1 23 Social Psychiatry and Psychiatric Epidemiology The International Journal for Research in Social and Genetic Epidemiology and Mental Health Services ISSN 0933-7954 Volume 48 Number 9 Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481-1489 DOI 10.1007/s00127-013-0690-2 Deliberate self-harm before psychiatric admission and risk of suicide: survival in a Danish national cohort Trine Madsen, Esben Agerbo, Preben B. Mortensen & Merete Nordentoft

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1 23
Social Psychiatry and PsychiatricEpidemiologyThe International Journal for Researchin Social and Genetic Epidemiology andMental Health Services ISSN 0933-7954Volume 48Number 9 Soc Psychiatry Psychiatr Epidemiol(2013) 48:1481-1489DOI 10.1007/s00127-013-0690-2
Deliberate self-harm before psychiatricadmission and risk of suicide: survival in aDanish national cohort
Trine Madsen, Esben Agerbo, PrebenB. Mortensen & Merete Nordentoft

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer-
Verlag Berlin Heidelberg. This e-offprint is
for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.
ORIGINAL PAPER
Deliberate self-harm before psychiatric admission and riskof suicide: survival in a Danish national cohort
Trine Madsen • Esben Agerbo • Preben B. Mortensen •
Merete Nordentoft
Received: 17 December 2012 / Accepted: 9 April 2013 / Published online: 23 April 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract
Purpose Psychiatric illness and deliberate self-harm
(DSH) are major risk factors of suicide. In largely 15 % of
psychiatric admissions in Denmark, the patient had an
episode of DSH within the last year before admission. This
study examined the survival and predictors of suicide in a
suicidal high-risk cohort consisting of hospitalized psy-
chiatric patients with recent DSH.
Methods This national prospective register-based study
examined all hospitalized psychiatric patients who self-
harmed within a year before admission. All admitted
patients, in the time period 1998–2006, were followed and
survival analyses techniques were used to identify predic-
tors of suicide.
Results The study population consisted of 17,257
patients; 520 (3 %) died by suicide during follow-up; 50 %
of the suicides occurred within a year from the index
admission. A rate of 1,645 suicides per 100,000 person–
years in the first year after psychiatric admission was
found. Adjusted analyses showed that a higher degree of
education, having DSH within a month before psychiatric
admission and contact with a private psychiatrist increased
the risk of suicide.
Conclusions Psychiatric hospitalized patients with recent
DSH revealed high suicide rates, even during hospitaliza-
tion. When discharging psychiatric patients with recent
DSH careful arrangement of follow-up treatment in the
outpatient setting is recommendable.
Keywords Self-harm � Suicide � Psychiatry �Epidemiology � Survival
Introduction
Psychiatric illness and deliberate self-harm (DSH) are both
major risk factors for completed suicide [1–6]. Hospitalized
psychiatric patients have a long-term prevalence of dying by
suicide on 4–5 % and those patients who in addition have a
history of DSH have a twice as high suicide risk (8–10 %) [7,
8]. Studies examining the risk of suicide among patients
treated for DSH have repeatedly showed that the risk of
suicide is highest within the first year after a non-fatal suicide
and that patients with DSH who have received psychiatric
treatment have an increased suicide risk compared to those
with no psychiatric treatment [9–20].
In about 1/3 of psychiatric admissions in Denmark the
patient has had a previous DSH episode [21], in fact in
15 % of the admissions the DSH episode occurred within
the last year, thus many patients appear at the psychiatric
clinic with two major suicidal risk factors: psychiatric ill-
ness and a recent episode of DSH. Whether the risk of
subsequent suicide differs in patients according to how
recent their episode of DSH was before the psychiatric
hospitalization is yet unexplored. For example, is the
T. Madsen (&) � M. Nordentoft
Psychiatric Center Copenhagen, Copenhagen University
Hospital, Bispebjerg Bakke 23, Building 13A,
2400 Copenhagen, Denmark
e-mail: [email protected]
M. Nordentoft
e-mail: [email protected]
E. Agerbo � P. B. Mortensen
National Center of Register-based Research,
University of Aarhus, Taasingegade 1,
8000 Aarhus C, Denmark
e-mail: [email protected]
P. B. Mortensen
e-mail: [email protected]
123
Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489
DOI 10.1007/s00127-013-0690-2
Author's personal copy

immediate risk of suicide higher in patients who received
no psychiatric hospital treatment in relation to their DSH
episode compared to those who were psychiatrically hos-
pitalized just after an episode? Knowledge of this could be
useful for psychiatric staff who daily assess suicidal risk in
psychiatric patients with a history of DSH. Furthermore,
getting a better understanding of factors associated with
suicide in this suicidal high-risk population, who are
already in contact with the mental health care system, may
enhance our possibility to identify and aid patients in a
suicidal crisis.
Both social and clinical characteristics are important
predictors of completed suicide; however, to our knowl-
edge these factors have not previously been examined in a
national cohort of psychiatrically hospitalized patients with
recent DSH. In addition, we wanted to highlight the risk of
completed suicide among patients admitted to psychiatric
hospital soon after an episode of DSH compared to the risk
in patients who had an episode of DSH more than 6 months
before the psychiatric admission.
Aims of the study
We aimed at estimating the survival, suicide rates and
predictors of suicide in a national cohort of psychiatric
patients who had an episode of DSH within a year before a
psychiatric hospital admission using register-based data.
