Data Analysis of the Burden of MDR-TB in India in 2011 Fairleigh Dickinson University Prof. Ashraf Mohammed MADS 6643 Community Needs Assessment and Quality Analysis Masters in Administrative Sciences (Global Health) 31 July 2014 TEAM -2 Humera Aslam 1636878 Keerti Kiran Mattapally 1598657 Manasvini Vimal Kumar 1637545 Sai Kishore Lanka 1599327

Data analysis of the burden of mdr tuberculosis in india in 2011
Jan 14, 2017
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Data Analysis of the Burden of MDR-TB in India in 2011
Fairleigh Dickinson UniversityProf. Ashraf Mohammed
MADS 6643
Community Needs Assessment and Quality AnalysisMasters in Administrative Sciences (Global Health)
31 July 2014TEAM -2
Humera Aslam 1636878Keerti Kiran Mattapally 1598657Manasvini Vimal Kumar 1637545Sai Kishore Lanka 1599327

Introduction contd..• Tuberculosis is an ancient disease identified as spinal tuberculosis in Egyptian
mummies..history dates to 1550-1080 BC.
Common organisms causing/spreading TB• Human type Mycobacterium Tuberculosis.• Human type Mycobacterium Africans.• Bovine Type Mycobacterium Bovis.• Vole type Mycobacterium Microti.
Source: Bing pictures. Retrieved from: http://www.bing.com/images/search?q=picture+of+M.
+TUBERCULOSOS&id=B2F487239F0BEE2386013843D306355248A850CD&FORM=IQFRBA#a

Introduction: Multi Drug Resistant Tuberculosis
Definition: Multidrug-resistant TB (MDR TB) is caused by an organism that is resistant to at least isoniazid and rifampin, the two most potent TB drugs. (CDC and Prevention, 2012)
XDR-TB:TB that is resistant to minimum four of the core anti-TB drugsInvolves resistance to the two most powerful anti-TB drugs-isoniazid and rifampicinin addition to resistance to any of the fluoroquinolones (such as ofloxacin or moxifloxacin) and to at least one of three injectable second-line drugs (amikacin, capreomycin or kanamycin) (Contd..)

WORLD STATSITICS ON TB (Intro. Contd..)• TB kills 2 million people worldwide/year• 2 billion people suffer from TB in the world, NOW i.e. 30% of world population• TB contributes to 38% of world’s DALYs lost (WHO, 2014). • 9 million NEW TB cases each year (World Medical Association, 2014)• BRICS Countries notify 46% incidence and 40% of all TB related deaths• 30% of world’s TB burden attributed to South Africa (WHO, 2014)• 500,000 of 9 million are MDR TB• 250,000 of MDR TB cases are in China + India i.e. 50% of global burden• For India, major reasons: - Improper diagnosis, treatment, follow up and compliance - Improper notification - Social stigma associated (World Medical Association, 2014)
(Contd..)

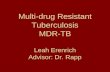
Distribution of Burden of TB in the world
India 21%
China 14%
Other countries
19%
Other 13HBCs
Philippines 3%
Pakistan 4%
Ethiopia 3%
Bangladesh 4%
S. Africa 5%
Nigeria 5%
Indonesia 5%

Aims, Objectives and Purpose • Aim : To estimate the burden of MDR-TB in India in 2011
• Objectives: 1. To identify the steps taken by the Indian government (RNTCP) towards the treatment of MDR-TB in India during 2011.
2. To evaluate the prescribing habits of the physicians in treatment of MDR-TB in India during 2011.
3. To investigate the relation between occupation and burden of MDR- TB in India during 2011.
• Purpose : To understand the reasons and identify possible interventions for the burden of MDR-TB in India.

