Page 1/24 Decreased plasma neuropeptides in rst-episode schizophrenia, bipolar disorder, major depressive disorder: associations with clinical symptoms and cognitive function Hua Yu Sichuan University Peiyan Ni Sichuan University Liansheng Zhao Sichuan University Yang Tian Sichuan University Mingli Li Sichuan University Xiaojing Li Zhejiang University School of Medicine Wei Wei Zhejiang University School of Medicine Jinxue Wei Sichuan University Wei Deng Zhejiang University Xiangdong Du Suzhou Psychiatry Hospital, Aliated Guangji Hospital of Soochow University Qiang Wang Sichuan University Wanjun Guo Zhejiang University School of Medicine Xiaohong Ma Sichuan University Jeremy Coid Sichuan University Tao Li ( [email protected] ) Zhejiang University Research Article

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Page 1/24
Decreased plasma neuropeptides in �rst-episodeschizophrenia, bipolar disorder, major depressivedisorder: associations with clinical symptoms andcognitive functionHua Yu
Sichuan UniversityPeiyan Ni
Sichuan UniversityLiansheng Zhao
Sichuan UniversityYang Tian
Sichuan UniversityMingli Li
Sichuan UniversityXiaojing Li
Zhejiang University School of MedicineWei Wei
Zhejiang University School of MedicineJinxue Wei
Sichuan UniversityWei Deng
Zhejiang UniversityXiangdong Du
Suzhou Psychiatry Hospital, A�liated Guangji Hospital of Soochow UniversityQiang Wang
Sichuan UniversityWanjun Guo
Zhejiang University School of MedicineXiaohong Ma
Sichuan UniversityJeremy Coid
Sichuan UniversityTao Li ( [email protected] )
Zhejiang University
Research Article
Page 2/24
Keywords: Schizophrenia, bipolar disorder, major depressive disorder, neuropeptide, disease monitoring
Posted Date: June 9th, 2022
DOI: https://doi.org/10.21203/rs.3.rs-1705849/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read FullLicense
Page 3/24
Abstract
BackgroundThere is an urgent need to identify differentiating and disease-monitoring biomarkers of schizophrenia, bipolardisorders (BD), and major depressive disorders (MDD) to improve treatment and management.
MethodsWe recruited 54 �rst-episode schizophrenia (FES) patients, 52 BD patients, 35 MDD patients, and 54 healthy controlsfrom inpatient and outpatient clinics. α-Melanocyte-Stimulating Hormone (α-MSH), β-endorphins, neurotensin,orexin-A, oxytocin, and substance P were investigated using quantitative multiplex assay method. Psychoticsymptoms were measured using the Brief Psychiatric Rating Scale (BPRS) and Positive and Negative SyndromeScale (PANSS), manic symptoms using the Young Mania Rating Scale (YMRS), and depressive symptoms using 17item-Hamilton Depression Rating Scale (HAMD). We additionally measured executive function using thecomputerized Cambridge Neuropsychological Test Automated Battery (CANTAB) given to all participants.
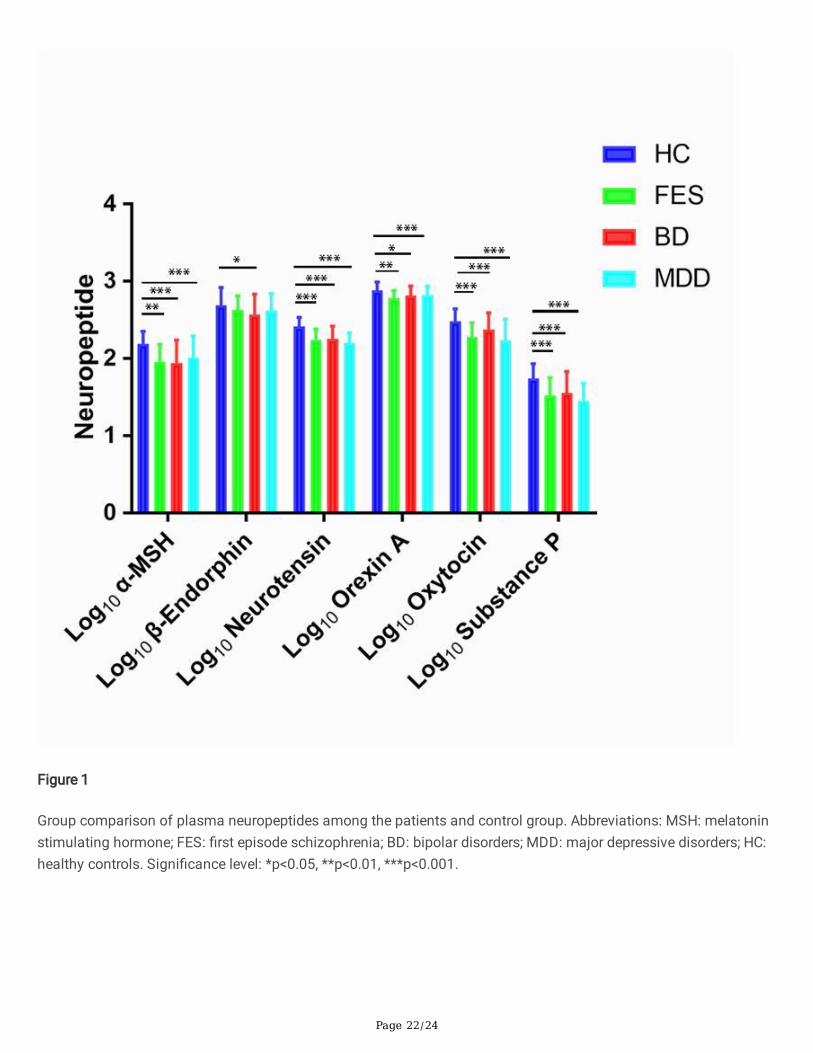
Resultsα-MSH, neurotensin, orexin-A, oxytocin, and substance P were decreased in the three patient groups compared withcontrols. Neurotensin outperformed all biomarkers in differentiating patient groups from controls. There were nosigni�cant differences for 6 neuropeptides in their ability to differentiate between the three patient groups. Higherneurotensin was associated with better executive function across the entire sample. Lower oxytocin and highersubstance p were associated with more psychotic symptoms in FES and BD groups. β-endorphin was associatedwith early morning wakening symptom in all three patient groups.
ConclusionOur research shows circulating neuropeptides have the potential to differentiate severe mental illnesses fromcontrols. These neuropeptides are promising treatment targets for improving clinical symptoms and cognitivefunction in FES, BD, and MDD.
BackgroundSchizophrenia (SCZ), bipolar disorder (BD), and major depressive disorders (MDD) are common and serious mentalillnesses associated with substantial morbidity and mortality as well as high personal and societal costs [1].Although these disorders are a severe public health problem [2], our understanding and treatment of mental illnesseshave lagged behind the progress of other medical �elds [3]. The main reason for this lag is the limitations of currentdiagnostic systems [4]. According to the diagnostic criteria of the Diagnostic and Statistical Manual (DSM) ofMental Disorders system, SCZ, BD, and MDD are split into three separate categories based on duration of illness,dysfunction in important areas of life, psychotic symptoms, and presence of depression or mania [5]. However,genetic studies show those three disorders share common genetic liability [6]. Furthermore, despite nosologicalspeci�city, these disorders can have shared mood disturbance (depression, euphoria, irritability, anhedonia, etc.),psychotic symptoms (hallucinations, delusions), and cognitive impairment (executive function, and memory

Page 4/24
impairment) [7–9]. Research has suggested that dimensional representations may be more accurate representationsthan simple categorical descriptions when applied to the diagnosis of psychotic and non-psychotic disorders [10].
In addition to this diagnostic issue, the etiopathology of these diseases is not well understood. Accumulating datafrom animal and human studies suggest that the pathophysiology of SCZ, BD and MDD are associated withmonoamine abnormality [7, 11–13]. Although the monoamine hypothesis is supported by the clinical e�cacy ofmany drugs for treating mental illness, there is usually a time lag between the acute pharmacological effects andclinical improvement [14]. Furthermore, their therapeutic effects are limited, with high relapse rates, and a proportionof patients will deteriorate over the life course [15–17]. The search for novel drugs for treating psychiatric disordersthat can improve on effectiveness with improved side-effect pro�le compared to currently available therapies is ofconsiderable importance [18, 19].
Recently, research into the mechanism and drug treatment of mental illness has focused increasingly onneuropeptides, which are distributed throughout the digestive, circulatory, and nervous systems, and can serve asneurotransmitters, neuromodulators, and hormones [17, 20, 21]. Neuropeptides are often co-localized and co-released with monoamine neurotransmitters such as dopamine, glutamate, or γ-aminobutyric acid (GABA) [22], andcan be detected peripherally. More than 100 neuropeptides have been identi�ed, and most act via one or more of acorrespondingly large number of 7-transmembrane, G protein-coupled receptors (GPCRs) (> 200) [22]. Neuropeptidesand their receptors modulate many diverse functions of the central nervous system, including reward, sleep,emotion, and executive function [23–25]. Previous studies have indicated β-endorphin, oxytocin, opioid peptides,orexin, and neurotensin (NT), are all implicated in mental illness [24, 26–28]. Lower cerebral spinal �uid (CSF)neurotensin concentrations appear to be correlated with greater psychopathology severity, including thoughtdisorder, de�cit symptoms, disorganized behavior, and impaired functioning [20]. NT de�ciency impairs the workingmemory function [29], and NT genes variances were associated with executive function among healthy participants[25]. Plasma oxytocin was reported to be correlated negatively with psychotic symptoms [30]. Animal andexperimental studies focused on neuropeptides in depression, found α-melanocyte stimulating hormone (MSH), andtheir receptors might have the potential to be treatment targets in stress-related mood disorders [31, 32]. β-endorphinis the most important primary agonist of mu-opioid receptors [33]. It is involved in reward-centric and homeostasis-restoring behaviors, which makes it a research target of interest in psychiatric disorders [33, 34].