Materials and methods
We had information on all psychiatric admissions in
Denmark from 1998 to 2006 from The Danish Psychiatric
Central Register [22], which covers all psychiatric inpatient
facilities in Denmark and contains longitudinal information
on all admissions and discharges since 1969. Since 1995,
data on psychiatric outpatient treatment has also been
recorded in this register. By the unique ten-digit identifier
number [23] assigned to all persons living in Denmark we
merged data from four other Danish longitudinal registers
to patients admitted to psychiatric inpatient care. Infor-
mation on hospital-treated DSH was retrieved from The
Danish Patient Registry [24]. From the health Insurance
Register [25], we merged information on all outpatient
private psychiatric and private psychologist appointments
subsidized or partly subsidized by the authorities. Finally,
the Integrated Database for Longitudinal Labor Market
Research gathers information annually on the entire pop-
ulation living in Denmark as of 31 December from several
administrative registers from 1980 onward [26].
From The Danish Cause of Death Register [27]
recordings of suicide according to The International Clas-
sification of Diseases, 10th revision [28] (ICD-10) codes
X60–X84 were obtained for the period from 1 January
1997 to 31 December 2006.
There are no private psychiatric hospitals in Denmark,
and all inpatient and outpatient treatment is free of charge
for all Danish citizens and persons with residence permit.
The study population included hospitalized psychiatric
patients with DSH within the last year before the date of
psychiatric admission aged 18 years or older in the period
from 1998 until 2006. Patients were followed from their
index admission, which was defined as the first psychiatric
admission preceded by an episode of DSH within the last
year.
Admissions with a DSH were registered in The Danish
Patient Registry. The recordings of DSH are not a straight
forward procedure in Denmark thus it was defined in the
following way, which has been validated in a Danish study
[29];
1. All hospital contacts with a cause of contact 4
(admitted because of suicide attempt/self-harm).
2. All contacts with a primary diagnosis of mental illness
and a secondary diagnosis with poisoning in ICD-10
code T36–T50 (medication and biological compounds)
or T52–T60 (chiefly non-medical compounds).
3. All contacts with a primary diagnosis of mental illness
and a secondary diagnosis with a cut lesion on
forearm, wrist or hand (ICD-10 code S51, S55, S59,
S61, S65 or S69).
4. All primary poisoning diagnosis with the following
ICD-10 codes: T39, T40, T42, T43, and T58.
It was found that this definition identified up to 70 % of
patients admitted with DSH (the remaining admitted
because of habitual self-mutilation with no suicidal inten-
tion and admissions due to non-intended poisoning).
The study included 17,257 patients with a median age
on 40 years (interquartile range 29 and 52) and in this
population more women (n = 9,462) than men
(n = 7,795) were psychiatrically admitted within a year
after DSH.
Information on clinical variables
Primary ICD-10 diagnosis given at the psychiatric admis-
sion was used. Diagnoses were categorized into substance
abuse (ICD-10 code F1), schizophrenia spectrum (ICD-10
code F2), affective disorders (ICD-10 code F3), adjustment
or stress-related disorders (ICD-10 code F4) or personality
disorders (ICD-10 code F6), and all others. Associations
between secondary diagnoses and suicide were also stud-
ied; substance abuse, affective disorders and personality
disorders (ICD-10 code F60). The number of psychiatric
admissions before the study period was also included in the
analyses to adjust for psychiatric history.
1482 Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489
123
Author's personal copy

Clinical outpatient care was defined according to whe-
ther a patient received (1) psychiatric outpatient treatment,
or consulted, (2) a private psychiatrist, or (3) a private
psychologist during the last year before the present psy-
chiatric admission.
Patients were categorized into four exclusive groups
according to the time between the date of the DSH and the
date of the psychiatric admission; as to whether the DSH
episode had happened in the last week, 1–3 weeks, 1–6 or
6–12 months before the psychiatric admission.
Information on social variables
We had information on the following socio-demographic
variables; Gross annual income (wages, pensions, unem-
ployment and social security benefits, and interest rates)
which was grouped into age–sex–year population-based
quartiles (i.e., also based on those who had never been
hospitalized); Employment status was divided into being
employed (including adolescents, students, housewives
without labor market attachment and patients with sick
benefits), unemployed, early retirement, and retired. The
Level of education was grouped into elementary school
(9 years in school), high school, vocational training, or a
bachelor degree or higher. Cohabitation status was divided
into five categories: (1) cohabiting/married (cohabiting is
defined as couples of the opposite sex who live together
with shared address and an age difference of less than
15 years and who are not first-degree relatives), (2)
unmarried and living alone, (3) divorced, (4) widowed or
(5) other living status.
Lastly, in the analyses, patients were divided into five
age groups: 18–30, 31–40, 41–50, 51–60 and over 60 years
and these age groups were incorporated in the analyses as
one quantitative covariate.
Generally, for both the clinical and the social variables
the categories in each variable that ordinarily in literature
has the lowest risk of suicide were chosen as the reference
group. One exception was the variable describing admis-
sion diagnosis where we chose the category which included
most patients (those with an affective diagnosis) as we
wanted our reference group to characterize the largest
proportion of the patient case mix. This choice yielded
more relevant clinical information compared to having one
of the less populous categories as reference.
Statistical analysis
Simple statistic procedures were carried out to illuminate
patient characteristics and suicide rates. Kaplan–Meier
curves were performed to illustrate the proportion of
suicide related to psychiatric diagnosis, the timing of
DSH and educational level and by log rank test we
assessed statistically differences in the survival of these
covariates [30]. In Cox regression analyses, we examined
covariates as predictors of suicide. Follow-up time star-
ted at the date of psychiatric admission until death or
until the final censoring date the 31 December 2006.
