PATIENT FACING SYSTEMS Decreasing Operating Room Turnover Time: A Resource Neutral Initiative Shawne Olson 1 & Stephanie Jaross 2 & Gail S. Rebischke-Smith 1 & Frank Chivers 3 & Stephanie K. Covel 1 & Carolyn E. Millen 1 Received: 11 December 2017 /Accepted: 26 March 2018 # Springer Science+Business Media, LLC, part of Springer Nature 2018 Introduction Important to leaders in healthcare organizations is the ability to deliver safe quality care to patients and support provider satisfaction, in a cost effective manner. Care of the patient in the operating room is one area in which leaders can assess these elements. In a 281 bed community hospital, affiliated with a large academic medical center, a process improvement project was undertaken to improve efficiency in the operating room. The facility has 12 operating rooms that support con- tinued surgical growth. A need exists to maximize operating room utilization as surgical volume increases. The creation of an effective strategy to increase access to the operating room may improve accessibility of the operating room for the care of surgical patients. Understanding the flow in the operating room provides the foundation for addressing this issue. The reduction of time between surgical cases is an important component that may improve access to care for patients and surgeons. Background The time spent in the operating room can be divided into two components; operative time and non-operative time. For the purpose of this process improvement initiative, operative time is defined as the time in which the surgeon makes the incision, performs the surgical procedure, and secures the dressing to the incision. Non-operative time includes all the remaining activities that take place from the time one patient exits the operating room until the surgeon makes the incision for the next surgical procedure in the same operating room. For ex- ample, case set-up, induction, positioning, skin prep, and draping. At the conclusion of operative time, non-operative time includes drape removal, emergence, patient transfer, and turnover time. Turnover time is defined as the time in which one patient exits the operating room until the next patient enters the oper- ating room. Turnover time includes: removing soiled linen and trash, cleaning the horizontal surfaces and the floor, changing the bed and /or bed position, acquiring positioning devices, and special equipment. The surgical case is set up by opening supplies and instruments, preparing the back table, completing the count, and preparing medications. Turnover time is a factor of which operating room personnel have some control. Other components of non-operative time are influenced by patient. For example, induction, airway manage- ment, ease of positioning, emergence and patient transfer are unique to each patient. The focus of this process improvement project was to maximize efficiency in the operating room by decreasing turnover time without adding resources. Literature review Access to operating room facilities is a limited resource [1]. One patient and surgeon dis-satisfier is the need for additional operating room time [1, 2]. A means by which operating room time could be increased is by decreasing non-operative time, ideally, without additional capital or human resources. The review of the literature is scant with studies directly addressing interventions designed to decrease non-operative time. Several studies address the causes of delayed turnover time, means by which to measure turnover time, and the need for additional resources to improve turnover time [ 3–5]. This article is part of the Topical Collection on Patient Facing Systems * Stephanie K. Covel [email protected] 1 University of Washington/Northwest Hospital, 1550 N. 115th St., B239, Seattle, WA 98133, USA 2 Proliance, 23628 107th Place W, Edmonds, WA 98020, USA 3 University of Washington/Northwest Hospital and Seattle Anesthesiologists, 1550 N. 115th St, Seattle, WA 98133, USA Journal of Medical Systems (2018) 42:96 https://doi.org/10.1007/s10916-018-0950-5

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PATIENT FACING SYSTEMS
Decreasing Operating Room Turnover Time: A Resource NeutralInitiative
Shawne Olson1& Stephanie Jaross2 & Gail S. Rebischke-Smith1
& Frank Chivers3 & Stephanie K. Covel1 &
Carolyn E. Millen1
Received: 11 December 2017 /Accepted: 26 March 2018# Springer Science+Business Media, LLC, part of Springer Nature 2018
Introduction
Important to leaders in healthcare organizations is the abilityto deliver safe quality care to patients and support providersatisfaction, in a cost effective manner. Care of the patient inthe operating room is one area in which leaders can assessthese elements. In a 281 bed community hospital, affiliatedwith a large academic medical center, a process improvementproject was undertaken to improve efficiency in the operatingroom. The facility has 12 operating rooms that support con-tinued surgical growth. A need exists to maximize operatingroom utilization as surgical volume increases.
The creation of an effective strategy to increase access tothe operating roommay improve accessibility of the operatingroom for the care of surgical patients. Understanding the flowin the operating room provides the foundation for addressingthis issue. The reduction of time between surgical cases is animportant component that may improve access to care forpatients and surgeons.
Background
The time spent in the operating room can be divided into twocomponents; operative time and non-operative time. For thepurpose of this process improvement initiative, operative timeis defined as the time in which the surgeon makes the incision,
performs the surgical procedure, and secures the dressing tothe incision. Non-operative time includes all the remainingactivities that take place from the time one patient exits theoperating room until the surgeon makes the incision for thenext surgical procedure in the same operating room. For ex-ample, case set-up, induction, positioning, skin prep, anddraping. At the conclusion of operative time, non-operativetime includes drape removal, emergence, patient transfer, andturnover time.