Despite these �ndings, neuropeptide studies still offer little insight into either core pathophysiology or treatmentoptions for SCZ, BD, and MDD [35]. Precise brain neuropeptide measurement using CSF from lumbar punctures isinvasive and not suitable for widespread use [36]. In contrast, plasma detection of neuropeptides is less invasive,can accurately detect concentration, and be used widely in clinical research. In this study, we used a new immuno-assay measurement to detect the plasma level of neuropeptides in �rst-episode schizophrenia (FES), BD, and MDD.Firstly, we tested whether neuropeptides can be used as a biomarker to distinguish FES, BD and MDD. As there issubstantial evidence suggesting that FES, BD, and MDD share clinical manifestations and cognitive dysfunction [37,38], we hypothesized that the biomarker of plasma neuropeptide may not be able to distinguish these diseases.Secondly, due to the cross-disorder existence of clinical symptoms and cognitive defects, we also hypothesized thatabnormal levels of neuropeptides would be associated with clinical symptoms and cognitive function across thepatient groups irrespective of diagnosis.
Materials And MethodsParticipants
Page 5/24
FES, BD, MDD, and healthy control (HC) volunteers were recruited for the current study from in- and outpatientpsychiatric facilities at West China Hospital of Sichuan University. We recruited �fty-four FES (26 male, 28 female),52 BD (21 male, 31 female), and 35 MDD (15 male, 20 female), diagnosed according to standard operational criteriain the Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV). 54 healthy volunteers (23 male, 31female) were included. Healthy volunteers were screened for major psychiatric disorders using the StructuredClinical Interview for DSM-IV, non-patient edition. Symptom severity scores were measured using the Positive andNegative Symptom Rating Scale (PANSS), the Brief Psychiatric Rating Scale (BPRS), the Young Mania Rating Scale(YMRS), and 17-item Hamilton Depression Rating Scale (HAMD). Patients were excluded if they met the criteria foralcohol or substance abuse within one year of screening, and signi�cant medical illness. All subjects were right-handed and provided written informed consent. The study was approved by the West China Hospital of SichuanUniversity Ethics committee.
Cognitive function measurement
Intelligence quotient (IQ), verbal IQ, and performance IQ scores of all participants were assessed using the seven-subtest short form of the revised Wechsler Adult Intelligence Scale in Chinese [39]. The CambridgeNeuropsychological Test Automated Battery (CANTAB) is a computerized tool used to measure cognitive function indiverse populations [40]. Stockings of Cambridge (SOC) is a part of the CANTAB task. Participants are shown twodisplays, each containing colored balls. Each participant must move the ball in the lower display to copy the patternshown in the upper display. During the test, participants are asked to make as few moves as possible to match thetwo patterns. SOC problems solved in minimum moves is a fundamental measure, recording the number ofoccasions upon which the subject has completed a test problem in the minimum possible number of moves. Itincluded mean moves for 2, 3, 4, and 5-move problems. Here, we used the problems solved in minimum moves for 5-move problems (MM5M). SOC-MM5M is a measure of spatial planning memory and executive function. A lowerscore indicates better performance.
Plasma neuropeptide measurements
Not fasted blood samples were collected by venipuncture between 4.00 p.m. and 4.30 p.m.using ethylenediaminetetraacetic acid as an anti-coagulant. Peripheral blood mononuclear cells were removed byrefrigerated centrifugation at 1,000 g for 10 min, and the separated plasma was immediately divided into 0.5-mLaliquots and stored at −80 °C. The MILLIPLEX® MAP Human Neuropeptide Magnetic Bead Panel is used for thesimultaneous quanti�cation of the following 6 analytes in any combination: α-MSH, β-Endorphin, Neurotensin,Orexin-A, Oxytocin, and Substance P. This kit may be used for the analysis of all or any combination of the aboveanalytes in tissue/cell lysate, culture supernatant samples, and CSF, serum or plasma samples.
Statistical analysis
Stata 14.0 and SPSS 24.0 were used for the analysis. The distribution of the continuous variables was checkedusing Shapiro-Wilk’s test. Log10 transformation was used to correct variables that were not normallydistributed. Parametric comparisons (t-test or one-way ANOVA with post-hoc Bonferroni analysis). Fisher’s exact testwas used to check the statistical signi�cance of between-group differences. Spearman or Pearson correlation wasconducted to test the correlation coe�cient for categorical variables or continuous variables respectively. Since thefour subjects’ groups were not matched on age, education levels, and body mass index (BMI), the differences incognitive function and plasma neuropeptides among groups were tested by ANCOVA. The results are presented asmean ± standard deviation unless otherwise speci�ed (Table 1). Differentiating performance of plasma markers
Page 6/24
was assessed using age-gender-BMI adjusted area-under-the-curve (AUC) values from receiver operatingcharacteristic (ROC) analyses (FES vs HC; BD vs HC; MDD vs HC; FES vs BD; FEP vs MDD; and BD vs MDD). The testaccuracy, sensitivity, speci�city, predictive values and AUC (AUC: 0.9–1.0 = excellent; 0.8–0.9 = good; 0.7–0.8 = fair;0.6–0.7 = poor; 0.5–0.6 = fail) were measured [41]. Differences in AUCs were evaluated using bootstrapping (n =1000). In a second step, we compared the best-performing plasma biomarker (based on AUC) to a modelincorporating all plasma biomarkers using logistic regression for each of the six contrasts used in the ROC analyses.Models were then compared using the Akaike information criterion (AIC) [42], where a difference of ≥ 2 pointsindicates a better model �t.
Finally, separate stepwise linear regression analyses were used to test associations between plasma neuropeptidesand clinical symptom scores or cognitive function. The linear regression model used age, gender, education, BMI,group status, log10 α-MSH, log10 β-endorphins, log10 neurotensin, log10 orexin A, log10 oxytocin, and log10 substanceP as independent variables. The least signi�cant variables were removed one at a time until only signi�cantvariables remained. Signi�cance was taken as P < 0.05. Supplementary Table 1 shows the factors excluded,respectively, in the linear regression models.
ResultsDemographic and clinical characteristics
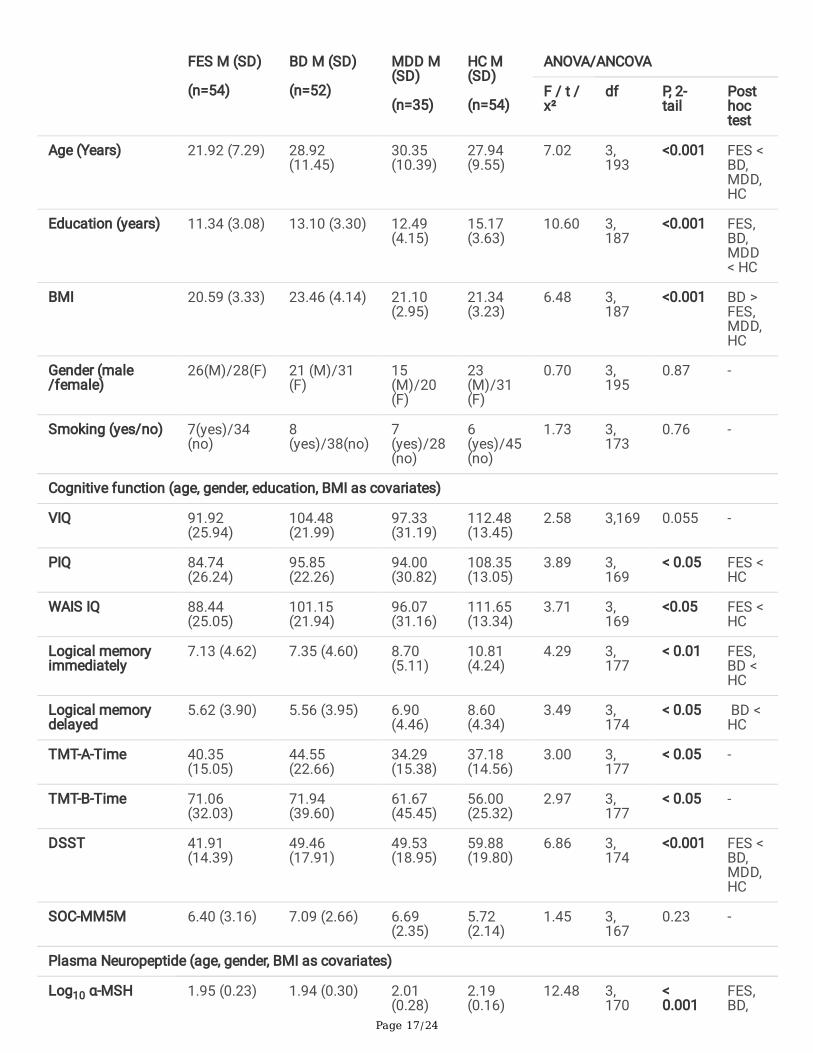
Demographic, clinical, plasma biomarkers, and cognitive features of patients and healthy controls are presented inTable 1. The FES group was younger than the other three groups. The BD group had a higher body mass index (BMI)compared to the other three groups. There were no gender differences between patients and controls. The threepatient groups had lower educational levels than the controls. Compared to FES and BD, the MDD group showedsigni�cantly increased HAMD scores. Because few MDD subjects were measured with YMRS, PANSS, and BPRS, weonly compared these symptom scores between FES and BD. The YMRS scores were signi�cantly higher in the BDgroup compared to the FES group. The PANSS total score and BPRS total score were signi�cantly increased in theFES group compared to the BD group. The BD group had a signi�cantly longer illness duration than the FES group.(See results in Table 1 and Supplementary Table 2)
Insert Table 1 here.
