare teamshould communicate to delirious patients face toface with simple, concise, and clear sentences,using a calm voice and reassuring approach at alltimes. A delirious patient may misinterpret areassuring touch from a family or team memberas an act of aggression, so avoid using touch as astrategy to redirect. If delusional beliefs occur, useverbal distraction to shift the attention of a delir-ious patient to another topic. Rapid movementsshould be avoided at all times. Delirious patientsare also hypersensitive to noise. In inpatient set-tings, unit-wide noise reduction strategies shouldbe implemented (Darbyshire and Young 2013).
9.2 Pharmacological Management
(See also chapter ▶ “Delirium”)
The Role for AntipsychoticsThe “off-license” use of antipsychotics to treatdelirium symptoms in palliative care patients hasbeen a mainstay of clinical practice despite limitedclinical evidence. Haloperidol has been the “prac-tice standard” for many years. As one of theputative pathophysiological mechanisms fordelirium development, the “cholinergic hypothe-sis” (with a deficit of acetylcholine and excess ofdopamine) supports the dominant role of haloper-idol as a potent dopamine-receptor antagonist indelirium management.
Back in 1996, Breitbart et al. reported a ran-domized, double-blind comparison trial in 30adult AIDS patients (Breitbart et al. 1996).Patients who received low-dose haloperidol orchlorpromazine were reported to have animprovement in delirium symptoms as measuredon the Delirium Rating Scale. Over the years,published literature has supported the use of anti-psychotics in delirium management (Casarett andInouye 2001; Michaud et al. 2007; Leentjens et al.2012; Breitbart and Alici 2012). The NationalInstitute for Health and Clinical Excellence(NICE) Clinical Guideline made the recommen-dation: “if a person with delirium is distressed orconsidered a risk to themselves orothers. . .consider giving short-term haloperidolor olanzapine” (NICE 2010). It should be noted
Table 4 (continued)
Delirium management strategies Details
General:
Monitor hydration and nutrition Encourage patient to drink, if able to swallow safelyConsider subcutaneous or intravenous hydration
Assist patient at mealtimesUse patient’s dentures, ensure diet consistency appropriate to
patient’s swallowing ability
Monitor bladder and bowel function Assess for urinary retention, constipation and fecal impactionImplement interventions as neededAvoid unnecessary catheterization
Assess and monitor pain Ensure analgesia is adequate
Consider referral to complementary services toreduce anxiety
For example, music therapy
12 S. H. Bush

that this comprehensive guideline excluded “peo-ple receiving end-of-life care.” In 2012, aCochrane review found insufficient evidence fordrug therapy for delirium management in termi-nally ill adult patients (Candy et al. 2012).Increasingly, recent systematic reviews have dem-onstrated a lack of evidence for antipsychoticefficacy, in addition to concerns regarding theirharmful effects, especially in patients with pre-existing dementia (Flaherty et al. 2011; Inouye etal. 2014b; Maust et al. 2015; Neufeld et al. 2016).
An Australian multisite, double-blind, parallel-arm, dose-titrated randomized clinical trial of oralrisperidone, haloperidol, or placebo solution overa 72-h period in adult inpatients with confirmeddelirium and receiving hospice or palliative carehas been recently published (Agar et al. 2017).The dosing schedule for antipsychotics (i.e., ris-peridone or haloperidol) was age-adjusted. In thetwo antipsychotic arms, participants �65 yearsreceived 0.5 mg as a loading dose, followed by0.5 mg orally every 12 h. The dose of antipsy-chotic was titrated by 0.25 mg on day 1, then by0.5 mg up to a maximum of 4 mg/day. Participants>65 years received half the loading, initial andmaximum doses of antipsychotic. All participantscould receive “rescue” midazolam in a dose of2.5 mg subcutaneously every 2 h as needed forsevere distress or safety. (The dose of midazolamwas not age-adjusted.) Of the 247 participantsincluded in the intention-to-treat (ITT) analysis,65.6% were male with a mean age of 74.9 years,and the majority had cancer (88.3%). The baselineAustralia-modified Karnofsky performance status(AKPS) ranged from 30% to 50%. Participantshad mild to moderate delirium, as evidenced bymedian baseline Memorial Delirium AssessmentScale (MDAS) scores ranging from 13.7 to 15.1.For this study, delirium precipitants were alsotreated “where clinically indicated” and all partic-ipants received nonpharmacological approachesas part of delirium care. For the purposes of thisstudy, three items on the Nu-DESC tool (assessinginappropriate behavior, inappropriate communi-cation, and illusions and hallucinations) werecombined to produce a delirium symptom score.In the ITT analysis, participants in the risperidoneand haloperidol arms had significantly higher
delirium symptom scores (p = 0.02 andp = 0.009, respectively) and received more “res-cue”midazolam, as compared to the placebo arm.Median survival was 26 days in the placebo arm,17 days in the risperidone arm, and 16 days in thehaloperidol arm. From a post hoc analysis, theauthors stated that participants “receiving an anti-psychotic drug were approximately 1.5 timesmore likely to die.” At the present time, it is notclear how to integrate the research findings fromthe study by Agar et al. (2017) into delirium careacross the disease trajectory, in particular for pal-liative care patients with severe delirium, or frailerpatients with a very poor performance status.
