Advancing Quality David Fillingham 7 th /8 th March 2013 1

David Fillingham: Advancing Quality
Jul 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Advancing Quality
David Fillingham 7th/8th March 2013
1

2

3
“Up and down the country there are brilliant examples of pioneering work, great ideas and
fantastic improvements in service. But, so often, these are isolated examples”
Sir David Nicolson, 2011

4

How can we get much better at spreading more widely and more rapidly and what works?
• Evidence based care bundles
• Technological innovations
• Innovations in service design
5

6
• A bit about AQuA
• The problem with Sauerkraut
• Lessons from experience (it’s the people, stupid)
• AQuA’s Model for Spread: - Advancing Quality - Discovery Community on Integration
• Some final thoughts and questions

About AQuA
• A membership organisation – funded by 68 CCGs and providers in the North West of England
• Our mission is to support our members to improve the quality of healthcare
• All sectors, commissioners and providers – a whole system approach • Firmly rooted in the North West but beginning to work more widely • Encouraging radical service transformation • Fully aligned with the North West’s two proposed Academic Health
Science Networks
7
• Infectious diseases •Hospitals
predominate • Acute intervention • Silo working • Paper based • Doctor knows best
• Chronic diseases • Community based Services • Prevention and self care • Integrated delivery network • Smart use of technology • Shared Decision Making
Industrial Age Medicine
Information Age Healthcare
8

9

And new for 2013/14…
• First Do No Harm… AQuA’s Response to the Francis Report • “Advancing Innovation” – in conjunction with the AHSNs • AQuA Academy support for senior leaders and improvement
experts • A strong focus on the needs of frail older people
10

11
The Sauerkraut Problem

How quickly does innovation spread? – the case of Scurvy amongst Seafarers
12
1497 Vasco de Gamas voyage around the Cape of Good Hope – 100 of 160 men lost to scurvy
1601 Captain James Lancaster – controlled ‘trial’ with lemon juice
1747 Dr James Lind – confirms citrus as effective
1768-80 Captain James Cook – Sauerkraut as a cure
1865 British Board of Trade mandates a healthy diet on all marine vessels
Time elapsed from definitive trial to full implementation = 264 years

Some theoretical perspectives…
• Rogers E. – The Diffusion of Innovation, 1995 • IHI White Paper – A framework for Spread , 2006 • USAID Technical Report – Options for large scale spread of simple high impact
interventions, 2010 • Greater Manchester's CLAHRC – Spreading Improvement and Innovation, 2010 • Greenhalgh et al – Diffusion of Innovations in Service Organisations Mill Bank
Quarterly Vol. 82 No. 4, 2004 • Dixon-Woods et al – Quality Improvement Through Clinical Communities, Journal
of Health Organisation and Management, Vol 26, Issue 2, 2012 • Fraser S. – Accelerates the Spread of Good Practice, 2002 • Gladwell M. – The Tipping Point, 2000
13

14
3 interacting factors… • The innovation itself (“stickiness”)
• The characteristics of the innovators
• The organisational context

15
Source: Rogers, E.M.

16
“Sauerkraut, Sobriety and the Spread of Change”
1. Find sound innovations
2. Find and support innovators
3. Invest in early adopters
4. Make early adopters activity visible
5. Trust and enable re-invention
6. Create slack for change
7. Lead by example
Berwick: Escape Fire

17
Lessons From Experience
(It’s the people, stupid)

Fillingham’s Motivational Matrix
Positive
Negative Out
look
on
Life
Disillusioned Sceptic
Enthusiastic Pragmatist
Embittered Cynic
Naïve Idealist
Grip on Reality
High Low
18

Converting the Sceptics
• Tackle stress and burnout – develop resilience • Make it specific to ‘my’ service • Use rigorous improvement methods • Robust and convincing data • Hands on experience • Reinforce through changed management system and
leadership style
19

AQuA’s Model of Spread
Change Champions and Communities of
Practice
Evidence and Intelligence
Peer to Peer Learning
Robust Improvement Methods
Incentives
20

Advancing Quality - AQ
• Programme established in 2007
• Adapted from Premier’s HQID programme in the US
• Now the dominant Regional CQUINS in the North West
• Has significantly improved reliability of evidence based processes leading to improved outcomes and productivity

Acute myocardial infarction (AMI)
1. Aspirin at arrival 2. Aspirin prescribed at discharge 3. ACE or ARB for LVSD 4. Smoking cessation advice/counseling 5. Beta blocker at arrival 6. Beta blocker prescribed at discharge 7. Thrombolytic received within 30 minutes of
hospital arrival 8. PCI received within 90 minutes of hospital
arrival
Hip and knee replacement
1. Prophylactic antibiotic received within one hour prior to surgical incision
2. Prophylactic antibiotic selection for surgical patients
3. Prophylactic antibiotics discontinued within 24 hours after surgery end time
4. Recommended Venous Thromboembolism prophylaxis ordered
5. Appropriate Venous Thromboembolism prophylaxis within 24 hours prior to surgery to 24 hours after surgery
Community-acquired pneumonia (CAP) 1. Oxygenation assessment within 24 hours
prior to or after hospital arrival 2. Initial antibiotic selection 3. Blood culture collected prior to first
antibiotic administration 4. Antibiotic timing, first dose of antibiotics
within six hours after hospital arrival 5. Smoking cessation advice/counseling
Coronary artery bypass graft (CABG)
1. Aspirin prescribed at discharge 2. Prophylactic antibiotic received within one
hour prior to surgical incision 3. Prophylactic antibiotic selection for surgical
patients 4. Prophylactic antibiotics discontinued within
48 hours after surgery end time Heart failure (HF)
1. Left Ventricular Systolic (LVS) assessment 2. Detailed discharge instructions 3. ACEI or ARB for LVSD 4. Smoking cessation advice/counseling
Evidence Based Measures

