CLINICAL—ALIMENTARY TRACT Delayed-Release Oral Mesalamine 4.8 g/day (800-mg Tablet) Is Effective for Patients With Moderately Active Ulcerative Colitis WILLIAM J. SANDBORN,* JAROSLAW REGULA, ‡ BRIAN G. FEAGAN, § ELENA BELOUSOVA, NJEGICA JOJIC, ¶ MILAN LUKAS, # BRUCE YACYSHYN,** PIOTR KRZESKI, ‡‡ CHYON–HWA YEH, §§ CHRISTI A. MESSER, §§ and STEPHEN B. HANAUER *Inflammatory Bowel Disease Clinic, Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota; ‡ Medical Center for Postgraduate Education and the Maria Sklodowska-Curie Memorial Cancer Center, Warsaw, Poland; § Robarts Research Institute, University of Western Ontario, London, Ontario, Canada; Moscow Regional Research Clinical Institute, Moscow, Russian Federation; ¶ KBC Zvezdara University Centre, Belgrade, Serbia; # General Faculty Hospital, Prague, Czech Republic; **University of Cincinnati, Cincinnati, Ohio; ‡‡ Procter & Gamble Pharmaceuticals, Inc, Egham, United Kingdom; §§ Procter & Gamble Pharmaceuticals, Inc, Mason, Ohio; University of Chicago, Chicago, Illinois This article has an accompanying continuing medical education activity on page 2158. Learning Objective: Upon completion of reading this article, successful learners will be able to apply the results of the study to their practice by weighing the potential benefits of mesalamine dosed at 2.4 or 4.8 g/d in individual patients with moderate ulcerative colitis. See related article, Calvet X et al, on page 1322 in CGH; see editorial on page 1880. BACKGROUND AND AIMS: It is not clear what induc- tion dose of mesalamine is optimal for treating patients with mildly and moderately active ulcerative colitis (UC). This study was conducted to determine the efficacy and safety of mesalamine 4.8 g/day compared with 2.4 g/day for the treatment of moderately active UC. METHODS: A multicenter, randomized, double-blind, 6-week, active-con- trol study (ASCEND III) was conducted to assess the non- inferiority of delayed-release mesalamine 4.8 g/day (Asacol HD, 800-mg tablet; Procter & Gamble, Pharmaceuticals, Inc, Mason, Ohio) with 2.4 g/day (Asacol, 400-mg tablet; Procter & Gamble Pharmaceuticals, Inc) in 772 patients with moderately active UC. The primary endpoint was treat- ment success (overall improvement) at week 6, defined as improvement in the Physician’s Global Assessment (based on clinical assessments of rectal bleeding, stool frequency, and sigmoidoscopy), with no worsening in any individual clinical assessment. RESULTS: The primary objective of noninferiority was met. Seventy percent (273 of 389) of patients who received 4.8 g/day of mesalamine achieved treatment success at week 6, compared with 66% (251 of 383) of patients receiving 2.4 g/day (95% confidence interval for 2.4 g/day minus 4.8 g/day, 11.2 to 1.9). In addition, 43% of patients who received 4.8 g/day mesalamine achieved clinical remission at week 6 compared with 35% of patients who received 2.4 g/day (P .04). A therapeutic advantage for the 4.8 g/day dose was observed among patients previ- ously treated with corticosteroids, oral mesalamines, rectal therapies, or multiple UC medications. Both regimens were well-tolerated with similar adverse events. CONCLU- SIONS: Delayed-release mesalamine 4.8 g/day (800-mg tablet) is efficacious and well-tolerated in patients with moderately active UC. M edications that deliver 5-aminosalicylate (me- salamine) as the active moiety are effective for induction and maintenance treatment in patients with mildly and moderately active ulcerative colitis (UC). 1,2 Based on favorable efficacy and safety profiles, mesalamine and its derivatives are recommended in multiple national treatment guidelines as first-line therapy for UC. 3-5 Never- theless, the dose-response of mesalamine in patients with active UC remains uncertain. The first drug used to deliver mesalamine was sulfasalazine, a pro-drug com- prised of sulfapyridine linked to mesalamine by an azo- bond, which contained 40% mesalamine. Early clinical trials demonstrated that induction therapy with sul- fasalazine was limited to doses of 46 g/day (contains 1.62.4 g/day mesalamine) because of side effects from sulfapyridine. 6,7 In order to reduce the side effects of sulfasalazine, new sulfa-free formulations were developed that delivered mesalamine directly to the distal small bowel and colon. 8 Two placebo-controlled dose-ranging trials were performed with delayed-release mesalamine (Asacol, 400-mg tablet; Procter & Gamble Pharmaceuti- cals, Inc, Mason, Ohio) at doses of 1.64.8 g/day. 9,10 In the first trial, delayed-release mesalamine 4.8 g/day (400-mg tablet) was superior to placebo and 1.6 g/day. 9 Abbreviations used in this paper: AE, adverse event; CFT, contact friability test; ITT, intent-to-treat; PFA, Patient’s Functional Assess- ment; PGA, Physician’s Global Assessment; UC, ulcerative colitis; UCDAI, xxx. © 2009 by the AGA Institute 0016-5085/09/$36.00 doi:10.1053/j.gastro.2009.08.069 CLINICAL– ALIMENTARY TRACT GASTROENTEROLOGY 2009;137:1934 –1943

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

C
Df
WMS
*a�
CP
Top
BtwTstmtiHIPwmioacnpt3f4cwfotwS
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
GASTROENTEROLOGY 2009;137:1934–1943
LINICAL—ALIMENTARY TRACT
elayed-Release Oral Mesalamine 4.8 g/day (800-mg Tablet) Is Effectiveor Patients With Moderately Active Ulcerative Colitis
ILLIAM J. SANDBORN,* JAROSLAW REGULA,‡ BRIAN G. FEAGAN,§ ELENA BELOUSOVA,� NJEGICA JOJIC,¶
ILAN LUKAS,# BRUCE YACYSHYN,** PIOTR KRZESKI,‡‡ CHYON–HWA YEH,§§ CHRISTI A. MESSER,§§ andTEPHEN B. HANAUER� �
Inflammatory Bowel Disease Clinic, Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota; ‡Medical Center for Postgraduate Educationnd the Maria Sklodowska-Curie Memorial Cancer Center, Warsaw, Poland; §Robarts Research Institute, University of Western Ontario, London, Ontario, Canada;Moscow Regional Research Clinical Institute, Moscow, Russian Federation; ¶KBC Zvezdara University Centre, Belgrade, Serbia; #General Faculty Hospital, Prague,zech Republic; **University of Cincinnati, Cincinnati, Ohio; ‡‡Procter & Gamble Pharmaceuticals, Inc, Egham, United Kingdom; §§Procter & Gambleharmaceuticals, Inc, Mason, Ohio; � �University of Chicago, Chicago, Illinois
his article has an accompanying continuing medical education activity on page 2158. Learning Objective: Upon completionf reading this article, successful learners will be able to apply the results of the study to their practice by weighing the
otential benefits of mesalamine dosed at 2.4 or 4.8 g/d in individual patients with moderate ulcerative colitis.tm
MimBattadpbtf1sstbt(ct(
fmU
See related article, Calvet X et al, on page1322 in CGH; see editorial on page 1880.
ACKGROUND AND AIMS: It is not clear what induc-ion dose of mesalamine is optimal for treating patientsith mildly and moderately active ulcerative colitis (UC).his study was conducted to determine the efficacy and
afety of mesalamine 4.8 g/day compared with 2.4 g/day forhe treatment of moderately active UC. METHODS: A
ulticenter, randomized, double-blind, 6-week, active-con-rol study (ASCEND III) was conducted to assess the non-nferiority of delayed-release mesalamine 4.8 g/day (Asacol
D, 800-mg tablet; Procter & Gamble, Pharmaceuticals,nc, Mason, Ohio) with 2.4 g/day (Asacol, 400-mg tablet;rocter & Gamble Pharmaceuticals, Inc) in 772 patientsith moderately active UC. The primary endpoint was treat-ent success (overall improvement) at week 6, defined as
mprovement in the Physician’s Global Assessment (basedn clinical assessments of rectal bleeding, stool frequency,nd sigmoidoscopy), with no worsening in any individuallinical assessment. RESULTS: The primary objective ofoninferiority was met. Seventy percent (273 of 389) ofatients who received 4.8 g/day of mesalamine achievedreatment success at week 6, compared with 66% (251 of83) of patients receiving 2.4 g/day (95% confidence intervalor 2.4 g/day minus 4.8 g/day, �11.2 to 1.9). In addition,3% of patients who received 4.8 g/day mesalamine achievedlinical remission at week 6 compared with 35% of patientsho received 2.4 g/day (P � .04). A therapeutic advantage
or the 4.8 g/day dose was observed among patients previ-usly treated with corticosteroids, oral mesalamines, rectalherapies, or multiple UC medications. Both regimens wereell-tolerated with similar adverse events. CONCLU-
IONS: Delayed-release mesalamine 4.8 g/day (800-mgablet) is efficacious and well-tolerated in patients withoderately active UC.
edications that deliver 5-aminosalicylate (me-salamine) as the active moiety are effective for
nduction and maintenance treatment in patients withildly and moderately active ulcerative colitis (UC).1,2
ased on favorable efficacy and safety profiles, mesalaminend its derivatives are recommended in multiple nationalreatment guidelines as first-line therapy for UC.3-5 Never-heless, the dose-response of mesalamine in patients withctive UC remains uncertain. The first drug used toeliver mesalamine was sulfasalazine, a pro-drug com-rised of sulfapyridine linked to mesalamine by an azo-ond, which contained 40% mesalamine. Early clinicalrials demonstrated that induction therapy with sul-asalazine was limited to doses of 4�6 g/day (contains.6�2.4 g/day mesalamine) because of side effects fromulfapyridine.6,7 In order to reduce the side effects ofulfasalazine, new sulfa-free formulations were developedhat delivered mesalamine directly to the distal smallowel and colon.8 Two placebo-controlled dose-rangingrials were performed with delayed-release mesalamineAsacol, 400-mg tablet; Procter & Gamble Pharmaceuti-als, Inc, Mason, Ohio) at doses of 1.6�4.8 g/day.9,10 Inhe first trial, delayed-release mesalamine 4.8 g/day400-mg tablet) was superior to placebo and 1.6 g/day.9
Abbreviations used in this paper: AE, adverse event; CFT, contactriability test; ITT, intent-to-treat; PFA, Patient’s Functional Assess-ent; PGA, Physician’s Global Assessment; UC, ulcerative colitis;CDAI, xxx.