Mean follow-up time was 1,514 days (just over 4 years).
The covariates were divided into two domains: social
variables and clinical related variables. A three-step
model of analysis was chosen. First step showed all
covariates association with suicide (referred to as the
univariable analyses). Second, assessments of explanatory
variables of suicide in each domain were carried out in
multivariable analyses. The final step (the joint multi-
variable analyses) included the significant predictors
(P value \0.05) from both the social and clinical domain
to assess independent predictors of suicide in multivari-
able analyses thereby adjustment for each domain were
taken into account.
Results
Out of the 17,257 patients, 520 patients died from suicide
during follow-up (3 %) and 1,859 (11 %) died from other
causes. Before being discharged from the current psychi-
atric admission, 32 of the patients died by suicide (6 % of
the suicides) while another 66 (13 %) completed suicide
within a month after discharge and another 261 (50 %)
within a year from psychiatric admission. Overall, the
suicide rate was 727 per 100,000 person–years and the rate
of suicide in the first year after psychiatric admission was
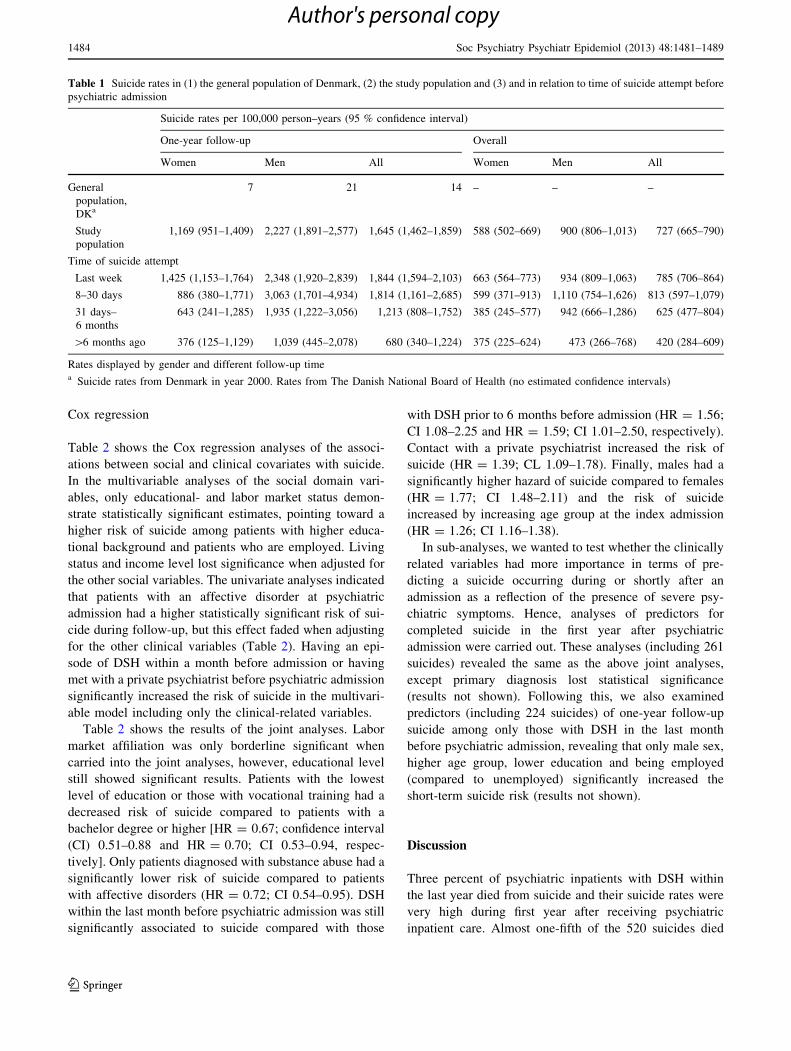
1,645 per 100,000 person–years (See Table 1). The rates
for men with DSH in the month before admission were
high, and in particular men had suicide rates up to 3,000
per 100,000 person–years within the first year. The same
pattern was seen in women, although with fairly lower
rates.