Method• Method: Review of literature from
WHO website Journal articles available from Center of Disease Control and Prevention Peer reviewed journal articles and Information from websites and publications of government bodies in India • Study setting: Meeting at FDU campus and holding meetings at home• Target population: Population deemed affected by TB and surveyed in previous
researches and that added to the databases of governmental organizations• Sampling: Not used since only literature review done• Study Design: Observational study by researching articles and reviewing literature• Inclusion Criteria: Articles on websites of WHO, CDC and Prevention, Ministry
of Health and Family Welfare, India, and NCBI, web pages of reknown newspapers and
• Exclusion Criteria: Information from Wikipedia, social networking sites and non-academic or unreliable media

Literature Review:MDR TB statistics in India, for 2011
INDIA’s TB BURDEN-ranks II among 27 High TB Burden countriesINDIA carries 1/5th of world’s MDR TB (Bhargava, Pinto & Pai, 2011)>80% of the burden is caused by PREMATURE deaths(WHO India, 2014)WHO estimates- 63,000 cases of MDR-TB in India in 2011RNTCP-10,267 cases (The Hindu, 2012).RNTCP is world’s largest anti-TB program > 1.5 million TB cases are diagnosed and treated /year under RNTCP21,000 new MDR TB cases (Data given by WHO)45,000 MDR TB cases among previously treated (Data given by WHO) 3% in new cases and 12-17% in retreatment cases (Global Health education & WHO, 2012)
GAP- Surveillance of medical practitioners’ prescribing habits in order to decrease the incidence of MDR-TB in India

Literature Review:MDR TB statistics in India, for 2011MDR TB
statistics in India
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2009 2010 2011 2012
Figure Legend
MDR-TB cases detected
MDR TB cases enrolled for treatment
Note: Sharp rise in no. of cases after 2011Reason: following slideSource:World Health Organization. (2013). Multi Drug Resistant Tuberculosis: October 2013 update. Retrieved from: http://www.who.int/tb/challenges/mdr/mdr_tb_factsheet.pdf?ua=1
Years

Mismanagement of TB by medical practitioners in India
No. of second line drugs in Rx No. of doctors prescribing No. of appropriate regimen Rx
5 4 1
4 5 1
3 8 3
2 16 3
1 35 0
0 13 0
Analysis of physician’s prescriptions for MDR-TB.Source: Udwadia et al., 2010
Notable points:6 out of 106 participating physicians prescribed correctly
106 different physicians prescribed 63 separate drug regimens3 out of 106 physicians prescribed correctly for MDR-TB
(Source: Udwadia et al., 2010 )

Prescriptions and Antibiotic Resistance
• Lack of surveillance over invariable administration of antibiotics –Increased Resistance• Drug Pressure – resistance against medicines• Unsupervised prescriptions available at pharmacies• Self Medication due to cheap availability• Lack of healthcare facilities• Overcrowded hospitals, clinics• Lack of knowledge of hazards• Antibiotic resistance-not treated as a medical issue• 2 way- approach 1. Use antibiotics for people who need them 2. Decrease the requirement of antibiotics and improve immunity of the people• Encourage doctors to practice in rural India (Ganguly, 2011)

Lit. Review: Reasons for rise in MDR TB cases in 2011see Table 5
Est. MDR-TB Notified
MDR-TB
MDR-TB
MDR-TB
DST labs
Nat Ref
Second
National
Approved
Infection
in the report among notified MDR-TB enrolled on treatment surveillance per 10m Lab line drug Guidelines expansion controlTB cases cases treatment success / survey pop. stock out plan plan

Reasons for rise in MDR TB cases contd..
Lack of awareness-free medication for TB (Global Health education, 2012) Stigma associated with TB, people ignore ‘common cough’ (Babu & Laxminarayan, 2012) Visit to private hospitals lack of supervision, spend money expensive treatment leave medication drug resistance (Bhargava, Pinto & Pai, 2011)
Improper use of anti-TB drugs a) Prescribing for other diseases/symptoms Primary Resistance b) Stopping due to side effects c) Inadequate administration of drugs
d) Little regulation of OTD sale Poor /underutilized diagnostic facilities (Bhargav, Pinto & Pai, 2011) TB made notifiable only in 2012 (MHFW, (India) 2012) Health care workers ignore epidemiological, treatment and control aspects (Bhargava, Pinto &
Pai, 2011)

