Defining Non-Classical Primary or Secondary Hypogonadism: Time for a Reset? Mohit Khera, M.D., M.B.A., M.P.H. Associate Professor of Urology Scott Department of Urology Baylor College of Medicine Houston, TX GnRH LH FSH Testosterone Testosterone Sperm Hypothalamus Pituitary Testis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Defining Non-Classical Primary or Secondary Hypogonadism:
Time for a Reset?
Mohit Khera, M.D., M.B.A., M.P.H.Associate Professor of Urology
Scott Department of Urology
Baylor College of Medicine
Houston, TX
GnRH
LH FSHTestosterone
Testosterone
Sperm
Hypothalamus
Pituitary
Testis

Testosterone Testing and Initiation
Layton et al. J Clin Endocrinol Metab 2014; 99(3):835-842

Diagnosis of Androgen Deficiency and Late Onset Hypogonadism (LOH)
Biochemical Signs and Symptoms
+

Diagnosing Hypogonadism Defined by 2010 Endocrine Guidelines

Prevalence of Androgen Deficiency
T = testosterone.
Mulligan T, et al. Int J Clin Pract. 2006;60(7):762-769.
Overall, 38.7% of men >45y
have T-levels<300 ng/mL
Percen
t Lo
w T
esto
stero
ne
0
10
20
30
40
50
60
>85
Patient Age Range
45 to
54
55 to
64
65 to
74
75 to
84

Results
Araujo et al., J Clin Endocrinol Metab 2007 Nov;92(11):4241-7
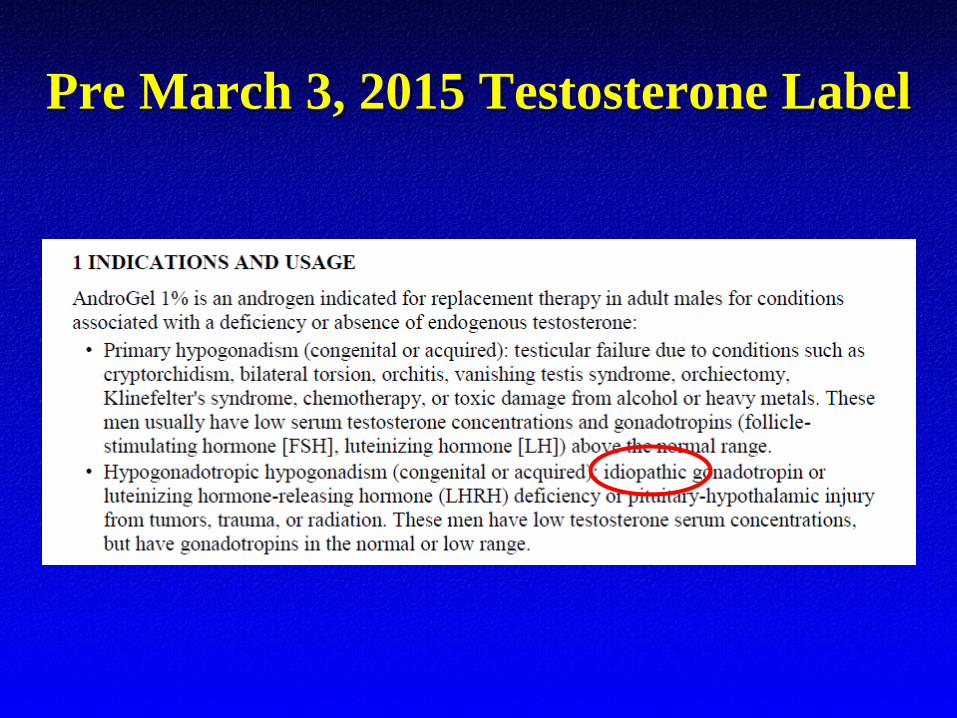
Pre March 3, 2015 Testosterone Label