Antipsychotics are usually used to relieve per-ceptual disturbances (such as hallucinations orillusions) or agitation. A practical approach atthis time is to maximize supportive non-pharmacological strategies for all patients, withidentification and appropriate management ofdelirium precipitating factors where their reversalis in alignment with established goals of care.Pharmacological management approaches shouldbe reserved for patients with severe agitation atrisk of harm to themselves or if safety concerns, orto target psychotic symptoms causing severe dis-tress. In these situations, the short-term use ofantipsychotics in the lowest clinically effectivedose may be indicated. This is in keeping withthe pharmacological recommendation of the 2010NICE Delirium Guideline (NICE 2010). Smallstarting doses of haloperidol (e.g., 0.5–1 mg POor subcut q1hr p.r.n.) may suffice. In elderly orfrail patients, lower doses should be used, e.g.,haloperidol 0.25–0.5 mg, and titrated gradually.The efficacy of haloperidol should be evaluated30–60 min after administration. Patients shouldalso have routine assessments for akathisia andother extrapyramidal side effects (EPS). First-generation antipsychotics (e.g., haloperidol)should be avoided in patients with Parkinson’sDisease or dementia with Lewy bodies (DLB),because of the risks of EPS and disease exacerba-tion. If treatment with an antipsychotic is requiredin these patients, then the second-generation anti-psychotic quetiapine may be considered.
Delirium as a Palliative Care Emergency 13

The Role for BenzodiazepinesBenzodiazepines are known to be deliriogenic,especially in higher doses, and are a risk factorfor falls (Clegg and Young 2011; Stone et al.2012). In view of this, it has been recommendedthat benzodiazepines are not used as first-linemedications for the management of delirium thatmay be reversible (Irwin et al. 2013). However,benzodiazepines do have a role as first-line agentsin managing agitation due to alcohol or benzodi-azepine withdrawal.
Returning to the seminal trial in AIDS patientsby Breitbart et al. mentioned above, only 6 of 30patients received lorazepam, as the researchersstopped the lorazepam arm early due to concernsof treatment-limiting side effects (Breitbart et al.1996). These included not only increased confu-sion, but also excess sedation, disinhibition, andataxia. A recent study in 49 CAM-positivepatients with agitation reported that a combinationprotocol of haloperidol and midazolam was moreeffective than haloperidol alone (FerrazGonçalves et al. 2016). The onset of action for asubcutaneous injection of midazolam is only5–10 min. The optimal role of “rescue” doses ofmidazolam and other benzodiazepines such aslorazepam in the crisis management of a severelyagitated and distressed delirious patient, who hasnot responded to nonpharmacological strategiesor an antipsychotic as first-line management,requires further study.
10 The Delirium Experience andSupport
Delirium causes significant distress for patients aswell as their families, countering the oft-hearddescription of the “pleasantly confused” patient(Breitbart et al. 2002; Bruera et al. 2009). In twostudies using the Delirium Experience Question-naire (DEQ) in hospitalized cancer patients,54–74% of patients recalled their own symptomsafter delirium resolution, and had significant asso-ciated distress (Breitbart et al. 2002; Bruera et al.2009). Of note, patients having no recall of theirdelirium episode were also significantly dis-tressed, and that hypoactive delirium was just as
distressing for patients as hyperactive delirium.Patients report feeling anxious, threatened, and alack of control, as well as feeling that they are notbeing listened to or understood by the healthcareteam. (See also Sect. 9.1 for communication strat-egies with delirious patients.) As part of theirdelirium experience, patients also experiencevisual hallucinations, misperceptions, and delu-sions which are frequently of staff, other patients,and deceased family members (Partridge et al.2013). Patients who have recovered from deliriummay require formal debriefing to alleviate theirfears.
While the presence of a reassuring familymember appears to be beneficial to deliriouspatients, family members experience distresswhen observing delirium in their loved one.Spouses and nonprofessional caregivers reporthigher distress rating scores on the DEQ thanpatients (Breitbart et al. 2002). Family membersoften feel helpless and describe negative emo-tions, include anxiety and caregiver burden(Buss et al. 2007; Finucane et al. 2017). Familydistress may be ameliorated if they are expectingdelirium as part of the patient’s illness (Partridgeet al. 2013). Families have previously described aneed for more informational support about delir-ium (Namba et al. 2007; Toye et al. 2014). Com-munication must be clear and consistent from allmembers of the interprofessional healthcare team,and tailored to the family’s needs. Family mem-bers report delirium information leaflets to be auseful strategy in supporting their needs (Otani etal. 2013).