• Need robust data – to identify opportunities to improve – to benchmark
• Rules based / algorithmic approach – Identifying patient cohorts – every patient – Data dictionary & reasons for exclusion from a
measure
• Web based measure data collection – Utilise existing data where available
Patient 1 Patient 2 Patient 3 Overall Trust Scores
Measure 1 2 of 3 = 66.6% Measure 2 3 of 3 = 100% Measure 3 1 of 3 = 33.3% Measure 4 3 of 3 = 100% Measure 5 3 of 3 = 100% Opportunities taken
4 of 5 5 of 5 3 of 5 12 of 15
Composite Process Score
80% 100% 60% 80%
Patient Appropriate Care (all or nothing)
0 of 1 1 of 1 0 of 1 1 of 3
Appropriate Care Score
33.3%
Robust data collection
23

A culture of change & collaboration • Regular collaborative learning events • Involvement from all provider & commissioner
organisations • Created networks of clinical and non clinical
communities • A willingness to share and learn
24

Incentives
• Additional financial rewards – first 18 months – top performers / top improvers
• Absorbed into CQUIN – regional scheme (0.01%)
• Benchmarking and friendly competition
• Public reporting www.advancingqualitynw.nhs.uk
25

Rapid improvement, sustained
Steady improvement, sustained
Raised the bar with a new measure!
Marathon not a sprint!
New condition
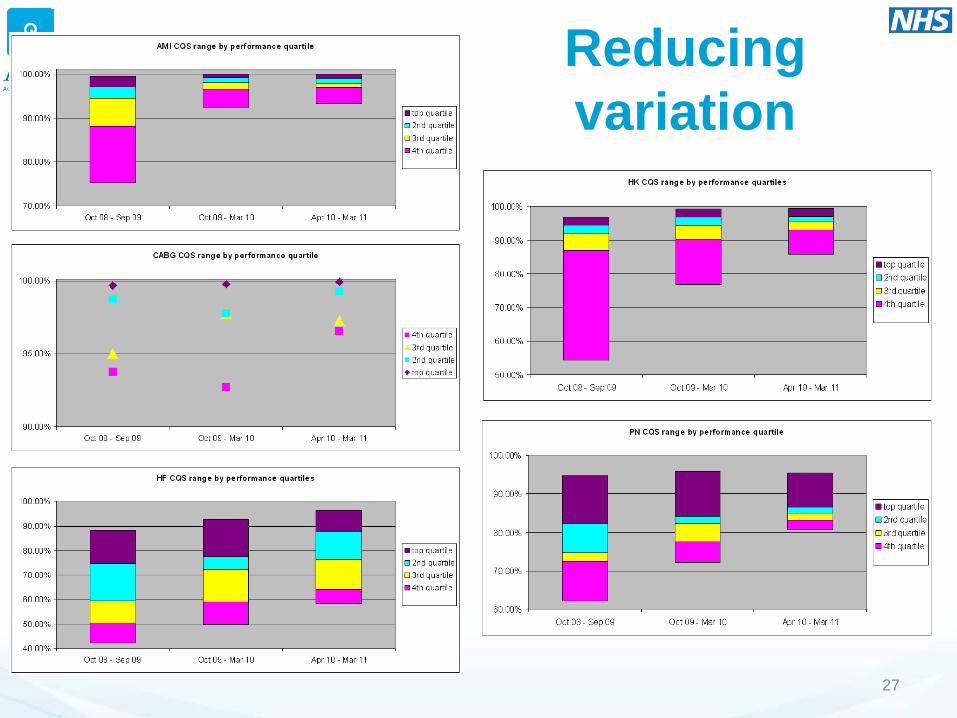
Reducing variation
27


Outcomes & cost effectiveness
• Overall (3 conditions) statistically significant reductions in mortality & LoS
• NW mortality gain greater than rest of England – >1% point reduction in mortality rate (>5% relative
rate) = c890 deaths averted.
• >20,000 hospital days saved (~£5m)
• >6000 QALYs gained as result of mortality reductions – based on healthy life expectancy of people in general population of
same age as the patient population. – Health gain of c£120m (£20k threshold, c£180m @ £30k) – 10 times more cost effective than break-even point

30
AQuA Discovery Community on Integration • We don’t have one accepted “right” model we can copy
• We don’t even have a single definition of integration
• The aim is to: - Steal with pride from elsewhere (creatively adapting) - Stimulate invention - Accelerate progress by mutual sharing and learning
• 8 Health Economies in cohort 1; 11 more in cohort 2

Discovery Community Model
Your
Learning
Learning from each other
Emerging national policy context
National and international case
studies
Faculty input
31

The Framework
32
Integration to Improve • Safety • Effectiveness • Population health • Use of resources
Service Design
Governance
Patient and Carer
Engagement
Leadership
Workforce
• Role design • Skills • Capacity
Infrastructure and IT
Financial and Contractual mechanisms
Culture
Healthcare value


34
Richard Gleave

AQuA’s Model of Spread
Change Champions and Communities of
Practice
Evidence and Intelligence
Peer to Peer Learning
Robust Improvement Methods
Incentives
35
AWR “Accelerated Wheel Reinvention”

36
A new ‘Context’ for Improvement and Spread

37
Some Final Thoughts and Questions…
• What are the most important priorities for spread? • Do we have enough “enthusiastic pragmatists”? • Is it “hit and hope” or do we have an aligned, systematic
approach? • How can we use the new improvement “context” to our
advantage? • How we can counter pessimism and setbacks with resilience,
energy and hope?
Related Documents