Cognitive function analysis
ANCOVA analysis indicated that there were signi�cant group differences in total IQ, and performance IQ, among theFES, BD, MDD, and HCs. Post-hoc analyses revealed decreased total IQ scores, and performance IQ scores in the FESpatient group compared to controls. There were no signi�cant differences in SOC-MM5M scores between thepatients and control groups. (See table 1)
Different patterns of plasma neuropeptides in the four subject groups
Controlling for age, gender, and BMI, the log10 α-MSH, log10 neurotensin, log10 orexin A, log10 oxytocin, and log10
substance P level were signi�cantly decreased in the three patient groups compared to controls. In addition, only theBD group showed decreased log10 β-endorphins compared to controls. We did not detect any signi�cant differencesbetween groups for six neuropeptides (See Table 1 and Figure 1).
Insert Figure 1 here
Page 7/24
Disease differentiating potential of plasma biomarkers
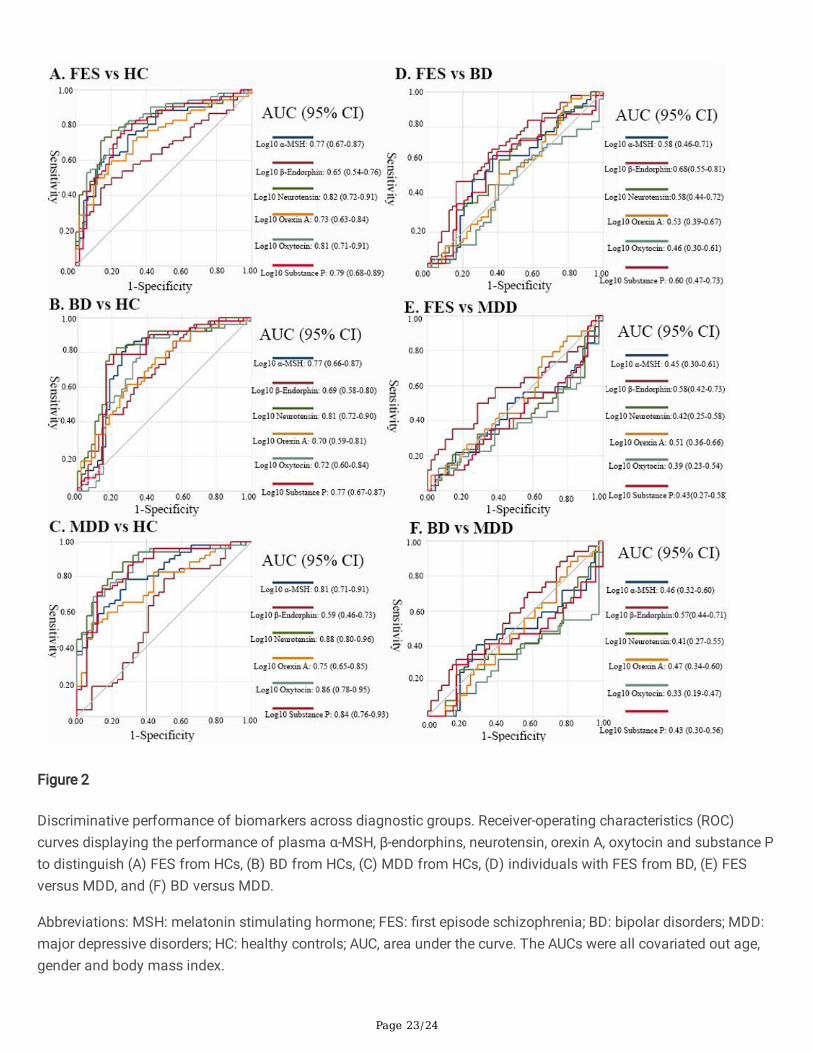
ROC curves demonstrating the differentiating potential of plasma neuropeptides are shown in Figure 2. Across allcomparisons, only patients compared with controls showed a good level of accuracy, and the differentiatingperformances between patient groups was poor. The highest AUC values were seen for plasma neurotensin whencomparing patients with controls; FES versus HC [AUC = 0.82, 95% con�dence interval [CI] 0.72-0.91; Figure 2A]; BDversus HC [AUC = 0.81, 95% CI 0.72-0.91; Figure 2B]; and MDD versus HC [AUC = 0.88, 95% CI 0.80-0.96; Figure 2C].Other AUCs for discriminating patients from controls which showed good levels of discrimination above 0.80included: oxytocin in FES vs HC [AUC = 0.88, 95% CI 0.80-0.96; Figure 2C]; oxytocin in MDD vs HC [AUC = 0.88, 95%CI 0.80-0.96; Figure 2C]; and a-MSH in MDD vs HC [AUC = 0.88, 95% CI 0.80-0.96; Figure 2C]. For contrasts betweenpatient groups, the AUCs are relatively poor (Figure D, E, F). Using logistic regression, lower AIC values were onlyobserved for models with neurotensin compared to models combining all plasma biomarkers in FES vs HC—acrossthe six contrasts investigated in the ROC analyses (Supplementary Table 3).
Insert Figure 2 here
Association between plasma neuropeptides and executive function
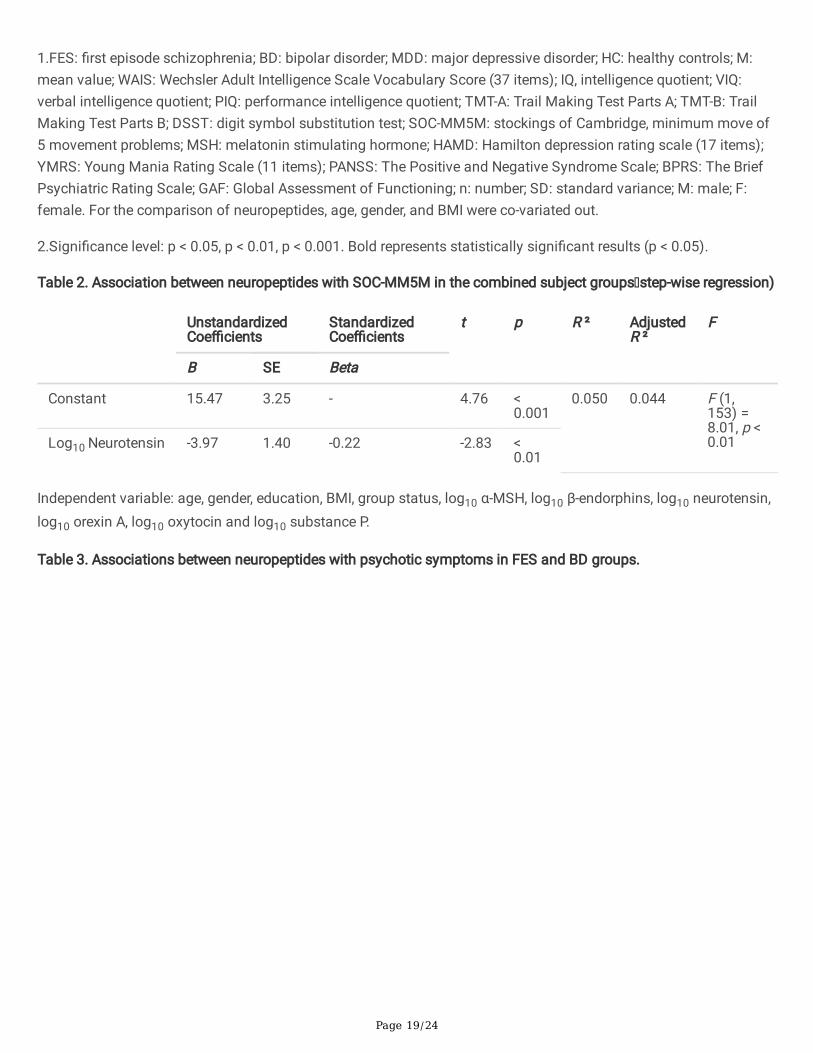
In the combined samples of the four groups, stepwise linear regression analysis using SOC-MM5M scores as thedependent variable and age, gender, education, BMI, group status, log10 α-MSH, log10 β-endorphins, log10
neurotensin, log10 orexin A, log10 oxytocin and log10 substance P as the independent variables showed that thelinear regression model was signi�cant (F1,153 = 8.01, P < 0.01). The adjusted multivariate coe�cient of
determination (R2) for the model was 0.050 for the predictor. The standardized β coe�cient value for neurotensinwas −0.22, with a t value of −2.83.
Insert Table 2 here.
