Dana V. Wallace, MD Dana V. Wallace, MD Assistant Clinical Professor Assistant Clinical Professor Nova Southeastern University Nova Southeastern University Davie, Florida Davie, Florida [email protected] [email protected]

Dana V. Wallace, MD Assistant Clinical Professor Nova Southeastern University Davie, Florida [email protected].
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dana V. Wallace, MDDana V. Wallace, MDAssistant Clinical ProfessorAssistant Clinical Professor
Nova Southeastern UniversityNova Southeastern UniversityDavie, FloridaDavie, Florida
[email protected]@gmail.com

ANAPHYLAXIS IN THE OFFICEANAPHYLAXIS IN THE OFFICEALLERGIST ALLERGIST and Staffand Staff BE PREPARED BE PREPARED
Templates and Forms Templates and Forms
ARE IMPORTANT!ARE IMPORTANT!
Templates & Forms for SITTemplates & Forms for SIT Cox, L., H. Nelson, et al. Cox, L., H. Nelson, et al. "Allergen "Allergen
immunotherapy: a practice parameter third immunotherapy: a practice parameter third update." update." J Allergy Clin ImmunolJ Allergy Clin Immunol 127127(1 Suppl): (1 Suppl): S1-55.S1-55.– http://www.jacionline.org/article/PIIS00916749100150
34/addons
[jacionline][jacionline] www.acaai.orgwww.acaai.org
– (ACAAI > Members > Practice Resources > Skin (ACAAI > Members > Practice Resources > Skin Testing & Immunotherapy)Testing & Immunotherapy)
Kalier, M., Lockey, R., edsKalier, M., Lockey, R., eds. Clinical Allergy and . Clinical Allergy and Immunology SeriesImmunology Series, 4, 4thth Edition Edition
www.drdanawallace.comwww.drdanawallace.com

Discussing SCIT Treatment OptionDiscussing SCIT Treatment Optionwww.drdanawallace.com

SLIT Patient Info (Part 1)SLIT Patient Info (Part 1)

SLIT Patient Info (Part 2)SLIT Patient Info (Part 2)

SLIT Patient Info (Part 3)SLIT Patient Info (Part 3)

SLIT Side EffectsSLIT Side Effects

Allergy Immunotherapy Allergy Immunotherapy Consent process should discuss:Consent process should discuss:
Treatment and alternativesTreatment and alternatives Potential benefitPotential benefit Potential risks, giving frequency of adverse Potential risks, giving frequency of adverse
events, including deathevents, including death Cost associated and coverage optionsCost associated and coverage options Anticipated duration of TxAnticipated duration of Tx Office policies that affect Tx, e.g. waiting Office policies that affect Tx, e.g. waiting
time, missed AIstime, missed AIs
Based on 2011 Immunotherapy PP

Consent to Allergen Consent to Allergen ImmunotherapyImmunotherapywww.acaai.org

CONSENT FORMS TO CONSIDERCONSENT FORMS TO CONSIDER
Allergy testing & immunotherapyAllergy testing & immunotherapy Permission to treat a minorPermission to treat a minor Consent to take allergy vaccine out of Consent to take allergy vaccine out of
office to another MD for administrationoffice to another MD for administration Consent from remote MD agreeing to Consent from remote MD agreeing to
administer AIadminister AI Privacy form to authorize info to specific Privacy form to authorize info to specific
people- e.g. child custody people- e.g. child custody
www.drdanawallace.com

Consent to take Allergen Extract Consent to take Allergen Extract Sets to another officeSets to another office
www.acaai.org

Cross-reacting AllergensCross-reacting Allergens jacionline

Recommended Documentation SCIT Recommended Documentation SCIT Prescription (Rx) Forms Prescription (Rx) Forms
Purpose:Purpose: – To define the contents of the allergen immunotherapy To define the contents of the allergen immunotherapy
extract in enough detail that it could be precisely extract in enough detail that it could be precisely duplicatedduplicated
Patient information: Patient information: – Name, chart number (if applicable), birth date, Name, chart number (if applicable), birth date,
telephone number (home/mobile), email, & picturetelephone number (home/mobile), email, & picture Preparation information: Preparation information:
– Name of person (& signature) preparing the allergen Name of person (& signature) preparing the allergen immunotherapy extract & date preparedimmunotherapy extract & date prepared
– Vial name, by allergens included (e.g., Trees, Grass or Vial name, by allergens included (e.g., Trees, Grass or abbreviations (e.g., T, G, with legend)abbreviations (e.g., T, G, with legend)
jacionline
Recommended Documentation SCIT Recommended Documentation SCIT Prescription (Rx) Forms Prescription (Rx) Forms
Allergen immunotherapy extract content information Allergen immunotherapy extract content information for for eacheach allergen: allergen:– Common name or genus and speciesCommon name or genus and species
– Concentration of available manufacturer’s extract Concentration of available manufacturer’s extract
– Volume of manufacturer’s extract to add to achieve the Volume of manufacturer’s extract to add to achieve the projected effective concentrationprojected effective concentration
• Calculate by dividing the projected effective concentration Calculate by dividing the projected effective concentration by the concentration of available manufacturer’s extract by the concentration of available manufacturer’s extract times the total volume times the total volume
– Extract manufacturer & lot number, expiration dateExtract manufacturer & lot number, expiration date
– Same detail for all mixes Same detail for all mixes
Vial expiration date should not exceed of any of the Vial expiration date should not exceed of any of the individual components individual components
jacionline