Turnover time is defined as the time in which one patientexits the operating room until the next patient enters the oper-ating room. Turnover time includes: removing soiled linenand trash, cleaning the horizontal surfaces and the floor,changing the bed and /or bed position, acquiring positioningdevices, and special equipment. The surgical case is set up byopening supplies and instruments, preparing the back table,completing the count, and preparing medications.
Turnover time is a factor of which operating room personnelhave some control. Other components of non-operative time areinfluenced by patient. For example, induction, airway manage-ment, ease of positioning, emergence and patient transfer areunique to each patient. The focus of this process improvementproject was to maximize efficiency in the operating room bydecreasing turnover time without adding resources.
Literature review
Access to operating room facilities is a limited resource [1].One patient and surgeon dis-satisfier is the need for additionaloperating room time [1, 2]. A means by which operating roomtime could be increased is by decreasing non-operative time,ideally, without additional capital or human resources. Thereview of the literature is scant with studies directly addressinginterventions designed to decrease non-operative time.Several studies address the causes of delayed turnover time,means by which to measure turnover time, and the need foradditional resources to improve turnover time [3–5].
This article is part of the Topical Collection on Patient Facing Systems
* Stephanie K. [email protected]
1 University of Washington/Northwest Hospital, 1550 N. 115th St.,B239, Seattle, WA 98133, USA
2 Proliance, 23628 107th Place W, Edmonds, WA 98020, USA3 University of Washington/Northwest Hospital and Seattle
Anesthesiologists, 1550 N. 115th St, Seattle, WA 98133, USA
Journal of Medical Systems (2018) 42:96 https://doi.org/10.1007/s10916-018-0950-5

According to Kumar & Malhotra [4] the reasons for delay inturnover time and inefficiency between surgical cases are mul-tifactorial, interdisciplinary, and unavoidable. However, theimpact of improved turnover time is increased access to theoperating room for surgeons and patients [2]. Overlapping ofthe induction of anesthesia improves operating room efficien-cy allowing additional surgical cases to be scheduled [2].Mercereau et al., [5] designed a patient flow model to includetwo operating rooms and an additional room for the anesthe-siologist to place a spinal block prior to the patient entering theoperating room.
Beaule, Frombach & Ryu [6] addressed the need to in-crease the number of cases performed in an eight hour day.In a retrospective chart review, the authors identified predic-tors of success, which included anesthesia preparation time,surgical duration, and anesthesia finishing time. Benchmarksfor success were identified and may be applied to a targetedgroup of interventions designed to increase available operativetime.
Other studies specifically addressed turnover time, the timeone patient exits the operating room until the next patient entersthe operating room. Cendan & Good [3] designed a study toimprove turnover times by assessing the current workflow inthe operating room, addressing the tasks performed by the circu-lating nurse, and notifying support staff. The results of this studydemonstrated an overall improvement in turnover times.Unfortunately, the authors were not able to attribute the improve-ment to a specific metric. According to Jerico, Perroca & daPenha [7] the nurse’s efficient use of resources can improveturnover time.
Bhatt, Carlson & Deckers [8] used a systems based approachto reduce turnover time through standardization in practice.Developing consistent criteria for operating room readiness,completing processes in parallel, and enhancing communicationamong staff and physicians, the authors were able achieve im-proved turnover times. Standardization and reliable methods fa-cilitate a reduction in variation, improve efficiency, and decreaseturnover time.
Benchmarks for operating room turnover time include threemajor categories, greater than 40 minutes, 25 to 40 minutes, andless than 25minutes. These groupingswere used byMecario [9] asa metric for calculating operating room efficiency. Turnover timewas one of eight measures used to assess proficiency in operatingroom utilization. The best performing hospitals had an averageturnover time of less than 25minutes for all types of surgical cases.
The review of the literature confirms access to operatingroom facilities is a limited resource [1]. Turnover time is con-trollable to some degree through the use of overlapping oper-ating rooms with or without separate teams and the use of aseparate room for the anesthesiologist to deliver a regionalanesthetic [5]. The literature lacks specific studies and inter-ventions designed to decrease turnover time and increase op-erative time that do not result in additional resources.
Methods
The purpose of the current process improvement initiative was toimprove operating room efficiency without requiring additionalresources. To address operating room efficiency, a review ofhistorical turnover times was completed using retrospective datareporting. Following the review of historical turnover times bysurgeon and service, focused observations of operating roomturnover were performed in October 2016 by surgical servicesleaders. A total of 40 procedures were observed.