Plasma neuropeptides were associated with psychotic symptoms in the FES and BD groups
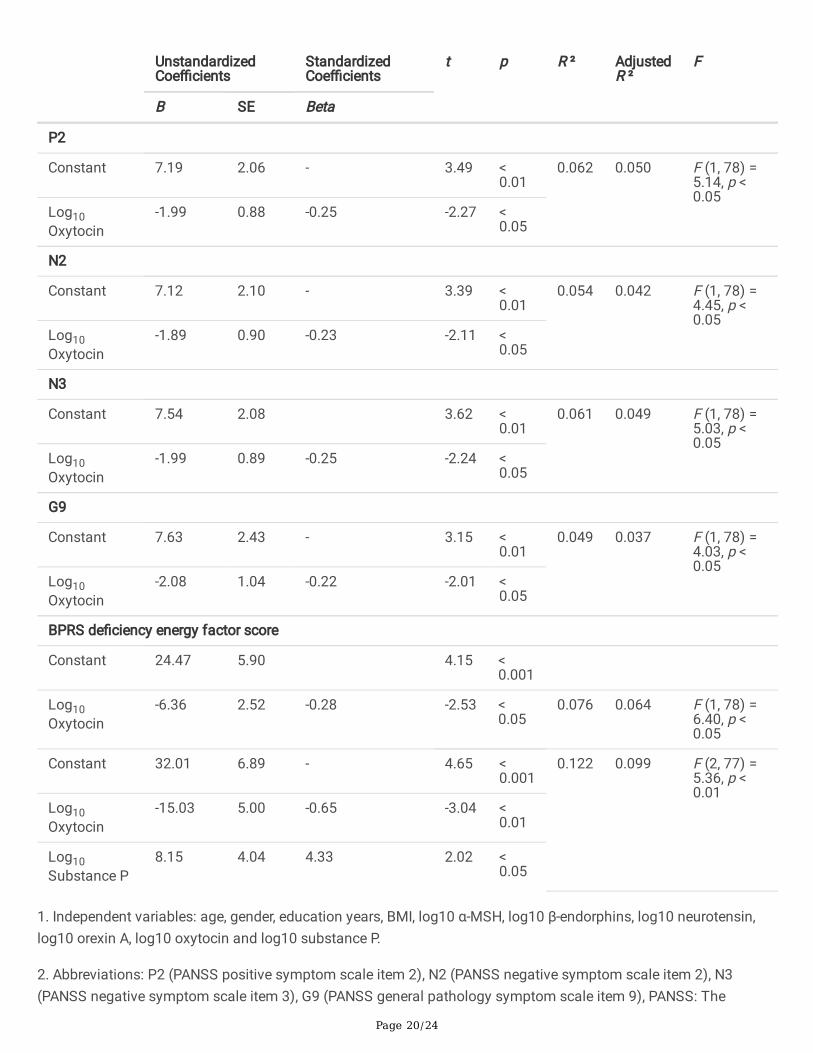
The summary of linear regression analyses for evaluating the relationships among PANSS subscales and BPRSfactor scores within FES and BD groups is presented in Table 2. When using age, gender, education, BMI, log10 α-MSH, log10 β-endorphins, log10 neurotensin, log10 orexin A, log10 oxytocin, and log10 substance P as the independentvariables, and P2 (positive symptom scale item 2), N2 (negative symptom scale item 2), N3 (negative symptomscale item 3), and G9 (general pathology symptom scale item 9) as independent variables, we found that theregression models were all signi�cant because all P values were all lower than 0.05. Oxytocin was the only variablethat could predict PANSS subscale symptom scores, with lower oxytocin levels predicting higher PANNSscores. When using the BPRS de�ciency energy factor score as the dependent variable, we found that oxytocin levelexplained a signi�cant amount of the variance in the BPRS de�ciency energy factor score in Step 1 (F = 6.40, p <0.05; R2 = 0.076; β = -0.28). In the second step, the inclusion of substance P (β = 4.33) enhanced the relationshipbetween BPRS de�ciency energy factor score and oxytocin level (β = -0.65) based on the magnitude of thestandardized beta-coe�cient in Step 2 (F = 5.36, p < 0.01; ΔR2 = 0.023). The adjusted multivariate coe�cient ofdetermination (R2) for the �nal model was 0.099 for the predictors. The standardized β coe�cient value for oxytocinand substance P were −0.65 and 4.33, with t values of −3.04 and 2.02 in step 2. (See results in Table 3)
Insert table 3 here.
Page 8/24
Plasma neuropeptide was associated with insomnia symptoms in all three psychiatric disorder groups
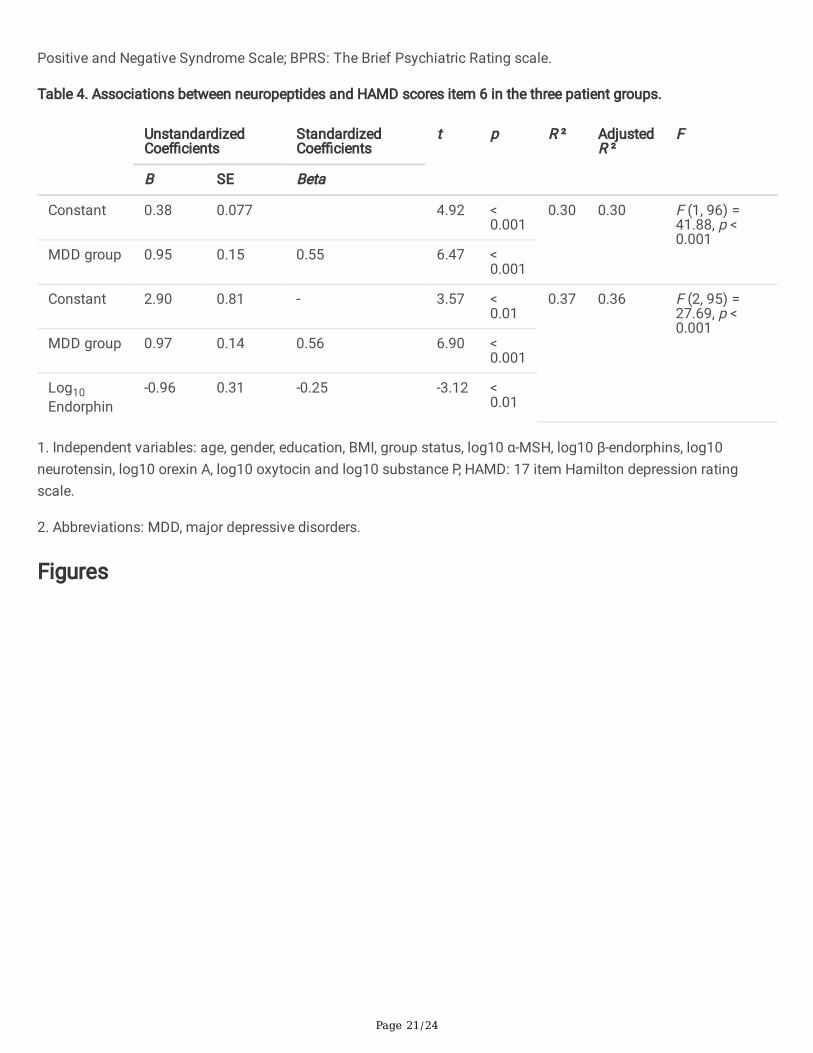
The summary of linear regression analyses for evaluating the relationships among depression severity, measured bythe HAMD-17 item 6 (which is a measurement of early morning wakening), in the three patient groups is presented inTable 4. MDD group status explained a signi�cant amount of the variance in early morning wakening severity inStep 1 (F = 41.88, p < 0.001; R2 = 0.30; β = 0.55). The inclusion of log10 endorphin (β = -0.25) enhanced therelationship between early morning awakening severity and MDD group status (β = 0.56) based on the magnitude ofthe standardized beta-coe�cient in Step 2 (F = 27.69, p < 0.001; ΔR2 = 0.06). The adjusted multivariate coe�cient ofdetermination (R2) in step 2 was 0.36 for the predictors. The standardized β coe�cient value for MDD group statusand log10 endorphin were 0.56 and -0.25, with t values of 6.90 and -3.12.
Insert Table 4 here.
Partial correlation between plasma neuropeptides and other clinical information
We conducted correlation analyses between neuropeptides and illness duration, age of onset, mood episodes, anddrug usage in the three patient groups, separately, but did not �nd any signi�cant correlations in either FES or MDDgroup. However, in the BD group, we found plasma β-endorphin level was signi�cantly positively correlated withillness duration (r = 0.41, p < 0.01). (See results in Supplementary Table 4)
DiscussionIn this study, we found that plasma α-MSH, orexin-A, oxytocin, neurotensin, and substance P, were all signi�cantlydecreased in FES, BD, and MDD groups compared to controls. β-endorphins were only decreased in the BD groupcompared to controls. In contrast, there were no signi�cant differences observed among the three patient groups forsix plasma neuropeptides. Neurotensin was the only plasma biomarker that could provide a relatively highdifferentiating potential to distinguish FES, BD, and MDD from controls (AUC = 0.82, 0.81, and 0.88 respectively).Furthermore, we have demonstrated that the plasma neuropeptides were differentially associated with speci�cclinical symptoms and executive function across disease groups, which supports the validity of the dimensionalapproach. Our results indicate that the dimensional and categorical approaches are complementary inrepresentation of severe mental illnesses and the combination of categorical and dimensional classi�cation couldtherefore be used in clinical and research settings [43].
To our knowledge, this is the �rst study that has examined plasma α-MSH, β-endorphins, Orexin-A, Oxytocin,neurotensin, and substance P in three major psychiatric disorders compared with healthy controls. In our test of thedifferentiating performance of plasma neuropeptides, our �nding that neurotensin has a good differentiatingpotential between patient groups and controls, with AUCs above 0.80, is new. Neurotensin is an endogenoustridecapeptide neurotransmitter that is heterogeneously distributed within the mammalian central nervous system(CNS) and has close neuroanatomical, functional associations with the dopamine neurotransmitter system [18, 44].Research evidence has already identi�ed the role of neurotensin in the pathophysiology of psychosis and themechanism of action of antipsychotic drugs [45, 46]. Decreased CSF neurotensin concentration has been found inpatients with schizophrenia, and improvements in overall psychopathology, including positive and negativesymptoms, were correlated with increases in CSF neurotensin concentrations during treatment [45, 47]. Our study isconsistent with previous research and we �nd decreased neurotensin in �rst episode, never treated schizophreniapatients. There has been little previous investigation of the effects of neurotensin in BD and MDD. However, it wasreported that neurotensin receptor 2 (NTSR2) was decreased in the anterior cingulate cortex of BD [48]. NTSR2

Page 9/24
mRNA and NTSR2 binding were reported to be down-regulated in transgenic mice expressing anxiety, stress, anddepression [49]. Furthermore, neurotensin receptor 1 (Ntsr1) knockout mice also showed increased anxiety anddespair behaviors [50]. Our results may be consistent with the hypothesis that plasma peptide changes areconsistent across the major psychiatric disorders, as these disorders may have transdiagnostic properties [51].
In our correlation analysis, we found that the measurement of SOC-MM5M was negatively associated withneurotensin. Our results are consistent with the previous study in humans which showed NT genes variances wereassociated with working memory performance among healthy participants [52]. We expanded the associationresults to a larger spectrum of the human sample, which includes the FES, BD, MDD, and HCs. Evidence hasindicated that neurotensin is often co-released with dopamine, and dopamine is widely expressed in the frontal lobe[53]. As SOC-MM5M is a measurement of frontal lobe function [54], our results suggested that neurotensin mighthave the potential to in�uence frontal lobe function. However, further exploration is needed. Above all, our resultssupport the possibility that plasma neurotensin has a central role in cognitive function, and it has the potential to bethe treatment target for improving cognitive de�cit in severe mental illness.
