bristol.ac.uk Data sets NHS digital, UK Renal Registry, NICOR, Stroke Registry, National Diabetes Audit and CPRD Dr Fergus Caskey Consultant senior lecturer, University of Bristol Honorary consultant nephrologist, North Bristol NHS Trust

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
bristol.ac.uk
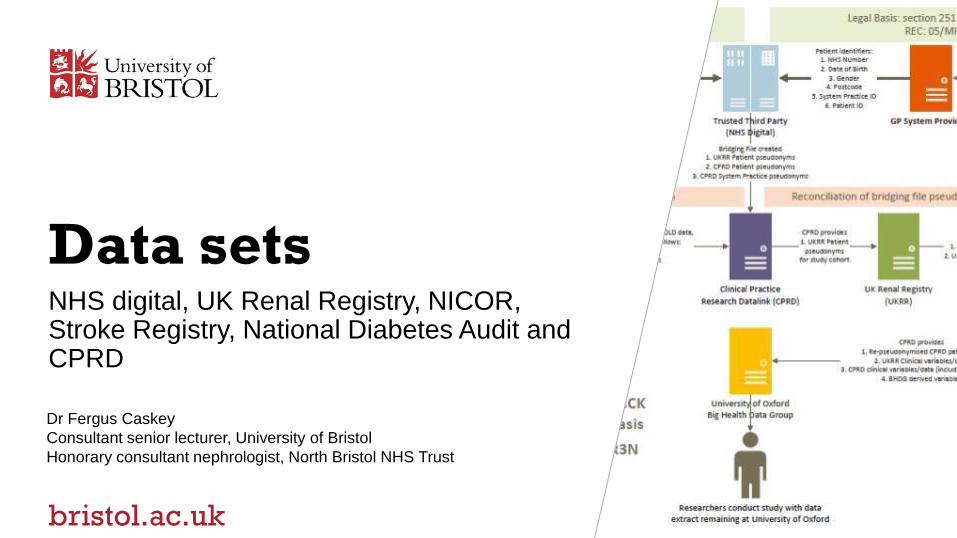
Data setsNHS digital, UK Renal Registry, NICOR, Stroke Registry, National Diabetes Audit and CPRD
Dr Fergus Caskey
Consultant senior lecturer, University of Bristol
Honorary consultant nephrologist, North Bristol NHS Trust
bristol.ac.uk
Brief
1. Describe the current data sets, registries and other resources in renal disease,
cardiovascular, stroke, diabetes and obesity
2. Examples of integration between different disease datasets
3. What is needed to maximise collection and presentation of data to underpin multi-
morbidity research
bristol.ac.uk
The databases
• NHS digital
• UK Renal Registry
• NICOR
• Stroke Registry
• National Diabetes Audit
• CPRD
Databases Hosting systems
• Other HQIP national audits: Joint; Anxiety depression; Maternal and perinatal; End of life care
bristol.ac.uk
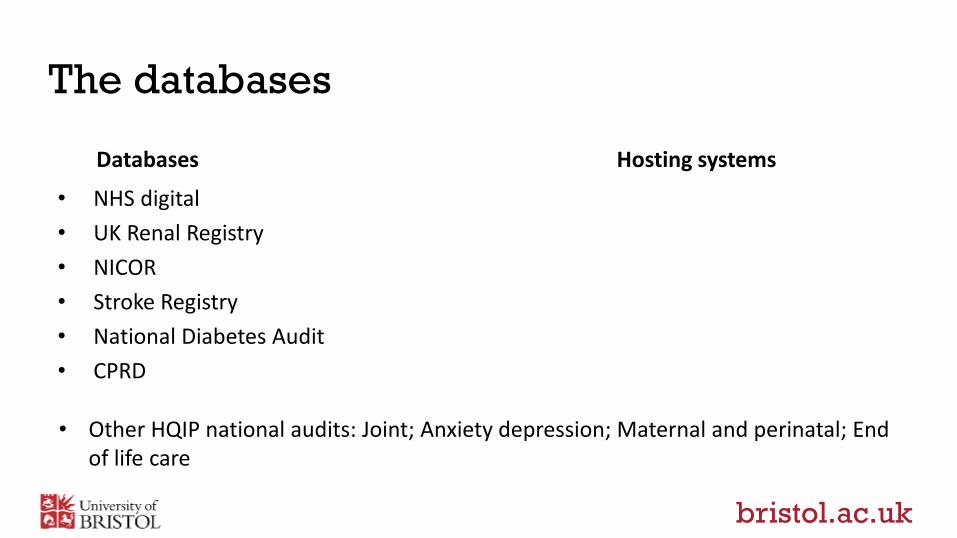
UKRR: The UK Renal Registry
Exported from biochemistry labs
Linked to HES and CR for audit
www.renalreg.org
datasets/the-uk-renal-registry-dataset/
about-us/working-with-us/
Caution!
