Dallas 2015 TFQO: David Boyle COI #26 EVREV 1: David Boyle #COI#26 EVREV 1: Jane McGowan #370 Taskforce: Neonatal Ventilation Strategies in the DR (NRP 809)

Dallas 2015 TFQO: David Boyle COI #26 EVREV 1: David Boyle #COI#26 EVREV 1: Jane McGowan #370 Taskforce: Neonatal Ventilation Strategies in the DR (NRP.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dallas 2015
TFQO: David Boyle COI #26EVREV 1: David Boyle #COI#26EVREV 1: Jane McGowan #370Taskforce: Neonatal
Ventilation Strategies in the DR
(NRP 809)
Dallas 2015COI Disclosure
EVREV 1: Boyle, COI#26: No conflicts
EVREV 2: McGowan, COI#370: No conflicts
Dallas 20152010 Treatment Recommendation
To establish initial lung inflation in apneic newborn infants, initiation of intermittent positive-pressure ventilation at birth can be accomplished with either shorter or longer inspiratory times.
Dallas 2015C2015 PICO
Population: Term and preterm infants who do not establish spontaneous respirations at birth Intervention: Administration of one or more pressure-limited sustained lung inflations (lasting >5) secondsComparison: Intermittent PPV with short inspiratory timesOutcomes: Air leaks (9), overall mortality (9), BPD (8), establishment of FRC (8), mechanical ventilation in first 72 hr (8), time to HR >100 bpm (8), Apgar at 5 minutes (7), CPR in DR (6), intubation in DR (6)
