WHAT IS GOOD FOR THE PATIENT IS GOOD FOR THE DOCTOR (OR HEALTH PROFESSIONAL) David Kopacz, M.D. Buchanan Rehabilitation Centre, ADHB [email protected]

David Kopacz, M.D. Buchanan Rehabilitation Centre, ADHB [email protected].
Dec 13, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
WHAT IS GOOD FOR THE PATIENT IS GOOD FOR THE DOCTOR
(OR HEALTH PROFESSIONAL)
David Kopacz, M.D.Buchanan Rehabilitation Centre,
Mental Health Recovery Principles Collaboration in decision making Respect for human needs of the
individual Empowerment of the person in
their own healing Self-responsibility Instill hope Focus on strengths, not just
symptoms or deficits

Physician Dissatisfaction2001 Kaiser Foundation study of 2,608 Physicians in the US
(KKF.org)
60% decreased enthusiasm practicing medicine
87% said physician morale decreased - past 5 yrs.
74% reported excessive administrative duties
56% lack of time for families, hobbies, friends
54% dissatisfied with lack of autonomy
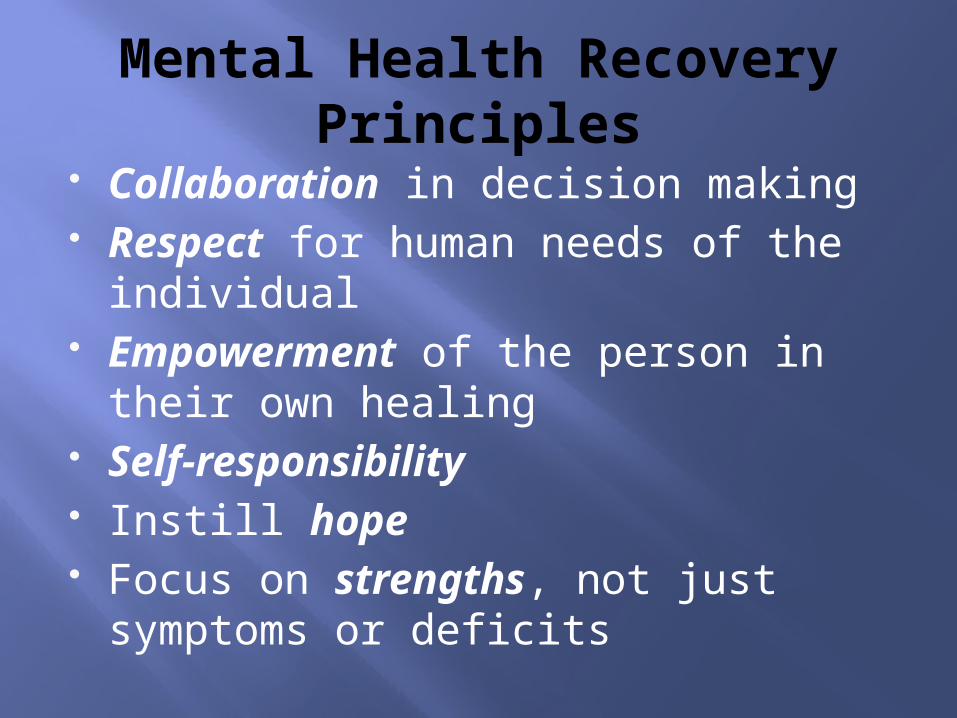
Burnout in New Zealand PhysiciansSurgenor & colleagues, “Burnout in hospital-based medical consultants in the New
Zealand public health system,” NZMJ, 2009
MBI* Subscale Low Burnout Medium Burnout
High Burnout
Emotional Exhaustion
48.1 % 22.2 % 29.7 %
Depersonalisation
50 % 25.6 % 24.4 %
Personal Accomplishment
31.2 % 36.5 % 32.2 %
*Maslach Burnout Inventory
Physician BurnoutPeterkin, Staying Human during Residency Training
Negative attitude toward self, others, work
Distancing from patients emotional needs
Overprescribing medication Emotional Exhaustion Decreased creativity Nonproductive hyperactivity Low sense of personal accomplishment &
job satisfaction
Organizational BurnoutPeterkin, Staying Human during Residency Training (II)
Decline in quality of services Climate of mistrust & hostility Impaired communication Decisions made in isolation Increased sick leave Increased staff turnover
What Makes Physicians Happy?Lipsenthal, Finding a Balance in a Medical Life
When their work is challenging
When individual growth is promoted
When they can make a difference in other people’s lives
Lipsenthal, Finding a Balance in a Medical Life (II)Having a Happy Physician Creates:
Increased patient satisfaction & improved health outcomes
Increased patient trust in their physician Better long-term adherence to therapies. Enhanced physician retention Fewer malpractice suits
The Way We Are Working Isn’t WorkingTony Schwartz, Jean Gomes, Catherine McCarthy, 2010
“The relentless urgency that characterizes most corporate cultures undermines creativity, quality, engagement, thoughtful deliberation, and, ultimately, performance,” (3).