The distress of family members increases witha patient’s symptom severity, terminal illness pro-gression and declining performance status(Dumont et al. 2006). The fact that delirium candeprive patients and family members of effectivecommunication becomes even more poignant inthe face of approaching death. As deliriouspatients are often psychologically absent althoughtheir body is still physically present, family mem-bers may experience “ambiguous” loss (Day andHiggins 2016). In turn, this may later lead todifficulties in an individual’s grief journey. Thehealthcare team has a pivotal role in supporting
14 S. H. Bush

families at this time, and legitimizing their feel-ings of loss.
Delirium also impacts on members of thehealthcare team. Nursing staff report “stress dueto the unpredictability of delirium and workload,”as well as safety concerns (Partridge et al. 2013).The behaviors of patients with hyperactive delir-ium who appear to be uncooperative or pulling attubes and lines can be particularly challenging tocare for, especially at night (Mc Donnell andTimmins 2012). Effective educational traininginterventions in the management of patients withdelirium are required for all members of theinterprofessional healthcare team, with the aimof increasing knowledge, skills, and self-efficacy,as well as providing a unified and consistentapproach to care. Unit-level debriefing sessionsmay be required following difficult cases as partof institutional support.
11 Refractory Delirium at the Endof Life
A symptom is defined as refractory if it cannot beadequately controlled and continues to cause dis-tress despite the use of all other possible andtolerable symptomatic treatments that do not com-promise consciousness (Cherny and Portenoy1994). The occurrence of an irreversible refrac-tory delirium in a physically declining palliativecare patient is a poor prognostic sign, indicatingthat death may occur in days or even hours, ratherthan weeks (Leonard et al. 2008; de la Cruz et al.2015b). This information should be sensitivelyexplained to the family, and patient where possi-ble, and support provided to prepare for the dyingphase.
Severe refractory delirium at the end of lifemay also necessitate “emergency” managementby the interprofessional healthcare team. Criticalaction is warranted to reduce not only potentialpatient distress, but also importantly family dis-tress at witnessing severe agitation in a loved oneapproaching the end of life which may subse-quently negatively impact on their bereavement(Morita et al. 2007; Cohen et al. 2009). In thewords of Dame Cicely Saunders who founded
St. Christopher’s Hospice in Sydenham, Londonin 1967: “How people die remains in the memoryof those who live on.” Dying patients with refrac-tory delirium, who remain very agitated and dis-tressed despite antipsychotics, may requireadditional pharmacological management in theform of palliative sedation.
12 Palliative Sedation forRefractory Agitated Delirium atthe End of Life
Over the years, authors and guidelines have pro-vided many definitions for palliative sedation, orsedation in the terminal phase (usually referring tothe last days up to the last 2 weeks of life) (Bush etal. 2014). As part of a 10-point framework in2009, the European Association of PalliativeCare (EAPC) defined “therapeutic sedation” or“palliative sedation” as “the monitored use ofmedications intended to induce a state ofdecreased or absent awareness (unconsciousness)in order to relieve the burden of otherwise intrac-table suffering in a manner that is ethically accept-able to the patient, family and health careproviders” (Cherny and Radbruch 2009). Propor-tionate palliative sedation is an ethically acceptedintervention and does not hasten death. Palliativesedation can be administered intermittently, astemporary “respite” sedation for an uncontrolledsymptom, or continuously. Midazolam is the med-ication most frequently used for palliative seda-tion and refractory delirium is the most commonindication (Maltoni et al. 2012).
See chapter ▶ “Palliative Sedation”.More evidence is needed on the efficacy of
palliative sedation for the management of refrac-tory delirium, as well as other refractory symp-toms at the end of life (Beller et al. 2015). Inaddition, it is important that palliative sedationguideline implementation is supported by com-prehensive staff training and education strategies.
Family members require ongoing support atthis time. While often feeling relief at seeingtheir loved one’s comfort, family members mayalso experience distress due to patient’s lack ofcommunication, guilt over the decision-making
Delirium as a Palliative Care Emergency 15
process, in addition to anticipatory grief (Chernyand ESMO Guidelines Working Group 2014).Family members have also reported receivinginsufficient or unclear information regarding pal-liative sedation (Bruinsma et al. 2013). Clearhealthcare team communication with familymembers and other team members should be apriority, especially before and during palliativesedation. Families often have mixed feelingsbetween wanting relief of the patient’s suffering,but also wanting consciousness maintained(Finucane et al. 2017). As a practice point, if apatient has become increasingly agitated over thecourse of a day, it can be advantageous for thehealth care team to brief the family in advance (aswell as the patient if possible) if the team antici-pates that the patient is likely to require sedationovernight for their comfort. This preparation mayhelp to mitigate some of the distress of familymembers if the sedated patient is not able tohave meaningful conversations with them thenext day.