© 2009 by the AGA Institute0016-5085/09/$36.00
doi:10.1053/j.gastro.2009.08.069

I1(odwrfp4stC84Sgm5mwgd7a.amApmptop
6tlmm
bsRRUtBp
tUa
csabtatstohnshipwidtlm(miocrmdPs
ttottatmai
tgsGlwtrSs
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
December 2009 DELAYED-RELEASE MESALAMINE UC THERAPY 1935
n the second trial, delayed-release mesalamine doses of.6 g/day and 2.4 g/day were both superior to placebowith only a slight nonsignificant advantage for 2.4 g/dayver 1.6 g/day).10 Results of these trials indicated thatelayed-release mesalamine doses of 2.4 and 4.8 g/dayere consistently more effective than 1.6 g/day and led to
egulatory (US Food and Drug Administration) approvalor induction therapy at the 2.4 g/day dose, but did notrovide information regarding the relative efficacy of a.8 g/day dose to 2.4 g/day. Subsequent dose-rangingtudies have been conducted to further explore this ques-ion.11,12 The ASCEND I trial (Assessing the Safety andlinical Efficacy of a New Dose of 5-ASA [4.8 g/day,00-mg tablet]) compared delayed-release mesalamine.8 g/day (800-mg tablet, sold as Asacol HD in the Unitedtates; Procter & Gamble Pharmaceuticals, Inc) with 2.4/day (Asacol, 400-mg tablet) in patients with mildly tooderately active UC.11 Treatment success occurred in
6% of patients (76 of 136) who received delayed-releaseesalamine 4.8g/day and 51% of patients (77 of 150)ho received 2.4 g/day (P � .441). A prespecified sub-roup analysis of 169 patients with moderately active UCemonstrated treatment success in 72% of patients (55 of6) treated with delayed-release mesalamine 4.8 g/daynd 57% (53 of 93) of patients treated with 2.4 g/day (P �
038). When results of the ASCEND I trial became avail-ble, a second trial, ASCEND II, was still in the recruit-ent phase. The protocol for the ongoing blinded
SCEND II trial was amended to limit the entry criteria toatients with moderately active UC. Only patients withoderate disease were included in the analysis for the
rimary endpoint, and the sample size of moderate pa-ients was increased.12 Treatment success occurred in 72%f patients (89 of 124) treated with 4.8 g/day and 59% ofatients (77 of 130) treated with 2.4 g/day (P � .036).Here we present results of the ASCEND III trial, a
-week noninferiority study designed to demonstratehat delayed-release mesalamine 4.8 g/day (800-mg tab-et) is effective and safe as compared with delayed-release
esalamine 2.4 g/day (400-mg tablet) in patients withoderately active UC.
Materials and MethodsPatientsThis multicenter, randomized, double-blind, dou-
le-dummy, active-controlled trial was conducted at 113ites in 14 countries (Belarus, Canada, Croatia, Czechepublic, Estonia, Hungary, Latvia, Lithuania, Poland,omania, Russian Federation, Serbia and Montenegro,kraine, and United States [including Puerto Rico]) be-
ween July 2006 and June 2007. The Institutional Reviewoard or Ethics Committee at each site approved therotocol, and all patients gave written informed consent.Criteria for eligibility were male or female patients 18
o 75 years of age with a diagnosis of moderately activeC that extended proximally beyond 15 cm from the
nal verge, as confirmed by flexible sigmoidoscopy or e
olonoscopy. Moderately active UC was defined as a Phy-ician’s Global Assessment (PGA) equal to 2 points, withscore of �1 point in both the stool frequency and rectalleeding clinical assessments and a score of �2 points inhe sigmoidoscopy assessment with a positive friabilityssessment. Patients were excluded from study participa-ion if they had UC confined to the rectum, short bowelyndrome, renal or hepatic disease, or a stool examina-ion positive for Clostridium difficile, bacterial pathogens,r ova and parasites. Additional exclusion criteria were aistory of allergy or hypersensitivity to salicylates, ami-osalicylates, or any component of the delayed-release me-alamine tablets, a history of HIV infection or AIDS, or aistory of alcohol or drug abuse. Patients were also excluded
f they had received an oral 5-aminosalicylate�containingroduct at a dose �1.6 g/day of mesalamine by any routeithin the last 7 days; taken any corticosteroids (oral,
ntravenous, intramuscular, or rectal) within the last 30ays; taken immunosuppressive drugs (including aza-hioprine, 6-mercaptopurine, methotrexate) within theast 90 days; received any antidiarrheal and/or antispas-
odic drugs within the previous 3 days; received aspirinexcept for cardioprotective indications up to a maxi-
um dose of 325 mg/day) or other nonsteroidal anti-nflammatory drugs within the last 7 days; used antibi-tics (other than topical antibiotics) or any productontaining omega-3 fatty acids within the last 7 days;eceived infliximab, adalimumab, or other biologic treat-
ent of UC within the last 90 days; or participated in anyrug or device clinical study within the last 30 days.regnant and/or lactating women were excluded fromtudy participation.
Following randomization, patients were prohibited fromaking aspirin (for any indication other than cardioprotec-ion, where the maximum allowed dose was 325 mg/day) orther nonsteroidal anti-inflammatory drugs; other medica-ions containing 5-aminosalicylate as the active moiety; cor-icosteroids; immunomodulatory agents; metronidazole;ntibiotics (other than topical antibiotics) for �10 dayshroughout the study; antidiarrheal and/or antispasmodic
edications; and any products containing omega-3 fattycids or any investigational or marketed drug that mightnterfere with the evaluation of the study medication.
Study DesignEligible patients were randomized (in a 1:1 ratio)
o receive either oral delayed-release mesalamine 2.4/day (Asacol, 400-mg tablet) or delayed-release me-alamine 4.8 g/day (Asacol HD, 800-mg tablet; Procter &amble Pharmaceuticals, Inc) for 6 weeks. The study was
ocally randomized at each site, and treatment allocationas stratified by gender. A double-blind, double-dummy
rial design was utilized. The investigator or designatedepresentative telephoned the Interactive Voice Responseystem for patient randomization and allocation oftudy medication once the patient was determined to be
ligible for the study. The treatment each patient received
wsdbr2ittl
(dsasaimwtasrsStfamtcbsfwerwccsCamc
rtsclcd
aCotafaa
mpitm
ticmtmTrwpwtwbpUp
dscticgU2dapdns1sdwlt
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1936 SANDBORN ET AL GASTROENTEROLOGY Vol. 137, No. 6
as not disclosed to the investigator, study-center per-onnel, patients, contracted monitors, contracted ven-ors, or the sponsor (except for selected clinical supplies,ioanalytical, or pharmacovigilance personnel). Patientsandomized to 2.4 g/day received two 400-mg tablets and
placebo tablets 3 times daily (placebo tablets weredentical in appearance to the 800-mg tablets), and pa-ients randomized to 4.8 g/day received two 800-mgablets and 2 placebo tablets 3 times daily (placebo tab-ets were identical in appearance to the 400-mg tablets).
Patient Schedule and Efficacy/SafetyEvaluationsPatients were assessed at screening and weeks 0
baseline), 3, and 6. PGA score was used for assessment ofisease severity and efficacy. Components of the PGAcoring system included stool frequency, rectal bleeding,nd sigmoidoscopy with contact friability test (CFT) as-essments (see Supplementary Table 1). Stool frequencynd rectal bleeding were rated on a scale from 0 to 3,ndicating normal to severe activity. These clinical assess-
ents were completed by the investigator at visits ateeks 0, 3, and 6 and were based on the patient’s recall of
hese symptoms during the previous 3 days. A novelpproach to sigmoidoscopy assessment was used in thistudy that featured review of digital images by a centraleader. Sigmoidoscopic disease activity was rated on acale from 0 to 3, indicating normal to severe activity (seeupplementary Table 2). The sigmoidoscopy scoring sys-em was modified from previous studies9 –12 to excluderiability from the definition of a score of 1 (mild). Inddition, the sigmoidoscopy assessment was furtherodified to include a CFT, where investigators touched
he most severely affected area of the sigmoid colon withlosed biopsy forceps.13 Results of this mandatory fria-ility test were incorporated into the sigmoidoscopycore, which was required to be a score of 2 if theriability test was positive. The sigmoidoscopy with CFTas performed in all patients at baseline and week 6 or
xit from the study. All sigmoidoscopy procedures wereecorded on videotape and reviewed by a central readerho was blinded to treatment group to monitor for
onsistency. Investigators were made aware of any dis-repancies between their score and the central reader’score. Investigator’s assessment of sigmoidoscopy withFT was used for assessment of the primary and second-ry endpoints of the study. The PGA score was deter-ined based on the assessment scores and investigator’s
linical judgment at weeks 0 and 6.Treatment success was defined as either a complete
esponse (remission) or a partial response (improvement)o treatment from baseline at week 6. A complete re-ponse was defined as PGA score equal to 0 points (ie,omplete resolution or normalization of all of the fol-owing: stool frequency, rectal bleeding, and sigmoidos-opy with CFT Assessment Score). A partial response was
efined as improvement from baseline in the PGA score lnd no worsening in any of the 3 component scores.linical remission was defined as a stool frequency scoref 0 and a rectal bleeding score of 0. The Patient’s Func-ional Assessment (PFA) was assessed at weeks 0, 3, and 6nd was rated on a scale of 0�3 indicating normalunction to severe impairment. The Mayo score (Ulcer-tive Colitis Disease Activity Index [UCDAI] score)9 waslso calculated at weeks 0 and 6.