The Way We Are Working Isn’t Working (II)
“The ethic of more, bigger, faster generates value that is narrow, shallow, and short term. More and more, paradoxically, leads to less and less,” (4).
The Way We Are Working Isn’t Working (III)
“‘How can we get more out of our people?’ leaders regularly ask us. We suggest they pose a different question: ‘How can I more intentionally invest in meeting the multidimensional needs of my employees so they’re freed, fueled, and inspired to bring the best of themselves to work every day?’” (20-21).
The Way We Are Working Isn’t Working (IV)
MULTI-DIMENSIONAL NEEDS OF HUMAN BEINGS
Significance (Spirit): What I stand for and believe in – what gives me a sense of meaning Self-expression (Mind): Freedom to develop and express my unique skills and talents Security (Emotions): Feeling appreciated, cared for, valued for who I am and what I do Sustainability (Body): Being able to regularly renew and take care of myself, so I’m healthy, fit, and resilient
The Way We Are Working Isn’t Working (V)
Organizational Example: GOOGLE
Time set aside for following personally-driven creative work that relates to the company
Exercise facilities on site Weekly group walks to brainstorm Time limits on meetings Organic food in cafeteria

Parker Palmer’s New ProfessionalThe Courage To Teach:
Exploring the Inner Landscape of a Teacher’s Life
“the very institutions in which we practice our crafts pose some of the gravest threats to professional standards and personal integrity. Yet higher education does little, if anything, to prepare students to confront, challenge, and help change the institutional conditions under which they will soon be working,” (199).

Parker Palmer’s work with the American College of Graduate Medical Education (II)
“it is the heart of the healer, not the system, that education has the best chance to touch and transform.”

Palmer’s work with the American College of Graduate Medical Education (III)
“Can we think of her [the trainee physician] not as a victim but as a moral agent uniquely positioned to challenge and help change the institution before, during, and after the moment of crisis?”
Parker Palmer’s New Professional (IV)
A new professional is “a person who not only is competent in his or her discipline but also has the skill and the will to resist and help transform the institutional pathologies that threaten the profession’s highest standards,” (202).