We found decreased oxytocin in plasma levels in schizophrenia as well as mood disorder patients. CSF and plasmaoxytocin levels were found to be decreased in drug-naive schizophrenia patients and chronic schizophrenia patientsand showed increased levels with antipsychotics drug treatment [55]. Reduced plasma oxytocin concentrations wereobserved in patients with MDD and BD compared to controls [30, 56]. Our results are consistent with previouslypublished studies that reported decreased plasma oxytocin in schizophrenia, BD, and MDD [30, 55, 56]. Furthermore,we found oxytocin was negatively correlated with negative and positive symptom subscales in bipolar and FESpatients. Clinical studies have shown that nasal administration of oxytocin improves some symptoms ofschizophrenia [57]. Our results suggest that oxytocin plays a central role in the pathophysiology of major psychiatricillnesses, and increased oxytocin levels in FES and BD patients may help with the treatment of psychotic symptoms[14].
In our study, we only found decreased β-endorphin in the BD group compared with controls, and there were nodifferences between FES or MDD and controls. Few studies have explored endorphin levels in BD, although a singleelectroconvulsive therapy (ECT) study reported that after ECT treatment, the patient group had signi�cantlyincreased endorphin levels [58]. We found that a core symptom of depression, early-morning wakefulness ofinsomnia, was negatively associated with β-endorphin. Because insomnia is one of the most common symptoms ofpsychiatric illness, and a previous study has reported that electroacupuncture induced sleep enhancement may bemediated, in part, by increasing the concentrations of β-endorphin [59]. Our �nding is therefore consistent with β-endorphin having a role in the pathophysiology of insomnia symptoms in major psychiatric illnesses.
We also found decreased Orexin A, α-MSH, and Substance P across the three patient groups, and these threeneuropeptides could discriminate patients from controls with modest accuracy (between 0.7–0.8). Loss of orexinneurons and decrease of orexin levels in plasma are observed in patients with depression, schizophrenia, and otherneurodegenerative diseases [26, 60, 61]. Our results may indicate that altered orexin-A signaling was disrupted inschizophrenia, BD, and MDD. α-MSH is one cleavage product of the pituitary hormone pro-opiomelanocortin (POMC),and numerous studies have described the role of POMC in metabolic syndrome [60]. Psychopharmacotherapystrongly impacts the metabolic system, in particular in schizophrenia and bipolar disorders [62]. As one of POMC’sdownstream effector hormones, decreased α-MSH may be a potential risk factor for metabolic syndrome in severalmental illnesses. We found that substance P was positively correlated with psychotic symptoms in FES and BD.Based on the fact that SP-containing neurons synapse with dopaminergic neurons in the midbrain, and that
Page 10/24
application of SP agonists in animal studies lead to increased dopaminergic turnover and locomotor activity [63–65], our results suggested that abnormal SP neurotransmission may be involved in the etiopathology of psychosis.
There are several limitations that need to be addressed. The �rst limitation of the study is that it remains unclearwhether plasma neuropeptide levels correlate with brain levels of neuropeptides because of the blood-brain barrier.In our study, we showed that plasma neuropeptides are correlated with cognitive function, psychotic and depressivesymptoms. This may indicate that circulating neuropeptides can re�ect the neuropeptide in the central nervoussystem [30]. The second limitation is that drug treatment may confound our results, as BD and MDD groups werepreviously medicated. Although we also did not detect any signi�cant correlation between drug usage andneuropeptide measurements, further studies must include �rst episode and drug naïve BD and MDD patients. Finally,the cross-sectional design of this study will not provide evidence of causality, and without longitudinal data, it is notpossible to establish a true cause and effect relationship [66]. We, therefore suggest that longitudinal observation ofchanges of neuropeptides in severe mental illness should be conducted in future research.
ConclusionIn conclusion, this is the �rst study to explore six neuropeptides, including α-MSH, β-Endorphin, Neurotensin, Orexin-A, Oxytocin, and Substance P, differences in FES, BD, and MDD, and their differentiating potential to distinguishdisease states. It is also the �rst to explore the relationship between plasma neuropeptide levels and psychotic,depressive symptoms, and executive function in FES, BD and MDD groups. If our results are con�rmed in furtherlarge-scale longitudinal studies, plasma neuropeptides, especially neurotensin, could help in the diagnosis of severemental disorders. We also con�rmed that plasma neuropeptides showed transdiagnostic change across three severemental illnesses, and these neuropeptides may be promising targets for treating clinical symptoms and cognitivede�cits. In summary, our results suggest the categorical and dimensional classi�cation of severe mental illnessshould therefore be used synergistically in future clinical and research settings [10].
AbbreviationsSchizophrenia, SCZ; �rst-episode schizophrenia, FES; BD: bipolar disorder; MDD: major depressivedisorder; Statistical Manual of Mental Disorders, DSM; γ-aminobutyric acid, GABA; G protein-coupled receptors,GPCRs; cerebral spinal �uid, CSF; neurotensin, NT; cerebral spinal �uid, CSF; neurotensin, NT; Brief PsychiatricRating Scale, BPRS; Young Mania Rating Scale, YMRS; 17-item Hamilton Depression Rating Scale, HAMD-17; Intelligence quotient, IQ; Cambridge Neuropsychological Test Automated Battery, CANTAB; Stockings ofCambridge, SOC; minimum moves for 5-move problems, MM5M; area under the curve, AUC; values from receiveroperating characteristic, ROC; body mass index, BMI; Akaike information criterion, AIC; substance p, SP; con�denceinterval, CI; Neurotensin receptor 1 gene, NTSR1; melanocyte-stimulating hormone, MSH.
DeclarationsAcknowledgement
The authors would like to thank all their coworkers at the A�liated Mental Health Centre & Hangzhou SeventhPeople’s Hospital, West China Hospital, the State Key Laboratory of Biotherapy in West China Hospital and SuzhouPsychiatry Hospital for their contributions to this research study.
Authors’ contributions
Page 11/24
H.Y., P.N., J.C., and T.L. developed the study, had full access to all data, and take responsibility for data integrity andaccuracy. H.Y., P.N., Q.W., and W.G. drafted the manuscript. W.W., J.W., X.D., W.D., and X.M. collected the data, andY.T., L.Z., M.L., and X.L. performed all data analyses. All authors agree to be accountable for all aspects of the work,ensuring that questions related to the accuracy or integrity of the data and results are appropriately investigated andresolved. All authors critically revised and approved the �nal version of the manuscript.
Funding
This work was supported by the National Natural Science Foundation of China Key Project (81630030 and81920108018 to T.L.), National Natural Science Foundation of China (81871054 and 81501159 to P.N., 82101598 toH.Y.), Post-Doctoral Research Project, West China Hospital, Sichuan University (2021HXBH034 to H.Y.), SpecialFoundation for Brain Research from Science and Technology Program of Guangdong (2018B030334001 to T.L.),2021 Project for Hangzhou Medical Disciplines of Excellence & Key Project for Hangzhou Medical Disciplines, 1.3.5Project for Disciplines of Excellence at West China Hospital of Sichuan University (ZY2016103, ZY2016203, andZYGD20004 to T.L.), and Introductory Project of the Suzhou Clinical Expert Team (SZYJTD201715 to X.D. and T.L.).
Availability of data and materials
All data used in the current study are available from the corresponding author on reasonable request. Because ofrestrictions based on privacy regulations and informed consent of participants, data cannot be made freelyavailable in a public repository.
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of West China Hospital, Sichuan University, and it complied withthe principles of the Declaration of Helsinki. All participants received a complete description of the study andprovided written informed consent. A copy of the written consent is available for review by the Editor of this journal.
Consent for publicationNot applicable.
Declaration of competing interest
The authors have declared that there are no con�icts of interest in relation to the subject of this study.
Author information
Hua Yu and Peiyan Ni contributed equally to this work
A�liations
Department of Neurobiology, A�liated Mental Health Center & Hangzhou Seventh People's Hospital, ZhejiangUniversity School of Medicine, Hangzhou, Zhejiang, China
Hua Yu, Wei Wei, Xiaojing Li, Wanjun Guo, Wei Deng, Tao Li
Page 12/24
NHC and CAMS Key Laboratory of Medical Neurobiology, MOE Frontier Science Center for Brain Science and Brain-machine Integration, School of Brain Science and Brain Medicine, Zhejiang University, Hangzhou, Zhejiang, China
Hua Yu, Wei Wei, Xiaojing Li, Wanjun Guo, Wei Deng, Tao Li
The Psychiatric Laboratory and Mental Health Center, West China Hospital, Sichuan University, Chengdu, Sichuan, PR China.
Hua Yu, Peiyan Ni, Yang Tian, Liansheng Zhao, Mingli Li, Xiaojing Li, Wei Wei, Jinxue Wei, Qiang Wang, Wanjun Guo,Xiaohong Ma, Jeremy Coid.
Suzhou Psychiatry Hospital, A�liated Guangji Hospital of Soochow University, Suzhou, Jiangsu, China
Xiangdong Du
Corresponding author
Correspondence to Tao Li.
References1. Chong HY, Teoh SL, Wu DB, Kotirum S, Chiou CF, Chaiyakunapruk N: Global economic burden of schizophrenia:
a systematic review. Neuropsychiatr Dis Treat 2016, 12:357–373.
2. Walker ER, McGee RE, Druss BG: Mortality in mental disorders and global disease burden implications: asystematic review and meta-analysis. JAMA psychiatry 2015, 72(4):334–341.
3. Yang Y, Liu S, Jiang X, Yu H, Ding S, Lu Y, Li W, Zhang H, Liu B, Cui Y et al: Common and Speci�c FunctionalActivity Features in Schizophrenia, Major Depressive Disorder, and Bipolar Disorder. Frontiers in psychiatry2019, 10:52.
4. Parker G: The DSM-5 classi�cation of mood disorders: some fallacies and fault lines. Acta Psychiatr Scand2014, 129(6):404–409.