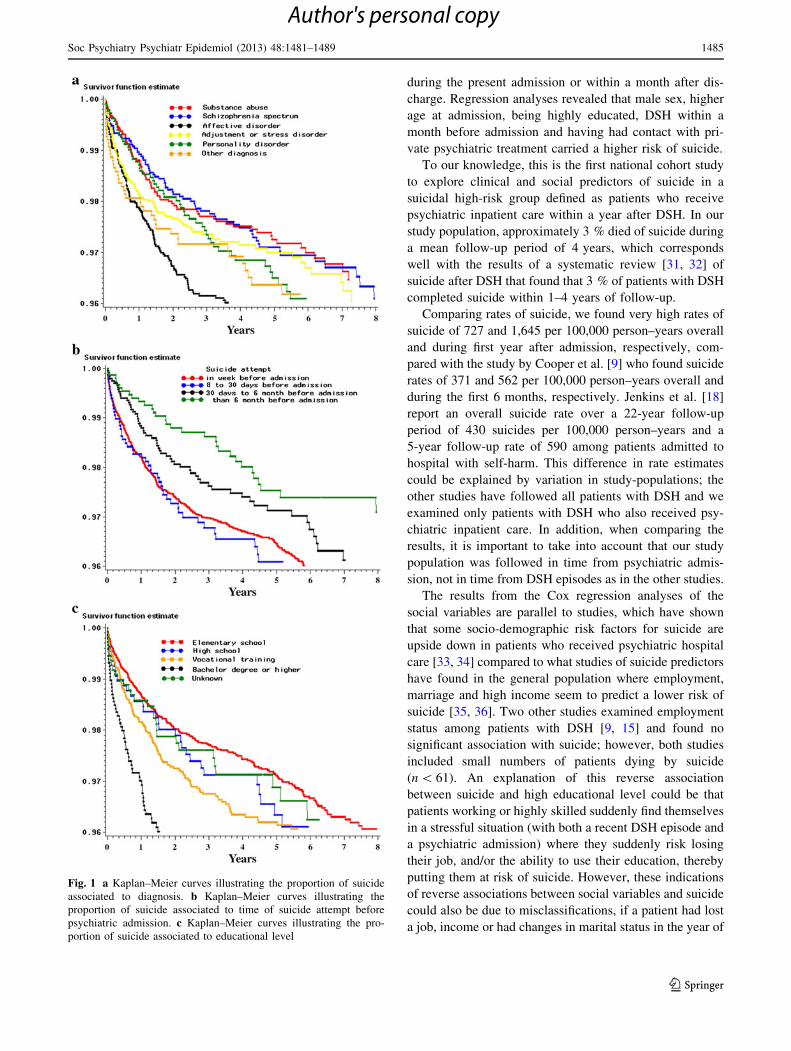
Survival curves
Figure 1 illustrates survival curves in relation to diagnosis
(Fig. 1a), time of DSH episode before psychiatric admis-
sion (Fig. 1b) and educational level (Fig. 1c). The curve
showing the survival by diagnosis indicates that in partic-
ular patients with an affective disorder or those with ‘‘other
diagnosis’’ had a higher risk of dying from suicide, espe-
cially in the first year after admission. Also the survival for
patients with DSH in the week or month before admission
decreased significantly faster compared to patients with
DSH more distant in time before the psychiatric admission.
The survival for patients with the highest educational
degree decreased rapidly in the first year compared to the
survival amongst patients with a lower level of education.
Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489 1483
123
Author's personal copy
Cox regression
Table 2 shows the Cox regression analyses of the associ-
ations between social and clinical covariates with suicide.
In the multivariable analyses of the social domain vari-
ables, only educational- and labor market status demon-
strate statistically significant estimates, pointing toward a
higher risk of suicide among patients with higher educa-
tional background and patients who are employed. Living
status and income level lost significance when adjusted for
the other social variables. The univariate analyses indicated
that patients with an affective disorder at psychiatric
admission had a higher statistically significant risk of sui-
cide during follow-up, but this effect faded when adjusting
for the other clinical variables (Table 2). Having an epi-
sode of DSH within a month before admission or having
met with a private psychiatrist before psychiatric admission
significantly increased the risk of suicide in the multivari-
able model including only the clinical-related variables.
Table 2 shows the results of the joint analyses. Labor
market affiliation was only borderline significant when
carried into the joint analyses, however, educational level
still showed significant results. Patients with the lowest
level of education or those with vocational training had a
decreased risk of suicide compared to patients with a
bachelor degree or higher [HR = 0.67; confidence interval
(CI) 0.51–0.88 and HR = 0.70; CI 0.53–0.94, respec-
tively]. Only patients diagnosed with substance abuse had a
significantly lower risk of suicide compared to patients
with affective disorders (HR = 0.72; CI 0.54–0.95). DSH
within the last month before psychiatric admission was still
significantly associated to suicide compared with those
with DSH prior to 6 months before admission (HR = 1.56;
CI 1.08–2.25 and HR = 1.59; CI 1.01–2.50, respectively).
Contact with a private psychiatrist increased the risk of
suicide (HR = 1.39; CL 1.09–1.78). Finally, males had a
significantly higher hazard of suicide compared to females
(HR = 1.77; CI 1.48–2.11) and the risk of suicide
increased by increasing age group at the index admission
(HR = 1.26; CI 1.16–1.38).
In sub-analyses, we wanted to test whether the clinically
related variables had more importance in terms of pre-
dicting a suicide occurring during or shortly after an
admission as a reflection of the presence of severe psy-
chiatric symptoms. Hence, analyses of predictors for
completed suicide in the first year after psychiatric
admission were carried out. These analyses (including 261
suicides) revealed the same as the above joint analyses,
except primary diagnosis lost statistical significance
(results not shown). Following this, we also examined
predictors (including 224 suicides) of one-year follow-up
suicide among only those with DSH in the last month
before psychiatric admission, revealing that only male sex,
higher age group, lower education and being employed
(compared to unemployed) significantly increased the
short-term suicide risk (results not shown).