At each visit, adverse events (AEs) and concomitantedications were recorded. Safety evaluations included
hysical examinations and serum creatinine. Differencesn creatinine levels from screening to week 6 and be-ween treatment groups were evaluated using graphical
ethods.
Statistical AnalysisThe primary endpoint was treatment success (par-
ial response plus complete response) at week 6 in thentent-to-treat (ITT) population. The ITT population in-luded all patients who were randomized and took 1 orore doses of study medication. For patients whose
reatment outcomes were missing at week 6, their treat-ent outcomes at week 6 were set to treatment failure.wo sensitivity analyses were performed to assess the
obustness of the primary efficacy result: (1) ITT patientsith a known week-6 treatment outcome and (2) per-rotocol analysis, which included all patients who had aeek-6 treatment outcome and no major protocol viola-
ions. Secondary endpoints included clinical remission ateeks 3 and 6; improvement in stool frequency, rectalleeding, and PFA assessments at weeks 3 and 6; im-rovement in the sigmoidoscopy with CFT, PGA, andCDAI assessments at week 6; and treatment success inatients with left-sided disease at week 6.The study was initially designed to determine whether
elayed-release mesalamine 4.8 g/day (800-mg tablet) wasuperior to 2.4 g/day (400-mg tablet) for treatment suc-ess at week 6 with a sample size of 470 patients. Whilehe ASCEND III study was still blinded and still recruit-ng, another delayed-release mesalamine formulation re-eived regulatory approval for both 2.4 g/day and 4.8/day for the treatment of mildly to moderately activeC, despite the absence of a dose-response between the.4 g/day and 4.8 g/day doses.14-16 The ASCEND III studyesign was amended (while the study was still blindednd recruiting) to a noninferiority design. The amendedrimary efficacy analysis was designed to assess whetherelayed-release mesalamine 4.8 g/day (800-mg tablet) wasoninferior to 2.4 g/day (400-mg tablet) for treatmentuccess at week 6. The noninferiority margin was set at0% with a one-sided hypothesis test at � � .025 level ofignificance. A two-sided 95% confidence interval for theifference between the 2.4 g/day and the 4.8 g/day groupsas computed. Noninferiority of 4.8 g/day was estab-
ished if the upper boundary of the 95% confidence in-erval was �10%. In addition, if noninferiority was estab-
ished between 4.8 g/day and 2.4 g/day, then superiority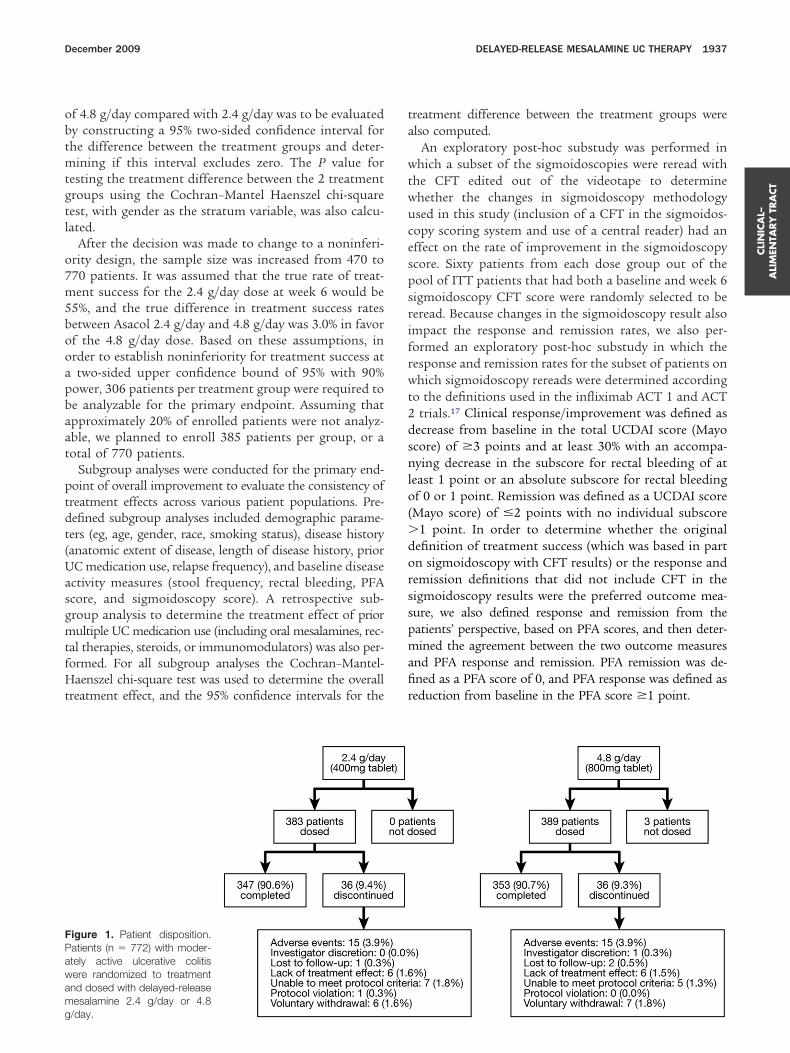
obtmtgtl
o7m5booapbaat
ptdt(UasgmtfHt
ta
wtwucespsrifrwt2dsnlo(�dorsspmafir
FPawamg
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
December 2009 DELAYED-RELEASE MESALAMINE UC THERAPY 1937
f 4.8 g/day compared with 2.4 g/day was to be evaluatedy constructing a 95% two-sided confidence interval forhe difference between the treatment groups and deter-
ining if this interval excludes zero. The P value foresting the treatment difference between the 2 treatmentroups using the Cochran–Mantel Haenszel chi-squareest, with gender as the stratum variable, was also calcu-ated.
After the decision was made to change to a noninferi-rity design, the sample size was increased from 470 to70 patients. It was assumed that the true rate of treat-ent success for the 2.4 g/day dose at week 6 would be
5%, and the true difference in treatment success ratesetween Asacol 2.4 g/day and 4.8 g/day was 3.0% in favorf the 4.8 g/day dose. Based on these assumptions, inrder to establish noninferiority for treatment success attwo-sided upper confidence bound of 95% with 90%
ower, 306 patients per treatment group were required toe analyzable for the primary endpoint. Assuming thatpproximately 20% of enrolled patients were not analyz-ble, we planned to enroll 385 patients per group, or aotal of 770 patients.
Subgroup analyses were conducted for the primary end-oint of overall improvement to evaluate the consistency ofreatment effects across various patient populations. Pre-efined subgroup analyses included demographic parame-ers (eg, age, gender, race, smoking status), disease historyanatomic extent of disease, length of disease history, priorC medication use, relapse frequency), and baseline disease
ctivity measures (stool frequency, rectal bleeding, PFAcore, and sigmoidoscopy score). A retrospective sub-roup analysis to determine the treatment effect of priorultiple UC medication use (including oral mesalamines, rec-
al therapies, steroids, or immunomodulators) was also per-ormed. For all subgroup analyses the Cochran–Mantel-aenszel chi-square test was used to determine the overall
reatment effect, and the 95% confidence intervals for the
igure 1. Patient disposition.atients (n � 772) with moder-tely active ulcerative colitisere randomized to treatmentnd dosed with delayed-releaseesalamine 2.4 g/day or 4.8
/day.reatment difference between the treatment groups werelso computed.
An exploratory post-hoc substudy was performed inhich a subset of the sigmoidoscopies were reread with
he CFT edited out of the videotape to determinehether the changes in sigmoidoscopy methodologysed in this study (inclusion of a CFT in the sigmoidos-opy scoring system and use of a central reader) had anffect on the rate of improvement in the sigmoidoscopycore. Sixty patients from each dose group out of theool of ITT patients that had both a baseline and week 6igmoidoscopy CFT score were randomly selected to beeread. Because changes in the sigmoidoscopy result alsompact the response and remission rates, we also per-ormed an exploratory post-hoc substudy in which theesponse and remission rates for the subset of patients onhich sigmoidoscopy rereads were determined according
o the definitions used in the infliximab ACT 1 and ACTtrials.17 Clinical response/improvement was defined as
ecrease from baseline in the total UCDAI score (Mayocore) of �3 points and at least 30% with an accompa-ying decrease in the subscore for rectal bleeding of at
east 1 point or an absolute subscore for rectal bleedingf 0 or 1 point. Remission was defined as a UCDAI scoreMayo score) of �2 points with no individual subscore
1 point. In order to determine whether the originalefinition of treatment success (which was based in partn sigmoidoscopy with CFT results) or the response andemission definitions that did not include CFT in theigmoidoscopy results were the preferred outcome mea-ure, we also defined response and remission from theatients’ perspective, based on PFA scores, and then deter-ined the agreement between the two outcome measures
nd PFA response and remission. PFA remission was de-ned as a PFA score of 0, and PFA response was defined aseduction from baseline in the PFA score �1 point.

