Data sources for measuring maternal mortality November 1, 2010 Rafael Lozano Professor of Global Health

Data sources for measuring maternal mortality
Jan 13, 2016
Data sources for measuring maternal mortality. November 1, 2010 Rafael Lozano Professor of Global Health. Outline. Input data and correction process by source PMDF to maternal deaths to rates Modeling approaches I: linear models Outlier detection - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Data sources for measuring maternal mortality
November 1, 2010
Rafael Lozano
Professor of Global Health

Outline
• Input data and correction process by source
• PMDF to maternal deaths to rates
• Modeling approaches I: linear models
• Outlier detection
• Modeling approaches II: space-time regression
• Predictive validity
• Uncertainty
2

Processing input data
3

Four major categories of data
• Vital registration
• Deaths in the household data from censuses and surveys
• Sibling histories from surveys
• National and subnational peer reviewed studies of maternal mortality (i.e. verbal autopsy studies, etc)
4

Four major categories of data
• Vital registration
• Deaths in the household data from censuses and surveys
• Sibling histories from surveys
• National and subnational peer reviewed studies of maternal mortality (i.e. verbal autopsy studies, etc)
5

Sources for vital registration data
• WHO Mortality Database
o Reported civil registration data from countries
o Periodically updated and released by WHO
• Country websites and official publications
• Sample registration systems, such as in India or China
6

Issues with vital registration
• Changes in the International Classification of Diseases (ICD) results in changes in coding assignments to underlying causes of death
• The use of tabulation lists in the ICD results in the loss of substantial detail of cause of death
• Deaths can be (and often are) assigned to causes that should not be considered underlying causes of death (garbage codes)
Together, this means that what counts as a “maternal death” in one country in one year, may not count as a “maternal death” in another country or another year.
7

Correcting vital registration
• Shortened cause of death list: 56 causes of interest to public health practitioners
o Causes mapped across ICD revisions to these 56 causes
o Maternal conditions encompass all O codes (O00 – O99)
8

Garbage codes
• Garbage coding is the biggest challenge to comparability across countries and over time in vital registration data
• Garbage codes: assigned causes of death which are not useful for public health analysis of cause-of-death data
• General approach to address problem:
1. Identify garbage codes
2. Identify target codes to which garbage codes should be reassigned
3. Choose the fraction of deaths assigned to a garbage code that should be reassigned to each target code
9

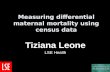
Fraction of deaths assigned to GCs in the latest ICD-10 year since 2000
10

Garbage codes
• General approach to address problem:
1. Identify garbage codes
2. Identify target codes to which garbage codes should be reassigned
3. Choose the fraction of deaths assigned to a garbage code that should be reassigned to each target code
11

Redistribution of garbage codes
1. Identify garbage codes
4 classifications of garbage codes:
• Type 1: Causes that should not be considered underlying causes of death
• i.e. R95-R99: Ill-defined and unknown causes of mortality
• Type 2: Intermediate causes of death
• i.e. I51: Heart failure
• Type 3: Immediate causes of death
• i.e. E87: Other disorders of fluid, electrolyte and acid-base balance
• Type 4: Unspecified causes within a larger grouping
• i.e. Malignant neoplasm without specification of site
12

Percentage of Type of Garbage Codes
13
All country years by age, only ICD 10All country years by ICD

Redistribution of garbage codes
2. Identify target codes to which garbage codes should be reassigned
• Based on pathophysiology, i.e.:
14
Peritonitis
Garbage code Target causes
Digestive diseases
Genitourinary diseases
Maternal conditions
Injuries

Redistribution of garbage codes
3. Choose the fraction of deaths assigned to a garbage code that should be reassigned to each target code
3 approaches:
i.Proportionate redistribution
• For causes with little information content
ii.Statistical models
• For heart failure
iii.Expert judgment
• Via review of published literature and consultation with experts, taking into account time trends in causes of death
15