v3.14 vs v4.2
UK coverage with automatic extraction
from EHRs (via Scottish Renal Registry
for Scotland)
bristol.ac.uk
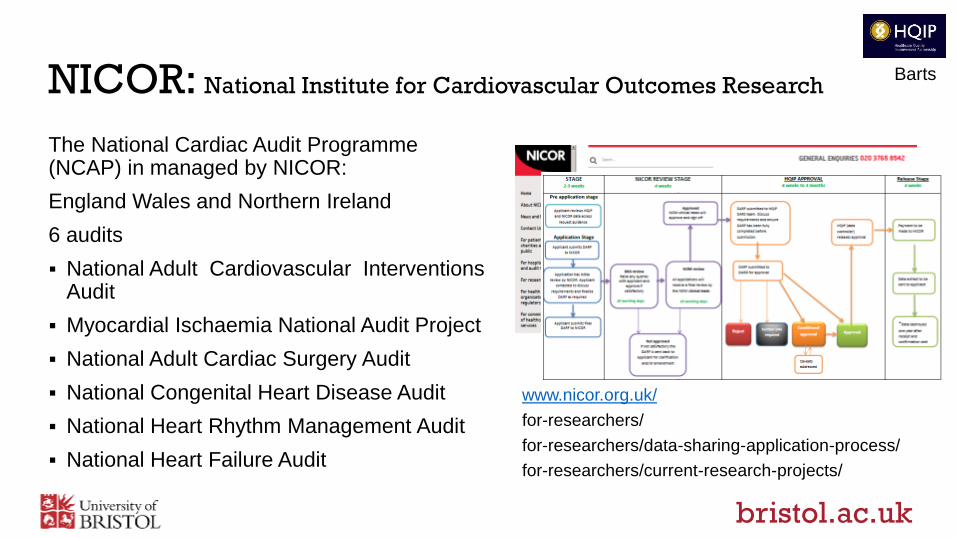
NICOR: National Institute for Cardiovascular Outcomes Research
The National Cardiac Audit Programme (NCAP) in managed by NICOR:
England Wales and Northern Ireland
6 audits
National Adult Cardiovascular Interventions Audit
Myocardial Ischaemia National Audit Project
National Adult Cardiac Surgery Audit
National Congenital Heart Disease Audit
National Heart Rhythm Management Audit
National Heart Failure Audit
www.nicor.org.uk/
for-researchers/
for-researchers/data-sharing-application-process/
for-researchers/current-research-projects/
Barts
bristol.ac.uk
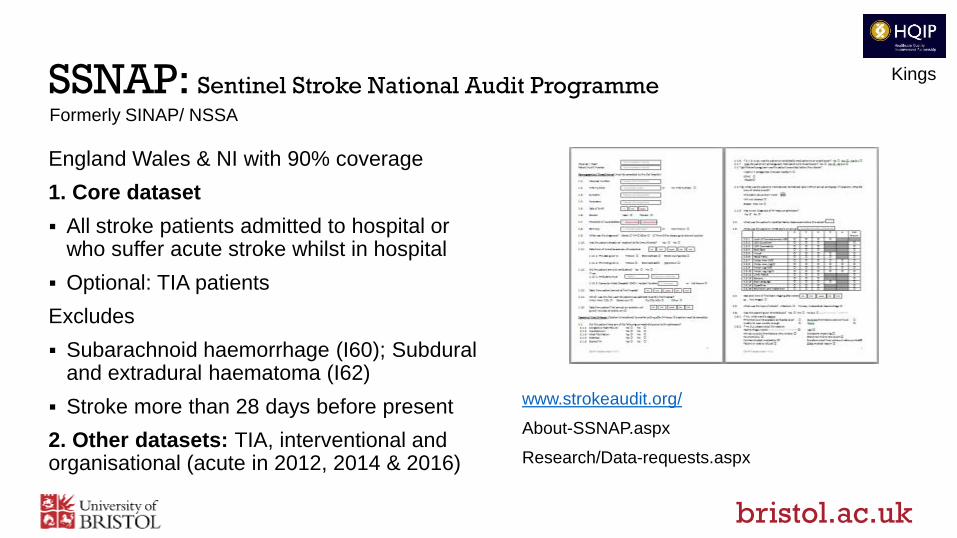
SSNAP: Sentinel Stroke National Audit Programme
England Wales & NI with 90% coverage
1. Core dataset
All stroke patients admitted to hospital or who suffer acute stroke whilst in hospital
Optional: TIA patients