dgpi
Alt3C
�2Rps
Fntamdfabagr6m
T
M
G
R
S
D
L
P
R
M
5D
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1938 SANDBORN ET AL GASTROENTEROLOGY Vol. 137, No. 6
ResultsCharacteristics and Disposition of the PatientsSeven-hundred and seventy-two patients were ran-
omized to treatment and dosed (2.4 g/day, n � 383; 4.8/day, n � 389). A summary of patient disposition isrovided in Figure 1. Baseline characteristics were similar
n the 2 treatment groups (Table 1).
EfficacyThe primary objective of noninferiority was met.
t week 6, 70.2% (273 of 389) of patients receiving de-ayed-release mesalamine 4.8 g/day (800-mg tablet) achievedreatment success at week 6, compared with 65.5% (251 of83) of those who received 2.4 g/day (400-mg tablet) (95%
able 1. Baseline Characteristics of Patients with ModerateUlcerative Colitis
Parameter
Mesalamine treatment groups
2.4 g/day(n � 383)
4.8 g/day(n � 389)
n % n %
ean age (y) 42.4 44.1�65 years 355 92.7 355 91.3�65 years 28 7.3 34 8.7
enderMale 216 56.4 217 55.8Female 167 43.6 172 44.2
aceCaucasian 368 96.1 378 97.2African American 6 1.6 3 0.8Other 9 2.3 8 2.1
moking historyCurrent nonsmoker 342 89.3 352 90.5Currently smokes 41 10.7 37 9.5
isease extent at baselineProctosigmoiditis 183 48.3 185 48.2Left-sided colitis 136 35.9 138 35.9Pancolitis 60 15.8 61 15.9
ength of disease history�1 y 111 29.0 98 25.21 to 5 y 131 34.2 148 38.0�5 to 10 y 72 18.8 82 21.1�10 y 69 18.0 61 15.7
rior treatmentSteroids (oral or IV) 157 41.0 157 40.4Immunomodulators 17 4.4 16 4.1Any oral 5-ASA 323 84.3 338 86.9Rectal therapies 188 49.1 192 49.4
elapse frequencyNewly diagnosed 76 19.8 69 17.7More than once a month 21 5.5 12 3.1Once every 6 months 108 28.2 121 31.1Once every 6�12 months 122 31.9 118 30.3Less than once a year 56 14.6 69 17.7ean UCDAI (standard
deviation)7.8 (0.68) 7.8 (0.68)
-ASA, 5-aminosalicylic acid; IV, intravenous; UCDAI, Ulcerative Colitisisease Activity Index.
I for 2.4 g/day minus 4.8 g/day treatment success rates, c
11.2 to 1.9) (Figure 2A). The comparison of 4.8 g/day to.4 g/day for superiority was not significant (P � .17).esults of the sensitivity analyses (analyzable and perrotocol) were consistent with these results (data nothown).
igure 2. (A) Treatment success at week 6. The 4.8 g/day dose wasoninferior to delayed-release mesalamine 2.4 g/day for the endpoint ofreatment success (overall improvement). Treatment success was defineds either a complete response (remission) or a partial response (improve-ent) to treatment from baseline at week 6. A complete response wasefined as complete resolution or normalization of all of the following: stool
requency, rectal bleeding, and sigmoidoscopy with contact friability testssessment score. A partial response was defined as improvement fromaseline in the Physician’s Global Assessment score and no worsening inny of the 3 component scores. The complete response rates in the 4.8/day and 2.4 g/day groups were 2.6% and 5.0%, respectively. The partialesponse rates in the 4.8 g/day and 2.4 g/day groups were 67.6% and0.6%, respectively. (B) Clinical remission at weeks 3 and 6. Significantlyore patients who received 4.8 g/day compared to 2.4 g/day achieved
linical remission at week 3 (P � .02) and week 6 (P � .04).
p.fb3nwasrfbghn
tiwcg
gadpmm
srA
Fvwtci(mh2Pbs
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
December 2009 DELAYED-RELEASE MESALAMINE UC THERAPY 1939
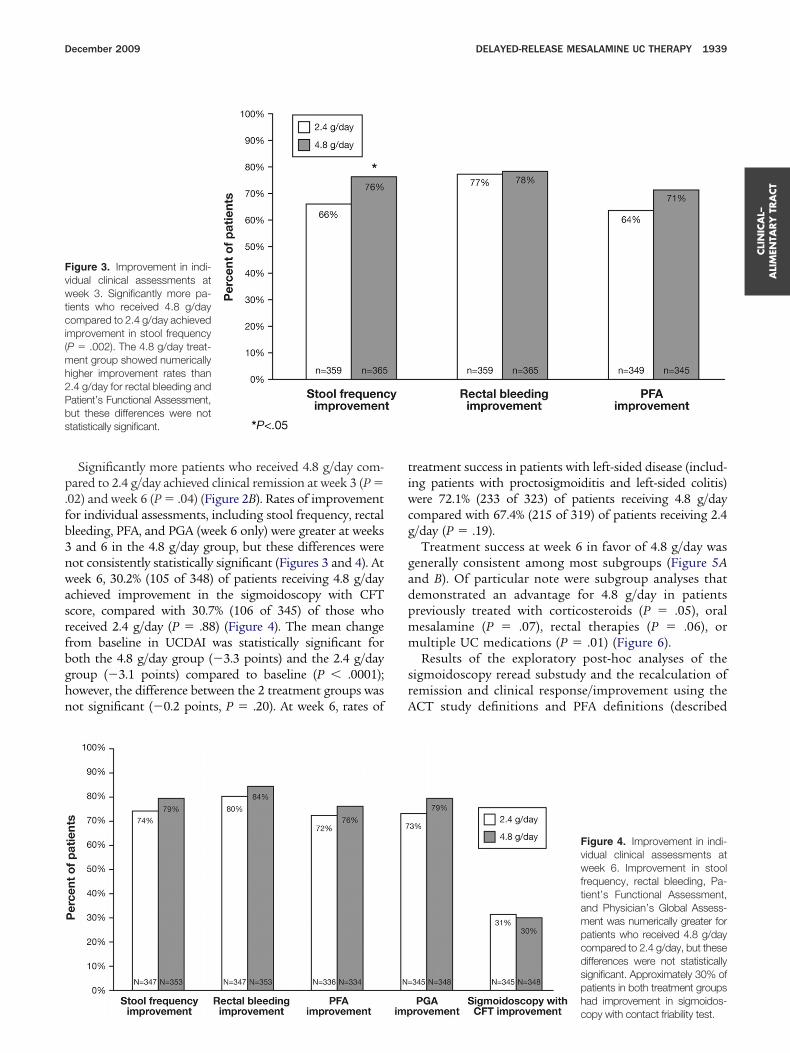
Significantly more patients who received 4.8 g/day com-ared to 2.4 g/day achieved clinical remission at week 3 (P �
02) and week 6 (P � .04) (Figure 2B). Rates of improvementor individual assessments, including stool frequency, rectalleeding, PFA, and PGA (week 6 only) were greater at weeksand 6 in the 4.8 g/day group, but these differences were
ot consistently statistically significant (Figures 3 and 4). Ateek 6, 30.2% (105 of 348) of patients receiving 4.8 g/daychieved improvement in the sigmoidoscopy with CFTcore, compared with 30.7% (106 of 345) of those whoeceived 2.4 g/day (P � .88) (Figure 4). The mean changerom baseline in UCDAI was statistically significant foroth the 4.8 g/day group (�3.3 points) and the 2.4 g/dayroup (�3.1 points) compared to baseline (P � .0001);owever, the difference between the 2 treatment groups wasot significant (�0.2 points, P � .20). At week 6, rates of
igure 3. Improvement in indi-idual clinical assessments ateek 3. Significantly more pa-
ients who received 4.8 g/dayompared to 2.4 g/day achieved
mprovement in stool frequencyP � .002). The 4.8 g/day treat-
ent group showed numericallyigher improvement rates than.4 g/day for rectal bleeding andatient’s Functional Assessment,ut these differences were nottatistically significant.
reatment success in patients with left-sided disease (includ-ng patients with proctosigmoiditis and left-sided colitis)ere 72.1% (233 of 323) of patients receiving 4.8 g/day
ompared with 67.4% (215 of 319) of patients receiving 2.4/day (P � .19).
