Definition: is a gynecological medical condition in women in which endometrial-like cells appear and flourish in areas outside the uterinegynecologicalendometrialcells,
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Definition:
is a gynecological medical condition in women in which endometrial-like cells appear and flourish in areas outside the uterine, most commonly on the ovaries. The uterine cavity is lined by endometrial cells, which are under the influence of female hormones. These endometrial-like cells in areas outside the uterus (endometriosis) are influenced by hormonal changes and respond in a way that is similar to the cells found inside the uterus. Symptoms often worsen with the menstrual cycle.

Endometriosis is typically seen during the reproductive years; it has been estimated that endometriosis occurs in roughly 5-10% of women. Symptoms may depend on the site of active endometriosis. Its main but not universal symptom is pelvic pain in various manifestations. Endometriosis is a common finding in women with infertility.
Signs and symptomsPelvic painA major symptom of endometriosis is recurring pelvic pain. The pain can be mild to severe cramping that occurs on both sides of the pelvis, in the lower back and rectal area, and even down the legs. The amount of pain a woman feels is not necessarily related to the extent or stage (1 through 4) of endometriosis.
Some women will have little or no pain despite having extensive endometriosis or endometriosis with scarring. On the other hand, women may have severe pain even though they have only a few small areas of endometriosis. However, pain does typically correlate to the extent of the disease. Symptoms of endometriosis-related pain may include:

dysmenorrhea painful, sometimes cramps during menses; pain may get worse overtime (progressive pain), also lower back pains linked to the pelvis
chronic pelvic pain – typically accompanied by lower back pain or abdominal pain
dyspareunia – painful sex
dysuria –sometimes painful voiding
dragging pain to the legs are reported more commonly by women with endometriosis. Those with sever disease appears to be more likely to report shooting rectal pain. Individual pain areas and pain intensity appears to be un related to area of endometriosis
Other symptoms may be present, including:
Constipationchronic fatigueheavy or long menstrual periods with small or large blood clotsgastrointestinal problems including diarrhea, bloating and painful defecationextreme pain in legs and thighsback painmild to extreme pain during intercourseextreme pain with or without the presence of mensespremenstrual spottingmild to severe feverheadachesdepressionhypoglycemia (low blood sugar)anxiety
Cause
the exact cause of endometriosis remains unknown, many theories have been presented to better understand and explain its development. These concepts do not necessarily exclude each other.

Cause
1. Estrogens: Endometriosis is a condition that is estrogen-dependent and thus seen primarily during the reproductive years.
In experimental models, estrogen is necessary to induce or maintain endometriosis.
Medical therapy is often aimed at lowering estrogen levels to control the disease.

2. Retrograde menstruation:
The theory of retrograde menstruation, first proposed by John A. Sampson, suggests that during a woman's menstrual flow, some of the endometrial debris exits the uterus through the fallopian tubes and attaches itself to the peritoneal surface (the lining of the abdominal cavity) where it can proceed to invade the tissue as endometriosis.
While most women may have some retrograde menstrual flow, typically their immune system is able to clear the debris and prevent implantation and growth of cells from this occurrence. However, in some patients, endometrial tissue transplanted by retrograde menstruation may be able to implant and establish itself as endometriosis.

2. Retrograde menstruation:
The theory of retrograde menstruation, first proposed by John A. Sampson, suggests that during a woman's menstrual flow, some of the endometrial debris exits the uterus through the fallopian tubes and attaches itself to the peritoneal surface (the lining of the abdominal cavity) where it can proceed to invade the tissue as endometriosis.
While most women may have some retrograde menstrual flow, typically their immune system is able to clear the debris and prevent implantation and growth of cells from this occurrence. However, in some patients, endometrial tissue transplanted by retrograde menstruation may be able to implant and establish itself as endometriosis.
Factors that might cause the tissue to grow in some women but not in others need to be studied, and some of the possible causes below may provide some explanation, e.g., hereditary factors, toxins, or a compromised immune system.

3. Müllerianosis
A competing theory states that cells with the potential to become endometrial are laid down in tracts during embryonic development and organogenesis. These tracts follow the female reproductive (Mullerian) tract as it migrates caudally (downward) at 8–10 weeks of embryonic life. Primitive endometrial cells become dislocated from the migrating uterus and act like seeds or stem cells. This theory is supported by fetal autopsy

4. Coelomic Metaplasia:
This theory is based on the fact that coelomic epithelium is the common ancestor of endometrial andperitoneal cells and hypothesizes that later metaplasia (transformation) from one type of cell to the other is possible, perhaps triggered by inflammation. This theory is further supported by laboratory observation of this transformation.