Excludes
Subarachnoid haemorrhage (I60); Subdural and extradural haematoma (I62)
Stroke more than 28 days before present
2. Other datasets: TIA, interventional and organisational (acute in 2012, 2014 & 2016)
www.strokeaudit.org/
About-SSNAP.aspx
Research/Data-requests.aspx
Formerly SINAP/ NSSA
Kings
bristol.ac.uk
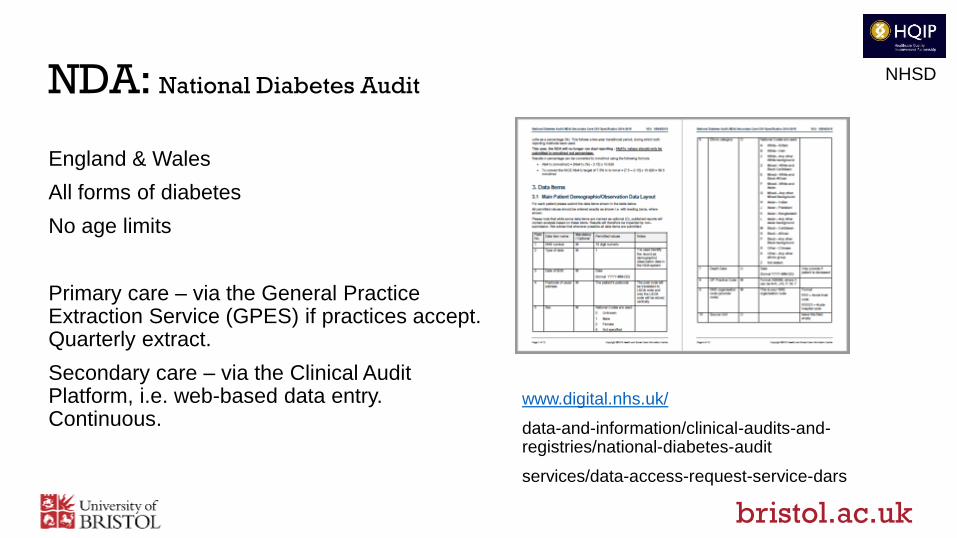
NDA: National Diabetes Audit
England & Wales
All forms of diabetes
No age limits
Primary care – via the General Practice Extraction Service (GPES) if practices accept. Quarterly extract.
Secondary care – via the Clinical Audit Platform, i.e. web-based data entry. Continuous.
www.digital.nhs.uk/
data-and-information/clinical-audits-and-registries/national-diabetes-audit
services/data-access-request-service-dars
NHSD
bristol.ac.uk
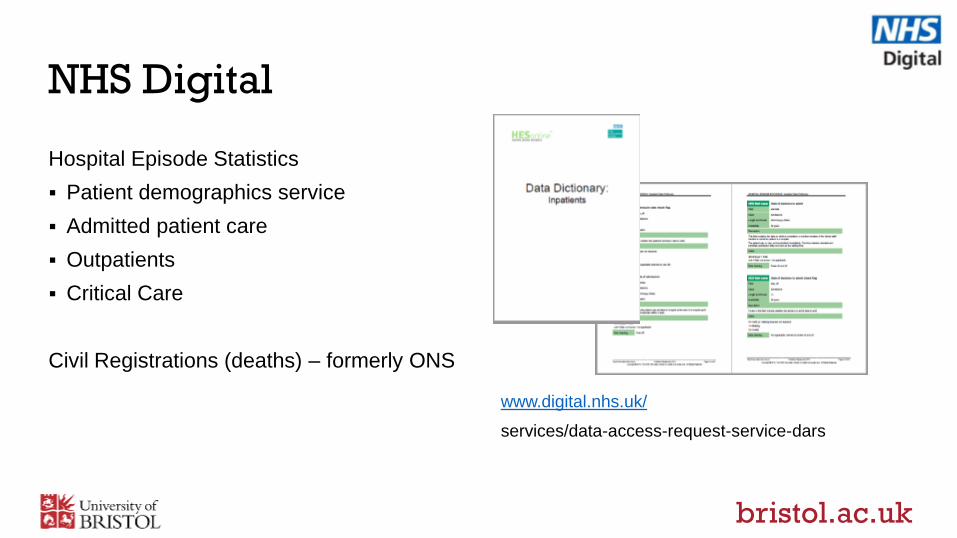
NHS Digital
Hospital Episode Statistics
Patient demographics service
Admitted patient care
Outpatients
Critical Care