13 Conclusion and Summary
Delirium is a clinical emergency requiring promptassessment and management according to apatient’s goals of care by all members of theinterprofessional healthcare team. Delirium canbe anticipated by the healthcare team if the patientis assessed to be in a high risk group, orapproaching the last hours to weeks of life. Thedevelopment of validated models (specific to pal-liative care populations) to predict delirium devel-opment and to predict response to treatment ofdelirium precipitants according to a patient’sgoals of care will assist in this endeavor. Furtherresearch is required to ascertain the optimal man-agement strategies of delirium, according tounderlying pathophysiology and across the palli-ative care patient’s illness trajectory. Planning forthe occurrence of delirium is of immense benefitto the patient, their family, and healthcare teamand, in turn, has the potential to reduce the distressassociated with this common deleteriousneurocognitive syndrome.
References
Agar MR, Lawlor PG, Quinn S, Draper B, Caplan G,Rowett D, et al. Efficacy of oral risperidone, haloperi-dol, or placebo for symptoms of delirium amongpatients in palliative care: a randomized clinical trial.JAMA Intern Med. 2017;177:34–42. https://doi.org/10.1001/jamainternmed.2016.7491.
American Psychiatric Association. Diagnostic and statisti-cal manual of mental disorders, text revision. 4th ed.Washington, DC: American Psychiatric Association;2000.
American Psychiatric Association. Diagnostic and statisti-cal manual of mental disorders. 5th ed. Washington,DC: American Psychiatric Association; 2013.
Bellelli G, Morandi A, Davis DHJ, Mazzola P, Turco R,Gentile S, et al. Validation of the 4AT, a new instrumentfor rapid delirium screening: a study in 234 hospitalisedolder people. Age Ageing. 2014;43:496–502. https://doi.org/10.1093/ageing/afu021.
Bellelli G, Morandi A, Di Santo SG, Mazzone A, Cheru-bini A, Mossello E, et al. “Delirium day”: a nationwidepoint prevalence study of delirium in older hospitalizedpatients using an easy standardized diagnostic tool.BMC Med. 2016;14:106. https://doi.org/10.1186/s12916-016-0649-8.
Beller EM, van Driel ML,McGregor L, Truong S,MitchellG. Palliative pharmacological sedation for terminally illadults. Cochrane Database Syst Rev. 2015;CD010206.https://doi.org/10.1002/14651858.CD010206.pub2
Body JJ, Niepel D, Tonini G. Hypercalcaemia and hypo-calcaemia: finding the balance. Support Care Cancer.2017;25:1639–49. https://doi.org/10.1007/s00520-016-3543-1.
Breitbart W, Alici Y. Agitation and delirium at the end oflife: “we couldn’t manage him”. JAMA.2008;300:2898–910. https://doi.org/10.1001/jama.2008.885.
Breitbart W, Alici Y. Evidence-based treatment of deliriumin patients with cancer. J Clin Oncol. 2012;30:1206–14.https://doi.org/10.1200/JCO.2011.39.8784.
Breitbart W, Marotta R, Platt MM, Weisman H, DerevencoM, Grau C, et al. A double-blind trial of haloperidol,chlorpromazine, and lorazepam in the treatment ofdelirium in hospitalized AIDS patients. Am J Psychia-try. 1996;153:231–7. https://doi.org/10.1176/ajp.153.2.231.
Breitbart W, Rosenfeld B, Roth A, Smith MJ, Cohen K,Passik S. The memorial delirium assessment scale.J Pain Symptom Manag. 1997;13:128–37. https://doi.org/10.1016/S0885-3924(96)00316-8.
Breitbart W, Gibson C, Tremblay A. The delirium experi-ence: delirium recall and delirium-related distress inhospitalized patients with cancer, their spouses/care-givers, and their nurses. Psychosomatics.2002;43:183–94.
Bruera E, Bush SH, Willey J, Paraskevopoulos T, Li Z,Palmer JL, et al. Impact of delirium and recall on thelevel of distress in patients with advanced cancer and
16 S. H. Bush

their family caregivers. Cancer. 2009;115:2004–12.https://doi.org/10.1002/cncr.24215.
Bruinsma S, Rietjens J, van der Heide A. Palliative seda-tion: a focus group study on the experiences of rela-tives. J Palliat Med. 2013;16:349–55. https://doi.org/10.1089/jpm.2012.0410.
Buckley NA, Dawson AH, Isbister GK. Serotonin syn-drome. BMJ. 2014;348:g1626.