Treatment success at week 6 in favor of 4.8 g/day wasenerally consistent among most subgroups (Figure 5And B). Of particular note were subgroup analyses thatemonstrated an advantage for 4.8 g/day in patientsreviously treated with corticosteroids (P � .05), oralesalamine (P � .07), rectal therapies (P � .06), orultiple UC medications (P � .01) (Figure 6).Results of the exploratory post-hoc analyses of the
igmoidoscopy reread substudy and the recalculation ofemission and clinical response/improvement using theCT study definitions and PFA definitions (described
Figure 4. Improvement in indi-vidual clinical assessments atweek 6. Improvement in stoolfrequency, rectal bleeding, Pa-tient’s Functional Assessment,and Physician’s Global Assess-ment was numerically greater forpatients who received 4.8 g/daycompared to 2.4 g/day, but thesedifferences were not statisticallysignificant. Approximately 30% ofpatients in both treatment groupshad improvement in sigmoidos-
copy with contact friability test.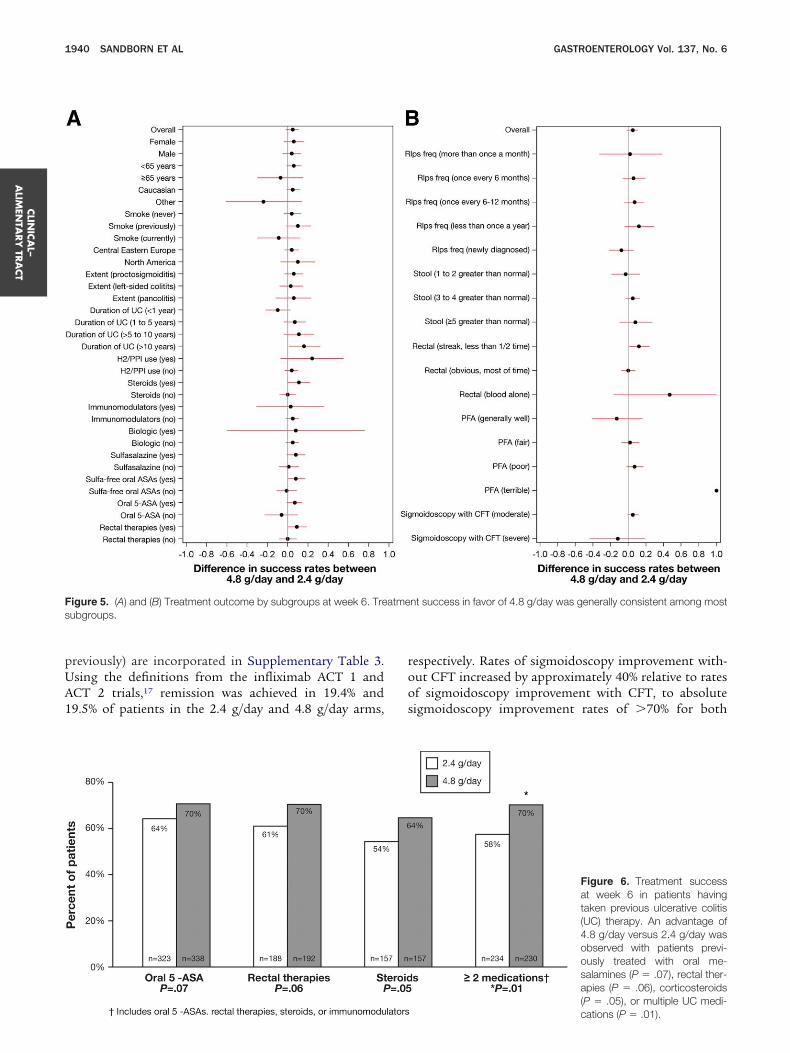
pUA1
roos
Fs
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1940 SANDBORN ET AL GASTROENTEROLOGY Vol. 137, No. 6
reviously) are incorporated in Supplementary Table 3.sing the definitions from the infliximab ACT 1 andCT 2 trials,17 remission was achieved in 19.4% and9.5% of patients in the 2.4 g/day and 4.8 g/day arms,
igure 5. (A) and (B) Treatment outcome by subgroups at week 6. Treubgroups.
espectively. Rates of sigmoidoscopy improvement with-ut CFT increased by approximately 40% relative to ratesf sigmoidoscopy improvement with CFT, to absoluteigmoidoscopy improvement rates of �70% for both
nt success in favor of 4.8 g/day was generally consistent among most
Figure 6. Treatment successat week 6 in patients havingtaken previous ulcerative colitis(UC) therapy. An advantage of4.8 g/day versus 2.4 g/day wasobserved with patients previ-ously treated with oral me-salamines (P � .07), rectal ther-apies (P � .06), corticosteroids(P � .05), or multiple UC medi-
atme
cations (P � .01).

dosCd
basdRc2csmsmtTh(pngnvsm2dwg
laS(s
tgdi..ndtdtgtgS4cfmdsfqeist
tu2hatmdvwfig2d
botuaIpsUcwdr
T
HCNN
M
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
December 2009 DELAYED-RELEASE MESALAMINE UC THERAPY 1941
ose groups when CFT is edited out. There was greaterverall agreement between PFA-based definitions and re-ponse and remission definitions that did not incorporateFT than between response and remission definitions thatid incorporate CFT (see Supplementary Table 3).
SafetyThe percent of patients with AEs was the same for
oth treatment groups (20.6%). A majority of AEs weressessed by the investigators as mild or moderate ineverity and doubtfully related to the study drug. A inci-ence of the most common AEs (Medical Dictionary foregulatory Activities�preferred terms: headache, ulcerative
olitis, nasopharyngitis, nausea) in patients was similar in the.4 g/day and 4.8 g/day groups (Table 2). The mostommonly identified causally related AEs were UC, nau-ea, and headache, and they were similar between treat-
ent groups. Thirty patients were withdrawn from thetudy because of AEs [15 patients (3.9%) in each treat-
ent group]. The most common cause for discontinua-ion was gastrointestinal symptoms associated with UC.he percent of patients with serious AEs was slightlyigher in the 2.4 g/day group than the 4.8 g/day group
1.6% and 1.0%, respectively). There were a total of 10atients with serious AEs; 6 in the 2.4 g/day group (UC,� 3; lower abdominal pain, n � 1; enterocolitis, n � 1,
astroenteritis, n � 1) and 4 in the 4.8 g/day group (UC,� 1; drug hypersensitivity, n � 1; colon cancer, n � 1;
asovagal syncope, n � 1). No deaths occurred during thetudy. Overall both treatments were well-tolerated, with a
ean of 0.4 and 0.3 AEs per patient in the 4.8 g/day and.4 g/day groups, respectively. There were no meaningfulifferences in serum creatinine from baseline to week 6ithin each treatment group or between the 2 treatmentroups at week 6.
DiscussionResults of the ASCEND III trial show that de-
ayed-release mesalamine 4.8 g/day (800-mg tablet) is safend effective for the treatment of moderately active UC.pecifically, the trial demonstrated that 4.8 g/day800-mg tablet) is noninferior to delayed-release me-
able 2. Adverse Events Occurring in �2% in EitherTreatment Group by MedDRA-Preferred Terms
Mesalamine treatment groups
MedDRA-preferred term
2.4 g/day(n � 383)
4.8 g/day(n � 389)
n % n %
eadache 13 3.4 12 3.1olitis ulcerative 12 3.1 10 2.6asopharyngitis 4 1.0 8 2.1ausea 11 2.9 5 1.3
edDRA, Medical Dictionary for Regulatory Activities.
alamine 2.4 g/day (400-mg tablet) for the endpoint of r
reatment success. Subgroup analyses demonstrated aenerally consistent advantage in favor of the 4.8 g/dayose, with borderline significant or significant differences
n patients previously treated with corticosteroids (P �05), oral mesalamines (P � .07), rectal therapies (P �06), or multiple UC medications (P � .01). It should beoted that 70% of patients who received the 4.8 g/dayose (800-mg tablet) achieved treatment success, consis-ent with the response rates observed with the 4.8 g/dayose (800-mg tablet) in 2 previous studies. In contrast,he treatment success rate of 66% achieved with the 2.4/day dose (400-mg tablet) in this study was higher thanhe treatment success rate of 55% achieved with the 2.4/day dose (400-mg tablet) in 2 previous studies.11,12
econdary analyses demonstrated an advantage for the.8 g/day dose over the 2.4 g/day dose for the endpoint oflinical remission, and no difference between the 2 dosesor the endpoints of sigmoidoscopy with CFT improve-
ent and treatment success in patients with left-sidedisease at 6 weeks. At 3 weeks there was demonstrateduperiority of the 4.8 g/day dose over the 2.4 g/day doseor the endpoints of clinical remission and stool fre-uency improvement. There were no significant differ-nces in AEs between the 2 doses. These are clinicallymportant results because symptom relief and a favorableafety profile are important considerations for UC pa-ients and physicians.
The optimal induction dose of mesalamine for thereatment of mildly and moderately active UC has beennclear. The ASCEND I and II trials demonstrated that.4 and 4.8 g/day doses of delayed-release mesalamineave similar efficacy in patients with mildly active UC,nd suggested that the 4.8 g/day dose might have aherapeutic advantage of 13% to 15% in patients with
oderately active UC.11,12 The larger ASCEND III trialemonstrated that the magnitude of the therapeutic ad-antage in patients with moderate disease is actually some-hat smaller (5%) and not significant. Taken together, thendings from these trials indicate that both 2.4 and 4.8/day doses of mesalamine are effective, and thus the lower.4 g/day dose may be preferred for patients with mildisease and some patients with moderate disease.