SCIT Prescription FormSCIT Prescription Form jacionline
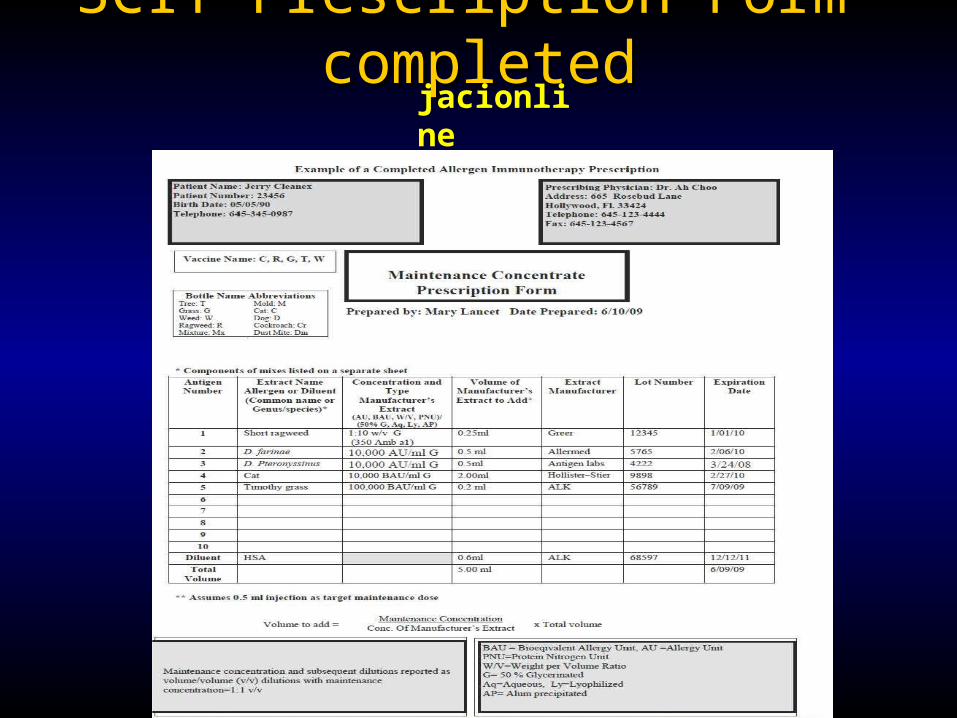
SCIT Prescription Form-completedSCIT Prescription Form-completedjacionline

IMMUNOTHERAPYRX FORM
MODIFIED BY DANA WALLACE,MD
Name: Jane Doe Chart #: 3341 Bottle Name: A
DOB: 8/29/1948 Bottle #: 177
Maintenance Concentrate Content Rx Total Vials 4
Allergen, Concentration Available, Manufacturer, Lot # , Expiration date
Projected Effective
Concentration available
Volume in ml extract to add
Remake if same Lot
1 Australian Pine 1:10 C 1C00061 8/19/03 1/100 1/10 0.50
2 Bald Cypress 1:10 C 2D00061 1/8/04 1/100 1/10 0.50
3 Bayberry 1:10 C 1J00041 1/8/04 1/100 1/10 0.50
4 Mulberry, Red 1:10 C 1J44691 3/24/03 1/100 1/10 0.50
5 Baccharia 1:20 G 225-40-2A19 10/2/03 1/100 1/10 0.50
6 Dog Fennel 1:10 C 1L3291 7/14/03 1/100 1/10 0.50
7 Pigweed, Spiny 1:10 C 0M00081 8/4/03 1/100 1/10 0.50
8 Ragweed, Short 1:10 C 1L00191 2/4/03 1/100 1/10 0.50
9 Sheep Sorrel 1:10 C 1G00191 5/1/03 1/100 1/10 0.50
10 Yellow Dock 1:10 C 0M00431 7/14/03 1/100 1/10 0.50
11 None 0 1/10 0.00
12 None 0 1/10 0.00
A=ALK 5.00C=Center 0.00
5 G+Greer 5HS=Hollister Steer
0.5 injected 1ml injectedMite Pteronysinus 1200 AU/ml 600AU/mlMites Farinae 4000 AU/ml 2000 AU/ml Date and Signature Cat 5000 BAU/ml 2500 BAU/mlOther Animals 1:100/ml 1:200/mlStandardized Grassed 8000 BAU/ml 4000 BAU/mlPollens 1:100/ml 1:200/mlMolds 1:50/ml 1:100/ml
High Protease:Dust Mites, Molds, Cockroach Low Protease: Pollens. Cat, Dog
Do not mix high with low protease allergens May mix low with low, high with high
Ragweed may be mixed in either group. Keep venomous insects separate
Remakes Date, initals & Date, initals & Date, initals & Date, initals &
Bottle Color/Vial Dilutions Volume:Volume Expiration Expiration Expiration Expiration
Brown 1:10,000,000 4 wks
Peach 1:1,000,000 4wksPink 1:100,000 4wksSilver 1:10,000 4wksGreen 1:1,1000 6wks
Blue 1/100 6mths
Yellow 1/10 6mthsRed Full Strength Earliest expiring constituent
Jane Doe Vial A
Dana V. Wallace MD 2699 Stirling Road Suite B305 Ft. Lauderdale,FL 33312 954-963-5363 fax 963-7099Revised 9/02
1/100
5
1/10 Australian Pine 1:10 C 1C00061 8/19/03
Bald Cypress 1:10 C 2D00061 1/8/04
Bayberry 1:10 C 1J 00041 1/8/04
Mulberry, Red 1:10 C 1J 44691 3/24/03
Dog Fennel 1:10 C 1L3291 7/14/03
Baccharia 1:20 G 225-40-2A19 10/2/03
Pigweed, Spiny 1:10 C 0M00081 8/4/03
Ragweed, Short 1:10 C 1L00191 2/4/03
Sheep Sorrel 1:10 C 1G00191 5/1/03
Yellow Dock 1:10 C 0M00431 7/14/03
None
None
1/100
1/100
1/100
1/100
1/100
1/100
1/100
1/100
1/100
1/10
1/10
1/10
1/10
1/10
1/10
1/10
1/10
1/10
1/10
1/10
5
Projected Effective ConcetrationAnitgen
Total ExtractDiluent
Total Volume
Factor is volume to be injected X 10
www.acaai.org (ACAAI > Members > Practice Resources > Skin Testing & Immunotherapy)