Post March 3, 2015 Testosterone Label
LH
(U
/L)
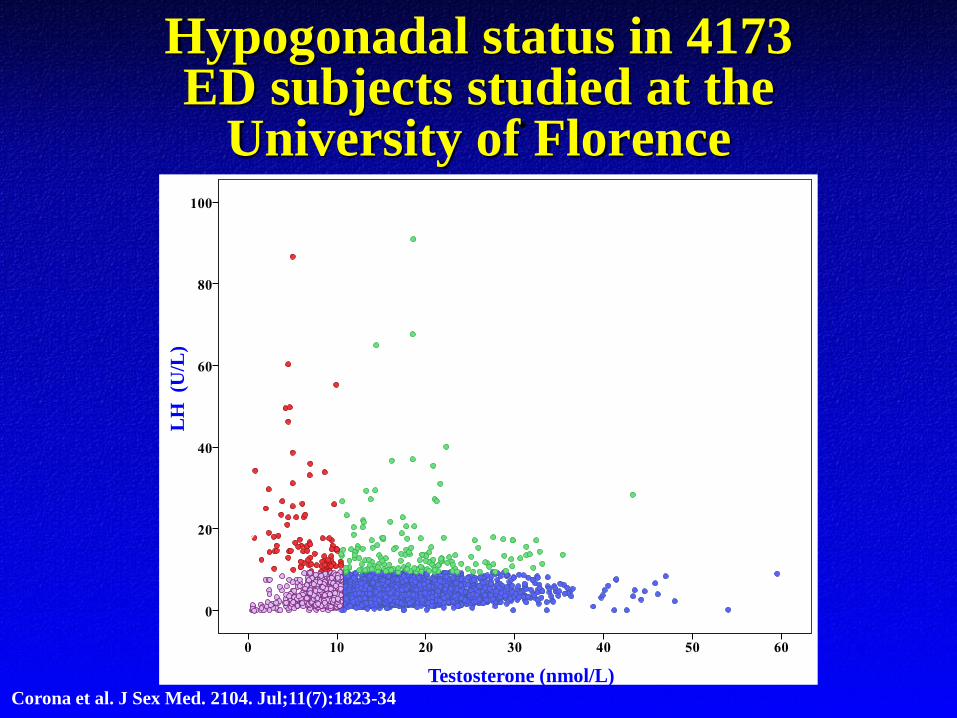
Testosterone (nmol/L)Corona et al. J Sex Med. 2104. Jul;11(7):1823-34
Hypogonadal status in 4173ED subjects studied at the
University of Florence

LH
(U
/L) Compensated
hypogonadism
(4.1%)
Primary
hypogonadism
(2.5%)
Secondary hypogonadism
(17.3%)
LH
= 9
.4 U
/L
Eugonadism
(76.1%)
Testosterone (nmol/L)
Corona et al. J Sex Med. 2104. Jul;11(7):1823-34
Hypogonadal status in 4173ED subjects studied at the
University of Florence

Unknown
Secondary
Primary
Eugonadism
Prevalence of Hypogonadism in Men
with ED
69.2%
Specific medical
conditions
3.2%
17.4%
50.4% 49.6%
89.1% 10.9%
Maseroli et al J Sex Med 2015 Apr;12(4):956-65.

Radiotherapy
Surgery
Genetic
Specific Medical Conditions Associated with
Secondary Hypogonadism
1.1
3.4
1.1 1.7
1.1
0.1
2.4
89.1% 10.9%
Trauma
PRL-adenomas
Empty sella DrugsUnknown
Specific medical conditions
Maseroli et al J Sex Med 2015 Apr;12(4):956-65.

Unknown
Concomitant metabolic disease
(Obesity, T2DM or MetS)
Specific Medical Conditions Associated with
Secondary Hypogonadism
71.8%28.2%
89.1% 10.9%
Unknown
Specific medical conditions
Maseroli et al J Sex Med 2015 Apr;12(4):956-65.

Traish, J Androl 2009
Low Testosterone Levels and Diabetes/Metabolic Syndrome

Relationship Between Total Testosterone and the Number of MS Components
To
tal
Testo
ste
ron
e (
nM
)m
ean
an
d 9
5%
co
nfi
den
ce i
nte
rval
Number of Metabolic Syndrome Components
Corona G et al. Eur Urol. 2006; 50: 595-604

SMSNA Colloquium
• August 2015 expert colloquium commissioned by the Sexual Medicine Society of North America (SMSNA) convened in Washington, DC
• Panel consisted of 17 experts in men’s health, sexual medicine, urology, endocrinology, and methodology
• Purpose: To discuss hypogonadal men with associated signs and symptoms accompanied by low or normal gonadotropin levels and do not have classical hypogonadism