Discussion
Three percent of psychiatric inpatients with DSH within
the last year died from suicide and their suicide rates were
very high during first year after receiving psychiatric
inpatient care. Almost one-fifth of the 520 suicides died
Table 1 Suicide rates in (1) the general population of Denmark, (2) the study population and (3) and in relation to time of suicide attempt before
psychiatric admission
Suicide rates per 100,000 person–years (95 % confidence interval)
One-year follow-up Overall
Women Men All Women Men All
General
population,
DKa
7 21 14 – – –
Study
population
1,169 (951–1,409) 2,227 (1,891–2,577) 1,645 (1,462–1,859) 588 (502–669) 900 (806–1,013) 727 (665–790)
Time of suicide attempt
Last week 1,425 (1,153–1,764) 2,348 (1,920–2,839) 1,844 (1,594–2,103) 663 (564–773) 934 (809–1,063) 785 (706–864)
8–30 days 886 (380–1,771) 3,063 (1,701–4,934) 1,814 (1,161–2,685) 599 (371–913) 1,110 (754–1,626) 813 (597–1,079)
31 days–
6 months
643 (241–1,285) 1,935 (1,222–3,056) 1,213 (808–1,752) 385 (245–577) 942 (666–1,286) 625 (477–804)
[6 months ago 376 (125–1,129) 1,039 (445–2,078) 680 (340–1,224) 375 (225–624) 473 (266–768) 420 (284–609)
Rates displayed by gender and different follow-up timea Suicide rates from Denmark in year 2000. Rates from The Danish National Board of Health (no estimated confidence intervals)
1484 Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489
123
Author's personal copy
during the present admission or within a month after dis-
charge. Regression analyses revealed that male sex, higher
age at admission, being highly educated, DSH within a
month before admission and having had contact with pri-
vate psychiatric treatment carried a higher risk of suicide.
To our knowledge, this is the first national cohort study
to explore clinical and social predictors of suicide in a
suicidal high-risk group defined as patients who receive
psychiatric inpatient care within a year after DSH. In our
study population, approximately 3 % died of suicide during
a mean follow-up period of 4 years, which corresponds
well with the results of a systematic review [31, 32] of
suicide after DSH that found that 3 % of patients with DSH
completed suicide within 1–4 years of follow-up.
Comparing rates of suicide, we found very high rates of
suicide of 727 and 1,645 per 100,000 person–years overall
and during first year after admission, respectively, com-
pared with the study by Cooper et al. [9] who found suicide
rates of 371 and 562 per 100,000 person–years overall and
during the first 6 months, respectively. Jenkins et al. [18]
report an overall suicide rate over a 22-year follow-up
period of 430 suicides per 100,000 person–years and a
5-year follow-up rate of 590 among patients admitted to
hospital with self-harm. This difference in rate estimates
could be explained by variation in study-populations; the
other studies have followed all patients with DSH and we
examined only patients with DSH who also received psy-
chiatric inpatient care. In addition, when comparing the
results, it is important to take into account that our study
population was followed in time from psychiatric admis-
sion, not in time from DSH episodes as in the other studies.
The results from the Cox regression analyses of the
social variables are parallel to studies, which have shown
that some socio-demographic risk factors for suicide are
upside down in patients who received psychiatric hospital
care [33, 34] compared to what studies of suicide predictors
have found in the general population where employment,
marriage and high income seem to predict a lower risk of
suicide [35, 36]. Two other studies examined employment
status among patients with DSH [9, 15] and found no
significant association with suicide; however, both studies
included small numbers of patients dying by suicide
(n \ 61). An explanation of this reverse association
between suicide and high educational level could be that
patients working or highly skilled suddenly find themselves
in a stressful situation (with both a recent DSH episode and
a psychiatric admission) where they suddenly risk losing
their job, and/or the ability to use their education, thereby
putting them at risk of suicide. However, these indications
of reverse associations between social variables and suicide
could also be due to misclassifications, if a patient had lost
a job, income or had changes in marital status in the year of
Fig. 1 a Kaplan–Meier curves illustrating the proportion of suicide
associated to diagnosis. b Kaplan–Meier curves illustrating the
proportion of suicide associated to time of suicide attempt before
psychiatric admission. c Kaplan–Meier curves illustrating the pro-
portion of suicide associated to educational level
Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489 1485
123
Author's personal copy

Table 2 Shows the frequency of suicides and patients, and the association between suicide and covariates in the Cox regression analyses
Characteristics Suicides (n)/patients (n) Hazard ratio (95 % CI)