Labels for allergen Labels for allergen immunotherapy extracts immunotherapy extracts
Each vial must have Each vial must have appropriate patient appropriate patient identifiersidentifiers, e.g., name, number, DOB, picture, e.g., name, number, DOB, picture
Contents, e.g, T, G, M, Df, D, etc.Contents, e.g, T, G, M, Df, D, etc. The dilution from the maintenance concentrate The dilution from the maintenance concentrate
(vol/vol) using color, numbers, letters(vol/vol) using color, numbers, letters Expiration date of individual vialExpiration date of individual vial
jacionline

Allergy Extract Vial Dilution & LabelingAllergy Extract Vial Dilution & Labelingwww.acaai.org

Allergy Extract Vial Dilution & LabelingAllergy Extract Vial Dilution & Labelingwww.acaai.org

Vial LabelsVial Labels www.acaai.org

Weekly Build-up TherapyWeekly Build-up Therapy jacionline

Cluster SCIT ScheduleCluster SCIT Schedule jacionline


SLIT Proposed SchedulesSLIT Proposed Schedules
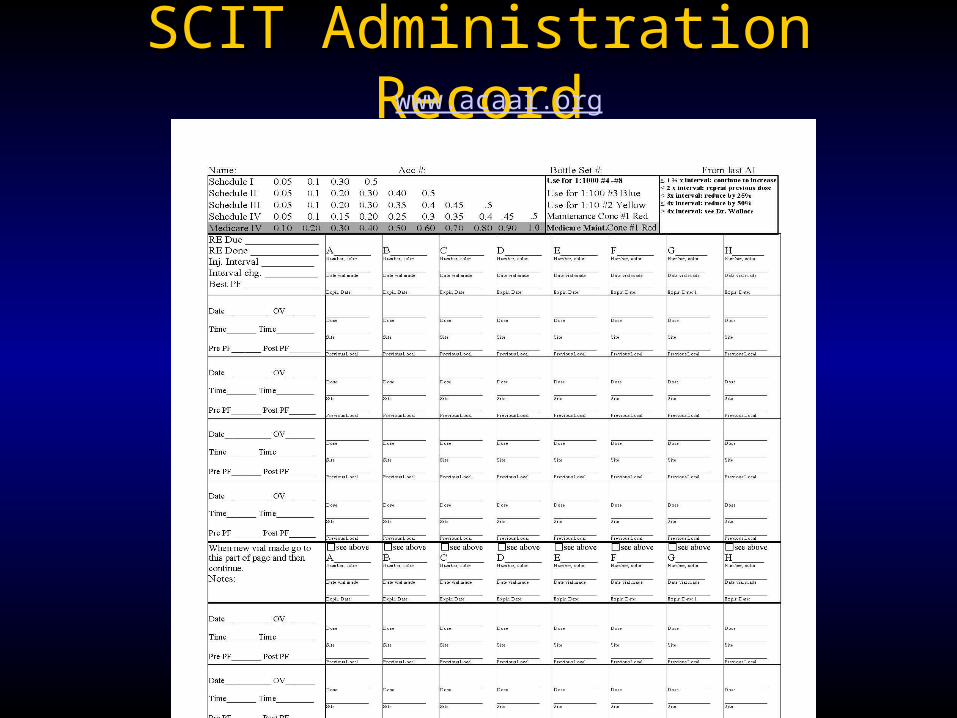
SCIT Administration RecordSCIT Administration Record List info in separate columnsList info in separate columns
– Date of injectionDate of injection– Arm administeredArm administered– Delivered volume in mmDelivered volume in mm– Currently on antihistamine (desirable)Currently on antihistamine (desirable)
Projected build-up scheduleProjected build-up schedule Description of any reaction (details may Description of any reaction (details may
appear on separate sheetappear on separate sheet Peak flow- pre and post SCIT may be Peak flow- pre and post SCIT may be
includedincluded
jacionline