5. Genetics: Hereditary factors recognized that daughters or sisters of patients with endometriosis are at higher risk of developing endometriosis themselves; for example, low progesterone levels may be genetic, and may contribute to a hormone imbalance.
There is an about 10-fold increased incidence in women with an affected first-degree relative. One study found a link between endometriosis and chromosome effect . The female siblings of patients with endometriosis the relative risk of endometriosis is about 5.7:1 versus a control population.

6. Immune system:
Research is focusing on the possibility that the immune system may not be able to cope with the cyclic of retrograde menstrual fluid.
In this context there is interest in studying the relationship of endometriosis toautoimmune disease, allergic reactions, and the impact of toxins.
It is still unclear what, if any, causal relationship exists between toxins, autoimmune disease, and endometriosis.
7. Environment:
There is a growing suspicion that environmental factors may cause endometriosis, specifically some plastics and cooking with certain types of plastic containers with microwave ovens. Other sources suggest that pesticides and hormones in our food cause a hormone imbalance.
8. Birth Defect: In rare cases where imperforate hymen does not resolve itself prior to the first menstrual cycle and goes undetected, blood and endometrium are trapped within the uterus of the patient until such time as the problem is resolved by surgical incision.
By the time a correct diagnosis has been made, endometrium and other fluids have filled the uterus and fallopian tubes with results similar to retrograde menstruation resulting in endometriosis.

Endometriosis in postmenopausal women does occur and has been described as an aggressive form of this disease characterized by complete progesterone resistance.
In less common cases, girls may have endometriosis symptoms before they even reach menarche.
Complications of endometriosis include:
Internal scarringAdhesionsPelvic cystsChocolate cyst of ovariesRuptured cystBlocked bowel (bowel obstruction)
Infertility can be related to scar formation and anatomical distortions due to the endometriosis; however, endometriosis may also interfere in more subtle ways: cytokines and other chemical agents may be released that interfere with reproduction.Other complications of endometriosis include bowel and ureteral obstruction resulting from pelvic adhesions. Also, peritonitis from bowel perforation can occur.Ovarian endometriosis may complicate pregnancy by decidualization, abscess and/or rupture, It is the most common adnexal mass detected during pregnancy, being present in 0.52% of deliveries as studied in the period 2002 to 2007. Still, ovarian endometriosis during pregnancy can be safely observed conservatively.
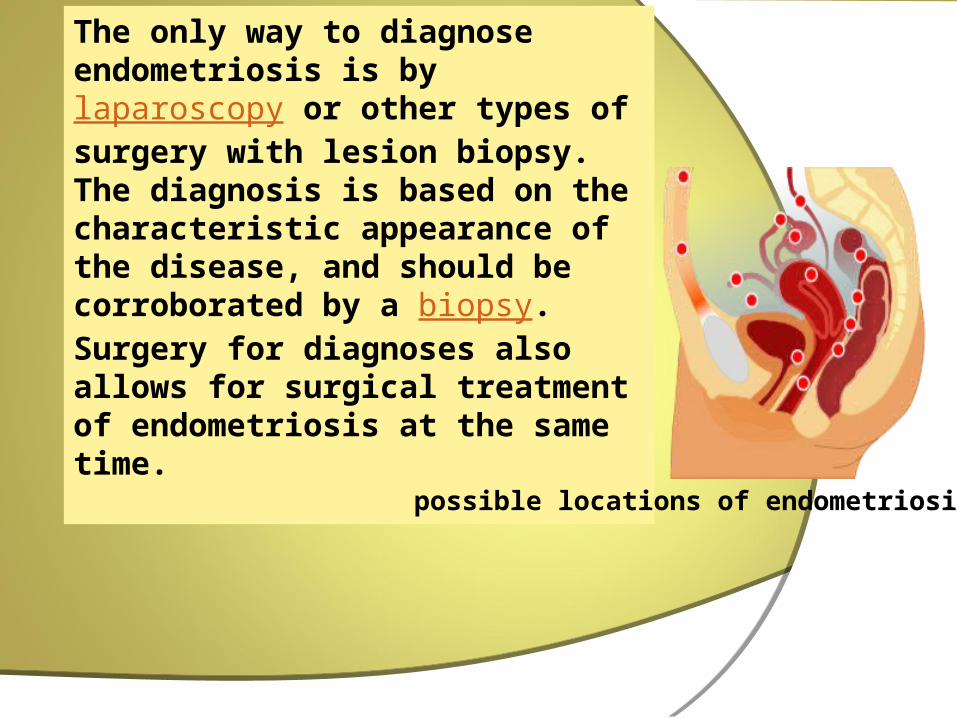
The only way to diagnose endometriosis is by laparoscopy or other types of surgery with lesion biopsy. The diagnosis is based on the characteristic appearance of the disease, and should be corroborated by a biopsy. Surgery for diagnoses also allows for surgical treatment of endometriosis at the same time.
possible locations of endometriosis
various stages show these findings:
Stage I (Minimal)Findings restricted to only superficial lesions and possibly a few filmy adhesionsStage II (Mild)In addition, some deep lesions are present in the cul-de-sacStage III (Moderate)As above, plus presence of endometriomas on the ovary and more adhesionsStage IV (Severe)As above, plus large endometriomas, extensive adhesions.

