MEDICAL TREATMENT OF HYPERTENSION: STATE OF THE ART Luis M Ruilope Cardiology Update Davos, february 14, 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

MEDICAL TREATMENT OF HYPERTENSION: STATE OF THE
ART
Luis M Ruilope
Cardiology Update
Davos, february 14, 2011

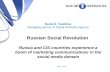
Number of deaths (000s)
0 2000 4000 6000 8000
Occupational risk factors for injury
Unsafe health care injections
Vitamin A deficiency
Zinc deficiency
Urban air pollution
Iron deficiency
Indoor smoke from solid fuels
Unsafe water, sanitation, and hygiene
Alcohol
Physical inactivity
High Body Mass Index
Deficient fruit and vegetable intake
Unsafe sex
Underweight
Cholesterol
Tobacco
Blood pressure
WHO Health Report 2002
World’s #1 killer: High blood pressure (HBP) and its consequences

BENEFIT OF BP CONTROL
•A fixed amount of
benefit corresponds
to a fixed amount of
drop in BP

J Hypertens 2009; 27:673–679.

New concepts even in the
presence of a good BP control• USUAL BP- True BP can not be measured with total
precision.
• MEAN BP- Average of several readings (ABPM, HBPM)
• BP VARIABILITY- The variation of BP with time. Can be
measured over minutes or over days, weeks or months.
• BP INSTABILITY- Transient fluctuations in BP usually in
response to a specific stimulus (posture, stress, pain).
Contributes to BP variability
• Peter M Rothwell, Lancet 2010, 375:938

7 26-MAY-2010
ROADMAP: Percentage of patients reaching BP goal§P
ati
en
ts r
ea
ch
ing
BP
go
al*
(%
)
Months
0 3 6 12 18 24 30 36 42 48
Olmesartan* Placebo*
§ BP goal: <130/80 mmHg
* Additional antihypertensive treatment except RAAS blockers at physician´s discretion, CCBs diuretics, BBs allowed to reach target BP goal

Average : 133.5 Standard vs. 119.3 Intensive, Delta = 14.2
Mean # Meds
Intensive: 3.2 3.4 3.5 3.4
Standard: 1.9 2.1 2.2 2.3

Documento del Grupo de Trabajo de la European Society of Hypertension
Mancia G, Laurent S, Agabiti-Rosei E, Ambrosioni E, Burnier M,
Caulfield MJ, Cifkova R, Clément D, Coca A, Dominiczak A, Erdine S,
Fagard R, Farsang C, Grassi G, Haller H, Heagerty A, Kjeldsen SE,
Kiowski W, Mallion JM, Manolis A, Narkiewicz K, Nilsson P, Olsen
MH, Rahn KH, Redon J, Rodicio J, Ruilope L, Schmieder RE,
Struijker-Boudier HA, van Zwieten PA, Viigimaa M, Zanchetti A.
Reappraisal of European Guidelines on Hypertension
Management: a European Society of Hypertension Task Force
document.
J Hypertens. 2009;27:2121-2158.

ESHESC and JNC 7 Guidelines Recommend Target BP Goals of <140/90 mmHg
for Uncomplicated Hypertension and <130/80 mmHg for Complicated Hypertension1
Type of hypertension BP goal (mmHg)
Uncomplicated <140/90
Complicated
Diabetes mellitus <130/80
Kidney disease <130/80*
Other high risk (stroke, myocardial
infarction)
<130/80
1. Task Force of ESH–ESC. J Hypertens 2007;25:110587
2. Chobanian et al. Hypertension 2003;42:1206–52
*Lower if proteinuria is >1 g/day

11
Reproduced with permission from: Mancia G. Eur Heart J 2007;28:1462–536.
Mancia G, et al. J Hypertens 2009;27:2121–58
Continuous lines show two-drug
combinations that have been found
to be well tolerated and effective
CCBs and ARBs are recommended as preferred
combination therapy partners
Diuretics
ACE inhibitors
CCBs
ARBsβ-blockers
1-blockers

Non-fatal MI (excluding
silent) + fatal CHD
Total coronary endpoint
Total CV events and procedures
All-cause mortality
CV mortality
Fatal/non-fatal stroke
Fatal/non-fatal HF
Development of renal impairment
0.5 1 2
ASCOT BPLA1
Amlodipine-based
betterAtenolol-based
better
Valsartan and Amlodipine: Cardiovascular Endpoints in High-risk
Hypertension1,2
0.5 2
Primary cardiac composite
endpoint
Cardiac mortality
Cardiac morbidity
All MI
All congestive heart failure
All stroke
All-cause death
New-onset diabetes
1
VALUE trial2
Favors
valsartan
Favors
amlodipine
Development of diabetes
1. Dahlöf et al. Lancet 2005;366:895–906; 2. Julius et al. Lancet 2004;363:2022–31