Garbage codes redistributed to maternal causes, based on expert judgment (ICD-10)
ICD-10 code Condition Fraction to maternal
D65 Disseminated intravascular coagulation [defibrination syndrome]
30%
K65 Peritonitis 20%
A40 Streptococcal septicaemia 14%
A41 Other septicaemia
I26 Pulmonary embolism 10%
K66.0 Peritoneal adhesions 50%
N17 Acute renal failure
0.4%N18 Chronic renal failure
N19 Unspecified renal failure
R57.9 Shock, unspecified 25%
R57.1 Hypovolaemic shock 35%
16

Garbage codes redistributed to maternal causes, based on proportions (ICD-10)
ICD-10 code Condition
R99 Other ill-defined and unspecified causes of mortality
R98 Unattended death
R09.2 Respiratory arrest
R96.0 Instantaneous death
R68.8 Other specified general symptoms and signs
R55 Syncope and collapse
R50.9 Fever, unspecified
R96.1 Death occurring less than 24 hours from onset of symptoms, not otherwise explained
R57.0 Cardiogenic shock
R56.8 Other and unspecified convulsions
R62.8 Other lack of expected normal physiological development
R10.4 Other and unspecified abdominal pain
R58 Haemorrhage, not elsewhere classified
R57.1 Hypovolaemic shock
R09.0 Other symptoms and signs involving the circulatory and respiratory systems
R02 Gangrene, not elsewhere classified
R40.2 Coma, unspecified
R04.8 Haemorrhage from other sites in respiratory passages
17

18

19

Maternal Mortality Audit Studies
• 32 studies have been published that use detailed audits of reproductive-aged deaths to ascertain the true number of maternal deaths compared to those registered.
• Assessment of these studies should exclude late maternal deaths and incidental causes to make them comparable to the GC algorithms for maternal mortality estimation.
o 30 studies identify either late maternal and incidental deaths, but only 5 studies identify both
• These studies provide an opportunity to validate the GC approach to maternal death correction.
20

21
Published Studies on Maternal Death Misclassification

Four major categories of data
• Vital registration
• Deaths in the household data from censuses and surveys
• Sibling histories from surveys
• National and subnational peer reviewed studies of maternal mortality (i.e. verbal autopsy studies, etc)
22

Deaths in the household
• Some censuses and surveys include a module on deaths occurring in the household over a specified period of time
o Was the deceased between the ages 15-49 and female?
o If yes: did she die while pregnant? During child birth? In the 6 weeks after giving birth or terminating the pregnancy?
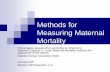
• Direct questioning about events in the household tends to lead to undercounting of vital events
23

Household Deaths are Usually Undercounts
24
-8-6
-4-2
0
0-4
5-9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-8
00-
45-
9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-8
0
male female
Gold Standard 1995.5 PHL DHS
Household A Household B Household C Household D
log
mor
talit
y ra
te
age group
Boholage-specific mortality rates

Four major categories of data
• Vital registration
• Deaths in the household data from censuses and surveys
• Sibling histories from surveys
• National and subnational peer reviewed studies of maternal mortality (i.e. verbal autopsy studies, etc)
25

Survey data for maternal mortality
• Difficult to capture in a survey because maternal deaths are rare – a very large sample size required
• Sibling histories yield high return of observations per respondent
• Availability of large datasets with information on sibling survival from household surveys
o DHS “maternal mortality” module
o CDC Reproductive Health Surveys
• However, naïve analysis of sibling histories can be misleading
o Survivor bias
o Recall bias

Gakidou-King weights• An algebraic correction for underrepresentation of high mortality
families
• “Upweight” observations from high mortality families
• Calculate a family-level weight in the survey micro-data
• This weight (Wf =Bf /Sf) is the inverse of the probability of surviving to the time of the survey
o Similar to a population sampling weight: the inverse of the probability of selection into the sample
27
survey. theof time the tosurviving siblings ofnumber
and size, sibship original
weight,levelfamily a is where
f
f
f
f
ff
S
B
W
S
BW