Bush SH, Leonard MM, Agar M, Spiller JA, Hosie A,Wright DK, et al. End-of-life delirium: issues regardingrecognition, optimal management, and the role of seda-tion in the dying phase. J Pain Symptom Manag.2014;48:215–30. https://doi.org/10.1016/j.jpainsymman.2014.05.009.
Buss M, Vanderwerker L, Inouye SK, Zhang B, Block S,Prigerson H. Associations between caregiver-perceiveddelirium in patients with cancer and generalized anxi-ety in their caregivers. J Palliat Med. 2007;10:1083–92.
Canadian Coalition for Seniors’ Mental Health. Guidelineon the assessment and treatment of delirium in olderadults at the end of life. Toronto: Canadian Coalitionfor Seniors’ Mental Health; 2010.
Candy B, Jackson Kenneth C, Jones L, Leurent B,Tookman A, King M. Drug therapy for delirium interminally ill adult patients. Cochrane Database SystRev. 2012;CD004770. https://doi.org/10.1002/14651858.CD004770.pub2
Caraceni A, Nanni O, Maltoni M, Piva L, Indelli M,Arnoldi E, et al. Impact of delirium on the short termprognosis of advanced cancer patients. Cancer.2000;89:1145–9.
Casarett D, Inouye SK. American College of Physicans-American Society of internal medicine end-of-life careconsensus panel. Diagnosis and management of delir-ium near the end of life. Ann Intern Med.2001;135:32–40.
Cherny N, ESMO Guidelines Working Group. ESMOClinical Practice Guidelines for the management ofrefractory symptoms at the end of life and the use ofpalliative sedation. Ann Oncol. 2014;25(Suppl 3):iii143–52. https://doi.org/10.1093/annonc/mdu238.
Cherny N, Portenoy R. Sedation in the management ofrefractory symptoms: guidelines for evaluation andtreatment. J Palliat Care. 1994;10:31–8.
Cherny N, Radbruch L. European Association for Pallia-tive Care (EAPC) recommended framework for the useof sedation in palliative care. Palliat Med.2009;23:581–93. https://doi.org/10.1177/0269216309107024.
Clegg A, Young JB. Which medications to avoid in peopleat risk of delirium: a systematic review. Age Ageing.2011;40:23–9. https://doi.org/10.1093/ageing/afq140.
Clegg A, Westby M, Young JB. Under-reporting of delir-ium in the NHS. Age Aging. 2011;40:283–6. https://doi.org/10.1093/ageing/afq157.
Cohen MZ, Pace EA, Kaur G, Bruera E. Delirium inadvanced cancer leading to distress in patients andfamily caregivers. J Palliat Care. 2009;25:164–71.
Darbyshire JL, Young JD. An investigation of sound levelson intensive care units with reference to the WHOguidelines. Crit Care. 2013;17:R187. https://doi.org/10.1186/cc12870.
Dasgupta M, Hillier LM. Factors associated with pro-longed delirium: a systematic review. Int Psychogeriatr.2010;22:373–94. https://doi.org/10.1017/S1041610209991517.
Day J, Higgins I. Mum’s absence(s): conceptual insightsinto absence as loss during a loved one’s delirium.J Clin Nurs. 2016;25:2066–73. https://doi.org/10.1111/jocn.13268.
de la Cruz M, Fan J, Yennu S, Tanco K, Shin S, Wu J, et al.The frequency of missed delirium in patients referred topalliative care in a comprehensive cancer center. Sup-port Care Cancer. 2015a;23:2427–33. https://doi.org/10.1007/s00520-015-2610-3.
de la CruzM, Ransing V, Yennu S,Wu J, Liu D, ReddyA, etal. The frequency, characteristics, and outcomes amongcancer patients with delirium admitted to an acute palli-ative care unit. Oncologist. 2015b;20:1425–31. https://doi.org/10.1634/theoncologist.2015-0115.
Dumont S, Turgeon J, Allard P, Gagnon P, Charbonneau C,Vézina L. Caring for a loved one with advanced cancer:determinants of psychological distress in family care-givers. J Palliat Med. 2006;9:912–21. https://doi.org/10.1089/jpm.2006.9.912.
Engel G, Romano J. Delirium, a syndrome of cerebralinsufficiency. J Chronic Dis. 1959;9:260–77.
Ferraz Gonçalves JA, Almeida A, Costa I, Silva P, CarneiroR. Comparison of haloperidol alone and in combinationwith midazolam for the treatment of acute agitation inan inpatient palliative care service. J Pain Palliat CarePharmacother. 2016;30:284–8.
Finucane AM, Lugton J, Kennedy C, Spiller JA. Theexperiences of caregivers of patients with delirium,and their role in its management in palliative caresettings: an integrative literature review.Psychooncology. 2017;26:291–300. https://doi.org/10.1002/pon.4140.