Parker Palmer’s New Professional (V)
“At the heart of every profession is an implicit affirmation that the mission of the profession must never be confused with the institutional structures in which it is pursued…We need professionals who are ‘in but not of’ their institutions, whose allegiance to the core values of their fields calls them to resist the institutional diminishment of those values,” (204).
RECOVERY FOR HEALTH PROFESSIONALSBoth Palmer and Schwartz recognize that there are fundamental human needs and dimensions that must be recognized and supported in order to create institutions in which people can be fully human, empowered, happy, and maximally productive.
Schwartz emphasizes the responsibilities of the organization to the employee.
Palmer emphasizes the responsibilities of the professional to the client, to self, and to the organization.
THE RESPONSIBILITY OF THE ORGANIZATION:
To empower the clinician as a new professional.
To support the clinician’s body, mind, emotions, and spirit…in order for the clinician to support the client’s body, mind, emotions, and spirit.
THE RESPONSIBILITY OF THE PROFESSIONAL:
To provide excellent technical treatment.To support & empower clients in body, mind, emotion, and spirit.To care for one’s own body, mind, emotions, and spirit.To be the ethical conscience of the organization when its policies undermine the human needs of the staff and clients.
RECOVERY PRINCIPLES THROUGHOUT THE ORGANIZATION
The way people are treated influences how they treat others.
Empower professionals to empower patients. Collaborate in decision making and policy
development. Respect the role of employees as new professionals. Support the human reality of professionals for peak
productivity. Instill hope. Focus on developing strengths of professionals, not
just a focus on weaknesses. Encourage new professionals to take self-
responsibility in their work and workplace.
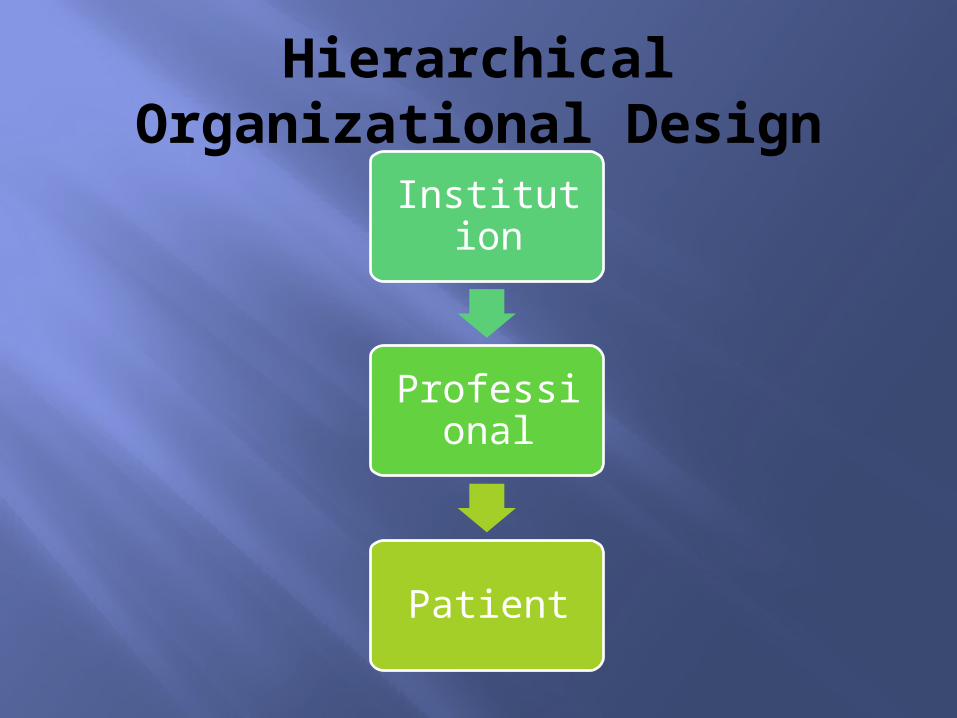
Hierarchical Organizational Design
Institution
Professional
Patient

Collaborative Organizational Design
Institution
Professional
Patient
References Lee Lipsenthal, Finding Balance in a Medical Life, Finding
Balance Inc, 2007. Kaiser Foundation web. Parker Palmer, The Courage to Teach: Exploring the Inner
Landscape of a Teacher’s Life, John Wiley & Sons, 10th Anniversary Edition 2007.
Alan Peterkin, Staying Human during Residency Training, University of Toronto Press, 2008.
Tony Schwartz, Jean Gomes and Catherine McCarthy The Way We are Working Isn’t Working: Four Forgotten Needs That Energize Great Performance, Free Press, 2010.
Lois Surgenor, Ruth Spearing, Jacqueline Horn, Annette Beautrais, Roger, Mulder, Peggy Chen, “Burnout in hospital-based medical consultants in the New Zealand public health system, New Zealand Medical Journal, 7 August 2009, Vol 122 No 1300, p. 11-18.


Parker Palmer’s New Professional (II)From work with the American College of Graduate Medical Education
“Not just the system failed in this case. The heart of the healer failed as well, a heart that
surely knew what was occurring but refused to recognize the fact. And it is the heart of the healer, not the system, that education has the best chance to touch and transform.
What caused the ‘heart failure’ in this resident, apparently leaving her with the sense that she
had no option but to play the stacked hand she had been dealt? Can we think of her not as a victim but as a moral agent uniquely positioned to challenge and help change the institution before, during, and after the moment of crisis?
If so, what might happen in residency programs to support the healer’s heart – and the courage to follow it – when conditions under which medicine is practiced threaten the heart’s imperatives?” (201-202).
(emphasis added)
Related Documents