A)- THE EVIDENCE SUGGESTS THAT TO IMPROVE
CV OUTCOMES WE REQUIRE A NEW PARADIGM
THAT EMPHASIZES RAPID ACHIEVEMENT OF BP
CONTROL (1).
B)- BP CONTROL SHOULD BE ATTAINED PREFERABLY
WITHIN 3 MONTHS OF INITIATING THERAPY (2)
1- Basile J. J Clin Hypertens 2008
2- Berlowitz DR & Franklin S. J Clin Hypertens 2010
BP CONTROL

Initiating therapy with the combination of
nifedipine GITS/telmisartan reduced office SBP
as early as 2 weeks
Re
du
cti
on
in
SB
P f
rom
ba
se
lin
e (
mm
Hg
)
Nifedipine GITS 20mg + telmisartan 80mg
Nifedipine GITS 20mg Nifedipine GITS 20mg + telmisartan 80mg
Telmisartan 80mg Nifedipine GITS 20mg + telmisartan 80mg
A
B
C
0 weeks 8 weeks 24 weeks
p=0.003
p=0.024
* * * * * * * * * * * *
*p<0.001 vs baseline
A B C A B CA B CA B C
Based on least-squared (LS) mean ± standard error of the mean (SE) data
Mancia G., et al. Blood pressure control by the nifedipine GITS-telmisartan combination in
patients at high cardiovascular risk. The TALENT Study. Manuscript in preparation. 2010

Primary composite endpoint of the LIFE
stratified by time-varying albuminuria.
Ibsen H et.al. J Hypertens 2004;22:1805.

Intensive vs standard BP lowering strategies
on albuminuria in ACCORD-BP
ACCORD Study Group. N Engl J Med 2010.
P=0.13
Intensive
0
4
8
12
16
20
24
28
32
36
Pa
tie
nts
(%
)
Microalbuminuria Macroalbuminuria
Standard
32.3%30.2%
P=0.009
8.7%6.6%

Albuminuria GroupsN (%)
Baseline Year 1 Year 2 Year 3 p
Total
Normal
High-Normal
Micro
Macro
970 (67.7)171 (11.9)
234 (16.3)
58 (4.0)
862 (60.2)
213 (14.9)
267 (18.6)
91 (6.4)
754 (54.1)
256 (18.4)
291 (20.9)
94 (6.7)
766 (54.9)223 (16.0)
302 (21.6)
104 (7.5)
0.004
No DM
Normal
High-Normal
Micro
Macro
906 (70.0)148 (11.4)
198 (15.3)
43 (3.3)
789 (63.0)
184 (14.7)
217 (17.3)
62 (5.0)
669 (56.1)
222 (18.6)
235 (19.7)
67 (5.6)
682 (58.2)184 (15.7)
238 (20.3)
67 (5.7)
0.005
DM
Normal
High-Normal
Micro
Macro
64 (46.4)23 (16.7)
36 (26.1)
15 (10.9)
73 (40.3)
29 (16.0)
50 (27.6)
29 (16.0)
85 (42.1)
34 (16.8)
56 (27.7)
27 (13.4)
84 (37.5)39 (17.4)
64 (28.6)
37 (16.5)
0.002
p DM <0.001 <0.001 <0.001 <0.001
Ruilope LM et al. In press 2011.

Development of new-onset microalbuminuria
among hypertensive patients according to
previous cardiovascular events
Ruilope LM et al. In press 2011.
New-onset microalbuminuria was seen in 9.9% of patients without a previous event
and in 17.2% (p=0.003) of those with a previous event.
Survival function
Time (months)
Previous CVD
events
No events
Events
% P
atie
nts
fre
e o
f m
icro
alb
um
inu
ria

CONCLUSIONS• Albuminuria appears and progresses under RAS
suppression either with ACEi or ARB.
• Renal function, severity of hypertension and glycemic
control are independent factors related with the increased
urinary albumin excretion.
• We need to know whether the capacity of RAS
suppression is finished or can be improved in order to
improve the outcome of our patients.
• New ways for RAS suppression have to be investigated in
these cohort of patients (dual blockade with ACEi-ARBs
plus Aliskiren, plus spironolactone).

Schematic differences between ACE/NEP inhibition (as with
omapatrilat) and angiotensin receptor blockade/NEP inhibition (as
with LCZ696).
ACE angiotensin-converting enzyme; Ang II angiotensin II; ARBs angiotensin receptor blockers;
AT1 angiotensin II type 1; NEP neprilysin; NPs natriuretic peptides
Segura J, Ruilope LM. Curr Hypertens Rep 2011; 13:74–78.

Change in placebo-subtracted mean sitting systolic blood pressure (A) and
mean sitting diastolic blood pressure (B) during the 8-week treatment period
Patients who discontinued the study drug without a blood pressure measurement after randomisation were excluded.


CONCLUSION
• Early BP control is desirable (increased use of
combinations). Initial BP is lower than it was
years ago.
• Other means of measuring BP different from
office BP measurement have to be used. This
could include BP variability.
• Trials with different combinations reflect
different outcomes.
• Long-term RAAS suppression could not impede
the development of cardiorenal damage
Related Documents