28

Four major categories of data
• Vital registration
• Sibling histories from surveys
• Deaths in the household data from censuses and surveys
• National and subnational peer reviewed studies of maternal mortality (i.e. verbal autopsy studies, etc)
29

Literature review to identify studies • In PubMed, searched for “maternal mortality” and “country name”
• Included studies had to be peer-reviewed, population-based, and provide clear description of methods
• 25 additional verbal autopsy studies which included “maternal” in the cause list
30
9,659 titles
593 abstracts
209 papers
61 extracted

Final Database by Source
Source of Data Site-Years of Observation
Vital registration 2186
Sibling Histories 204
Surveillance Systems 20
Census/Survey Deaths in Household 26
National VA 35
Subnational VA 180
Total 2651
31
• No data for 21 countries, representing 2.2% of births

Density of site-years of observation, 1980-2008
32

Density of site-years of observation, 1980-2008
33

Data sources in each country
• National and subnational sources included
• Since the time of publication, new data sources have come to light:
o Italicized: incorporated into model since the Lancet 2010 publication
o Italicized and in blue font: sources that we are aware of but have not yet identified and incorporated
34

Bangladesh
35
Sub-nationally representative data sources
Year Source
1980-2006 Matlab Demographic Surveillance Site
1982 Alauddin M. Maternal mortality in rural Bangladesh: the Tangail district. Stud.Fam.Plann. 1986;17(1):13-21.
1983 Khan AR, et al. Maternal mortality in rural Bangladesh: the Jamalpur district. Stud.Fam.Plann. 1986:7-12.
1987 Fauveau V, et al.. Effect on mortality of community-based maternity-care programme in rural Bangladesh. The Lancet 1991;338(8776):1183-1186.
2000 INDEPTH
2003 Chowdhury ME, et al. Determinants of reduction in maternal mortality in Matlab, Bangladesh: a 30-year cohort study. The Lancet 2007;370(9595):1320-1328.
Nationally representative data sources
Year Source
2000-2001 Bangladesh Maternal Mortality and Maternal Health Services Survey (BMMS) household deaths module, microdata
2001 Bangladesh Maternal Mortality and Maternal Health Services Survey (BMMS) sibling history microdata

36

Bhutan
37
Sub-nationally representative data sources
Year Source
Nationally representative data sources
Year Source
2005 Tabulated census household deaths data

38

Cambodia
39
Sub-nationally representative data sources
Year Source
Nationally representative data sources
Year Source
2000 Demographic and Health Survey (DHS) sibling history microdata
2005 Demographic and Health Survey (DHS) sibling history microdata
2008 Tabulated census household deaths data

40

India
41
Nationally representative data sources
Year Source
1982, 1997, 1999, 2001, 2002, 2004
National Sample Registration Scheme (SRS)
1992 National Family Health Survey I microdata (deaths in the household)
1998 National Family Health Survey II microdata (deaths in the household & VA)
1999-2004 District Level Household Survey (DLHS) II microdata (deaths in the HH)
2002 Special Survey – Nationwide
2004-2008 District Level Household Survey (DLHS) III microdata (deaths in the HH)