Three major opportunities to improve efficiency werefound related to workflow for the anesthesiologist, circulatingnurse, and post-anesthesia care nurse. A process improvementinitiative was designed to address workflow elements with agoal of a 10% reduction in operating room turnover over timesby the end of the pilot project.
Changes in workflow included: the circulating nurse seeingthe patient in the pre-operative holding area before going to theoperating room to set up the case. Next, the anesthesiologistplaces the spinal for the patient, and when the operating roomis ready, the pre-admission nurse transports the patient to theoperating room. The preadmission nurse assists the circulatingnurse and the anesthesiologist in transferring from the patient tothe operating room bed. When the case is complete and thesurgeon is closing the skin, the circulating nurse calls the postanesthesia care unit. A nurse from post anesthesia care unitcomes to the operating room to receive report from both thecirculating nurse and the anesthesiologist. After the dressing issecured, the drapes are removed and the patient is transferredback to the stretcher, the post anesthesia care unit nurse and thecirculating nurse transport the patient to the post anesthesia careunit. This allows the anesthesiologist to go directly to the pre-admission area to see the next patient and place the spinal anes-thetic. The circulating nurse goes from the post anesthesia careunit to the pre-admission area to see the next patient pre-operatively before returning to the operating room to completethe turnover and ready the room for the next patient.
Proposed changes were discussed with surgical services lead-ership. Input was obtained from surgeons, anesthesiologists, andstaff prior to implementation. Staff with new roles and responsi-bilities were given focused training leading up to the implemen-tation date. Education and training were provided to the pre-admission and post anesthesia care unit nurses regarding appro-priate surgical attire, operating room traffic patterns, safe patienthandling, and safe patient transport.
Results
The pilot project was implemented on January 4, 2017. Theprocess improvement initiative included patients undergoing atotal joint replacement with spinal anesthesia for one orthope-dic surgeon. The results of the pilot demonstrate the ability to
96 Page 2 of 3 J Med Syst (2018) 42:96
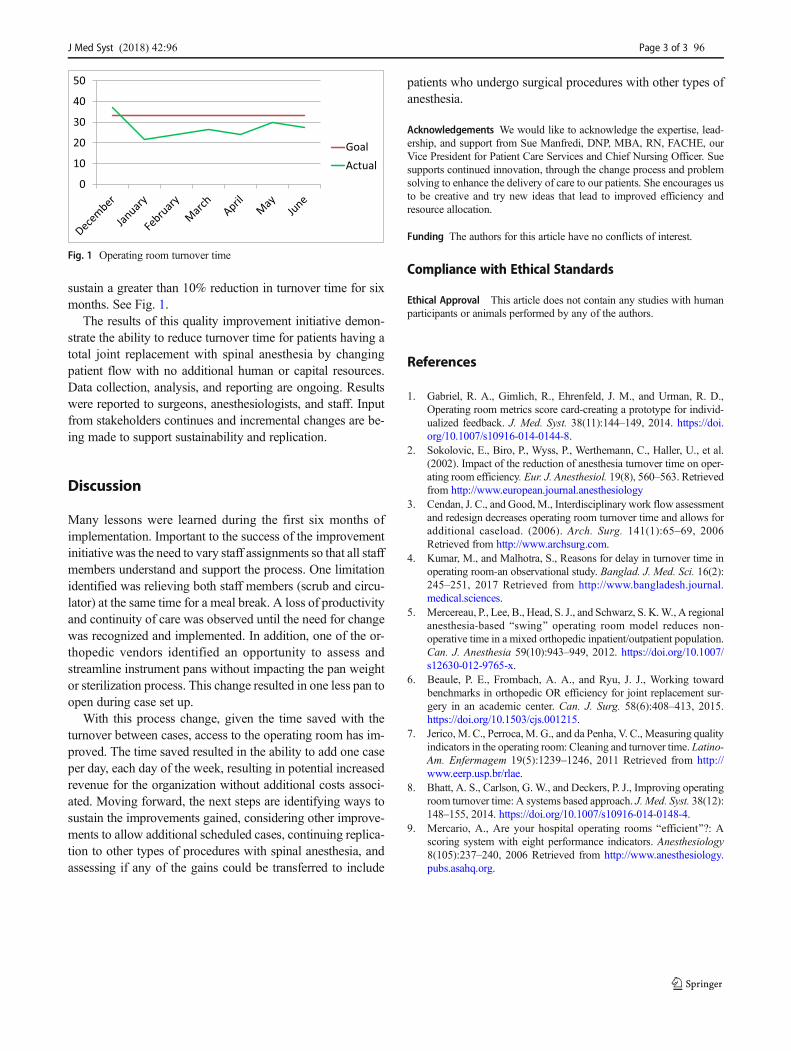
sustain a greater than 10% reduction in turnover time for sixmonths. See Fig. 1.