5. Owen MJ, Sawa A, Mortensen PB: Schizophrenia. Lancet (London, England) 2016, 388(10039):86–97.
�. Calabrò M, Porcelli S, Crisafulli C, Albani D, Kasper S, Zohar J, Souery D, Montgomery S, Mantovani V,Mendlewicz J et al: Genetic variants associated with psychotic symptoms across psychiatric disorders.Neuroscience letters 2020, 720:134754.
7. Batinic B, Ristic I, Zugic M, Baldwin DS: Treatment of Symptom Clusters in Schizophrenia, Bipolar Disorder andMajor Depressive Disorder With the Dopamine D3/D2 Preferring Partial Agonist Cariprazine. Frontiers inpsychiatry 2021, 12:784370.
�. Barron DS, Gao S, Dadashkarimi J, Greene AS, Spann MN, Noble S, Lake EMR, Krystal JH, Constable RT,Scheinost D: Transdiagnostic, Connectome-Based Prediction of Memory Constructs Across PsychiatricDisorders. Cereb Cortex 2020.
9. Opel N, Goltermann J, Hermesdorf M, Berger K, Baune BT, Dannlowski U: Cross-Disorder Analysis of BrainStructural Abnormalities in Six Major Psychiatric Disorders: A Secondary Analysis of Mega- and Meta-analyticalFindings From the ENIGMA Consortium. Biol Psychiatry 2020, 88(9):678–686.
10. Potuzak M, Ravichandran C, Lewandowski KE, Ongür D, Cohen BM: Categorical vs dimensional classi�cationsof psychotic disorders. Compr Psychiatry 2012, 53(8):1118–1129.
Page 13/24
11. Nakamura S: Integrated pathophysiology of schizophrenia, major depression, and bipolar disorder asmonoamine axon disorder. 2022, 14(1).
12. Zhang JP, Lencz T, Zhang RX, Nitta M, Maayan L, John M, Robinson DG, Fleischhacker WW, Kahn RS, Ophoff RAet al: Pharmacogenetic Associations of Antipsychotic Drug-Related Weight Gain: A Systematic Review andMeta-analysis. Schizophr Bull 2016, 42(6):1418–1437.
13. Brigitta B: Pathophysiology of depression and mechanisms of treatment. Dialogues in clinical neuroscience2002, 4(1):7–20.
14. Goh KK, Chen C-H, Lane H-Y: Oxytocin in Schizophrenia: Pathophysiology and Implications for FutureTreatment. Int J Mol Sci 2021, 22(4):2146.
15. Carlsson A, Waters N, Holm-Waters S, Tedroff J, Nilsson M, Carlsson ML: Interactions Between Monoamines,Glutamate, and GABA in Schizophrenia: New Evidence. Annual Review of Pharmacology and Toxicology 2001,41(1):237–260.
1�. Gitlin MJ, Swendsen J, Heller TL, Hammen C: Relapse and impairment in bipolar disorder. Am J Psychiatry1995, 152(11):1635–1640.
17. Barde S, Rüegg J, Prud’homme J, Ekström TJ, Palkovits M, Turecki G, Bagdy G, Ihnatko R, Theodorsson E,Juhasz G et al: Alterations in the neuropeptide galanin system in major depressive disorder involve levels oftranscripts, methylation, and peptide. Proceedings of the National Academy of Sciences 2016, 113(52):E8472.
1�. Griebel G, Holsboer F: Neuropeptide receptor ligands as drugs for psychiatric diseases: the end of thebeginning? Nature reviews Drug discovery 2012, 11(6):462–478.
19. Baldessarini RJ, Tondo L, Baethge CJ, Lepri B, Bratti IM: Effects of treatment latency on response tomaintenance treatment in manic-depressive disorders. Bipolar Disorders 2007, 9(4):386–393.
20. Cáceda R, Kinkead B, Nemeroff CB: Involvement of Neuropeptide Systems in Schizophrenia: Human Studies. In:International review of neurobiology. Volume 78, edn.: Academic Press; 2007: 327–376.
21. Ni P, Tian Y, Gu X, Yang L, Wei J, Wang Y, Zhao L, Zhang Y, Zhang C, Li L et al: Plasma neuropeptides ascirculating biomarkers of multifactorial schizophrenia. Compr Psychiatry 2019, 94:152114.
22. Hökfelt T, Barde S, Xu Z-QD, Kuteeva E, Rüegg J, Le Maitre E, Risling M, Kehr J, Ihnatko R, Theodorsson E et al:Neuropeptide and Small Transmitter Coexistence: Fundamental Studies and Relevance to Mental Illness.Frontiers in Neural Circuits 2018, 12:106.
23. Nestler EJ, Hyman SE, Holtzman DM, Malenka RC: Neuropeptides. In: Molecular Neuropharmacology: AFoundation for Clinical Neuroscience, 3e. edn. New York, NY: McGraw-Hill Education; 2015.
24. de Wied D, Sigling HO: Neuropeptides Involved in the Pathophysiology of Schizophrenia and Major Depression.Neurotoxicity Research 2002, 4(5–6):453–468.
25. Wang M, Ma H, Huang YL, Zhu G, Zhao JP: Association of Neurotensin receptor 1 gene polymorphisms withprocessing speed in healthy Chinese-Han subjects. Journal of molecular neuroscience: MN 2014, 54(4):787–789.
2�. LaCrosse AL, Olive MF: Neuropeptide systems and schizophrenia. CNS & neurological disorders drug targets2013, 12(5):619–632.
27. Beckmann H, Lang RE, Gattaz WF: Vasopressin–oxytocin in cerebrospinal �uid of schizophrenic patients andnormal controls. In., vol. 10. Netherlands: Elsevier Science; 1985: 187–191.
2�. Glovinsky D, Kalogeras KT, Kirch DG, Suddath R, Wyatt RJ: Cerebrospinal �uid oxytocin concentration inschizophrenic patients does not differ from control subjects and is not changed by neuroleptic medication.
Page 14/24
Schizophr Res 1994, 11(3):273–276.
29. Pedersen CA, Gibson CM, Rau SW, Salimi K, Smedley KL, Casey RL, Leserman J, Jarskog LF, Penn DL: Intranasaloxytocin reduces psychotic symptoms and improves Theory of Mind and social perception in schizophrenia.Schizophr Res 2011, 132(1):50–53.
30. Cochran DM, Fallon D, Hill M, Frazier JA: The role of oxytocin in psychiatric disorders: a review of biological andtherapeutic research �ndings. Harv Rev Psychiatry 2013, 21(5):219–247.
31. Kormos V, Gaszner B: Role of neuropeptides in anxiety, stress, and depression: from animals to humans.Neuropeptides 2013, 47(6):401–419.
32. Kokare DM, Dandekar MP, Singru PS, Gupta GL, Subhedar NK: Involvement of alpha-MSH in the social isolationinduced anxiety- and depression-like behaviors in rat. Neuropharmacology 2010, 58(7):1009–1018.
33. Pilozzi A, Carro C, Huang X: Roles of β-Endorphin in Stress, Behavior, Neuroin�ammation, and Brain EnergyMetabolism. International journal of molecular sciences 2020, 22(1).
34. Hegadoren KM, O'Donnell T, Lanius R, Coupland NJ, Lacaze-Masmonteil N: The role of beta-endorphin in thepathophysiology of major depression. Neuropeptides 2009, 43(5):341–353.
35. Nemeroff CB, Bissette G: Neuropeptides, dopamine, and schizophrenia. Annals of the New York Academy ofSciences 1988, 537:273–291.
3�. Simrén J, Leuzy A, Karikari TK, Hye A, Benedet AL, Lantero-Rodriguez J, Mattsson-Carlgren N, Schöll M, MecocciP, Vellas B et al: The diagnostic and prognostic capabilities of plasma biomarkers in Alzheimer's disease.Alzheimer's & dementia: the journal of the Alzheimer's Association 2021, 17(7):1145–1156.
37. Lee RS, Hermens DF, Naismith SL, Lagopoulos J, Jones A, Scott J, Chitty KM, White D, Robillard R, Scott EM etal: Neuropsychological and functional outcomes in recent-onset major depression, bipolar disorder andschizophrenia-spectrum disorders: a longitudinal cohort study. Transl Psychiatry 2015, 5(4):e555.
3�. Huang Y-C, Lee Y, Lee C-Y, Lin P-Y, Hung C-F, Lee S-Y, Wang L-J: De�ning cognitive and functional pro�les inschizophrenia and affective disorders. BMC psychiatry 2020, 20(1):39–39.
39. Wechsler D: WAIS-R Manual: Wechsler Adult Intelligence Scale-revised: Psychological Corporation; 1981.
40. Green R, Till C, Al-Hakeem H, Cribbie R, Téllez-Rojo MM, Osorio E, Hu H, Schnaas L: Assessment ofneuropsychological performance in Mexico City youth using the Cambridge Neuropsychological TestAutomated Battery (CANTAB). Journal of clinical and experimental neuropsychology 2019, 41(3):246–256.
41. Chan MK, Krebs MO, Cox D, Guest PC, Yolken RH, Rahmoune H, Rothermundt M, Steiner J, Leweke FM, vanBeveren NJM et al: Development of a blood-based molecular biomarker test for identi�cation of schizophreniabefore disease onset. Translational Psychiatry 2015, 5(7):e601-e601.
42. Akaike H: Information Theory and an Extension of the Maximum Likelihood Principle. In: Selected Papers ofHirotugu Akaike. edn. Edited by Parzen E, Tanabe K, Kitagawa G. New York, NY: Springer New York; 1998: 199–213.
43. Demjaha A, Morgan K, Morgan C, Landau S, Dean K, Reichenberg A, Sham P, Fearon P, Hutchinson G, Jones PBet al: Combining dimensional and categorical representation of psychosis: the way forward for DSM-V and ICD-11? Psychol Med 2009, 39(12):1943–1955.
44. Panksepp J, Harro J: Future of neuropeptides in biological psychiatry and emotional psychopharmacology:Goals and strategies. In: Textbook of biological psychiatry. edn. New York, NY, US: Wiley-Liss; 2004: 627–659.