India, continued
42
Sub-nationally representative data sources
Year Source
1980-1998 Survey of Causes of death (SCD)
1986 Bhatia JC. Levels and causes of maternal mortality in southern India. Stud.Fam.Plann. 1993;24(5):310-318.
1989 Gupta N, et al. Maternal mortality in seven districts of Uttar Pradesh - an ICMR Task Force Study. Indian Journal of Public Health 2006;50(3):173-178.
1990-1998 Medical Certification of Causes of Death (MCCD9)
1992 Kumar R, et al. Maternal mortality inquiry in a rural community of north India. International Journal of Gynecology & Obstetrics 1989;29(4):313-319.
1992 Kakrani V, et al. A study of registration of deaths at primary health centre-with special reference, to. Indian J.Med.Sci. 1996;50(6):196.
1999-2001 Medical Certification of Causes of Death (MCCD10)
2000 Singh RB, Singh V, Kulshrestha SK, Singh S, Gupta P, Kumar R, et al. Social class and all-cause mortality in an urban population of North India. Acta Cardiol. 2005 Dec;60(6):611-617.
2002 Iyengar K, et al. Pregnancy-related deaths in rural Rajasthan, India: exploring causes, context, and care-seeking through verbal autopsy. Journal of Health, Population and Nutrition 2009;27(2):293.
2004 Joshi R, et al. Verbal autopsy coding: are multiple coders better than one? Bull.World Health Organ. 2009;87:51-57.
2005 Barnett S, et al. A prospective key informant surveillance system to measure maternal mortality - findings from indigenous populations in Jharkhand and Orissa, India. BMC Pregnancy Childbirth 2008 Feb 28;8:6.
2007 Dongre A, et al. A community based cross sectional study on feasibility of lay interviewers in ascertaining causes of adult deaths by using verbal autopsy in rural Wardha. Online Journal of Health And Allied Sciences 2009;7(4).

43

Indonesia
44
Sub-nationally representative data sources
Year Source
1981 Fortney JA, et al. Reproductive mortality in two developing countries. Am.J.Public Health 1986 Feb;76(2):134-138.
2006 Ronsmans C, et al. Professional assistance during birth and maternal mortality in two Indonesian districts. Bull.World Health Organ. 2009 Jun;87(6):416-423.
Nationally representative data sources
Year Source
1994 Demographic and Health Survey (DHS) sibling history microdata
1997 Demographic and Health Survey (DHS) sibling history microdata
2002 Demographic and Health Survey (DHS) sibling history microdata
2007 Demographic and Health Survey (DHS) sibling history microdata

45

Lao, People’s Democratic Republic of
46
Sub-nationally representative data sources
Year Source
Nationally representative data sources
Year Source
1990 Fauveau VA. The Lao People's Democratic Republic: maternal mortality and female mortality: determining causes of deaths. World Health Stat.Q. 1995;48(1):44-46.
Sources that could potentially be incorporated, with access
1995 Census data
2005 Census data

47

Nepal
48
Sub-nationally representative data sources
Year Source
Nationally representative data sources
Year Source
1996 Demographic and Health Survey (DHS) sibling history microdata
2006 Demographic and Health Survey (DHS) sibling history microdata
Sources that could potentially be incorporated, with access
2008-2009 National maternal mortality enquiry

49

Pakistan
50
Sub-nationally representative data sources
Year Source
1986, 1990 Fikree FF, et al. Maternal mortality in different Pakistani sites: ratios, clinical causes and determinants. Acta Obstet.Gynecol.Scand. 1997;76(7):637-645.
Nationally representative data sources
Year Source
1993-1994 Vital registration
2006 Demographic and Health Survey (DHS) Verbal autopsy microdata

51

The Philippines
52
Sub-nationally representative data sources
Year Source
Nationally representative data sources
Year Source
1981, 1992-1998, 2001-2005
Vital registration data
1993 Demographic and Health Survey (DHS) sibling history microdata
1998 Demographic and Health Survey (DHS) sibling history microdata
Sources that could potentially be incorporated, with access
2006 Family Planning Survey

53

Sri Lanka
54
Sub-nationally representative data sources
Year Source
Nationally representative data sources
Year Source
1980-1989, 1991-2006
Vital registration data
Sources that could potentially be incorporated, with access
ARFH Surveillance data

55

Thailand
56
Sub-nationally representative data sources
Year Source
Nationally representative data sources
Year Source
1980-1987, 1990-2000, 2002-2007
Vital registration data
2004-2006 Chandoevwit W, et al, Using multiple data for calculating the maternal mortality ratio in Thailand, TDRI Quarterly Review. 2007;22(3):13-19
1995, 1997 BHP studies, via Chandoevwit W, et al, Using multiple data for calculating the maternal mortality ratio in Thailand, TDRI Quarterly Review. 2007;22(3):13-19

57
Related Documents