Civil Registrations (deaths) – formerly ONS
www.digital.nhs.uk/
services/data-access-request-service-dars
bristol.ac.uk
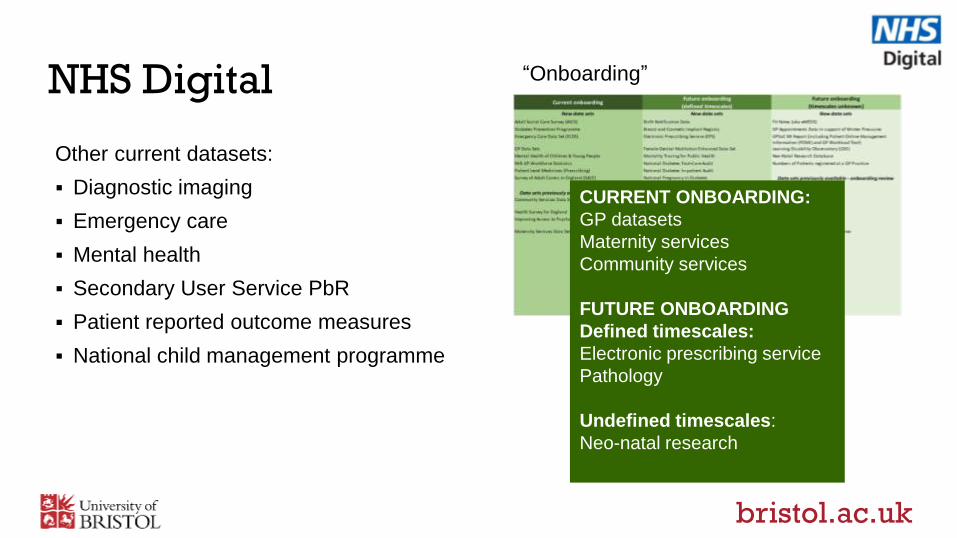
NHS Digital
CURRENT ONBOARDING:
GP datasets
Maternity services
Community services
FUTURE ONBOARDING
Defined timescales:
Electronic prescribing service
Pathology
Undefined timescales:
Neo-natal research
“Onboarding”
Other current datasets:
Diagnostic imaging
Emergency care
Mental health
Secondary User Service PbR
Patient reported outcome measures
National child management programme
bristol.ac.uk
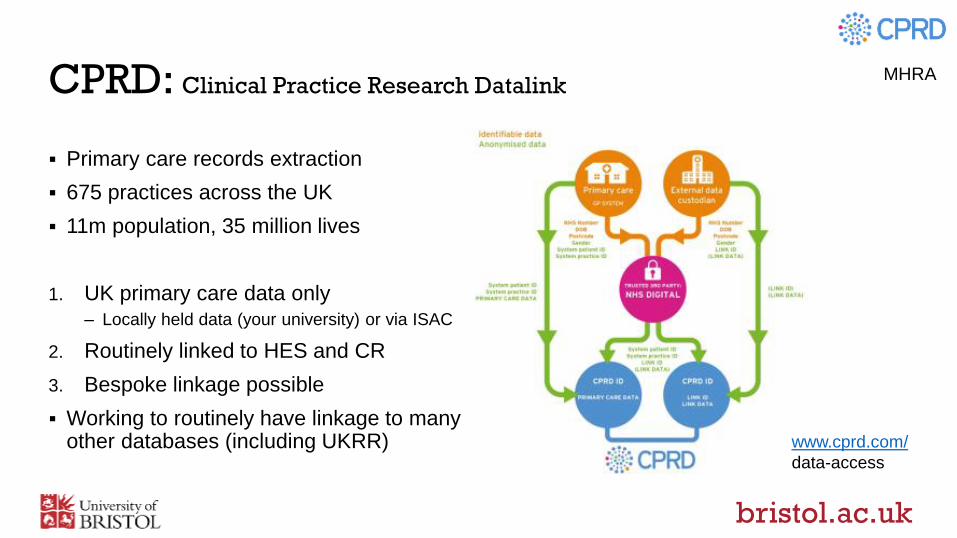
CPRD: Clinical Practice Research Datalink
Primary care records extraction
675 practices across the UK
11m population, 35 million lives
1. UK primary care data only
– Locally held data (your university) or via ISAC
2. Routinely linked to HES and CR
3. Bespoke linkage possible
Working to routinely have linkage to many other databases (including UKRR)
MHRA
www.cprd.com/