Flaherty J, Gonzales J, Dong B. Antipsychotics in thetreatment of delirium in older hospitalized adults: asystematic review. J Am Geriatr Soc. 2011;59(Suppl2):S269–76. https://doi.org/10.1111/j.1532-5415.2011.03675.x.
Fong TG, Davis D, Growdon ME, Albuquerque A, InouyeSK. The interface between delirium and dementia inelderly adults. Lancet Neurol. 2015;14:823–32.
Gagliese L, Rodin R, Chan V, Stevens B, Zimmermann C.How do healthcare workers judge pain in older pallia-tive care patients with delirium near the end of life?Palliat Support Care. 2016;14:151–8. https://doi.org/10.1017/S1478951515000929.
Gagnon P, Allard P, Gagnon B, Mérette C, Tardif F. Delir-ium prevention in terminal cancer: assessment of amulticomponent intervention. Psychooncology.2012;21:187–94. https://doi.org/10.1002/pon.1881.
Gaudreau JD, Gagnon P, Harel F, Roy MA. Impact ondelirium detection of using a sensitive instrument
Delirium as a Palliative Care Emergency 17

integrated into clinical practice. Gen Hosp Psychiatry.2005;27:194–9. https://doi.org/10.1016/j.genhosppsych.2005.01.002.
Hosie A, Davidson PM, Agar M, Sanderson CR, Phillips J.Delirium prevalence, incidence, and implications forscreening in specialist palliative care inpatient settings:a systematic review. Palliat Med. 2013;27:486–98.https://doi.org/10.1177/0269216312457214.
Hshieh TT, Yue J, Oh E, Puelle M, Dowal S, Travison T, etal. Effectiveness of multicomponent non-pharmacological delirium interventions: a meta-analy-sis. JAMA Intern Med. 2015;175:512–20. https://doi.org/10.1001/jamainternmed.2014.7779.
Hu MI, Glezerman IG, Leboulleux S, Insogna K, GucalpR, Misiorowski W, Yu B, Zorsky P, Tosi D, Bessudo A,Jaccard A, Tonini G, Ying W, Braun A, Jain RK.Denosumab for treatment of hypercalcemia of malig-nancy. J Clin Endocrinol Metab. 2014;99:3144–52.https://doi.org/10.1210/jc.2014-1001.
Hui D, dos Santos R, Reddy S, Nascimento M, ZhukovskyDS, Paiva CE, et al. Acute symptomatic complicationsamong patients with advanced cancer admitted to acutepalliative care units: a prospective observational study.Palliat Med. 2015;29:826–33. https://doi.org/10.1177/0269216315583031.
Indelicato R, Portenoy RK. Opioid rotation in the manage-ment of refractory cancer pain. J Clin Oncol.2002;20:348–52. https://doi.org/10.1200/JCO.2002.20.1.348.
Inouye SK, Van Dyck CH, Alessi CA, Balkin S, Siegal AP,Horwitz RI. Clarifying confusion: the confusion assess-ment method: a new method for detection of delirium.Ann Intern Med. 1990;113:941–8. https://doi.org/10.7326/0003-4819-113-12-941.
Inouye SK, Baker DI, Fugal P, Bradley EH. Disseminationof the hospital elder life program: implementation,adaptation, and successes. J Am Geriatr Soc.2006;54:1492–9.
Inouye SK,Westendorp R, Saczynski J. Delirium in elderlypeople. Lancet. 2014a;383:911–22. https://doi.org/10.1016/S0140-6736(13)60688-1.
Inouye SK, Marcantonio E, Metzger E. Doing damage indelirium: the hazards of antipsychotic treatment inelderly persons. Lancet Psychiatr. 2014b;1:312–5.
Irwin S, Pirrello R, Hirst J, Buckholz G, Ferris F. Clarifyingdelirium management: practical, evidence-based,expert recommendations for clinical practice. J PalliatMed. 2013;16:423–35. https://doi.org/10.1089/jpm.2012.0319.
Katus L, Frucht S. Management of serotonin syndrome andneuroleptic malignant syndrome. Curr Treat OptionsNeurol. 2016;18:39. https://doi.org/10.1007/s11940-016-0423-4.
Kerr CW, Donnelly JP, Wright ST, Luczkiewicz DL,McKenzie KJ, Hang PC, et al. Progression of deliriumin advanced illness: a multivariate model of caregiverand clinician perspectives. J Palliat Med.2013;16:768–73. https://doi.org/10.1089/jpm.2012.0561.
Kim S-Y, Kim S-W, Kim J-M, Shin I-S, Bae K-Y, Shim H-J, et al. Differential associations between delirium andmortality according to delirium subtype and age: aprospective cohort study. Psychosom Med.2015;77:903–10.