IImmmmuunnootthheerraappyy VVaacccciinnee AAddmmiinniissttrraattiioonn FFoorrmm
Best Baseline Peak Flow: ___________________
Date Time Health screen abnormal1
Anti-histamine
taken?2
Peak
Flow
Arm Vial Number
or Dilution
Delivered
Volume
Reaction 3
Arm Vial Number
or Dilution
Delivered
Volume
Reaction Injector
Initials
1. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______
2. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 3. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 4. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 5. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 6. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 7. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 8. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 9. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 10. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 11. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 12. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 13. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 14. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 15. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 16. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 17. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 18. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 19. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L ________ ________ _________ _______ 20. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L _______ ________ _________ _______ 21. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L _______ ________ _________ _______ 22. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L _______ ________ _________ _______ 23. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L _______ ________ _________ _______ 24. ___/____/____ _______ Y N Y N ___________ R L ________ ________ ____________ R L _______ ________ _________ _______
1. Health screen refers to either a written or verbal interview of the patient prior to the administration of the allergy injection regarding: the presence of increased allergy or asthma symptoms or symptoms of respiratory tract infection, beta-blocker use, change in health status (including pregnancy) or adverse reaction to previous injection. A yes answer to this health screen may require further evaluation (see health screen record on back page). 2. Antihistamine use: to improve consistency in interpretation of reactions it should be noted if the patient has taken an antihistamine on injection days. Physician may also request that an antihistamines be taken consistently on injection days: recommended: Y N 3. Reaction: refers to either immediate or delayed systemic or local reactions. Local reactions (noted as LR) can be reported in millimeters as the longest diameter of wheal and erythema.. The details of the symptoms and treatment of a systemic reaction (noted as SSRR) would be recorded elsewhere in the medical record. Guidelines for dose reduction after a systemic reaction on a separate instruction sheet.
Date to reorder: __/__/__
Vaccine Name Abbreviations* Tree: T Mold: M Grass: G Cat: C Weed: W Dog: D Ragweed: R Cockroach: Cr Mixture: Mx Dust Mite: Dm
SCHEDULE Vial 5 Vial 4 Vial 3 Vial 2 Vial 1
Injector signature
Initials
Patient Name: Date of Birth: Patient Number: Telephone Number: Diagnosis:
Prescribing Physician: Address: Telephone: Fax:
Dilution Color
Vial number
1:10,000 (v/v) Silver
5
1:1000 (v/v) Green
4
1:100 (v/v) Blue
3
1:10 (v/v) Yellow
2
Maintenance 1:1 (v/v) Red
1 Expiration date(s)
____/____/____ ____/____/____ ____/____/____ ____/____/____ ____/____/____
Vial A: Extract name* Vial B: Extract name
Vaccine A: vaccine contents* Vaccine B: _______________
ALLERGY INJECTION
ADMIN. FORM
www.acaai.org (ACAAI > Members > Practice Resources > Skin Testing & Immunotherapy)
Health Screen Form (Pre SCIT)Health Screen Form (Pre SCIT)
Patient identifiers, date, baseline peak flow & BP, Patient identifiers, date, baseline peak flow & BP, if advised to use antihistamines with SCITif advised to use antihistamines with SCIT
Records status of: Records status of: – Asthma control, consider standardized instrument and Asthma control, consider standardized instrument and
Peak Flow pre and postPeak Flow pre and post
– Beta-blocker useBeta-blocker use
– Pregnancy or other recent health care status, including Pregnancy or other recent health care status, including recent infection or allergy/asthma flarerecent infection or allergy/asthma flare
– Previous adverse reaction to SCITPrevious adverse reaction to SCIT
– Consider BP measurementConsider BP measurement
jacionline
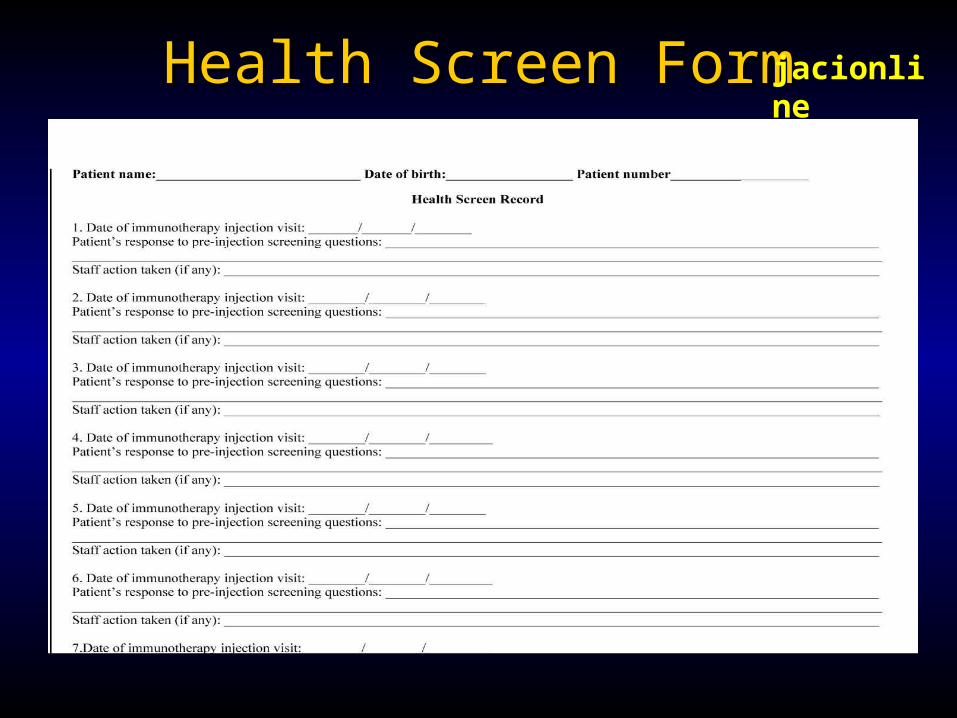
Health Screen FormHealth Screen Form jacionline
PRE-INJECTION
HEALTH SCREEN
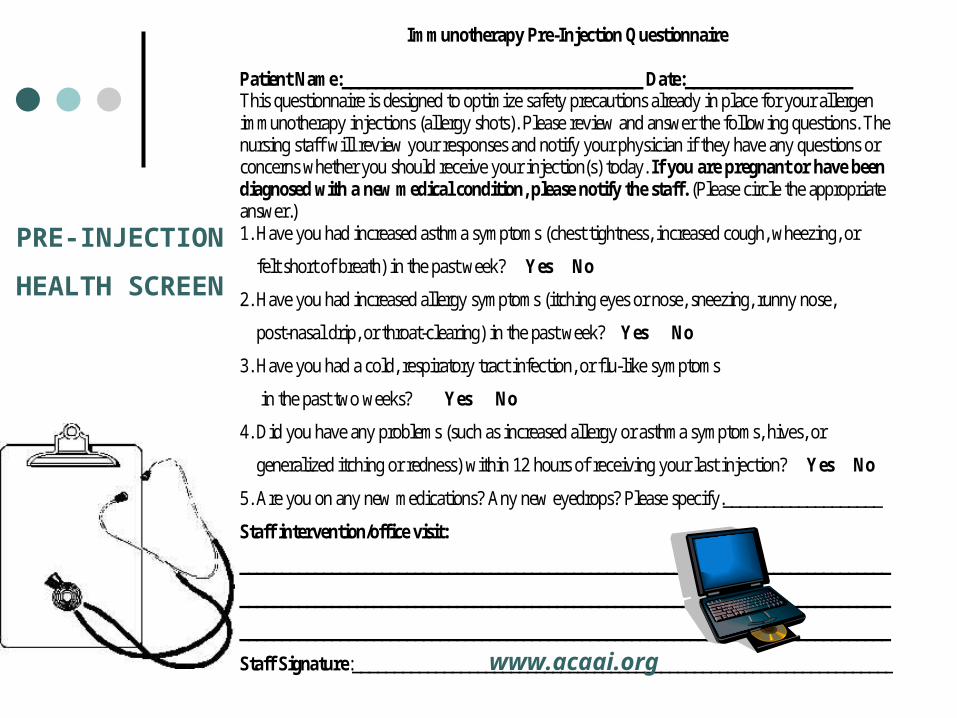
Immunotherapy Pre-Injection Questionnaire
Patient Name:____________________________________ Date:____________________ This questionnaire is designed to optimize safety precautions already in place for your allergen immunotherapy injections (allergy shots). Please review and answer the following questions. The nursing staff will review your responses and notify your physician if they have any questions or concerns whether you should receive your injection(s) today. If you are pregnant or have been diagnosed with a new medical condition, please notify the staff. (Please circle the appropriate answer.) 1. Have you had increased asthma symptoms (chest tightness, increased cough, wheezing, or
felt short of breath) in the past week? Yes No
2. Have you had increased allergy symptoms (itching eyes or nose, sneezing, runny nose,
post-nasal drip, or throat-clearing) in the past week? Yes No
3. Have you had a cold, respiratory tract infection, or flu-like symptoms
in the past two weeks? Yes No
4. Did you have any problems (such as increased allergy or asthma symptoms, hives, or
generalized itching or redness) within 12 hours of receiving your last injection? Yes No
5. Are you on any new medications? Any new eyedrops? Please specify.___________________
Staff intervention/office visit:
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Staff Signature:_________________________________________________________________ www.acaai.org