data-access
bristol.ac.uk
Brief
1. Describe the current data sets, registries and other resources in renal disease,
cardiovascular, stroke, diabetes and obesity
2. Examples of integration between different disease datasets
3. What is needed to maximise collection and presentation of data to underpin multi-
morbidity research
bristol.ac.uk
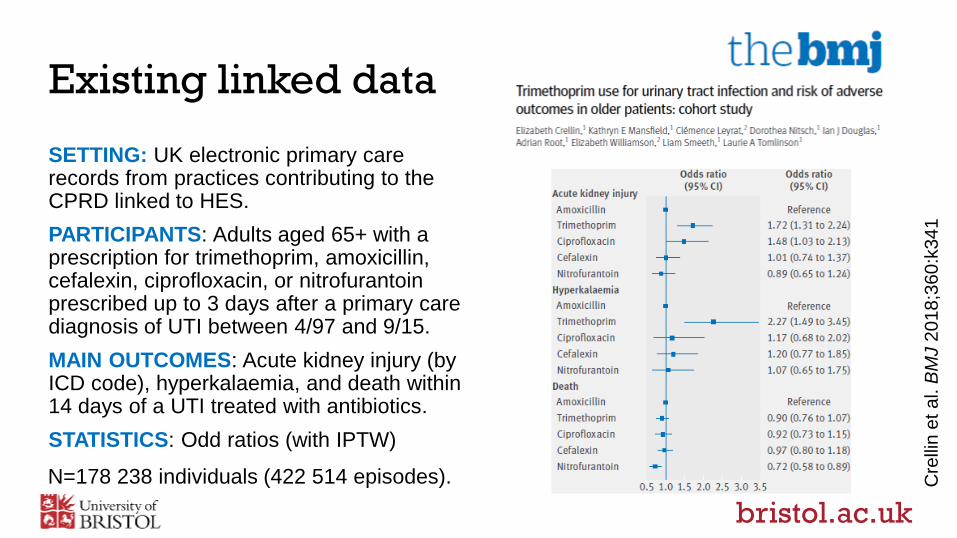
Existing linked data
SETTING: UK electronic primary care records from practices contributing to the CPRD linked to HES.
PARTICIPANTS: Adults aged 65+ with a prescription for trimethoprim, amoxicillin, cefalexin, ciprofloxacin, or nitrofurantoin prescribed up to 3 days after a primary care diagnosis of UTI between 4/97 and 9/15.
MAIN OUTCOMES: Acute kidney injury (by ICD code), hyperkalaemia, and death within 14 days of a UTI treated with antibiotics.
STATISTICS: Odd ratios (with IPTW)
Cre
llin
et a
l. B
MJ 2
01
8;3
60
:k34
1
N=178 238 individuals (422 514 episodes).