Laurila JV, LaakkonenML, Laurila JV, Timo SE, Reijo TS.Predisposing and precipitating factors for delirium in afrail geriatric population. J Psychosom Res.2008;65:249–54. https://doi.org/10.1016/j.jpsychores.2008.05.026.
Lawlor PG, Bush SH. Delirium in patients with cancer:assessment, impact, mechanisms and management. NatRev Clin Oncol. 2015;12:77–92. https://doi.org/10.1038/nrclinonc.2014.147.
Lawlor P, Gagnon B, Mancini I, Pereira J, Hanson J,Suarez-Almazor M, et al. Occurrence, causes, and out-come of delirium in patients with advanced cancer: aprospective study. Arch Intern Med. 2000;160:786–94.
Leentjens AFG, Rundell J, Rummans T, Shim JJ, OldhamR, Peterson L, et al. Delirium: an evidence-based med-icine (EBM) monograph for psychosomatic medicinepractice, commissioned by the Academy of Psychoso-matic Medicine (APM) and the European Associationof Consultation Liaison Psychiatry and Psychoso-matics (EACLPP). J Psychosom Res.2012;73:149–52. https://doi.org/10.1016/j.jpsychores.2012.05.009.
Leonard MM, Raju B, Conroy M, Donnelly S, TrzepaczPT, Saunders J, et al. Reversibility of delirium in ter-minally ill patients and predictors of mortality. PalliatMed. 2008;22:848–54. https://doi.org/10.1177/0269216308094520.
Leonard MM, Agar M, Spiller JA, Davis B, MohamadMM, Meagher DJ, et al. Delirium diagnostic and clas-sification challenges in palliative care: subsyndromaldelirium, comorbid delirium-dementia, and psychomo-tor subtypes. J Pain Symptom Manag.2014;48:199–214.
Maltoni M, Scarpi E, Rosati M, Derni S, Fabbri L, MartiniF, et al. Palliative sedation in end-of-life care and sur-vival: a systematic review. J Clin Oncol.2012;30:1378–83. https://doi.org/10.1200/JCO.2011.37.3795.
Marcantonio ER, Ngo LH, O’Connor M, Jones RN, CranePK, Metzger ED, et al. 3D-CAM: derivation and vali-dation of a 3-minute diagnostic interview for CAM-defined delirium: a cross-sectional diagnostic teststudy. Ann Intern Med. 2014;161:554–61. https://doi.org/10.7326/M14-0865.
Maust DT, Kim HM, Seyfried LS, Chiang C, Kavanagh J,Schneider LS, et al. Antipsychotics, other psychotro-pics, and the risk of death in patients with dementia:number needed to harm. JAMA Psychiat.2015;72:438–45. https://doi.org/10.1001/jamapsychiatry.2014.3018.
Mc Donnell S, Timmins F. A quantitative exploration ofthe subjective burden experienced by nurses when car-ing for patients with delirium. J Clin Nurs.
18 S. H. Bush

2012;21:2488–98. https://doi.org/10.1111/j.1365-2702.2012.04130.x.
Meagher DJ, Leonard M, Donnelly S, Conroy M, AdamisD, Trzepacz PT. A longitudinal study of motor subtypesin delirium: frequency and stability during episodes. JPsychosom Res. 2012;72:236–41. https://doi.org/10.1016/j.jpsychores.2011.11.013.
Michaud L, Büla C, Berney A, Camus V, Voellinger R,Stiefel F, et al. Delirium: guidelines for general hospi-tals. J Psychosom Res. 2007;62:371–83.
Morandi A, Pandharipande P, Trabucchi M, Rozzini R,Mistraletti G, Trompeo AC, et al. Understanding inter-national differences in terminology for delirium andother types of acute brain dysfunction in critically illpatients. Intensive Care Med. 2008;34:1907–15.https://doi.org/10.1007/s00134-008-1177-6.
Morandi A, Davis D, Bellelli G, Arora RC, Caplan GA,Kamholz B, et al. The diagnosis of delirium super-imposed on dementia: an emerging challenge. J AmMed Dir Assoc. 2017;18:12–8. https://doi.org/10.1016/j.jamda.2016.07.014.
Morita T, Tei Y, Tsunoda J, Inoue S, Chihara S. Underlyingpathologies and their associations with clinical featuresin terminal delirium of cancer patients. J Pain SymptomManag. 2001;22:997–1006.
Morita T, Akechi T, Ikenaga M, Inoue S, Kohara H,Matsubara T, et al. Terminal delirium: recommenda-tions from bereaved families’ experiences. J PainSymptom Manag. 2007;34:579–89. https://doi.org/10.1016/j.jpainsymman.2007.01.012.
Nakajima N, Satake N, Nakaho T. Indications and practiceof artificial hydration for terminal ill cancer patients.Curr Opin Support Palliat Care. 2014;8:358–63.https://doi.org/10.1097/SPC.0000000000000089.