Preparing your office staff for Preparing your office staff for ANAPHYLAXISANAPHYLAXIS
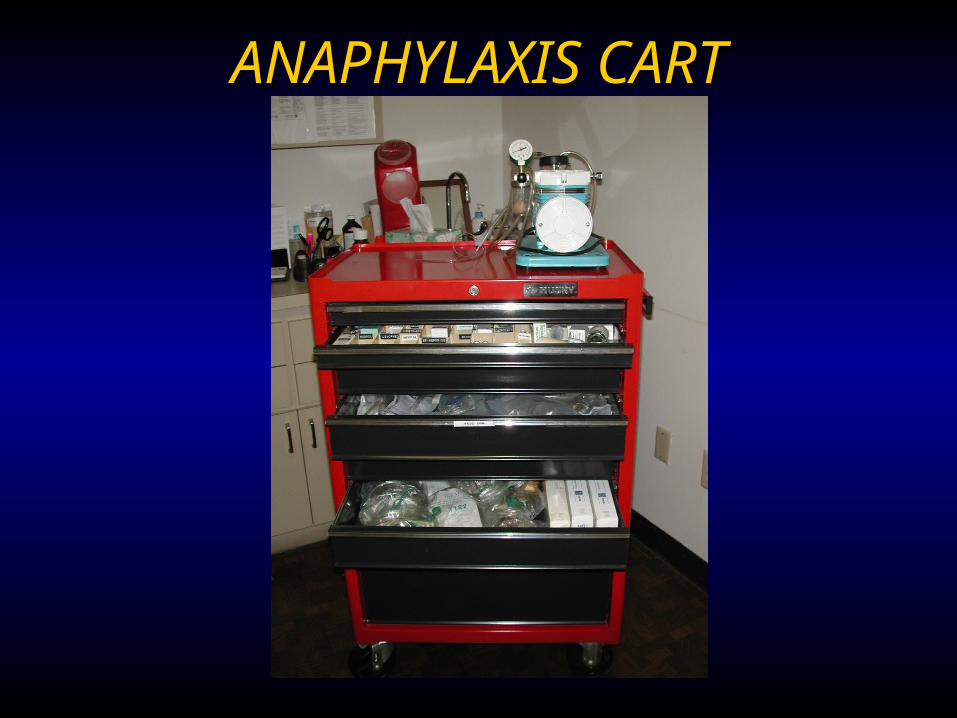
ANAPHYLAXIS CARTANAPHYLAXIS CART

Supplies and Equipment for Anaphylaxis Treatment in office
“NECESSARY” Stethoscope and Stethoscope and
sphygmomanometersphygmomanometer *Epinephrine 1:1000*Epinephrine 1:1000 OxygenOxygen IV FluidsIV Fluids Tourniquets, syringes, Tourniquets, syringes,
hypodermic needles, hypodermic needles, large-bore needles large-bore needles
“CONSIDER HAVING”” One-way valve facemaskOne-way valve facemask Diphenhydramine inj.Diphenhydramine inj. Corticosteroids inj.Corticosteroids inj.
“MAYBE” Vasopressor (Dopamine)Vasopressor (Dopamine) GlucagonGlucagon Automatic defibrillatorAutomatic defibrillator Oral airwayOral airway
* Required 2011 JTF Anaphylaxis PP