Disadvantages of medicinal interventionsAdverse effects are commonNot likely to improve fertilitySome can only be used for limited periods of time
Advantages of surgeryHas significant efficacy for pain control. Has increased efficacy over medicinal intervention for infertility treatmentCombined with biopsy, it is the only way to achieve a definitive diagnosisCan often be carried out as a minimal invasive (laparoscopic) procedure to reduce morbidity and minimalize the risk of post-operative adhesions
Disadvantages of surgeryCostRisks are "poorly defined... and probably underestimated." In one study, 3-10% experienced major complications from surgery.
Efficacy is questionable. In the same study, substantial short-term pain relief was experienced by approximately 70-80% of the subjects. However, at 1 year follow-up, approximately 50% of the subjects needed analgesics or hormonal treatments
HEALTH ASSESSMENT
HISTORY TAKING/HEALTH HISTORY
Ensure the baseline history and identify problem.Midwife must access: - General health and family history of patient. - Age of menarche (first menstruation). - Patient’s last menstrual period (LMP), description of menstrual pattern and flow. - Risk for sexually transmitted disease (STD’s). - Pregnancy history : number of pregnancies, live births, stillborn births, type of fetal abnormalities. - Abortion history. - Drug, allergy, substance abuse, and smoking history. - Symptoms of present disorder, such as painful intercourse or characteristic of vaginal discharge, and duration.
PHYSICAL EXAMINATION
Perform the gynecologic examination (pelvic examination), an inspection, and palpation of pelvic reproductive system.Obtains examination gloves, lubricant, several sizes of bivalve speculums and light source.Firstly inspect the external genitalia and adjacent structures, following inspection of the vaginal wall and cervix by using a bivalve speculum.Next, one or two fingers of a lubricated, gloves hand are placed into vagina.Do the vaginal-abdominal palpitation, structures beyond the vaginal orifice are examined.Access the position, size, and contour of the uterus, ovaries, and other pelvic structures.At the end of examination, a gloved finger is inserted into the rectum to palpate the posterior surface of the uterus.
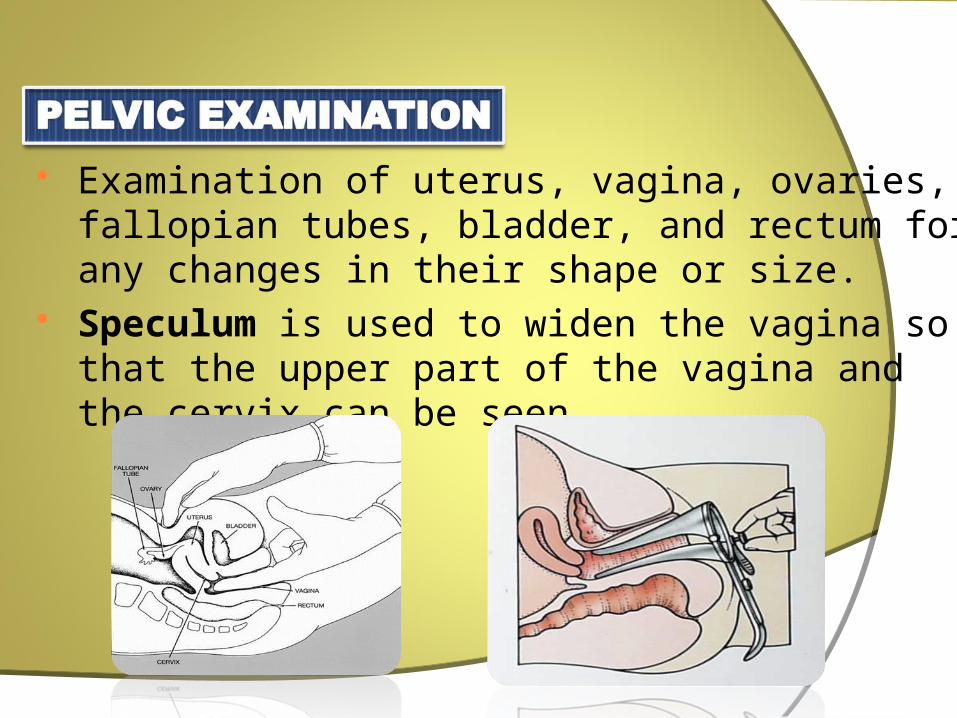
Examination of uterus, vagina, ovaries, fallopian tubes, bladder, and rectum for any changes in their shape or size.
Speculum is used to widen the vagina so that the upper part of the vagina and the cervix can be seen