bristol.ac.uk
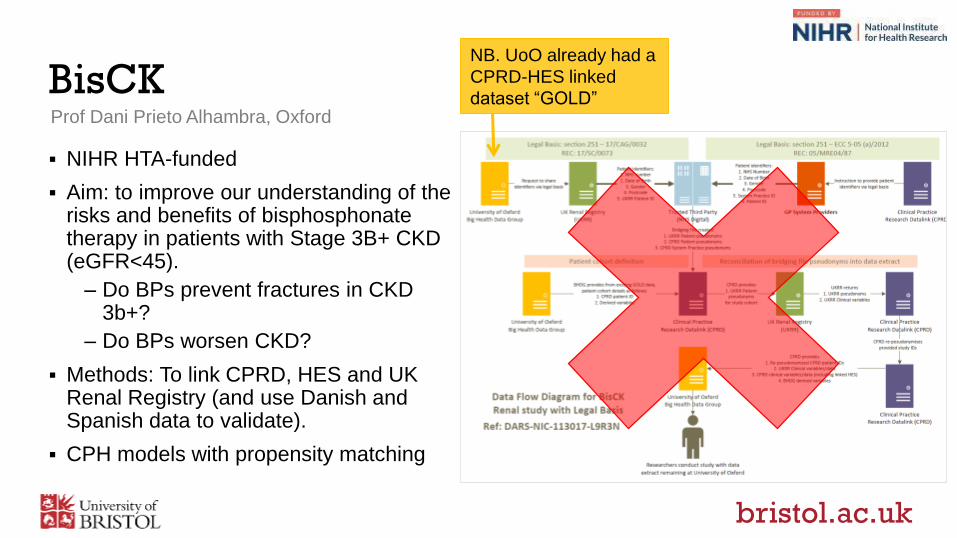
BisCK
NIHR HTA-funded
Aim: to improve our understanding of the risks and benefits of bisphosphonate therapy in patients with Stage 3B+ CKD (eGFR<45).
– Do BPs prevent fractures in CKD 3b+?
– Do BPs worsen CKD?
Methods: To link CPRD, HES and UK Renal Registry (and use Danish and Spanish data to validate).
CPH models with propensity matching
NB. UoO already had a
CPRD-HES linked
dataset “GOLD”Prof Dani Prieto Alhambra, Oxford
bristol.ac.uk
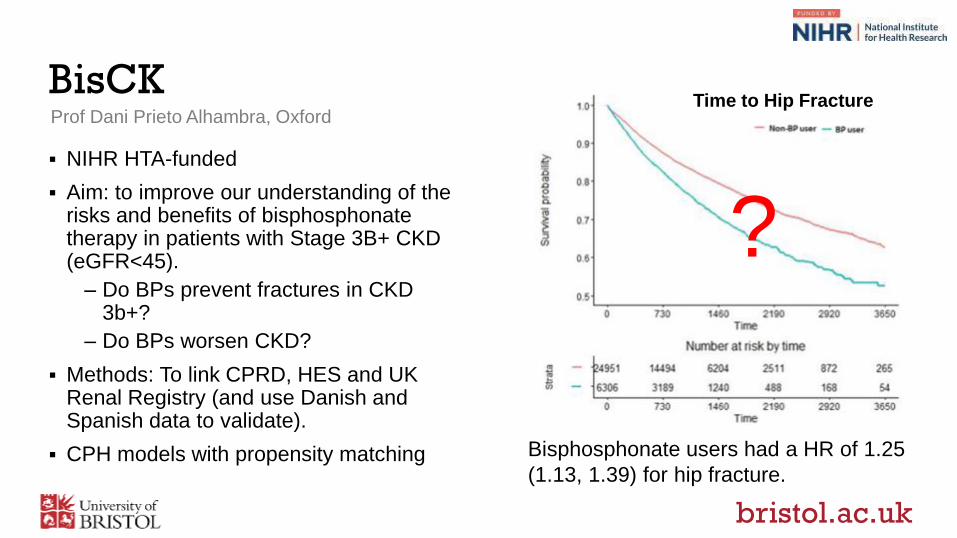
BisCKTime to Hip Fracture
Bisphosphonate users had a HR of 1.25
(1.13, 1.39) for hip fracture.
Prof Dani Prieto Alhambra, Oxford
? NIHR HTA-funded
Aim: to improve our understanding of the risks and benefits of bisphosphonate therapy in patients with Stage 3B+ CKD (eGFR<45).
– Do BPs prevent fractures in CKD 3b+?
– Do BPs worsen CKD?
Methods: To link CPRD, HES and UK Renal Registry (and use Danish and Spanish data to validate).