From a clinical practice perspective, some patients mayenefit from initial therapy with the 4.8 g/day dose andther patients who fail to respond to initial inductionherapy with 2.4 g/day may benefit from dose escalationp to 4.8 g/day without compromising safety. Subgroupnalysis of the combined data set for the ASCEND I andI trials,18 as well as the ASCEND III trial, indicate thatatients who have previously been treated with cortico-teroids, oral mesalamines, rectal therapies, or multipleC medications may have incremental benefit from re-
eiving initial therapy with the 4.8 g/day dose. A studyith another delayed-release mesalamine formulationemonstrated that some patients who fail to achieveemission with 2.4 g/day administered over 8 weeks may
espond to dose escalation to 4.8 g/day administered for
adc
fto3rsartsmsmhdwcFrw
dtowoootdsastocb
tdrntg
(fm4aiMs
Uw
aG1
1
1
1
1
1
1
1
1
CLIN
ICA
L–A
LIMEN
TARY
TRA
CT
1942 SANDBORN ET AL GASTROENTEROLOGY Vol. 137, No. 6
n additional 8 weeks.19 Thus, treatment with a 4.8 g/dayose will continue to play an important role in thelinical care of selected patients with UC.
Although response rates for rectal bleeding and stoolrequency in the ASCEND III study were generally similaro those reported in previous studies, the absolute ratesf sigmoidoscopy improvement observed (approximately0%) are somewhat lower than those that have beeneported in other recent induction studies with me-alamine11,12,14,15 and other agents.17 This was most likelyn artifact of technique and definition.20 We incorpo-ated a CFT performed with closed biopsy forceps passedhrough the therapeutic channel of a flexible sigmoido-cope into our definition of sigmoidoscopy improve-
ent. CFT has not been performed in studies evaluatingigmoidoscopy improvement/mucosal healing in the
odern era, and the technique that we utilized may havead the effect of overestimating friability (and thus un-erestimating sigmoidoscopy improvement) as comparedith the usual technique of assessing contact friability
aused by normal passage of the flexible sigmoidoscope.or this reason, rates of sigmoidoscopy improvementeported in the ASCEND III trial cannot be comparedith those reported in other UC studies.Results of the post-hoc sigmoidoscopy reread substudy
emonstrated that inclusion of the CFT had an impor-ant impact on the sigmoidoscopy results, with the ratef sigmoidoscopy improvement increasing from 30%ith the CFT included to �70% when it was editedut. The sigmoidoscopy with CFT also impacted theperating characteristics of the PGA subscore andverall UCDAI instrument, but the difference betweenreatment groups remained similar. These recalculationsemonstrate that when response and remission are mea-ured in a similar way, rates of response and remissionre generally similar to those reported in previous me-alamine studies. There was better overall agreement be-ween PFA-based response and remission definitions andutcome measures that did not incorporate CFT, indi-ating that in future clinical trials CFT should likely note included as part of the sigmoidoscopy assessment.
Both doses of delayed-release mesalamine were well-olerated and had low rates of serious AEs. There was noose-related toxicity in patients administered delayed-elease mesalamine at 4.8 g/day. Additionally, there wereo significant differences in serum creatinine from baseline
o week 6 in either of the 2 dose groups, or between the doseroups at week 6.
In conclusion, delayed-release mesalamine 4.8 g/day800-mg tablet) is a safe and effective therapeutic optionor treatment of moderately active UC. Patients with
oderately active UC receiving delayed-release mesalamine.8 g/day (800-mg tablet) had a similar likelihood ofchieving treatment success at week 6 as patients receiv-ng delayed-release mesalamine 2.4 g/day (400-mg tablet).
oderate patients treated previously with cortico-
teroids, oral mesalamines, rectal therapies, or multipleC medications may benefit from induction therapyith the 4.8 g/day dose.
Supplementary Data
Note: To access the supplementary materialccompanying this article, visit the online version ofastroenterology at www.gastrojournal.org, and at doi:0.1053/j.gastro.2009.08.069.
References
1. Sutherland L, MacDonald JK. Oral 5-aminosalicylic acid for induc-tion of remission in ulcerative colitis. Cochrane Database SystRev 2006;Apr 19(2):CD000543. Review.
2. Sutherland L, MacDonald JK. Oral 5-aminosalicylic acid for main-tenance of remission in ulcerative colitis. Cochrane DatabaseSyst Rev. 2006;Apr 19(2):CD000544. Review.
3. Carter MJ, Lobo AJ, Travis SP. IBD Section British Society ofGastroenterology. Guidelines for the management of inflamma-tory bowel disease in adults. Gut 2004;53(Suppl 5):V1–V16.
4. Kornbluth A, Sachar DB. Practice Parameters Committee of theAmerican College of Gastroenterology. Ulcerative colitis practiceguidelines in adults (update): American College of Gastroenterology,Practice Parameters Committee. Am J Gastroenterol 2004;99:1371–1385.
5. Travis SPL, Stange EF, Lémann M, et al. European evidence-based consensus on the management of ulcerative colitis: cur-rent management. J Crohns Colitis 2008;2:24–62.
6. Baron JH, Connell AM, Lennard-Jones JE, et al. Sulfasalazine andsalicylazosulphadimidine in ulcerative colitis. Lancet 1962;1:1094–1096.
7. Dick AP, Grayson AP, Carpenter RG, et al. A controlled trial ofsulphasalazine in the treatment of ulcerative colitis. Gut 1964;5:437–442.
8. Sandborn WJ. Oral 5-ASA therapy in ulcerative colitis: what arethe implications of the new formulations? J Clin Gastroenterol2008;42:338–344.
9. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosal-icylic acid therapy for mildly to moderately active ulcerative colitis.A randomized study. N Engl J Med 1987;317:1625–1629.
0. Sninsky CA, Cort DH, Shanahan F, et al. Oral mesalamine(Asacol) for mildly to moderately active ulcerative colitis. A mul-ticenter study. Ann Intern Med 1991;115:350–355.
1. Hanauer SB, Sandborn WJ, Dallaire C, et al. Delayed-release oralmesalamine 4.8 g/day (800 mg tablets) compared to 2.4 g/day(400 mg tablets) for the treatment of mildly to moderately activeulcerative colitis: the ASCEND I trial. Can J Gastroenterol 2007;21:827–834.
2. Hanauer SB, Sandborn WJ, Kornbluth A, et al. Delayed-releaseoral mesalamine at 4.8 g/day (800 mg tablet) for the treatmentof moderately active ulcerative colitis: the ASCEND II trial. Am JGastroenterol 2005;100:2478–2485.
3. Baron JH, Connell AM, Lennard-Jones JE. Variation between ob-servers in describing mucosal appearances in proctocolitis. BrMed J 1964;1:89–92.
4. Kamm MA, Sandborn WJ, Gassull M, et al. Once-daily high con-centration MMX mesalamine in active ulcerative colitis. Gastro-enterology 2007;132:66–75.
5. Lichtenstein GR, Kamm MA, Boddu P, et al. Effect of once- ortwice-daily MMX mesalamine (SPD476) for the induction of re-mission of mild to moderately active ulcerative colitis. Clin Gas-troenterol Hepatol 2007;5:95–102.
6. Shire LLC. Prescribing information for Lialda (mesalamine) de-layed release tablets. Package insert; 2007.
7. Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induc-tion and maintenance therapy for ulcerative colitis. N Engl J Med
2005;353:2462–2476.
1
1
2
R
IH5
A
e(INstPtdboWSac
pA((AJCRBC(CP(DDDFGH(HMP(M
KFCKM(KSR((MT(MZCPARR(RPE(SRRLSR(STHJVCdRI
C
cGsohDPPcGPP
F
CLI
NIC
AL–
ALI
MEN
TARY
TRA
CT
December 2009 DELAYED-RELEASE MESALAMINE UC THERAPY 1943
8. Hanauer SB, Ramsey D, Sandborn WJ. Efficacy of delayed-releaseoral mesalamine in patients who received previous ulcerative colitistreatment. Gastroenterology 2008;134(Suppl 1):A490.
9. Kamm MA, Lichtenstein GR, Sandborn WJ, et al. Effect of ex-tended MMX mesalamine therapy for acute, mild-to-moderateulcerative colitis. Inflamm Bowel Dis 2009;15:1–8.
0. D’Haens G, Sandborn WJ, Feagan BG, et al. A review of activityindices and efficacy endpoints for clinical trials of medical therapy inadults with ulcerative colitis. Gastroenterology 2007;132:763–786.
Received April 26, 2009. Accepted August 27, 2009.
eprint requestsAddress requests for reprints to: William J. Sandborn, MD,
nflammatory Bowel Disease Clinic, Division of Gastroenterology andepatology, Mayo Clinic, 200 First Street SW, Rochester, Minnesota5905. e-mail: [email protected]; fax: (507) 266-0335.