Social Determinants of TB in India• Socio-economic inequalities - access to healthcare living conditions psychosocial circumstances risk factors• High numbers and movement of population - lack of food /unavailability - malnutrition - poor ventilation, overcrowding - unawareness about free treatment options• Inappropriate diagnosis and treatment• Non-adherence to treatment regimen• Unavailable healthcare facilities and poor transportation (James et al, 2011)

Relation between occupations and TB incidence
• Who had a history of exposure to TB (OR = 10.92, 95% CL 4.92-24.22) • Four silica-using industries-quarrying (OR = 3.96, 95% CL 0.36-44.02)• Nonmetallic mineral and stone products (OR = 4.00, 95% CL 0.72-22.10)• Pottery and related products (OR = 1.99, 95% CL 0.49-8.06)• Hospitals (OR = 2.10, 95% CL 1.08-4.10)• Eating and drinking establishments (OR = 2.83, 95% CL 1.11-7.20)• Ship and boat building and repair (OR = 1.84, 95% CL 0.76-4.43)• Agriculture (OR = 2.31, 95% CL 0.82-6.50) (Rosenman, 1996) ODDS Ratio: Ratio of probability of TB occurring in these occupations to that of not
occurring

RNTCP’s Role in reducing DALYs lost (1997-2006)
Achievements: COST BENEFIT ANALYSIS
• 1.3 million deaths averted• Total health benefit = 29.2 million disability-adjusted life years (DALYs)• Estimated loss without intervention in 2006, =1.8 times more DALYs lost• Economic well being achieved=US$88.1 billion• Total public expenditure = US$ 768 million• RNTCP’s share=US$ 299 million• Government’s contribution=US$ 469 million• Average cost of TB control=US$ 26/DALY• Contributing return of US$ 115/$ spent (Goodchild et al, 2011).

Fraction of TB patients getting cured-A stacked venn diagram
Source:Bhargava, A., Pinto, L. & Pai, M. (2011). Mismanagement of tuberculosis in India: cause, consequences and the way forward. Hypothesis. 9. (1). 1-13. Retrieved from: http://www.hypothesisournal.com/wp-content/uploads/2011/09/vo0l9no1-hj09.pdf

Most burdened Indian state-Jharkhand• Jharkhand is one of the states of India is highly epidemic toward this disease• Spread of TB Disease in Jharkhand in the year 2010-2011 (Mishra & Srivastava,
2014).
Population covered by Revised National TB Control Program (RNTCP)
Number of suspect examined
Number of smear positive patients diagnosed
Total patients registered for treatment
Number of all smear positive cases registered within seven days of diagnosis
Number of all smear positive patients registered within one month of diagnosis
Number of pediatric TB patients out of all new smear positive patients
31,500,000 155,738 23,051 38,574 18,356 21,289 1794

Limitations of the review
• Concentrates on literature available for 2011, not recent• Review does not compare Indian scenario with other HBCs in detail• It just estimates the burden of the disease, detailed treatment modalities
not given• Corrective measures for social determinants of TB not listed• Could not focus on each and every district of India

RESULTS
1. RNTCP has been successful in treating TB patients and reducing burden by averting 1.3 million deaths in 2006
2. Prescriptions are not supervised, and uncalled for antibiotic administration due to lack of surveillance, easy availability and self medication causes severe drug resistance
3. Occupations involving silica exposure, non metal minerals’ mining and hospital environment exposure increase the risk of contracting Tuberculosis

Recommendations
• Strict surveillance for MDR –TB cases and pharmacists against selling antibiotics without prescriptions
• Rapid strides in RNTCP program penetration • Notification of all TB bases as well as suspected TB cases• Strict rules on sale of any medicines without prescription• Training Needs Assessment for doctors and healthcare staff and training to be
carried out• RNTCP should be helped financially by the government • NGOs’ participation in spreading awareness

Discussion/ConclusionThere is a definite and urgent need to tackle MDR-TB on a war footing basis, with
primary objectives being notification of disease (TB), discouragement of administration of antibiotics invariably and at the drop of a hat and saving lives. Increased awareness among private practitioners with training for proper use of antibiotics is required and regular surveillance by RNTCP with deployment of trained health care force and sophisticated testing methods may contribute to decreasing the burden of MDR-TB
Conclusion: Burden of MDR -TB in India is very high, in fact second only in the world and rigorous concentrated efforts are needed to address the issue