Univariable Multivariablea Joint analyses
Social covariates
Labor market status
Employed 229/7159 1 1 1
Unemployed 86/3,890 0.68 (0.53–0.87) 0.77 (0.60–0.99) 0.80 (0.62–1.03)
Early retirement 126/4,444 0.88 (0.70–1.09) 0.80 (0.63–1.02) 0.81 (0.63–1.03)
Retired 76/1,633 1.73 (1.34–2.25) 1.05 (0.74–1.51) 1.04 (0.73–1.47)
Unknown 3/131 0.84 (0.27–2.62) 0.97 (0.15–6.09) 1.15 (0.34–3.82)
Gross incomec
Highest quartile 64/1,763 1 1
Third quartile 89/2,375 1.00 (0.72–1.37) 1.01 (0.73–1.40)
Second quartile 111/3,552 0.82 (0.60–1.11) 0.86 (0.63–1.17)
Lowest quartile 253/9,436 0.68 (0.52–0.90) 0.75 (0.56–1.02)
Unknown 3/131 0.69 (0.22–2.20) d
Educationc
Bachelor degree or higher 71/1,475 1 1 1
Vocational training 143/4,328 0.66 (0.50–0.88) 0.64 (0.49–0.85) 0.70 (0.53–0.94)
High school 33/1,082 0.59 (0.39–0.90) 0.86 (0.56–1.31) 0.84 (0.55–1.29)
Primary school 243/9,258 0.51 (0.40–0.67) 0.68 (0.51-0.90) 0.67 (0.51-0.88)
Unknown 30/1,114 0.57 (0.37–0.87) 0.53 (0.34–0.85) 0.56 (0.36–0.89)
Living status
Married/cohabiting 231/6,473 1 1
Living alone/not married 162/6,961 0.65 (0.53–0.79) 0.82 (0.65–1.03)
Divorced 83/2,755 0.85 (0.66–1.09) 0.84 (0.65–1.08)
Widow 39/885 1.38 (0.98–1.94) 1.11 (0.76–1.62)
Other living status 5/183 0.84 (0.35–2.03) 1.05 (0.26–4.24)
Clinical covariates
Admission Diagnosis
Affective diagnosis 161/4,120 1 1 1
Substance abuse 84/3,450 0.59 (0.46–0.77) 0.66 (0.50–0.88) 0.72 (0.54–0.95)
Schizophrenia 75/2,895 0.61 (0.46–0.80) 0.83 (0.61–1.12) 0.85 (0.63–1.15)
Adjustment and stress disorder 93/3,399 0.69 (0.53–0.89) 0.80 (0.62–1.05) 0.85 (0.65–1.10)
Personality disorder 59/1,873 0.74 (0.55–1.00) 1.11 (0.80–1.53) 1.18 (0.86–1.62)
Other 48/1,520 0.83 (0.60–1.14) 0.90 (0.65–1.25) 0.99 (0.71–1.37)
Secondary diagnosis
Substance abuse (No) 428/14,069 1 1
Substance abuse (Yes) 92/3188 0.97 (0.77–1.22) 0.98 (0.78–1.23)
Affective disorder (No) 493/16,552 1 1
Affective disorder (Yes) 27/705 1.40 (0.95–2.06) 1.34 (0.90–2.00)
Personality disorder (No) 493/16150 1 1
Personality disorder (Yes) 27/1,107 0.80 (0.55–1.19) 0.91 (0.62–1.35)
Timing of suicide attempt before admission
Prior to 6 months 31/1,572 1 1 1
31 days to 6 months 63/2,428 1.41 (0.92–2.16) 1.36 (0.89–2.09) 1.35 (0.88–2.09)
8–30 days 49/1,501 1.79 (1.14–2.81) 1.60 (1.02–2.51) 1.59 (1.01–2.50)
Last week 377/11,756 1.75 (1.21.2.52) 1.58 (1.09–2.28) 1.56 (1.08–2.26)
Private psychiatrist
No 443/15,375 1 1 1
1486 Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489
123
Author's personal copy

hospital admission, because we only had information on
social covariates from the year before admission.
Ordinarily, the literature on suicide among psychiatric
patients has found that patients with affective disorders
have a significantly higher risk of suicide compared to
patients with schizophrenia [21, 37]. Yet Tidemalm et al.,
Haukka et al., and our results indicate that the risk of
suicide in patients with DSH who had been hospitalized
with a diagnosis of schizophrenia or unipolar/bipolar dis-
order was similar, thus the type of psychiatric diagnosis as
a predictor of suicide may differ in psychiatric patients
with or without DSH. In sub-analyses, we further tested
whether psychiatric diagnosis (and the other clinically
related covariates) explained more in the cohort of DSH
patients by examining predictors for completed suicide in
the first year after psychiatric admission. These analyses
supported the finding that diagnosis lost impact as a pre-
dictor of suicide in patients who recently self-harmed,
possibly indicating that clinicians should not base suicidal
risk prognosis on specific psychiatric diagnosis. Our results
as well as studies using clinical interviews have estimated
that around 90 % of patients with DSH have a psychiatric
disorder [38, 39], which make it relevant in future studies
to further test the importance of type and severity of psy-
chiatric diagnoses in patients with DSH.
In addition, we also found that contact with a private
psychiatrist appeared to increase the risk. The latter
association could signal that private psychiatrists have
been trained to identify acute suicidal patients and are
accordingly quick to admit them to psychiatric hospital
care; however, we are not able to assess this within our
data.
Patients with a DSH in the month before admission had
a higher risk of suicide during the complete follow-up
period and during the first year after admission. These
patients were most likely in many cases admitted to psy-
chiatric care as they had a present suicidal risk and thereby
a higher risk for completing suicide in the near future,
whereas those with DSH more than 6 months ago had
survived the first period with an elevated suicidal risk after
the DSH episode without receiving psychiatric treatment,
possibly indicating DSH with a lesser degree of suicidal
intent. In essence, our results from a cohort of psychiatric
inpatients with DSH within the last year reflect earlier
studies showing that the risk of completed suicide is
highest in the first period after DSH.