45. Sharma RP, Janicak PG, Bissette G, Nemeroff CB: CSF neurotensin concentrations and antipsychotic treatmentin schizophrenia and schizoaffective disorder. The American journal of psychiatry 1997, 154(7):1019–1021.
Page 15/24
4�. Widerlöv E, Lindström LH, Besev G, Manberg PJ, Nemeroff CB, Breese GR, Kizer JS, Prange AJ, Jr.: SubnormalCSF levels of neurotensin in a subgroup of schizophrenic patients: normalization after neuroleptic treatment.Am J Psychiatry 1982, 139(9):1122–1126.
47. Cáceda R, Kinkead B, Nemeroff CB: Involvement of neuropeptide systems in schizophrenia: human studies.International review of neurobiology 2007, 78:327–376.
4�. Tomita H, Ziegler ME, Kim HB, Evans SJ, Choudary PV, Li JZ, Meng F, Dai M, Myers RM, Neal CR et al: G protein-linked signaling pathways in bipolar and major depressive disorders. Frontiers in genetics 2013, 4:297.
49. Peeters PJ, Fierens FL, van den Wyngaert I, Goehlmann HW, Swagemakers SM, Kass SU, Langlois X, Pullan S,Stenzel-Poore MP, Steckler T: Gene expression pro�les highlight adaptive brain mechanisms in corticotropinreleasing factor overexpressing mice. Brain research Molecular brain research 2004, 129(1–2):135–150.
50. Fitzpatrick K, Winrow CJ, Gotter AL, Millstein J, Arbuzova J, Brunner J, Kasarskis A, Vitaterna MH, Renger JJ,Turek FW: Altered sleep and affect in the neurotensin receptor 1 knockout mouse. Sleep 2012, 35(7):949–956.
51. Zhu Y, Womer FY, Leng H, Chang M, Yin Z, Wei Y, Zhou Q, Fu S, Deng X, Lv J et al: The Relationship BetweenCognitive Dysfunction and Symptom Dimensions Across Schizophrenia, Bipolar Disorder, and Major DepressiveDisorder. Frontiers in Psychiatry 2019, 10:253.
52. Li J, Chen C, Chen C, He Q, Li H, Li J, Moyzis RK, Xue G, Dong Q: Neurotensin receptor 1 gene (NTSR1)polymorphism is associated with working memory. PLoS One 2011, 6(3):e17365.
53. Petrie KA, Schmidt D, Bubser M, Fadel J, Carraway RE, Deutch AY: Neurotensin activates GABAergic interneuronsin the prefrontal cortex. The Journal of neuroscience: the o�cial journal of the Society for Neuroscience 2005,25(7):1629–1636.
54. Robbins TW, James M, Owen AM, Sahakian BJ, Lawrence AD, McInnes L, Rabbitt PM: A study of performanceon tests from the CANTAB battery sensitive to frontal lobe dysfunction in a large sample of normal volunteers:implications for theories of executive functioning and cognitive aging. Cambridge Neuropsychological TestAutomated Battery. Journal of the International Neuropsychological Society: JINS 1998, 4(5):474–490.
55. Sasayama D, Hattori K, Teraishi T, Hori H, Ota M, Yoshida S, Arima K, Higuchi T, Amano N, Kunugi H: Negativecorrelation between cerebrospinal �uid oxytocin levels and negative symptoms of male patients withschizophrenia. Schizophr Res 2012, 139(1–3):201–206.
5�. Ozsoy S, Esel E, Kula M: Serum oxytocin levels in patients with depression and the effects of gender andantidepressant treatment. Psychiatry Res 2009, 169(3):249–252.
57. Matsuzaki M, Matsushita H, Tomizawa K, Matsui H: Oxytocin: a therapeutic target for mental disorders. Thejournal of physiological sciences: JPS 2012, 62(6):441–444.
5�. Chaudhry HR, Hofmann P, Loimer N, Kotter M, Quehenberger F, Fueger G: Prolactin and beta-endorphin serumelevations after ECT in manic patients. Acta Psychiatr Scand 2000, 102(5):386–389.
59. Cheng CH, Yi PL, Lin JG, Chang FC: Endogenous opiates in the nucleus tractus solitarius mediateelectroacupuncture-induced sleep activities in rats. Evidence-based complementary and alternative medicine:eCAM 2011, 2011:159209.
�0. Tsuchimine S, Hattori K, Ota M, Hidese S, Teraishi T, Sasayama D, Hori H, Noda T, Yoshida S, Yoshida F et al:Reduced plasma orexin-A levels in patients with bipolar disorder. Neuropsychiatr Dis Treat 2019, 15:2221–2230.
�1. Chen Q, de Lecea L, Hu Z, Gao D: The hypocretin/orexin system: an increasingly important role inneuropsychiatry. Medicinal research reviews 2015, 35(1):152–197.
Page 16/24
�2. Raue S, Wedekind D, Wiltfang J, Schmidt U: The Role of Proopiomelanocortin and α-Melanocyte-StimulatingHormone in the Metabolic Syndrome in Psychiatric Disorders: A Narrative Mini-Review. Front Psychiatry 2019,10:834.
�3. Blomeley C, Bracci E: Substance P depolarizes striatal projection neurons and facilitates their glutamatergicinputs. The Journal of physiology 2008, 586(8):2143–2155.
�4. Roberts GW, Ferrier IN, Lee Y, Crow TJ, Johnstone EC, Owens DG, Bacarese-Hamilton AJ, McGregor G,O'Shaughnessey D, Polak JM et al: Peptides, the limbic lobe and schizophrenia. Brain research 1983, 288(1–2):199–211.
�5. Trépanier MO, Hopperton KE, Mizrahi R, Mechawar N, Bazinet RP: Postmortem evidence of cerebralin�ammation in schizophrenia: a systematic review. Mol Psychiatry 2016, 21(8):1009–1026.
��. Carlson MD, Morrison RS: Study design, precision, and validity in observational studies. Journal of palliativemedicine 2009, 12(1):77–82.
TablesTable 1. Demographic and clinical characteristics of FES, BD, MDD and HC.
Page 17/24
FES M (SD)
(n=54)
BD M (SD)
(n=52)
MDD M(SD)
(n=35)
HC M(SD)
(n=54)
ANOVA/ANCOVA
F / t /x²
df P, 2-tail
Posthoctest
Age (Years) 21.92 (7.29) 28.92(11.45)
30.35(10.39)
27.94(9.55)
7.02 3,193
<0.001 FES <BD,MDD,HC
Education (years) 11.34 (3.08) 13.10 (3.30) 12.49(4.15)
15.17(3.63)
10.60 3,187
<0.001 FES,BD,MDD< HC
BMI 20.59 (3.33) 23.46 (4.14) 21.10(2.95)
21.34(3.23)
6.48 3,187
<0.001 BD >FES,MDD,HC
Gender (male/female)
26(M)/28(F) 21 (M)/31(F)
15(M)/20(F)
23(M)/31(F)
0.70 3,195
0.87 -
Smoking (yes/no) 7(yes)/34(no)
8(yes)/38(no)
7(yes)/28(no)
6(yes)/45(no)
1.73 3,173
0.76 -
Cognitive function (age, gender, education, BMI as covariates)
VIQ 91.92(25.94)
104.48(21.99)
97.33(31.19)
112.48(13.45)
2.58 3,169 0.055 -
PIQ 84.74(26.24)
95.85(22.26)
94.00(30.82)
108.35(13.05)
3.89 3,169
< 0.05 FES <HC
WAIS IQ 88.44(25.05)
101.15(21.94)
96.07(31.16)
111.65(13.34)
3.71 3,169
<0.05 FES <HC
Logical memoryimmediately
7.13 (4.62) 7.35 (4.60) 8.70(5.11)
10.81(4.24)
4.29 3,177
< 0.01 FES,BD <HC
Logical memorydelayed
5.62 (3.90) 5.56 (3.95) 6.90(4.46)
8.60(4.34)
3.49 3,174
< 0.05 BD <HC
TMT-A-Time 40.35(15.05)
44.55(22.66)
34.29(15.38)
37.18(14.56)
3.00 3,177
< 0.05 -
TMT-B-Time 71.06(32.03)
71.94(39.60)
61.67(45.45)
56.00(25.32)
2.97 3,177
< 0.05 -
DSST 41.91(14.39)
49.46(17.91)
49.53(18.95)
59.88(19.80)
6.86 3,174