Sound waves that shows organs and structures in the pelvis; bladder, ovaries, uterus, cervix, and fallopian tubes
Abnormalities : small ovarian cysts, leiomyoma, endometrial carcinoma.
Evaluation of endometrium : thickness.

Procedure used to examine the vagina, uterus, fallopian tubes, ovaries, and bladder.
Transducer (probe) is inserted into the vagina that causes sound waves to bounce off organs inside the pelvis.
Creates a sonogram.
Diagnostic Investigations
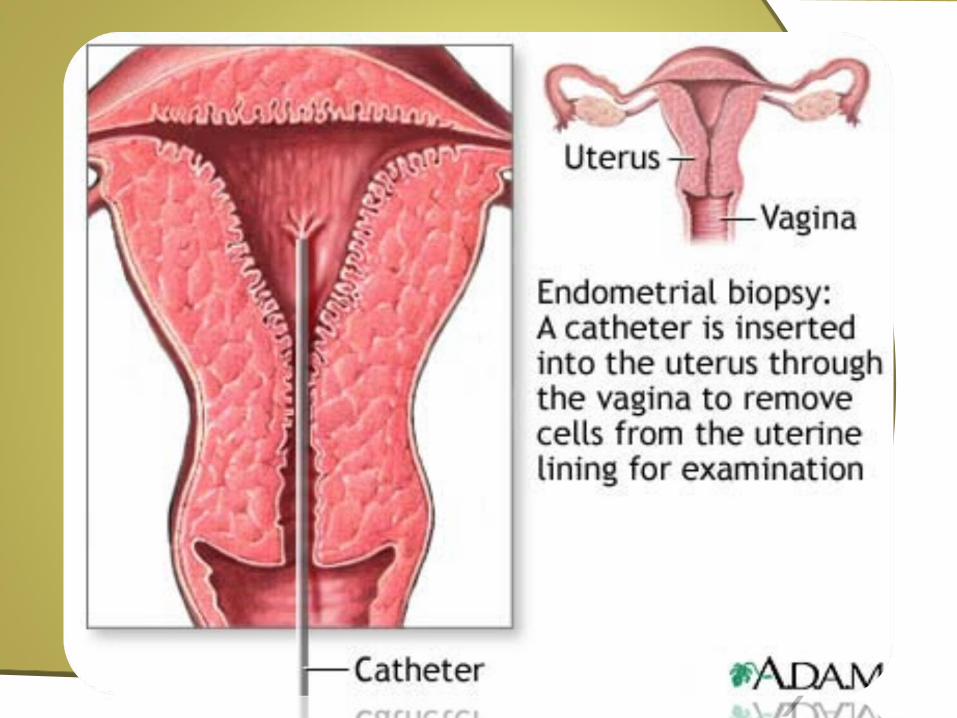
Hysteroscopy is the examination of the whole endometrial cavity, lower segment and cervical canal ; to detect small polyps or sub-mucous fibroids.
Hysteroscopy alone (without biopsy) is not very accurate in diagnosing endometrial hyperplasia and carcinoma.
Endometrial biopsy or aspirate is to exclude endometrial pathology like hyperplasia, endometrial disorders or malignancies.