CPH models with propensity matching
bristol.ac.uk
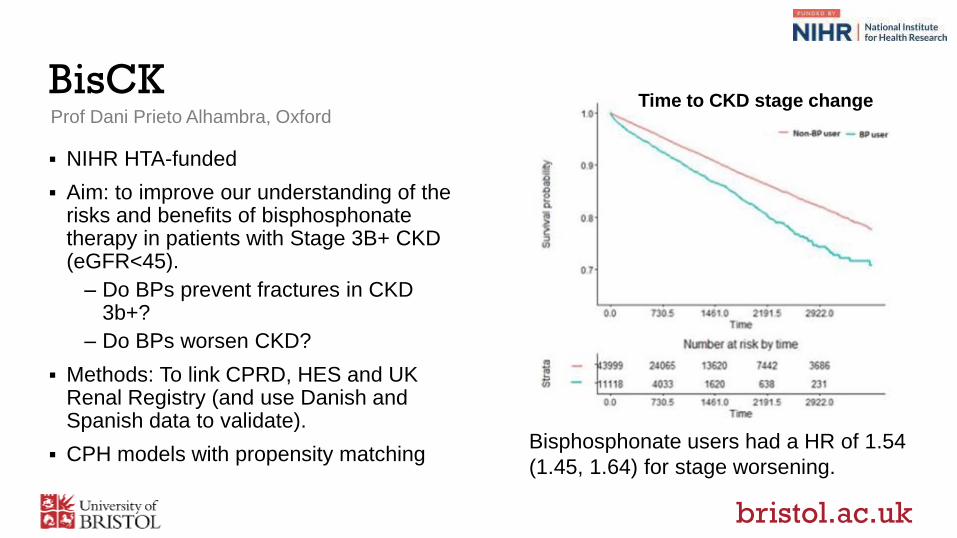
BisCK
Bisphosphonate users had a HR of 1.54
(1.45, 1.64) for stage worsening.
Time to CKD stage changeProf Dani Prieto Alhambra, Oxford
NIHR HTA-funded
Aim: to improve our understanding of the risks and benefits of bisphosphonate therapy in patients with Stage 3B+ CKD (eGFR<45).
– Do BPs prevent fractures in CKD 3b+?
– Do BPs worsen CKD?
Methods: To link CPRD, HES and UK Renal Registry (and use Danish and Spanish data to validate).
CPH models with propensity matching
bristol.ac.uk
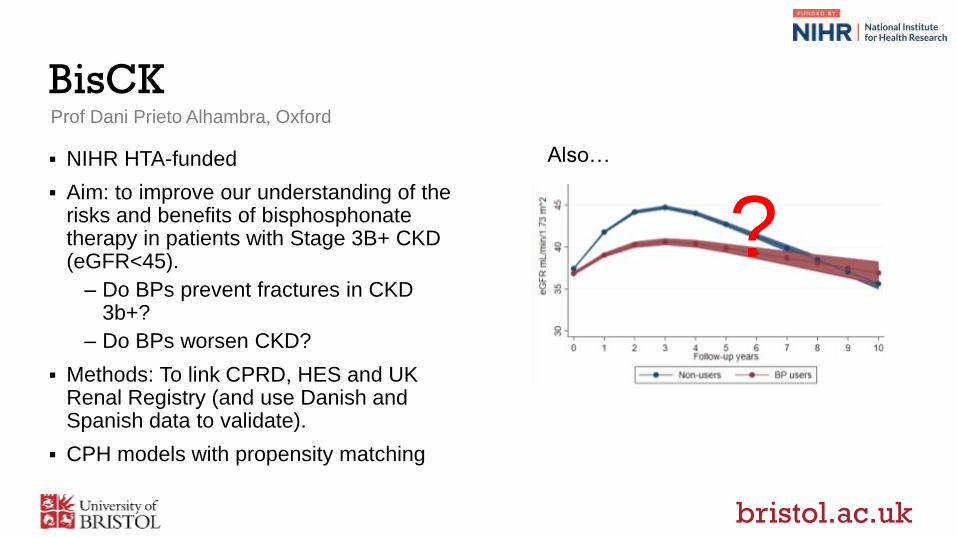
BisCK
Also…
Prof Dani Prieto Alhambra, Oxford
? NIHR HTA-funded
Aim: to improve our understanding of the risks and benefits of bisphosphonate therapy in patients with Stage 3B+ CKD (eGFR<45).
– Do BPs prevent fractures in CKD 3b+?
– Do BPs worsen CKD?
Methods: To link CPRD, HES and UK Renal Registry (and use Danish and Spanish data to validate).