Namba M, Morita T, Imura C, Kiyohara E, Ishikawa S,Hirai K. Terminal delirium: families’ experience.Palliat Med. 2007;21:587–94.
National Institute for Health and Care Excellence. Delir-ium: diagnosis, prevention and management. Clinicalguideline 103. 2010. http://www.nice.org.uk/CG103.Accessed 2 May 2017.
Neufeld K, Yue J, Robinson T, Inouye SK, Needham D.Antipsychotic medication for prevention and treatmentof delirium in hospitalized adults: a systematic reviewand meta-analysis. J Am Geriatr Soc. 2016;64:705–14.https://doi.org/10.1111/jgs.14076.
Otani H, Morita T, Uno S, Yamamoto R, Hirose H,Matsubara T, et al. Usefulness of the leaflet-based inter-vention for family members of terminally ill cancerpatients with delirium. J Palliat Med.2013;16:419–22. https://doi.org/10.1089/jpm.2012.0401.
Oxford University Press. Oxford dictionary. 2017. https://en.oxforddictionaries.com/definition/medical_emergency. Accessed 22 Mar 2017.
Partridge JS, Martin FC, Harari D, Dhesi JK. The deliriumexperience: what is the effect on patients, relatives andstaff and what can be done to modify this? Int J GeriatrPsychiatry. 2013;28:804–12. https://doi.org/10.1002/gps.3900.
Pealing L, Iliffe S. A woman with forgetfulness and falls.BMJ. 2011;24:d7412. https://doi.org/10.1136/bmj.d7412.
PendleburyS, LovettN, Smith S, Dutta N, BendonC,Lloyd-Lavery A, et al. Observational, longitudinal study ofdelirium in consecutive unselected acute medical admis-sions: age-specific rates and associated factors, mortalityand re-admission. BMJ Open. 2015;5:e007808. https://doi.org/10.1136/bmjopen-2015-007808.
Ryan DJ, O’Regan NA, Caoimh RÓ, Clare J, O’ConnorM,Leonard M, et al. Delirium in an adult acute hospitalpopulation: predictors, prevalence and detection. BMJOpen. 2013;3:e001772. https://doi.org/10.1136/bmjopen-2012-001772.
Sands MB, Dantoc BP, Hartshorn A, Ryan C, Lujic S.Single question in delirium (SQiD): testing its efficacyagainst psychiatrist interview, the confusion assess-ment method and the memorial delirium assessmentscale. Palliat Med. 2010;24:561–5. https://doi.org/10.1177/0269216310371556.
Schuurmans MJ, Shortridge-Baggett LM, Duursma SA.The delirium observation screening scale: a screeninginstrument for delirium. Res Theory Nurs Pr.2003;17:31–50.
Siddiqi N, Harrison JK, Clegg A, Teale EA, Young J,Taylor J, et al. Interventions for preventing delirium inhospitalised non-ICU patients. Cochrane Database SystRev. 2016;CD005563. https://doi.org/10.1002/14651858.CD005563.pub3
Stewart AF. Clinical practice. Hypercalcemia associatedwith cancer. N Engl J Med. 2005;352:373–9. https://doi.org/10.1056/NEJMcp042806.
Stone C, Lawlor P, Savva G, Bennett K, Kenny R. Pro-spective study of falls and risk factors for falls in adultswith advanced cancer. J Clin Oncol. 2012;30:2128–33.https://doi.org/10.1200/JCO.2011.40.7791.
Toye C, Matthews A, Hill A, Maher S. Experiences, under-standings and support needs of family carers of olderpatients with delirium: a descriptive mixed methodsstudy in a hospital delirium unit. Int J Older PeopleNursing. 2014;9:200–8. https://doi.org/10.1111/opn.12019.
Trzepacz PT, Mittal D, Torres R, Kanary K, Norton J,Jimerson N. Validation of the delirium rating scale-revised-98: comparison with the delirium rating scaleand the cognitive test for delirium [internet]. J Neuro-psychiatry Clin Neurosci. 2001;13:229–42.
Winnipeg Regional Health Authority. WRHA policy num-ber: 110.000.200: advance care planning – goals ofcare. 2011. http://www.wrha.mb.ca/index.php.Accessed 2 May 2017.
World Health Organization. The ICD-10 classification ofmental and behavioural disorders: clinical descriptionsand diagnostic guidelines. 1992. http://www.who.int/classifications/icd/en/bluebook.pdf. Accessed 3 May2017.
Zimberg M, Berenson S. Delirium in patients with cancer:nursing assessment and intervention. Oncol NursForum. 1990;17:529–38.
Delirium as a Palliative Care Emergency 19
Related Documents