ANAPHPYLAXIS CART INVENTORY AND UPDATE LIST
2005
ANAPHYLAXIS CART
Algorithm for Tx Treatment Recording Sheet Pulse Oximeter Stethoscope Twin Jet Nebulizer Ambu Bag- Child (450 ml) (2)
Adult (1500ml) (2) (Disposable, latex-free)
Sphygmomanometer & cuffs: child, Adult regular, and oversized
Laryngoscopes Adult and Pediatric (optional)
Defibrillator with heart monitor (Optional)
IV ADMINISTRATION DRUGS IV Pole Epinephrine 1:1000 1cc ampules (10) 1000cc .9 Normal Saline (4 bags)
Hydroxyethyl starch (Hespan) 500 ml bag (2) Epinephrine 1:10,000 10cc pre-mixed syringes (2)
(Optional) 3-Way Stopcock (2) Epinephrine 1:1000 30 cc multidose vials (1)
Micro drip IV set (2) 60 gtt/ml
Benadryl (diphenhydramine) IV 1 ml ampule, 50 mg/ml (2)
Macro drip IV (2) 10-15 gtt/ml Benadryl liquid 12.5 mg/ml (4 oz) & 25 mg tablets (10) Extension tubing (2) Zyrtec (Cetirizine) 5mg/ml (4 oz), 5 mg (5) & 10 mg (5)
tablets T-Connector (2) Zantac(ranitidine HCL) IV 2 ml vial, 25 mg/ml (2) Catheters #22, 20, 18 (2 each) Zantac(ranitidine HCL) PO 1 oz, 15 mg/ml & 150 mg
tablets Butterfly Needles #21, #19 (3 each) Albuterol 2.5 mg unit dose (3) or Xopenex 1.25 mg (3)
and .63 mg (3) inhalant solution Syringes 1cc, 5cc, 10cc, 20cc, 50cc (5 each) Atrovent Inhalant solution .083% unit doses (2) Needles # 16, #18, #20, #22 (5 each) Aminophylline IV, 500 mg vial , 50 mg/cc(1) Tourniquet (2) Prednisolone Syrup 15 mg/tsp 4 oz Cushioned IV Boards (2) Solu-Medrol 1 ml vial, 40 mg/ml (3)
4x4 cotton sponges (10) Medrol 4 mg tablets # 20
1” tape Synthetic (Transpore) Atropine (ipratropium bromide) 4 ml vial, 0.5 mg/ml (2) Alcohol Swabs (10) Dopamine 10cc vial, 40 mg/ml (2) Latex Free Gloves- 1 box M, L Glucagon 1 mg vial (3 vials) Saline 30 cc, 10 cc (5 each) NaHCO3 50 mEq/50 ml (Optional) (2) D5W 250 ml (4), 500 ml (1), 30 ml (2) Calcijex IV calcium 1 mg/ampule (Optional)
Valium IV 10 ml vial (Optional)
AIRWAY OXYGEN DELIVERY Face mask-infant, toddler, child, adult O2 E-Tank with wheeled carrier Oral Airways-6 cm, 7cm, 8cm, 9 cm, 10cm Gas regulator Endotracheal tubes 3.5, 5,6,7, 8, 9, 10
(optional) Tank wrench
Scalpel, disposable (2) Pediatric oxygen mask Adult oxygen mask Nasal canula
Extension tubing Note (#) number of units to order Check and restock monthly and after each use:
Year_______
Month Initial Month Initial Month Initial Month Initial
Jan. April July Oct.
Feb. May Aug. Nov.
March June Sept. Dec.
Practice Name Practice Address
Practice Phone Number
www.acaai.org