Methodological issues
We had access to data on psychiatric admissions from 1997
to 2006, and as we wanted to ensure that the clinical data
was from the first psychiatric admission after an episode of
DSH, we chose a study period starting from 1998 and to
include only patients with DSH within the last year before
psychiatric admission. Making that choice weakens the
generalizability of our results since it meant that we had to
exclude patients who had an episode of DSH more than a
year before the psychiatric admission, thus our results only
apply to psychiatric inpatients with recent DSH. Adding to
this point, some of the included patients have had earlier
psychiatric admissions. It may have been optimal to follow
only first-time admitted psychiatric patients who recently
self-harmed to avoid studying patients who had survived
the elevated risk of suicide in the first year after first
Table 2 continued
Characteristics Suicides (n)/patients (n) Hazard ratio (95 % CI)
Univariable Multivariablea Joint analyses
Yes 77/1,882 1.44 (1.13–1.83) 1.44 (1.13–1.85) 1.39 (1.09–1.78)
Private psychologist
No 500/16,588 1 1
Yes 20/669 1.03 (0.66–1.60) 1.16 (0.74–1.82)
Psychiatric outpatient
No 435/14,474 1 1
Yes 85/2,783 1.03 (0.82–1.30) 1.07 (0.85–1.36)
No. of psychiatric admission
By increasing admission no. – 0.99 (0.98–1.00) 0.99 (0.98–1.00)
Na not applicablea Adjusted for sex and age group and analyses carried out separately among the social variables and the clinical-related variables, respectivelyc Gross income was not adjusted for educational level to avoid over-adjustment as well as labor market status, educational level and living status
were not adjusted for gross income because income is closely related to thesed Parameter estimate = 0
Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489 1487
123
Author's personal copy

admission [40]. However, since we did not know whether
this association was of importance in our study population
and to avoid compromising our power, we chose instead to
test whether the number of previous psychiatric admissions
significantly predicted suicide and found no significant
difference. Another point to emphasize is, that we only had
access to information on DSH through register-based data,
hence patients who had a less physically harming episode
of DSH is in most cases not registered as this would not
lead to hospitalization. Therefore, the true cohort of psy-
chiatric patients with recent DSH is probably larger in size,
yet we believe our cohort almost certainly includes those at
highest suicidal risk and another point to highlight is that
our defined cohort is identifiable for the clinical staff in the
medical files.
We wanted to examine only patients who died from
subsequent suicide after psychiatric admission, therefore to
ensure exclusion of those who were psychiatrically
admitted due to the DSH episode and died from somatic
consequences that DSH episode, we tested whether the
method of the DSH described in The Danish Patient Reg-
istry was the same as the method of the suicide described in
the Cause of Death register and whether the patients were
somatically admitted from the day of the DSH until the day
they were discharged because of suicide. To estimate the
problem size we checked everyone with DSH in the week
before psychiatric admission who also died during the first
week of admission, leaving us in doubt with seven patients.
If they actually died of the DSH episode before admission
then this will lead to a slight overestimation of the results.
In conclusion, this study demonstrated extremely high
suicide rates in a population of patients with DSH who
within a year also received psychiatric inpatient care and
found that DSH within a month before admission and a
higher level of education increased the risk for completing
suicide, in particular within the first year after admission.
Acknowledgments A fund providing support to the prevention of
suicide and suicide attempt administered by The Ministry of Interior
and Social Affairs in Denmark. The authors report no financial or
other relationship relevant to the subject of this article.
Conflict of interest On behalf of all authors, the corresponding
author states that there is no conflict of interest.
References
1. Harris E, Barraclough B (1997) Suicide as an outcome for mental
disorders. A meta-analysis. Br J Psychiatry 170:205–228
2. Hawton K, van Heeringen K (2009) Suicide. Lancet 373:
1372–1381
3. Iribarren C, Sidney S, Jacobs DR Jr, Weisner C (2000) Hospi-
talization for suicide attempt and completed suicide:
epidemiological features in a managed care population. Soc
Psychiatry Psychiatr Epidemiol 35:288–296
4. Ostamo A, Lonnqvist J (2001) Excess mortality of suicide at-
tempters. Soc Psychiatry Psychiatr Epidemiol 36:29–35
5. Karasouli E, Owens D, Abbott RL, Hurst KM, Dennis M (2011)
All-cause mortality after non-fatal self-poisoning: a cohort study.
Soc Psychiatry Psychiatr Epidemiol 46:455–462
6. Judd F, Jackson H, Komiti A, Bell R, Fraser C (2012) The profile
of suicide: changing or changeable? Soc Psychiatry Psychiatr
Epidemiol 47:1–9
7. Bostwick JM, Pankratz VS (2000) Affective disorders and suicide
risk: a reexamination. Am J Psychiatry 157:1925–1932
8. Nordentoft M, Mortensen PB, Pedersen CB (2011) Absolute risk
of suicide following first hospital contact with mental disorder.