<0.001 FES <BD,MDD,HC
SOC-MM5M 6.40 (3.16) 7.09 (2.66) 6.69(2.35)
5.72(2.14)
1.45 3,167
0.23 -
Plasma Neuropeptide (age, gender, BMI as covariates)
Log10 α-MSH 1.95 (0.23) 1.94 (0.30) 2.01(0.28)
2.19(0.16)
12.48 3,170
<0.001
FES,BD,
Page 18/24
MDD<HC
Log10 β-Endorphin 2.63 (0.18) 2.57 (0.26) 2.62(0.22)
2.69(0.16)
3.18 3,184
< 0.05 BD <HC
Log10 Neurotensin 2.24 (0.14) 2.25 (0.17) 2.20(0.13)
2.41(0.12)
19.27 3,184
<0.001
FES,BD,MDD< HC
Log10 Orexin A 2.78 (0.10) 2.81 (0.13) 2.78(0.091)
2.88(0.11)
7.61 3,184
<0.001
FES,BD,MDD< HC
Log10 Oxytocin 2.28 (0.18) 2.37 (0.22) 2.23(0.18)
2.48(0.16)
14.75 3,176
<0.001
FES,BD,MDD< HC
Log10 SubstanceP
1.52 (0.23) 1.55 (0.28) 1.45(0.23)
1.74(0.19)
12.96 3,181
<0.001
FES,BD,MDD< HC
Clinical parameters
HAMD total score 7.03 (5.12) 10.70 (8.03) 21.81(5.50)
- 45.56 2,112
<0.001
FES <BD <MDD
YMRS total score 5.00 (6.01) 10.07(11.31)
- - -2.25 74 0.027 FES <BD
PANSS 86.24(18.99)
54.09(20.71)
- - 7.64 87 <0.001
FES >BD
BPRS 46.70 (9.78) 32.30(11.76)
- - 2.39 87 <0.001
FES >BD
GAF 45.77(12.80)
54.11(13.63)
53.10(10.05)
- 5.89 2,122
< 0.01 FES <BD,MD
Age �rst episode(years)
21.17 (7.44) 24.04(10.03)
27.21(11.20)
- 3.68 2,120
< 0.05 FES <MDD
Duration of illness(months)
12.79(21.40)
65.45(64.07)
39.21(55.80)
- 11.03
2,116
<0.001
FES <BD
Depressiveepisode
- 2.22 (1.48) 1.77(1.07)
- 1.43 69 0.16 -
Manic/hypomanicepisode
- 1.98 (1.64) - - - - - -
Antidepressants(Yes/No)
- 24/28 18/16 - 0.38 1, 86 0.54 -
Mood stabilizers(Yes/No)
- 32/20 - - - - - -
Antipsychotics(Yes/No)
- 30/22 3/32 21.40 1, 87 <0.001
BD >MDD
Page 19/24
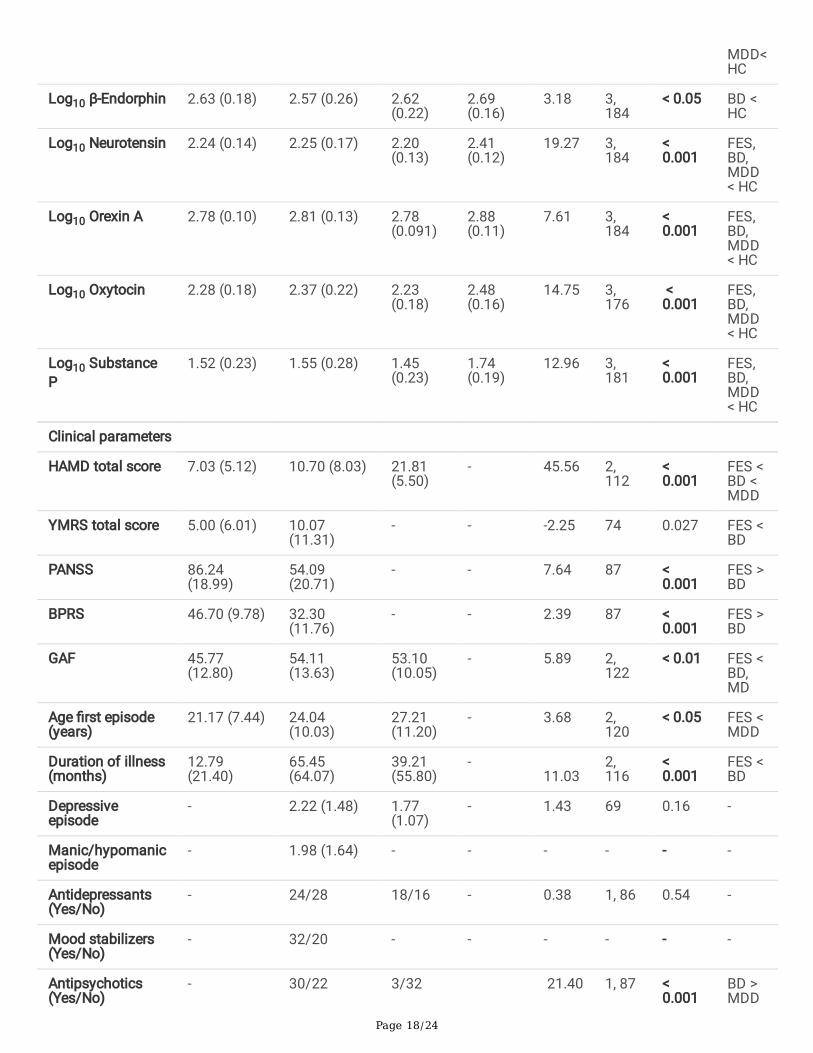
1.FES: �rst episode schizophrenia; BD: bipolar disorder; MDD: major depressive disorder; HC: healthy controls; M:mean value; WAIS: Wechsler Adult Intelligence Scale Vocabulary Score (37 items); IQ, intelligence quotient; VIQ:verbal intelligence quotient; PIQ: performance intelligence quotient; TMT-A: Trail Making Test Parts A; TMT-B: TrailMaking Test Parts B; DSST: digit symbol substitution test; SOC-MM5M: stockings of Cambridge, minimum move of5 movement problems; MSH: melatonin stimulating hormone; HAMD: Hamilton depression rating scale (17 items);YMRS: Young Mania Rating Scale (11 items); PANSS: The Positive and Negative Syndrome Scale; BPRS: The BriefPsychiatric Rating Scale; GAF: Global Assessment of Functioning; n: number; SD: standard variance; M: male; F:female. For the comparison of neuropeptides, age, gender, and BMI were co-variated out.
2.Signi�cance level: p < 0.05, p < 0.01, p < 0.001. Bold represents statistically signi�cant results (p < 0.05).
Table 2. Association between neuropeptides with SOC-MM5M in the combined subject groups step-wise regression)
UnstandardizedCoe�cients
StandardizedCoe�cients
t p R ² AdjustedR ²
F
B SE Beta
Constant 15.47 3.25 - 4.76 <0.001
0.050 0.044 F (1,153) =8.01, p <0.01Log10 Neurotensin -3.97 1.40 -0.22 -2.83 <
0.01
Independent variable: age, gender, education, BMI, group status, log10 α-MSH, log10 β-endorphins, log10 neurotensin,log10 orexin A, log10 oxytocin and log10 substance P.
Table 3. Associations between neuropeptides with psychotic symptoms in FES and BD groups.
Page 20/24
UnstandardizedCoe�cients
StandardizedCoe�cients
t p R ² AdjustedR ²
F
B SE Beta
P2
Constant 7.19 2.06 - 3.49 <0.01
0.062 0.050 F (1, 78) =5.14, p <0.05
Log10Oxytocin
-1.99 0.88 -0.25 -2.27 <0.05
N2
Constant 7.12 2.10 - 3.39 <0.01
0.054 0.042 F (1, 78) =4.45, p <0.05
Log10Oxytocin
-1.89 0.90 -0.23 -2.11 <0.05
N3
Constant 7.54 2.08 3.62 <0.01
0.061 0.049 F (1, 78) =5.03, p <0.05
Log10Oxytocin
-1.99 0.89 -0.25 -2.24 <0.05
G9
Constant 7.63 2.43 - 3.15 <0.01
0.049 0.037 F (1, 78) =4.03, p <0.05
Log10Oxytocin
-2.08 1.04 -0.22 -2.01 <0.05
BPRS de�ciency energy factor score
Constant 24.47 5.90 4.15 <0.001
Log10Oxytocin
-6.36 2.52 -0.28 -2.53 <0.05
0.076 0.064 F (1, 78) =6.40, p <0.05
Constant 32.01 6.89 - 4.65 <0.001
0.122 0.099 F (2, 77) =5.36, p <0.01
Log10Oxytocin
-15.03 5.00 -0.65 -3.04 <0.01
Log10Substance P
8.15 4.04 4.33 2.02 <0.05
1. Independent variables: age, gender, education years, BMI, log10 α-MSH, log10 β-endorphins, log10 neurotensin,log10 orexin A, log10 oxytocin and log10 substance P.
2. Abbreviations: P2 (PANSS positive symptom scale item 2), N2 (PANSS negative symptom scale item 2), N3(PANSS negative symptom scale item 3), G9 (PANSS general pathology symptom scale item 9), PANSS: The
Page 21/24
Positive and Negative Syndrome Scale; BPRS: The Brief Psychiatric Rating scale.
Table 4. Associations between neuropeptides and HAMD scores item 6 in the three patient groups.
UnstandardizedCoe�cients
StandardizedCoe�cients
t p R ² AdjustedR ²
F
B SE Beta
Constant 0.38 0.077 4.92 <0.001
0.30 0.30 F (1, 96) =41.88, p <0.001
MDD group 0.95 0.15 0.55 6.47 <0.001
Constant 2.90 0.81 - 3.57 <0.01
0.37 0.36 F (2, 95) =27.69, p <0.001
MDD group 0.97 0.14 0.56 6.90 <0.001
Log10Endorphin
-0.96 0.31 -0.25 -3.12 <0.01
1. Independent variables: age, gender, education, BMI, group status, log10 α-MSH, log10 β-endorphins, log10neurotensin, log10 orexin A, log10 oxytocin and log10 substance P, HAMD: 17 item Hamilton depression ratingscale.
2. Abbreviations: MDD, major depressive disorders.
Figures
Page 22/24
Figure 1
Group comparison of plasma neuropeptides among the patients and control group. Abbreviations: MSH: melatoninstimulating hormone; FES: �rst episode schizophrenia; BD: bipolar disorders; MDD: major depressive disorders; HC:healthy controls. Signi�cance level: *p<0.05, **p<0.01, ***p<0.001.
Page 23/24
Figure 2
Discriminative performance of biomarkers across diagnostic groups. Receiver-operating characteristics (ROC)curves displaying the performance of plasma α-MSH, β-endorphins, neurotensin, orexin A, oxytocin and substance Pto distinguish (A) FES from HCs, (B) BD from HCs, (C) MDD from HCs, (D) individuals with FES from BD, (E) FESversus MDD, and (F) BD versus MDD.
Abbreviations: MSH: melatonin stimulating hormone; FES: �rst episode schizophrenia; BD: bipolar disorders; MDD:major depressive disorders; HC: healthy controls; AUC, area under the curve. The AUCs were all covariated out age,gender and body mass index.
Page 24/24
Supplementary Files
This is a list of supplementary �les associated with this preprint. Click to download.
SupplementarymaterialsHY1PN1.docx
Related Documents