The results of this quality improvement initiative demon-strate the ability to reduce turnover time for patients having atotal joint replacement with spinal anesthesia by changingpatient flow with no additional human or capital resources.Data collection, analysis, and reporting are ongoing. Resultswere reported to surgeons, anesthesiologists, and staff. Inputfrom stakeholders continues and incremental changes are be-ing made to support sustainability and replication.
Discussion
Many lessons were learned during the first six months ofimplementation. Important to the success of the improvementinitiative was the need to vary staff assignments so that all staffmembers understand and support the process. One limitationidentified was relieving both staff members (scrub and circu-lator) at the same time for a meal break. A loss of productivityand continuity of care was observed until the need for changewas recognized and implemented. In addition, one of the or-thopedic vendors identified an opportunity to assess andstreamline instrument pans without impacting the pan weightor sterilization process. This change resulted in one less pan toopen during case set up.
With this process change, given the time saved with theturnover between cases, access to the operating room has im-proved. The time saved resulted in the ability to add one caseper day, each day of the week, resulting in potential increasedrevenue for the organization without additional costs associ-ated. Moving forward, the next steps are identifying ways tosustain the improvements gained, considering other improve-ments to allow additional scheduled cases, continuing replica-tion to other types of procedures with spinal anesthesia, andassessing if any of the gains could be transferred to include
patients who undergo surgical procedures with other types ofanesthesia.
Acknowledgements We would like to acknowledge the expertise, lead-ership, and support from Sue Manfredi, DNP, MBA, RN, FACHE, ourVice President for Patient Care Services and Chief Nursing Officer. Suesupports continued innovation, through the change process and problemsolving to enhance the delivery of care to our patients. She encourages usto be creative and try new ideas that lead to improved efficiency andresource allocation.
Funding The authors for this article have no conflicts of interest.
Compliance with Ethical Standards
Ethical Approval This article does not contain any studies with humanparticipants or animals performed by any of the authors.
References
1. Gabriel, R. A., Gimlich, R., Ehrenfeld, J. M., and Urman, R. D.,Operating room metrics score card-creating a prototype for individ-ualized feedback. J. Med. Syst. 38(11):144–149, 2014. https://doi.org/10.1007/s10916-014-0144-8.
2. Sokolovic, E., Biro, P., Wyss, P., Werthemann, C., Haller, U., et al.(2002). Impact of the reduction of anesthesia turnover time on oper-ating room efficiency. Eur. J. Anesthesiol. 19(8), 560–563. Retrievedfrom http://www.european.journal.anesthesiology
3. Cendan, J. C., and Good, M., Interdisciplinary work flow assessmentand redesign decreases operating room turnover time and allows foradditional caseload. (2006). Arch. Surg. 141(1):65–69, 2006Retrieved from http://www.archsurg.com.
4. Kumar, M., and Malhotra, S., Reasons for delay in turnover time inoperating room-an observational study. Banglad. J. Med. Sci. 16(2):245–251, 2017 Retrieved from http://www.bangladesh.journal.medical.sciences.
5. Mercereau, P., Lee, B., Head, S. J., and Schwarz, S. K.W., A regionalanesthesia-based Bswing^ operating room model reduces non-operative time in a mixed orthopedic inpatient/outpatient population.Can. J. Anesthesia 59(10):943–949, 2012. https://doi.org/10.1007/s12630-012-9765-x.
6. Beaule, P. E., Frombach, A. A., and Ryu, J. J., Working towardbenchmarks in orthopedic OR efficiency for joint replacement sur-gery in an academic center. Can. J. Surg. 58(6):408–413, 2015.https://doi.org/10.1503/cjs.001215.
7. Jerico,M. C., Perroca,M. G., and da Penha, V. C., Measuring qualityindicators in the operating room: Cleaning and turnover time. Latino-Am. Enfermagem 19(5):1239–1246, 2011 Retrieved from http://www.eerp.usp.br/rlae.
8. Bhatt, A. S., Carlson, G. W., and Deckers, P. J., Improving operatingroom turnover time: A systems based approach. J. Med. Syst. 38(12):148–155, 2014. https://doi.org/10.1007/s10916-014-0148-4.
9. Mercario, A., Are your hospital operating rooms Befficient^?: Ascoring system with eight performance indicators. Anesthesiology8(105):237–240, 2006 Retrieved from http://www.anesthesiology.pubs.asahq.org.
0
10
20
30
40
50
GoalActual
Fig. 1 Operating room turnover time
J Med Syst (2018) 42:96 Page 3 of 3 96

Journal of Medical Systems is a copyright of Springer, 2018. All Rights Reserved.
Related Documents