cknowledgmentsEditorial and writing support were provided by Judith M. Pepin, an
mployee of Procter & Gamble Pharmaceuticals. The ASCENDAssessing the Safety and Clinical Efficacy of a New Dose of 5-ASA)II Steering Committee of academic investigators (WJS, JR, BGF, EB,J, ML, SBH) were involved in the design and execution of thetudy; interpretation of results; and drafting and final approval ofhe manuscript. Procter & Gamble Pharmaceutical scientists (BY,K, C-H Y, CAM) were involved with the conception and design ofhe study; assembly, analysis, and interpretation of data; andrafting and final approval of the manuscript. Data were collectedy Procter & Gamble Pharmaceuticals and a clinical researchrganization, and analyzed by Procter & Gamble Pharmaceuticals.JS wrote the first draft of the manuscript and the ASCEND III
teering Committee made the decision to publish. The academicuthors had full access to and vouch for the veracity andompleteness of the data and data analyses.The authors wish to thank the ASCEND III Investigators who
articipated in this study, as listed here in alphabetical order: Olgalexeeva (Nizhny Novogrod, Russian Federation), Istvan Altorjay
Debrecen, Hungary); Stephen Amann (Tupelo, MS), Frank AndersonVancouver, BC, Canada), Greg Anderson (Cincinnati, OH), Jeffreyron, MD (San Francisco, CA), Jeffrey Axler (Toronto, ON, Canada),effrey Baker, MD (Toronto, ON, Canada), Marko Banic (Zagreb,roatia), Scott Becker, MD (Austin, TX), Elena Belousova (Moscow,ussian Federation), Paul Bermanski, MD (Huntington, NY), Pierreoucher, MD (Longueuil, QC, Canada), Marc Bradette (Quebec, QC,anada), Robert Braun, MD (Topeka, KS), Eugeniusz ButrukWarszawa, Poland), Tawfik Chami, MD (Zephyrhills, FL), Naokihiba (Guelph, ON, Canada), Irena Ciecko-Michalska (Krakow,oland), Maria Czerwinska (Krakow, Poland), John Dalena, MD
Cedar Knolls, NJ), Chrystian Dallaire (Quebec, QC, Canada), Olexiyatsenko (Kharkiv, Ukraine), Glen Davis (Little Rock, AR), Godaenapiene (Vilnius, Lithuania), Jelena Derova (Riga, Latvia), Geraldryden (Louisville, KY), Marko Duvnjak (Zagreb, Croatia), Fredowler, MD (Charlotte, NC), Philip Ginsburg (Hamden, CT), Johnriffin (Murray, UT), Flavio Habal (Toronto, ON, Canada), Ljiljanaadnadjev (Novi Sad, Serbia and Montenegro), Richard Hansen
Littleton, CO), Robert Hardi, MD (Chevy Chase, MD), Douglasomoky (Kingsport, TN), Ivo Horny (Strakonice, Czech Republic),arek Horynski (Sopot, Poland), Anthony Infantolino (Philadelphia,A), Zofia Jamrozik-Kruk (Czestochowa, Poland), Gilles Jobin
Montreal, QC, Canada), Njegica Jojic (Belgrade, Serbia and
ontenegro), Waldemar Karnafel (Warszawa, Poland), Miroslava Maticic (Zagreb, Croatia), Oleg Khrustalev (Yaroslavl, Russianederation), Robert Kindel (Cincinnati, OH), Mariusz Klin (Panamaity, FL), Michal Konecny (Olomouc, Czech Republic), Asherornbluth (New York, NY), Darius Kriukas (Panevezys, Lithuania),iodrag Krstic (Beograd, Serbia and Montenegro), Stephen Kuehn
Jacksonville, FL), Piyush Kumar, MD (Encinitas, CA), Limasupcinskas (Kaunas, Lithuania), Olena Levchenko (Odessa, Ukraine),cott Levenson, MD (San Carlos, CA), Milan Lukas (Praha 2, Czechepublic), A.J. Magana, MD (Scottsbluff, NE), Ewa Malecka-Panas
Lodz, Poland), Pramod Malik, MD (Chesapeake, VA), Mircea ManucBucuresti, Romania), Jury Marakhouski (Minsk, Belarus), Bennoargus (Tallinn, Estonia), Elena Mikhailova (Gomel, Belarus),
atyana Mikhailova (Moscow, Russian Federation), Nikola MilinicBeograd, Serbia and Montenegro), P. Miller (Birmingham, AL), Samoussa, MD (Tucson, AZ), Tudor Nicolaie (Bucharest 1, Romania),bigniew Pawlak (Wloclawek, Poland), Pierre Pare (Quebec City, QC,anada), Oliviu Pascu (Cluj-Napoca, Romania, Canada), Sergeiimanov (Vitebsk, Belarus), Henryk Pluta (Abbotsford, BC, Canada),rthur Poch (Shreveport, LA), Juris Pokrotnieks (Riga, Latvia), Yaserayyan (Bismarck, ND), Triin Remmel (Tallinn, Estonia), Brankaoganovic (Beograd, Serbia and Montenegro), Peter Rosenberg, MD
Pasadena, CA), Janusz Rudzinski (Bydgoszcz, Poland), Valeriiusinovich (Minsk, Belarus), Grazyna Rydzewska (Warszawa,oland), Michael Safdi, MD (Cincinnati, OH), Riina Salupere, (Tartu,stonia), William Sandborn (Rochester, MN), Jerrold SchwartzArlington Heights, IL), Chris Shepela (Minneapolis, MN), Natalliailivontchik (Minsk, Belarus), Vladimir Simanenkov (St. Petersburg,ussian Federation), Teresa Sligh (Burbank, CA), Carol Stanciu (Iasi,omania), David Stanton, MD (Orange, CA), Jiri Stehlik (Usti nadabem, Czech Republic), Michal Stepka (Pruszkow, Poland), Davortimac (Rijeka, Croatia), Anatolii Svintsitskyi (Kyiv, Ukraine),ichmond Sy (Ottawa, ON, Canada), Tomasz Sylwestrowicz
Saskatoon, SK, Canada), Tibor Szaloki (Vac, Hungary), Gyorgyzekely (Budapest, Hungary), Judit Szicsek (Budapest, Hungary),adeusz Tacikowski (Warszawa, Poland), Jawahar Taunk, MD (Palmarbor, FL), Robert Tepper, MD (Great Neck, NY), Esther Torres (Sanuan, PR), Zsolt Tulassay (Budapest, Hungary), Raimondaanagaitiene (Vilnius, Lithuania), Tomas Vanasek (Hradec Kralove,zech Republic), Aliaksandr Varabei (Minsk Region, Belarus), Willeme Villiers, MD (Lexington, KY), Mihail Radu Voiosu (Bucuresti,omania), and Mykhailo Zakharash (Kyiv, Ukraine). ClinicalTrials.gov
dentifier NCT00350415.
onflicts of interestThe authors disclose the following: Dr Sandborn has served as a
onsultant for and received research funding from Procter &amble Pharmaceuticals and Shire Pharmaceuticals, and haserved as a consultant for Salix Pharmaceuticals. Dr Regula hasbtained lecture fees from Abbott and Schering Plough. Dr Feaganas received honorariums from Procter & Gamble Pharmaceuticals.r Yacyshyn was previously employed by Procter & Gambleharmaceuticals. Drs Krzeski, Yeh, and Messer are employees ofrocter & Gamble Pharmaceuticals. Dr Hanauer has served as aonsultant for and received clinical research support from Procter &amble Pharmaceuticals and has served as a consultant to Shireharmaceuticals, Ferring Pharmaceuticals, and Salixharmaceuticals. The remaining authors disclose no conflicts.
undingThis study was funded by Procter & Gamble Pharmaceuticals, Inc,
ason, Ohio.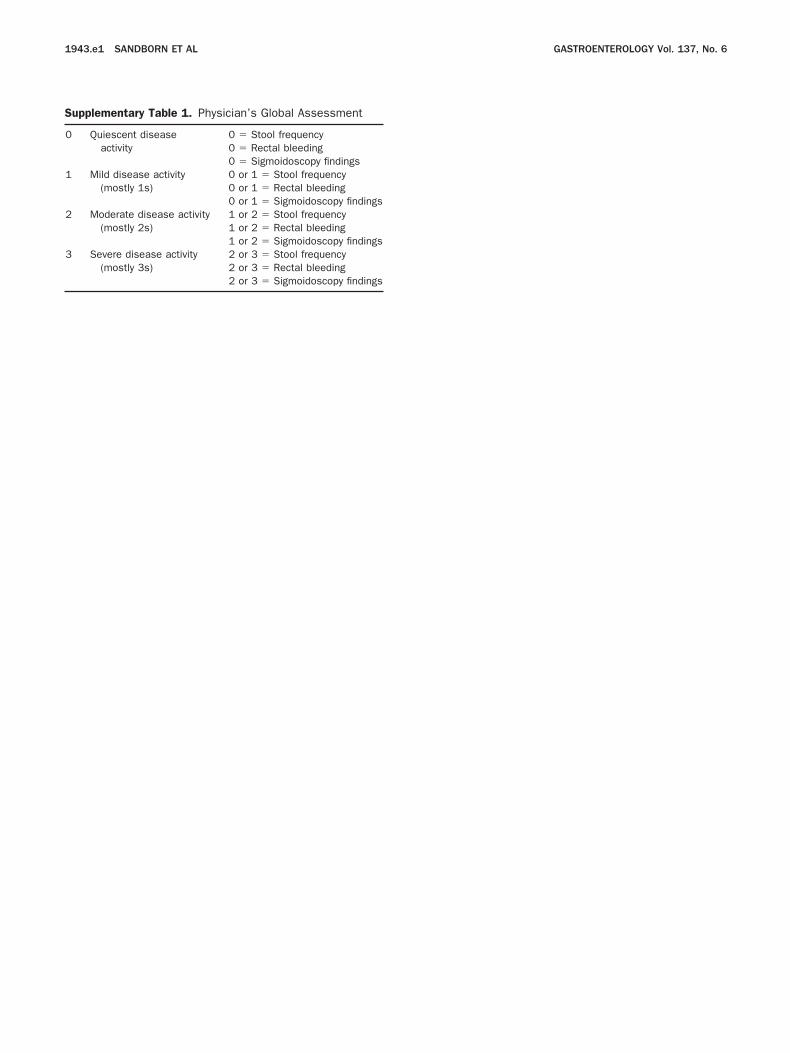
S
1943.e1 SANDBORN ET AL GASTROENTEROLOGY Vol. 137, No. 6
upplementary Table 1. Physician’s Global Assessment
0 Quiescent diseaseactivity
0 � Stool frequency0 � Rectal bleeding0 � Sigmoidoscopy findings
1 Mild disease activity(mostly 1s)
0 or 1 � Stool frequency0 or 1 � Rectal bleeding0 or 1 � Sigmoidoscopy findings