ACKNOWLEDGEMENT
We would like to sincerely thank Prof. Ashraf Mohammed for his incessant help,
guidance and support to us in reviewing this literature and for answering our
innumerable questions smilingly. This presentation would not have been possible
without his constant supervision.
We would also like to heartily thank our classmates for helping us throughout the
development of the slides and further, would also like to express our gratitude to
the jury who took time to come here and advise us towards improvement.
Sincerely,
Team 2
31 July 2014

References• Babu, R.G & Laxminarayan, R. (2012). The unsurprising story of MDR TB
resistance in India. Elsevier Health Journal. 92. 301-306. Retrieved from: https://www.academia.edu/4171244/REVIEW_The_unsurprising_story_of_MDR-TB_resistance_in_India
• Bhargava, A., Pinto, L. & Pai, M. (2011). Mismanagement of tuberculosis in India: cause, consequences and the way forward. Hypothesis. 9. (1). 1-13.
Retrieved from: http://www.hypothesisjournal.com/wp-content/uploads/2011/09/vo0l9no1-hj09.pdf
• Dhar, A. (2012 ,March 30).India contests WHO figures for multi drug resistant TB. The Hindu. Retrieved from:
http://www.thehindu.com/sci-tech/health/policy- and-issues/india-contests-who-figures-for-multidrug-resistant-t b/article3251900.ece
• Ganguly, N.K. (2011). Situation analysis: Antibiotic use and resistance in India. Global Antibiotic Resistance Partnership.Retrieved from:
http://www.cddep.org/sites/cddep.org/files/publication_files/India-report-web.pdf?issuusl=ignore
• Goodchild,M., Sahu, S.,Wares, F., Dewan, P., Shukla, R.S., Chauhan, L.S., &Floyd, K. (2011). A cost-benefit analysis of scaling up tuberculosis control in India. The International Journal of Tuberculosis and Lung Disease.15. (3).358-362. Retrieved from: http://www.ncbi.nlm.nih.gov/pubmed/21333103

References contd..
• James, R.H., Boccia, D., Evans, C.A., Adato, M., Petticrew, M. & Porter, J.D.H. (2011). The social determinants of tuberculosis: From evidence to action. Am J Public Health 101.(4). 654-662. doi: 10.2105/AJPH.2010.199505
• Mishra, B. K. & Srivastava, J. (2014). Mathematical model on pulmonary and multidrug-resistant tuberculosis patients with vaccination. Journal of Egyptian Mathematical Society. 22. (2). 311-316. Retrieved from http://www.sciencedirect.com/science/article/pii/S1110256X13000965
• Ministry of Health and Family Welfare. (2012). Guidance for TB notification in India. Retrieved from: http://www.tbcindia.nic.in/pdfs/Guidance%20tool%20for%20TB%20notifica tion%20in%20India%20-%20FINAL.pdf
• Rosenman, K.D. & Hall, N. (1996).Occupational risk factors for developing tuberculosis.Pubmed. 30.(2).148-154. Retrieved from: http://www.ncbi.nlm.nih.gov/pubmed/8844044
• Udwadia ZF, Pinto LM, Uplekar MW (2010) Tuberculosis Management by Private Practitioners in Mumbai, India: Has Anything Changed in Two Decades? PLoS ONE 5(8): e12023. doi:10.1371/journal.pone.0012023
• World Medical Association, Inc. (2014). Tuberculosis. WMA. Retrieved from: http://www.wma.net/en/20activities/30publichealth/70tuberculosis/index.html

References contd..
• World Health Organization. (2014). Tuberculosis in BRICS: challenges and opportunities for leadership within the post-2015 agenda. Bulletin of the World Health Organization. Retrieved from: http://www.who.int/bulletin/volumes/92/6/13- 133116/en/
• WHO India, (.2014). World TB Day 2013. WHO India. Retrieved from: http://www.searo.who.int/india/topics/tuberculosis/tbday_2013/en/
Related Documents