CPH models with propensity matching
bristol.ac.uk
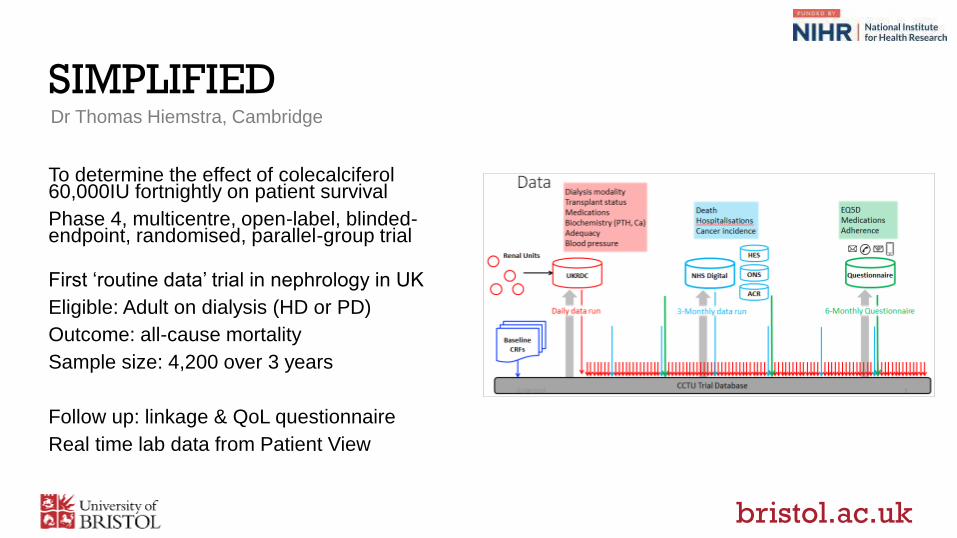
SIMPLIFIED
To determine the effect of colecalciferol60,000IU fortnightly on patient survival
Phase 4, multicentre, open-label, blinded-endpoint, randomised, parallel-group trial
First ‘routine data’ trial in nephrology in UK
Eligible: Adult on dialysis (HD or PD)
Outcome: all-cause mortality
Sample size: 4,200 over 3 years
Follow up: linkage & QoL questionnaire
Real time lab data from Patient View
Dr Thomas Hiemstra, Cambridge
bristol.ac.uk
Other work underway
VICORI
Virtual Cardio-oncology research initiative
CI Dr Dave Adlam, Leicester
Linking:
The National Cardiac Audit Programme (NCAP)
National Cancer Registration and Analysis Service (NCRAS)
Aims to investigate if:
cardiac conditions are managed differently in cancer patients and cardiovascular outcomes are influenced by a prior cancer diagnosis
if cardiovascular treatments, interventions and surgery alter cancer risk or outcomes
if cancer treatments cause long term adverse cardiovascular diseases states or cardiovascular events
if pre-existent cardiac disease alters cancer management or outcomes
bristol.ac.uk
Other work underway
QECKD
Quality and Equity in Cardiac care in Kidney Disease: the promise of big data
CI Dr Jemima Scott, Bristol
Linking:
The National CKD Audit
MINAP
HES, CR & PEDW
UKRR
Aims to explore:
the completeness of acute coronary syndrome (ACS) event capture by MINAP and HES, and determine the validity of the use of admission creatinine (at time of ACS) as a proxy for pre-admission CKD stage.
access to care and outcomes post ACS for the CKD and RRT populations.
From this pilot work we can plan large-scale research studies investigating CVD in CKD populations.
bristol.ac.uk
Brief
1. Describe the current data sets, registries and other resources in renal disease,
cardiovascular, stroke, diabetes and obesity
2. Examples of integration between different disease datasets
3. What is needed to maximise collection and presentation of data to underpin
multi-morbidity research
bristol.ac.uk
What is needed going forwards?
All the data sitting in one place already linked, released for research on a single application!
If that’s not possible:
– Patience (and apply for permissions to link through a trusted third partner)
A better understanding of the suitability of statistical methods to draw causal inferences, particularly with reference to:
– Capturing all the confounding by indication in the routine data
– Time varying nature of confounding/ confounding by indication
bristol.ac.uk
Conclusion
There are lots of data out there
Permissions required – getting clearer
Several organisations are working to bring them together for research
Great opportunities for epidemiology and health inequalities
BUT
Do they capture all the confounders?
What can we conclude applying novel statistics to observational data?

Thank you for your attention
Studies cited:
Trimethoprim and AKI – Dr E Crellin (London)
BisCKD – Prof D Prieto Alhambra (Oxford)
SIMPLIFIED – Dr T Hiemstra (Cambridge)
VICORI – Dr D Adlam (Leicester)
QECKD – Dr J Scott (Bristol)
@fjcaskey @bristolrenal
Related Documents