Arch Gen Psychiatry 68(10):1058–1064
9. Cooper J, Kapur N, Webb R, Lawlor M, Guthrie E, kway-Jones
K, Appleby L (2005) Suicide after deliberate self-harm: a 4-year
cohort study. Am J Psychiatry 162:297–303
10. Qin P, Jepsen P, Norgard B, Agerbo E, Mortensen PB, Vilstrup
H, Sorensen HT (2009) Hospital admission for non-fatal poi-
soning with weak analgesics and risk for subsequent suicide: a
population study. Psychol Med 39:1867–1873
11. Haukka J, Suominen K, Partonen T, Lonnqvist J (2008) Deter-
minants and outcomes of serious attempted suicide: a nationwide
study in Finland, 1996–2003. Am J Epidemiol 167:1155–1163
12. Runeson B, Tidemalm D, Dahlin M, Lichtenstein P, Langstrom N
(2010) Method of attempted suicide as predictor of subsequent
successful suicide: national long term cohort study. BMJ 341:
c3222
13. Tidemalm D, Langstrom N, Lichtenstein P, Runeson B (2008)
Risk of suicide after suicide attempt according to coexisting
psychiatric disorder: Swedish cohort study with long term follow-
up. BMJ 337:a2205
14. Hawton K, Zahl D, Weatherall R (2003) Suicide following
deliberate self-harm: long-term follow-up of patients who pre-
sented to a general hospital. Br J Psychiatry 182:537–542
15. de Moore GM, Robertson AR (1996) Suicide in the 18 years after
deliberate self-harm a prospective study. Br J Psychiatry 169:
489–494
16. Suominen K, Isometsa E, Suokas J, Haukka J, Achte K, Lonnq-
vist J (2004) Completed suicide after a suicide attempt: a 37-year
follow-up study. Am J Psychiatry 161:562–563
17. Owens D, Wood C, Greenwood DC, Hughes T, Dennis M (2005)
Mortality and suicide after non-fatal self-poisoning: 16-year
outcome study. Br J Psychiatry 187:470–475
18. Jenkins GR, Hale R, Papanastassiou M, Crawford MJ, Tyrer P
(2002) Suicide rate 22 years after parasuicide: cohort study. BMJ
325:1155
19. Nordentoft M, Breum L, Munck LK, Nordestgaard AG, Hunding
A, Laursen Bjaeldager PA (1993) High mortality by natural and
unnatural causes: a 10 year follow up study of patients admitted
to a poisoning treatment centre after suicide attempts. BMJ
306:1637–1641
20. Nordentoft M (2007) Prevention of suicide and attempted suicide
in Denmark. Epidemiological studies of suicide and intervention
studies in selected risk groups, Lægeforeningens Forlag, Copen-
hagen, Denmark
21. Madsen T, Agerbo E, Mortensen PB, Nordentoft M (2011) Pre-
dictors of psychiatric inpatient suicide: a national prospective
register-based study. J Clin Psychiatry 73:144–451
22. Munk-Jorgensen P, Mortensen PB (1997) The Danish Psychiatric
Central Register. Dan Med Bull 44(1):82–84
23. Pedersen CB, Gotzsche H, Moller JO, Mortensen PB (2006) The
Danish Civil Registration System. A cohort of eight million
persons. Dan Med Bull 53:441–449
1488 Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489
123
Author's personal copy

24. Andersen TF, Madsen M, Jorgensen J, Mellemkjaer L, Olsen JH
(1999) The Danish National Hospital Register. A valuable source
of data for modern health sciences. Dan Med Bull 46:263–268
25. Olivarius ND, Hollnagel H, Krasnik A, Pedersen PA, Thorsen H
(1997) The Danish National Health Service Register. A tool for
primary health care research. Dan Med Bull 44:449–453
26. Statistik Danmarks (1991) IDA: An Integrated database for
Labour Market Research. Danmarks Statistik Printing (in Dan-
ish), Copenhagen Ref Type: Report
27. Juel K, Helweg-Larsen K (1999) The Danish registers of causes
of death. Dan Med Bull 46:354–357
28. World Health Organization (1992) International Statistical Clas-
sification of Diseases, 10th Revision (ICD-10). World Health
Organization, Geneva
29. Helweg-Larsen K (2005) Suicide in Denmark. National Institute
of Public Health (publication in Danish), Denmark
30. Kleinbaum D, Klein M (2005) Survival analysis—a self-learning
text. Springer Science ? Business Media, NewYork
31. Owens D, Horrocks J, House A (2002) Fatal and non-fatal rep-
etition of self-harm. Systematic review. Br J Psychiatry
181:193–199
32. Holley H, Fick G, Love E (1998) Suicide following an inpatient
hospitalization for a suicide attempt: a Canadian follow-up study.
Soc Psychiatry Psychiatr Epidemiol 33:543–551
33. Agerbo E (2007) High income, employment, postgraduate edu-
cation, and marriage: a suicidal cocktail among psychiatric
patients. Arch Gen Psychiatry 64:1377–1384
34. Hunt IM, Kapur N, Webb R, Robinson J, Burns J, Turnbull P,
Shaw J, Appleby L (2007) Suicide in current psychiatric in-
patients: a case-control study The National Confidential Inquiry
into Suicide and Homicide. Psychol Med 37:831–837
35. Qin P, Agerbo E, Mortensen PB (2003) Suicide risk in relation to
socioeconomic, demographic, psychiatric, and familial factors: a
national register-based study of all suicides in Denmark,
1981–1997. Am J Psychiatry 160:765–772
36. McLean J, Maxwell M, Platt S, Harris F, Jepson R (2008) Risk
and Protective factors for Suicide and Suicidal behaviour: A
Literature Review. Scottish Government Social Research,
Scotland
37. Qin P, Nordentoft M (2005) Suicide risk in relation to psychiatric
hospitalization: evidence based on longitudinal registers. Arch
Gen Psychiatry 62:427–432
38. Beautrais AL, Joyce PR, Mulder RT, Fergusson DM, Deavoll BJ,
Nightingale SK (1996) Prevalence and comorbidity of mental
disorders in persons making serious suicide attempts: a case-
control study. Am J Psychiatry 153:1009–1014
39. Haw C, Hawton K, Houston K, Townsend E (2001) Psychiatric
and personality disorders in deliberate self-harm patients. Br J
Psychiatry 178:48–54
40. Nordentoft M, Laursen TM, Agerbo E, Qin P, Hoyer EH, Mor-
tensen PB (2004) Change in suicide rates for patients with
schizophrenia in Denmark, 1981–97: nested case-control study.
BMJ 329:261
Soc Psychiatry Psychiatr Epidemiol (2013) 48:1481–1489 1489
123
Author's personal copy
Related Documents