ANAPHYLAXIS TREATMENT
www.drdanawallace.com

Drug Start Strength Add Final dilution or max
A=adult, C=child Method of Delivery Frequency Adult
(A) Child < 12 (C) Dose/kg ***
X wt in KG = Dose
Epinephrine Aqueous (Epi)
1:1000 1ml=1mg= 1000mcg
1:1000 Max .3 mg C
IM lateral thigh
Q ≤ 5 min 0.2-0.5 mg (ml) 0.01mg (ml) /kg max 0 .3 mg
X _____ =___ mg (ml)
Auto Injector (Epi-Pen or TwinJect)
1:1000 1ml=1mg
1:1000 IM lateral thigh
Q ≤5 min SR, .3 mg JR , 0.15 mg <15 kg .15 mg
Epi Infusion 1st choice after IM
1:1000 1ml=1mg
250 ml D5W 1:250,000=4.0μg/ml IV infusion continual 1-4 μg/min=.25-1.0 ml/min (15-60 microdrops/minute)
0.1 μg/kg/min X_____
_______ 1 μg=.25ml
μg/ min
Epi IV (or IO) after cardiac arrest, if not responding to infusion or Tracheal (T)
1:1000 1-3ml=1-3mg 1:1000
9-27 ml Saline None
1:10,000 1:1000, .3 max C
IV #1 slow push Over 3 minutes Flush T with 10 ml saline A, 5ml C
3-5 minutes rapid
10-30 ml T: .3-.5ml of 1:1000
.1ml/kg (0.01 mg/ kg ) max 0.3 mg=3ml T: .05-.1 ml/kg
X_____ X_____
=______ =______
ml ml
Epi IV after cardiac arrest, if not responding to above
1:1000 3-5ml=3-5 mg
27-45 ml Saline
1:10,000 IV #2 Over 3 minutes
3-5 minutes 10-30 ml
1ml/kg (0.1 mg/kg) max 30 ml
X______ X_______
=______ =______
ml ml
Epi IV high dose infusion after cardiac arrest, if not responding to above
1:1000 1mg= 1 ml
250 ml D5W 1:250,000=4.0μg/ml Max 10 μg/min A, C
IV infusion continual 4-10 μg/min=1.0-2.5ml/min (60-150 microdrops/minute)
0.1 μg/kg/min and ↑ up to 10 μg/min
X_______ _______ 1 μg=.25ml
μg/ min
Diphenhydramine (Benadryl) IV/IM/PO
50 mg/ml IV/IM 12.5 mg/5ml PO
Or 25 mg PO tablet/capsule
Max 24 hr A=400 mg C=300 mg
IM/IV PO
repeat 1x PRN then q 6 hr
25-50 mg 1 mg /kg or 2 mg /kg
X______ X______
=______ =_____
mg mg
Cetirizine (Zyrtec) PO 5 mg/5ml or 5 mg, 10 mg tablet
PO 10 mg PO-A
2.5-10 mg PO-C mg
Ranitidine HCl (Zantac) IV/IM/PO
25 mg/ml IV/IM 75 mg/5 ml or 150 mg tablet PO
20 ml D5W for IV
IV over 5 minutes PO
Q 6 hr
50 mg IV/IM 150 mg PO
1 mg/kg IV/IM 2 mg/kg PO
X______ X______
=______ =______
mg mg
Albuterol 2.5 mg in 3 ml .083% Nebulized Q 20 min 2.5 mg 1.25-2.5 mg 1.25-2.5 mg Levalbuterol (Xopenex) .63-1.25 mg in 3
ml Nebulized Q 20 min 1.25 mg 0.63-1.25 mg 0.63-1.25 mg
Ipratropium bromide (Atrovent)
.02% in 2.5 ml vial May add to Albuterol or Xopenex
Nebulized Q 6 hr 500 mcg= 1 vial
250-500 mcg = ½-1 vial
250-500 = ½-1 vial
mcg
Aminophylline (optional)
500 mg/10 ml Add to 100 ml Saline, micro drip
IV over 30 minutes 5 mg/kg 5 mg/kg X______ =______ mg
Normal Saline 1000 ml bags 1-2 L needed in adult
IV infusion over first 60 minutes
Continue, but reduce after BP stable
20-30 ml/kg 25% first 10 minutes
30 ml/kg X______ =______ ml
Hydroxyethyl starch Hespan (2nd choice)
500 ml IV infusion over first 60 minutes
500 ml 30 ml/kg X______ =______ ml
Methylprednisolone (Solu-Medrol)
40 mg/ml Max 2 mg/kg/24 hr IV push Q 6 hours 1 mg/kg 1 mg/kg X______ =______ mg
Prednisolone (Pediapred) 5 mg/5 ml PO ? repeat X1 in 6 hrs 25-50 mg 0.5 mg/kg X______ =______ mg Methylprednisolone 4 mg PO ? repeat X1 in 6 hrs 20-40 mg 0.4 mg/kg X______ =______ mg Atropine 0.5 mg/ml Max 2 mg A
Max 1 mg C Subcut. Q 10 min. .3-.5 mg 0.02 mg X______ =______ mg
Glucagon (Side effects= N and V)
1 mg/ml = 1000 μg/ml
If Infusion use D5W or Saline
Max 1 mg C IV over 5 min Follow with Infusion 5-15 μg/minute
1-5 mg 20-30 μg/kg (1 mg max)
X_____ =______ mg
NaHCO3 50 mEq/50 ml 2nd dose ½ first dose IV Q 10 min 50-100 mEq 1 mEq/kg X______ =______ mEq Dopamine 400 mg 500 ml D5W 800 μg/ml IV infusion to ↑ BP 2-20 μg/kg/minute 2-20 μg/kg/minute X______ =______ μg/min
Patient Name_______________________Patient Name_______________________ TABLE OF ANAPHYLAXIS DRUGSTABLE OF ANAPHYLAXIS DRUGS
www.drdanawallace.com
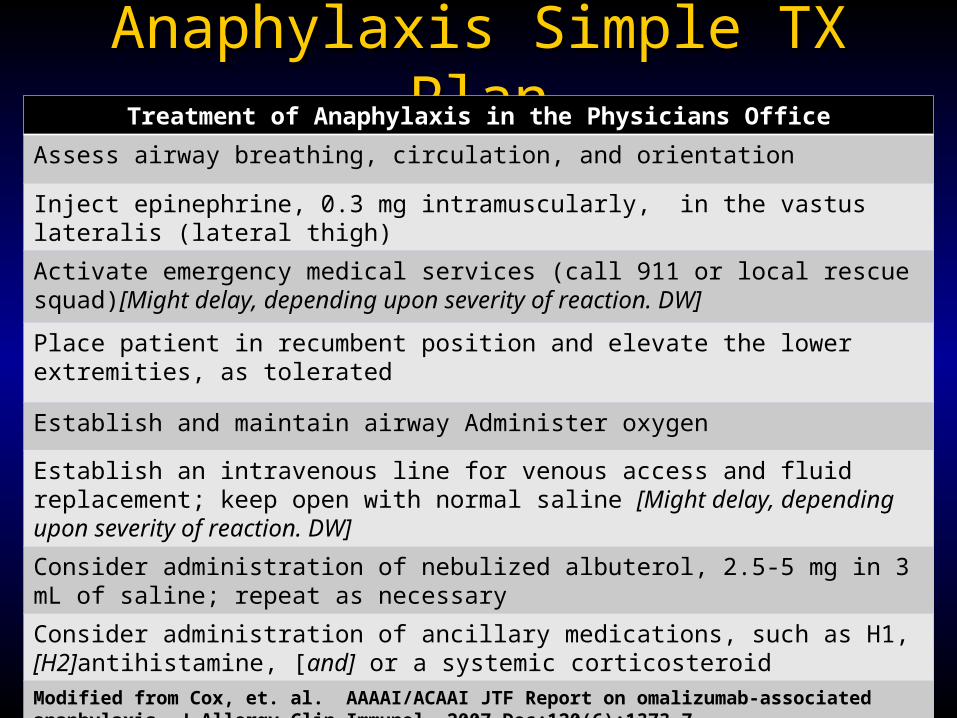
Anaphylaxis Simple TX PlanAnaphylaxis Simple TX PlanTreatment of Anaphylaxis in the Physicians Office
Assess airway breathing, circulation, and orientation
Inject epinephrine, 0.3 mg intramuscularly, in the vastus lateralis (lateral thigh)
Activate emergency medical services (call 911 or local rescue squad)[Might delay, depending upon severity of reaction. DW]
Place patient in recumbent position and elevate the lower extremities, as tolerated
Establish and maintain airway Administer oxygen
Establish an intravenous line for venous access and fluidreplacement; keep open with normal saline [Might delay, depending upon severity of reaction. DW]
Consider administration of nebulized albuterol, 2.5-5 mg in 3 mL of saline; repeat as necessary
Consider administration of ancillary medications, such as H1, [H2]antihistamine, [and] or a systemic corticosteroid
Modified from Cox, et. al. AAAAI/ACAAI JTF Report on omalizumab-associated anaphylaxis. J Allergy Clin Immunol. 2007 Dec;120(6):1373-7.