Diagnostic Investigations
These tests can rule out hyperthyroidism or hypothyroidism and hyperprolactinemia.
These conditions cause ovarian dysfunction leading to possible menorrhagia.

MEDICAL & SURGICAL MANAGEMENT

In endometriosis management the goal is to
provide pain relief, to restrict progression of the
process, and to restore or preserve fertility where
needed. In younger women, surgical treatment
attempts to remove endometrial tissue and
preserving the ovaries without damaging normal
tissue.
In women who do not have need to maintain
reproductive life, hysterectomy and/or removal of
the ovaries may be an option; however, this will
not guarantee that the endometriosis and/or the
symptoms of endometriosis will not come back,
and surgery may induce adhesions which can
lead to complications.

Treatments for endometriosis in women who do not wish to become pregnant include:
1. Progesterone or Progestins neutralizes and inhibits the
growth of the endometrium.
Progestins are chemical alternatives of natural
progesterone
Avoiding products with xenoestrogens, which have a
similar effect to naturally produced estrogen and can
increase growth of the endometrium.
2. Hormone contraception therapy:
Oral contraceptives reduce the menstrual pain
associated with endometriosis. They may
function by reducing or eliminating menstrual
flow and providing estrogen support.
Typically, it is a long-term approach.

Recently Seasonale was approved to reduce
periods to 4 per year. Other OCPs have
however been used like this off label for
years. Continuous hormonal consists of the
use of combined oral contraceptive pills
eliminates monthly bleeding episodes.
3. Danazol (Danocrine) and gestrinone are
suppressive steroids with some androgenic
activity. Both agents inhibit the growth of
endometriosis but their use remains limited
as they may cause hirsutism and voice
changes.

4. Gonadotropin Releasing Hormone (GnRH)
agonist: These agents work by increasing the
levels of GnRH that results in down
regulation,inducing by decreasing-
FSH and LH levels. While effective in some
patients, they induce unpleasant menopausal
symptoms, and over time may lead
to osteoporosis. These drugs can only be
used for six months at a time.

5. Lupron depo shot is a GnRH agonist and is
used to lower the hormone levels in the woman's
body to prevent or reduce growth of
endometriosis. The injection is given in 2
different doses a once a month for 3 month shot
or for 6 month shot with the dosage of
according to dr. prescription.
6. Aromatase inhibitors are medications that
block the formation of estrogen and have become
of interest for researchers who are treating
endometriosis.
NSAIDs Anti-inflammatory. They are commonly
used in conjunction with other therapy. For more
severe cases narcotic prescription drugs may be
used. NSAID injections can be helpful for severe
pain or if stomach pain prevents oral NSAID use.
7. Morphine sulphate tablets (MST) and other
opioid painkillers work by mimicking the action
of naturally occurring pain-reducing chemicals
called "endorphins".
8. Diclofenac suppository or pill form to reduce
inflammation and as an analgesic reducing
pain.
Surgery
Procedures are classified as
1. conservative when reproductive organs are
retained,
semi-conservative when ovarian function is allowed
to continue,
radical when the uterus and ovaries are removed.
removal, excision (called cystectomy) or ablation of
endometriosis, adhesions, resection of
endometriomas, and restoration of normal pelvic
anatomy as much as is possible.
2. Radical therapy in endometriosis removes the uterus
(hysterectomy) and tubes and ovaries (bilateral
salpingo-oophorectomy) and thus the chance for
reproduction. Radical surgery is generally reserved for
women with chronic pelvic pain that is disabling and
treatment-resistant. Not all patients with radical
surgery will become pain-free.
3. Semi-conservative therapy preserves a healthy
appearing ovary, and yet, it also increases the risk of
recurrence.

For patients with extreme pain, a presacral
neurectomy may be indicated where the
nerves to the uterus are cut. neurectomy is
more effective in pain relief if the pelvic pain
is midline concentrated, and not as effective
if the pain extends to the left and right lower
quadrants of the abdomen.
2. Endometrial destruction or ablation
Destroy or remove the endometrial tissue.
Performed for women who has been diagnosed with menorrhagia and cannot or do not want to have hysteroscopy procedure.
Endometrial ablation destroys a thin layer of the lining of the uterus and stops the menstrual flow.
In some women, menstrual bleeding does not stop but is reduced to normal or lighter levels.

Surgical Management

Related Documents