2 Moderate disease activity(mostly 2s)
1 or 2 � Stool frequency1 or 2 � Rectal bleeding1 or 2 � Sigmoidoscopy findings
3 Severe disease activity(mostly 3s)
2 or 3 � Stool frequency2 or 3 � Rectal bleeding
2 or 3 � Sigmoidoscopy findings
S
S
F
a
lb
p
December 2009 DELAYED-RELEASE MESALAMINE UC THERAPY 1943.e2
upplementary Table 2. Sigmoidoscopy Assessment Scoreand Friability Assessment
igmoidoscopy assessmentscorea
0 Normal Intact vascular pattern, no friabilityor granularity
1 Mild Erythema; diminished or absentvascular markings; mildgranularity
2 Moderate Marked erythema, granularity;absent vascular markings;bleeds with minimal trauma; noulcerations
3 Severe Spontaneous bleeding, ulcerationsriability assessmentb
Negative No bleeding after light touch to theworst affected mucosa
Positive Bleeding after light touch to theworst affected mucosa between15 cm and 60 cm from the analverge
For initial entry into the study, the sigmoidoscopy score had to be ateast a 2.For initial entry into the study, the friability assessment had to be
ositive.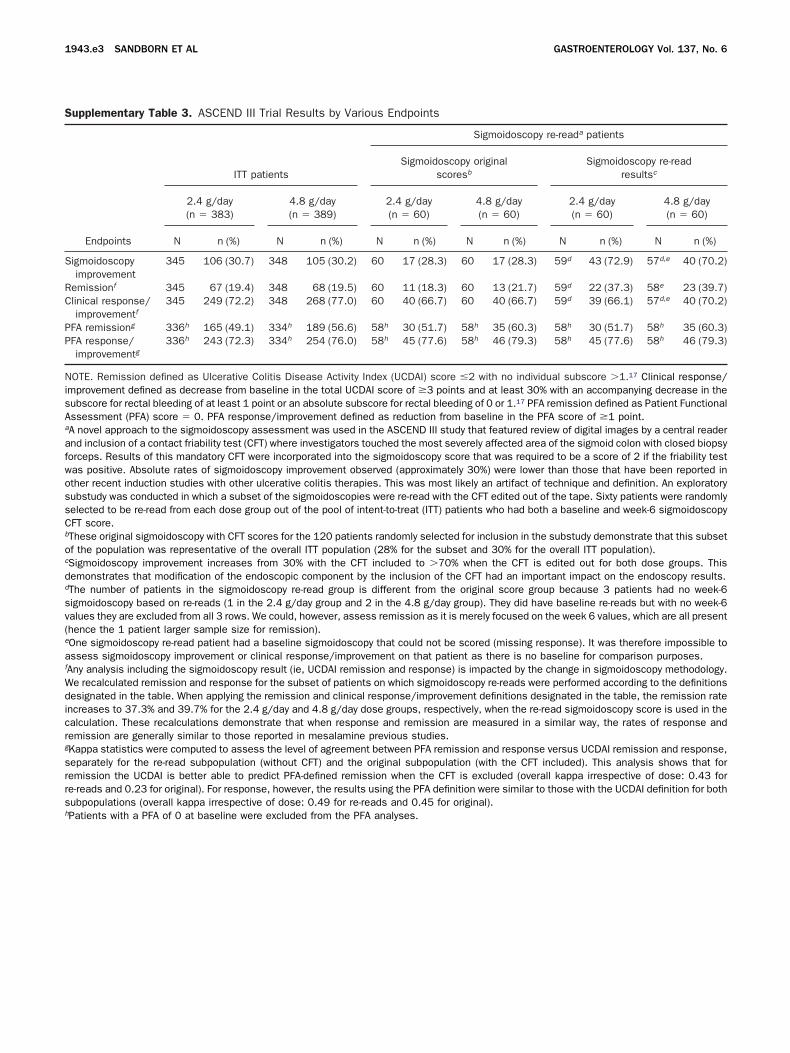
S
S
RC
PP
NisAa
afwossCb
oc
dd
sv(e
af
Wdicrg
srrsh
1943.e3 SANDBORN ET AL GASTROENTEROLOGY Vol. 137, No. 6
upplementary Table 3. ASCEND III Trial Results by Various Endpoints
Endpoints
ITT patients
Sigmoidoscopy re-reada patients
Sigmoidoscopy originalscoresb
Sigmoidoscopy re-readresultsc
2.4 g/day(n � 383)
4.8 g/day(n � 389)
2.4 g/day(n � 60)
4.8 g/day(n � 60)
2.4 g/day(n � 60)
4.8 g/day(n � 60)
N n (%) N n (%) N n (%) N n (%) N n (%) N n (%)
igmoidoscopyimprovement
345 106 (30.7) 348 105 (30.2) 60 17 (28.3) 60 17 (28.3) 59d 43 (72.9) 57d,e 40 (70.2)
emissionf 345 67 (19.4) 348 68 (19.5) 60 11 (18.3) 60 13 (21.7) 59d 22 (37.3) 58e 23 (39.7)linical response/improvementf
345 249 (72.2) 348 268 (77.0) 60 40 (66.7) 60 40 (66.7) 59d 39 (66.1) 57d,e 40 (70.2)
FA remissiong 336h 165 (49.1) 334h 189 (56.6) 58h 30 (51.7) 58h 35 (60.3) 58h 30 (51.7) 58h 35 (60.3)FA response/improvementg
336h 243 (72.3) 334h 254 (76.0) 58h 45 (77.6) 58h 46 (79.3) 58h 45 (77.6) 58h 46 (79.3)
OTE. Remission defined as Ulcerative Colitis Disease Activity Index (UCDAI) score �2 with no individual subscore �1.17 Clinical response/mprovement defined as decrease from baseline in the total UCDAI score of �3 points and at least 30% with an accompanying decrease in theubscore for rectal bleeding of at least 1 point or an absolute subscore for rectal bleeding of 0 or 1.17 PFA remission defined as Patient Functionalssessment (PFA) score � 0. PFA response/improvement defined as reduction from baseline in the PFA score of �1 point.A novel approach to the sigmoidoscopy assessment was used in the ASCEND III study that featured review of digital images by a central readernd inclusion of a contact friability test (CFT) where investigators touched the most severely affected area of the sigmoid colon with closed biopsyorceps. Results of this mandatory CFT were incorporated into the sigmoidoscopy score that was required to be a score of 2 if the friability testas positive. Absolute rates of sigmoidoscopy improvement observed (approximately 30%) were lower than those that have been reported inther recent induction studies with other ulcerative colitis therapies. This was most likely an artifact of technique and definition. An exploratoryubstudy was conducted in which a subset of the sigmoidoscopies were re-read with the CFT edited out of the tape. Sixty patients were randomlyelected to be re-read from each dose group out of the pool of intent-to-treat (ITT) patients who had both a baseline and week-6 sigmoidoscopyFT score.These original sigmoidoscopy with CFT scores for the 120 patients randomly selected for inclusion in the substudy demonstrate that this subsetf the population was representative of the overall ITT population (28% for the subset and 30% for the overall ITT population).Sigmoidoscopy improvement increases from 30% with the CFT included to �70% when the CFT is edited out for both dose groups. Thisemonstrates that modification of the endoscopic component by the inclusion of the CFT had an important impact on the endoscopy results.The number of patients in the sigmoidoscopy re-read group is different from the original score group because 3 patients had no week-6igmoidoscopy based on re-reads (1 in the 2.4 g/day group and 2 in the 4.8 g/day group). They did have baseline re-reads but with no week-6alues they are excluded from all 3 rows. We could, however, assess remission as it is merely focused on the week 6 values, which are all presenthence the 1 patient larger sample size for remission).One sigmoidoscopy re-read patient had a baseline sigmoidoscopy that could not be scored (missing response). It was therefore impossible tossess sigmoidoscopy improvement or clinical response/improvement on that patient as there is no baseline for comparison purposes.
Any analysis including the sigmoidoscopy result (ie, UCDAI remission and response) is impacted by the change in sigmoidoscopy methodology.e recalculated remission and response for the subset of patients on which sigmoidoscopy re-reads were performed according to the definitionsesignated in the table. When applying the remission and clinical response/improvement definitions designated in the table, the remission rate
ncreases to 37.3% and 39.7% for the 2.4 g/day and 4.8 g/day dose groups, respectively, when the re-read sigmoidoscopy score is used in thealculation. These recalculations demonstrate that when response and remission are measured in a similar way, the rates of response andemission are generally similar to those reported in mesalamine previous studies.Kappa statistics were computed to assess the level of agreement between PFA remission and response versus UCDAI remission and response,eparately for the re-read subpopulation (without CFT) and the original subpopulation (with the CFT included). This analysis shows that foremission the UCDAI is better able to predict PFA-defined remission when the CFT is excluded (overall kappa irrespective of dose: 0.43 fore-reads and 0.23 for original). For response, however, the results using the PFA definition were similar to those with the UCDAI definition for bothubpopulations (overall kappa irrespective of dose: 0.49 for re-reads and 0.45 for original).
Patients with a PFA of 0 at baseline were excluded from the PFA analyses.
Related Documents