POST AN ANAPHYLAXIS PROTOCOL POST AN ANAPHYLAXIS PROTOCOL AND/OR ALGORITHM (in visible location )AND/OR ALGORITHM (in visible location )

Allergen Immunotherapy Systemic Reation/Anaphylaxis Treatment Record
Name:________________________ Date________________________________ Date of Birth__________________ Prescribing Physician__________________ Allergens: Tree-Grass-Weed-Mites-Cockroach-Animal Dander-Mold-Hymenoptera Prior systemic rxn:__________ Hx of asthma?_____________ Date/time of injection:_________________ Date/time of rxn:____________________ Dilution (Vial #): ________________ New? Yes No History of the systemic reaction (SR): Immediate measures: __Assess airway, breathing, circulation, and orientation __Epinephrine IM into thigh __Activate EMS (call 911 or local rescue squad) Y/N Time called:______AM/PM __Management algorithm reviewed (as needed) Signs & Symptoms: Respiratory: Skin : Eye/Nasal: Vascular Other: Shortness of breath Hives Runny nose Hypotension Difficulty swallowing Wheezing Angioedema Red eyes Chest discomfort Abdominal pain, nausea, diarrhea Cough Generalized itch Congestion Dizziness Diaphoresis Stridor Flushing Sneezing Headache Time
Resp. rate/ PEFR Pulse/ O2 Saturation
BP
Intervention, Medications, Exam Comments
Time (AM/PM)/ Condition upon release:_____________________________________________________ Patient instructions:______________________________________________________________________ Follow-up call to patient: Time________ Comments:___________________________________________ Clinical impression: True SR Questionable SR No SR Comments:_________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Dosage adjustment?: ____________________________________________________________________ Signatures_______________________________ RN ___________________________________MD/DO
ANAPHYLAXIS TX RECORD
www.acaai.org

WAO Grading System for SCIT Systemic WAO Grading System for SCIT Systemic Reactions: Reactions: GRADE 1- one organ systemGRADE 1- one organ system
42

WAO Grading System for SCIT Systemic WAO Grading System for SCIT Systemic Reactions: Reactions: GRADE 2GRADE 2
Symptoms/signs of more than one organ system presentSymptoms/signs of more than one organ system presentoror
Lower respiratoryLower respiratory Asthma: cough, wheezing, SOB (e.g. < than 40% PEF or FEV1 Asthma: cough, wheezing, SOB (e.g. < than 40% PEF or FEV1
, responding to inhaled bronchodilator), responding to inhaled bronchodilator)oror
GastrointestinalGastrointestinal Abdominal cramps, vomiting, or diarrheaAbdominal cramps, vomiting, or diarrhea
OrOr
OtherOther: uterine cramps: uterine cramps
Patients may describe a feeling of doomPatients may describe a feeling of doom
Might include any of the symptoms listed in grade 1

WAO Grading System for SCIT Systemic WAO Grading System for SCIT Systemic Reactions: Reactions: GRADE 3GRADE 3
Lower respiratoryLower respiratory Asthma (e.g. 40% PEF or FEV1 Asthma (e.g. 40% PEF or FEV1 ))
oror
Upper respiratoryUpper respiratory Laryngeal, uvula, or tongue edema with or Laryngeal, uvula, or tongue edema with or
without stridorwithout stridor
Note: Might include any of the symptoms listed in grade 1 and 2Patients may describe a feeling of doom

WAO Grading System for SCIT Systemic WAO Grading System for SCIT Systemic Reactions: Reactions: GRADE 4GRADE 4
Lower or upper respiratoryLower or upper respiratory– Respiratory failure with or without loss of Respiratory failure with or without loss of
consciousnessconsciousness
oror
CardiovascularCardiovascular– Hypotension with or without loss of Hypotension with or without loss of
consciousnessconsciousness
Note: Might include any of the symptoms listed in grade 1, 2, and 3Adults may describe a feeling of doom

WAO Grading System for SCIT Systemic WAO Grading System for SCIT Systemic Reactions: Reactions: GRADE 5GRADE 5
DeathDeath
[We [We
MustMust
Prevent]Prevent]

Thank You DANA WALLACE, MDdrdanawallace@gmail.comwww.drdanawallace.comMEDICALPROFESSIONAL (USER NAME)Allergy (PASSWORD)
Related Documents