• AOH is a clinical and biochemical syndrome characterized by a deficiency of testosterone with signs and symptoms that can be caused by testicular and/or hypothalamic-pituitary dysfunction
• AOH is clinically distinct from classical primary and secondary hypogonadism
• AOH is characterized by T deficiency and the failure to mount an adequate compensator pituitary response to low T levels; gonadotropin levels are low or in the normal range
• AOH more often occurs in men who have chronic medical conditions
• AOH is not a new category of hypogonadism; but rather, a condition we had been treating with TTh that we previously classified as idiopathic hypogonadism
Khera et al. Mayo Clin Proc. 2016 Jul;91(7):908-26

Is it Safe and Beneficial to Treat AOH Patients with Testosterone
Therapy?Medical Benefits
• Diabetes
• Metabolic syndrome
• Obesity
• Osteoporosis
• Cardiovascular
Symptomatic Benefits
• Erectile dysfunction
• Libido
• Muscle strength
• Energy
• Mood/Depression
We have more safety and benefits data on patients with
AOH than we do with patients with classical primary or
secondary hypogonadism

Effects on Insulin Resistance From Testosterone Therapy: The Times 2 Study
• A 12-month, multicenter, prospective, randomized, double-blind, placebo-controlled study
Study Design
• 220 hypogonadal men with Type 2 diabetes and metabolic syndromePopulation
• Significant improvement in insulin resistance in all patients (15.2% at 6m and 16.4% at 12m)
• Significant improvement in HDL (-0.049 mmol/L) and LDL cholesterol (-0.210 mmol/L), lipoprotein a (-0.31 mmol/L) in selected groups
• Significant improvement in erectile function (IIEF increase of 4.8 points)
• CVE higher in placebo (10.7 vs. 4.6%; P = 0.095)
Results
Jones TH, et al. Diabetes Care. 2011;34(4):828-837.
IIEF = International Index of Erectile Function

Effects on HbA1c From Testosterone Therapy: BLAST Study
• 30 week double-blind placebo-controlled study of long-acting T undeconoatefollowed by open label 52 weeks
Study Design
• 211 male type 2 diabeticsPopulation
• Significant improvement in HbA1c at 6 and 18 weeks
• Significantly reduction in waist circumference, weight and BMI related to achieving adequate serum testosterone levels
• 1 patient with CAD died of an MI in open label
Results
Hackett et al J Sex Med.2014 Mar;11(3):840-56

Effects of Testosterone Treatment on BodyFat and Lean Mass in Obese Men on a
Hypocaloric Diet
• 56-week, randomised, double-blind, parallel, placebo-controlled study
Study Design
• 82 obese adult men (BMI ≥30 kg/m2) with median age 53 years Population
• TTh resulted in a significant reduction in fat mass (-2.9 kg) and visceral fat (-2678 mm2) over dieting alone
• 1 CVE in control group and 1 CVE in TRT group
Results
Fui et al. BMC Medicine (2016) 14:153

• 137 RPC studies assessing TTh and changes in IIEF
• 14 studies were included with 2,298 subject
• Mean follow-up 40.1 weeks
• Mean age 60.2 years
• “nearly all studies included in this meta-analysis were comprised of populations of men without classic hypogonadism”
Corona et al. Eur Urol. 2017 epub

Results
Corona et al. Eur Urol. 2017 epub

• RPC Trial of 790 men 65 years and older
• T gel or placebo for 12 months
• Participation in one or more of 3 trials
• Sexual Function Trial
• Physical Function Trial
• Vitality Trial
• 63% of subjects were obese
Snyder et al N Engl J Med. 2016 Feb 18;374(7):611-24

Results
• Significant improvement in sexual activity, sexual desire and erectile function
• Significant improvement in 6 min walking distance when all 3 trials were combined
• Improvement in mood and severity of depressive symptoms compared to placebo
• No improvement in vitality Snyder et al N Engl J Med. 2016 Feb 18;374(7):611-24

Snyder et al N Engl J Med. 2016 Feb 18;374(7):611-24
Results
• Year 1: 7 men in each group were adjudicated to have major CVE (MI, stroke, or death from CV causes
• Year 2: 2 men in the testosterone group and 9 men in the placebo group were adjudicated to have had major CVE

Conclusion• Most hypogonadal patients being treated
with TTh today are being treated off-label
• AOH is a true medical condition which comprises the majority of the patients that are being treated with TTh
• Historically, studies assessing the safety and benefits of TTh have consisted mainly of patients with non-classical secondary hypogonadism, or AOH
• Patients with non-classical and classical primary and secondary hypogonadism all appear to equally benefit from TTh, irrespective of the etiology of their disease

Thank You
Texas Medical Center, Houston
Related Documents