Dallas 2015Inclusion/Exclusion& Articles Found
Inclusions: Human and animal studies (RCTs and nonRCTs) comparing an initial sustained inflation (≥5 sec) immediately after birth to PPV
Exclusions: Mechanical ventilation or other interventions prior to administration of a sustained inflation, an initial sustained inflation of less than 5 seconds, review articles, abstracts
Number of Articles initially identified: 88
Number of articles included: 17RCTs
• Human: 3• Animal: 9
Non-RCTs• Human: 5
Dallas 2015Inclusion/Exclusion& Articles Found
Number in Evidence Profile tables: 5 Evidence Profile Tables include 3 human RCTs and 2 human cohort studies
9 animal studies and 3 human observational studies included in the worksheet provide biologic plausibility/context for this intervention
Dallas 20152015 Proposed Treatment Recommendations
We suggest an initial sustained inflation (>5 seconds duration) should not be used as routine care for preterm infants without spontaneous respirations immediately after birth, but may be considered. (Weak recommendation, Moderate quality of evidence)
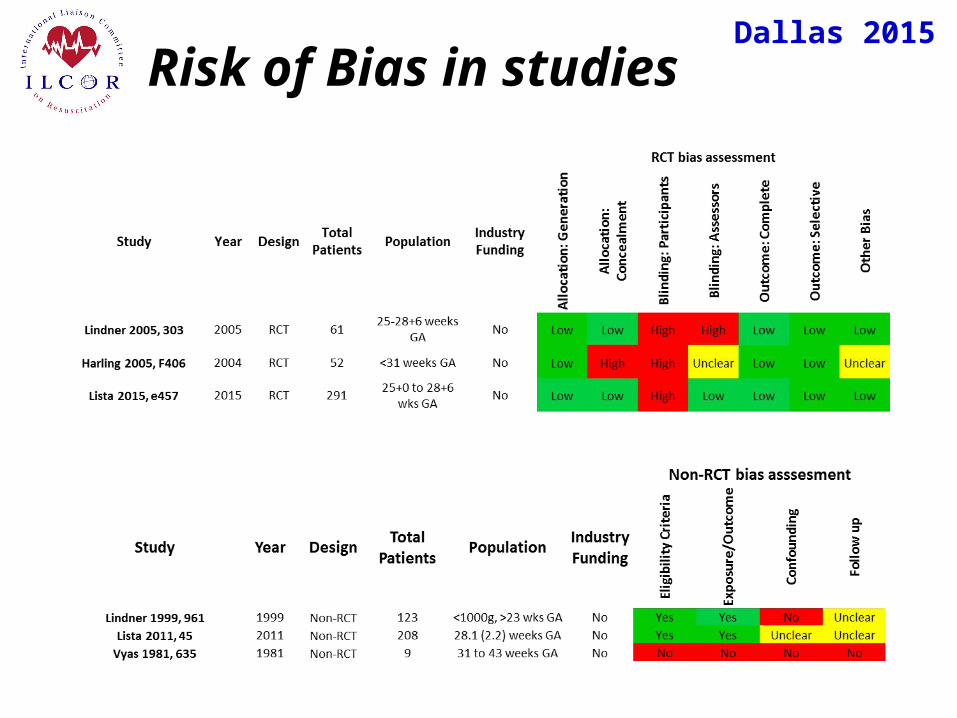
Dallas 2015 Risk of Bias in studies
Dallas 2015Mechanical ventilation <72 hours
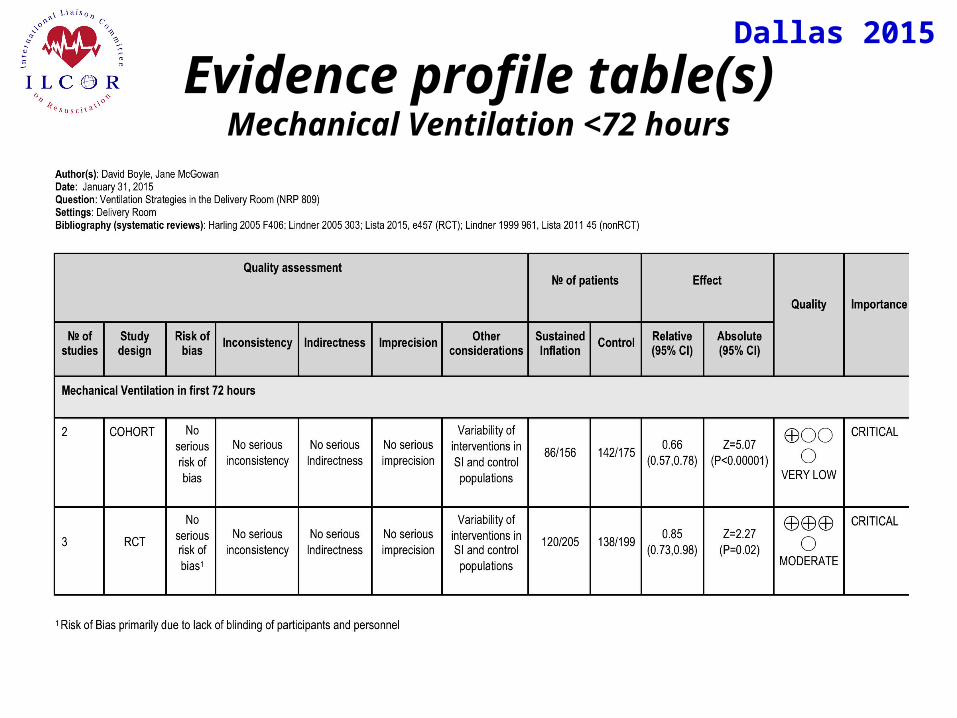
Dallas 2015Evidence profile table(s)
Mechanical Ventilation <72 hours
Dallas 2015BPD
Dallas 2015Evidence profile table(s)
BPD
Dallas 2015Mortality
Dallas 2015Evidence profile table(s)MORTALITY
Dallas 2015Air Leaks
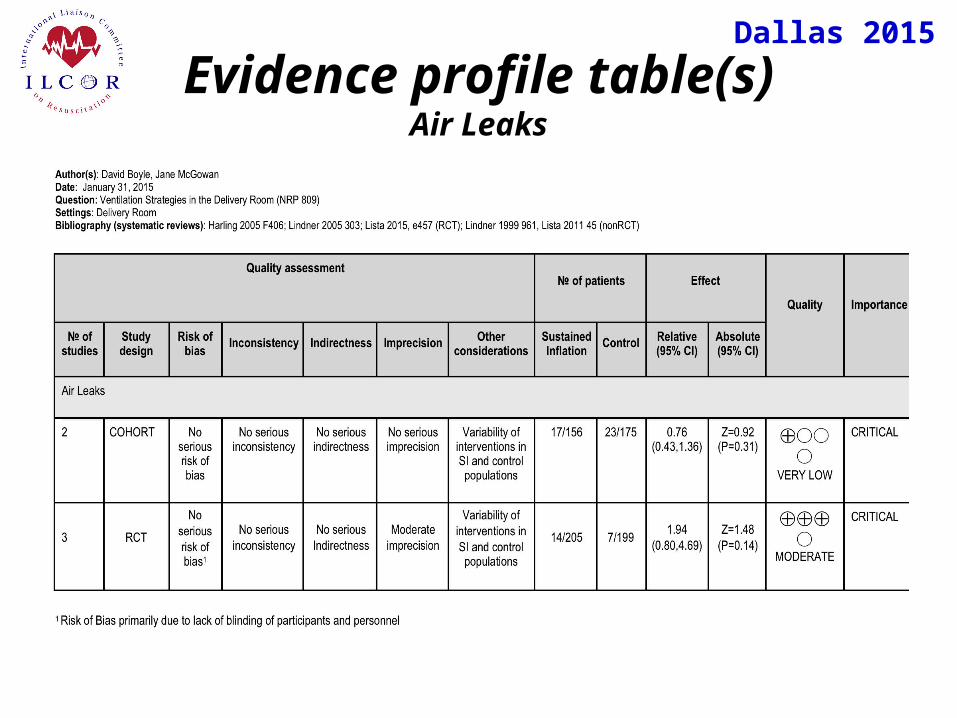
Dallas 2015Evidence profile table(s)
Air Leaks
Dallas 2015Proposed Consensus on Science statements
Regarding the administration of sustained inflation in newborn infants without spontaneous respirations:
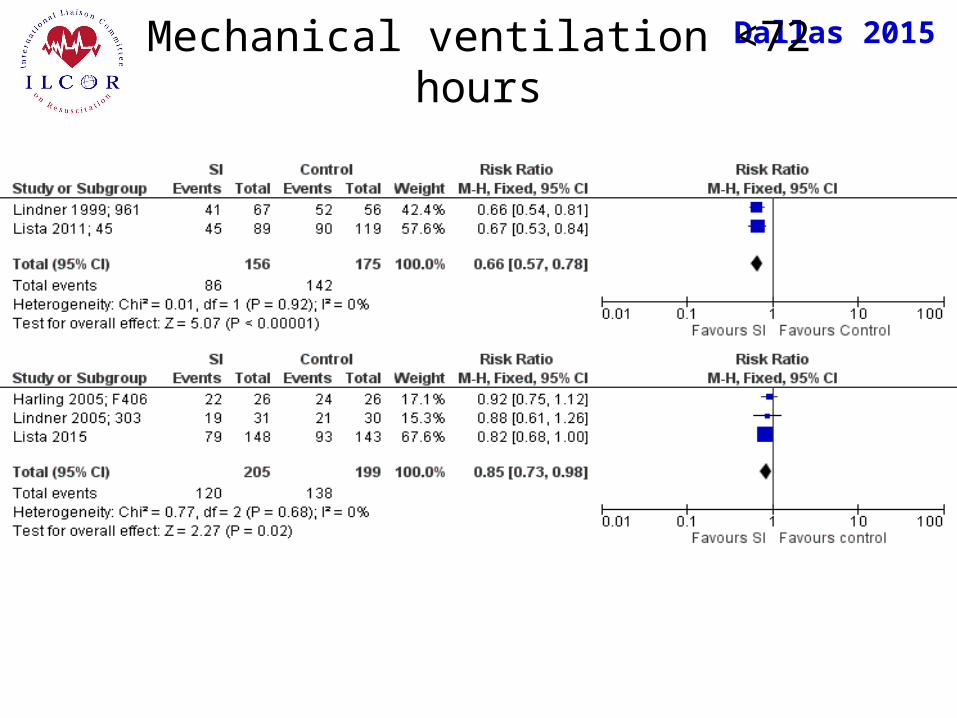
For the critical outcome of need for mechanical ventilation in the first 72 hours after birth, moderate quality evidence (downgraded for other considerations) from three RCTs enrolling 404 newborns showed significant benefit (Harling 2005 F406; Lindner 2005 303; Lista 2015 e457). In addition, very low quality evidence (downgraded for other considerations) from two cohort studies with a total of 331 patients also showed significant benefit (Lindner 1999 961, Lista 2011 45).
Dallas 2015Proposed Consensus on Science statements
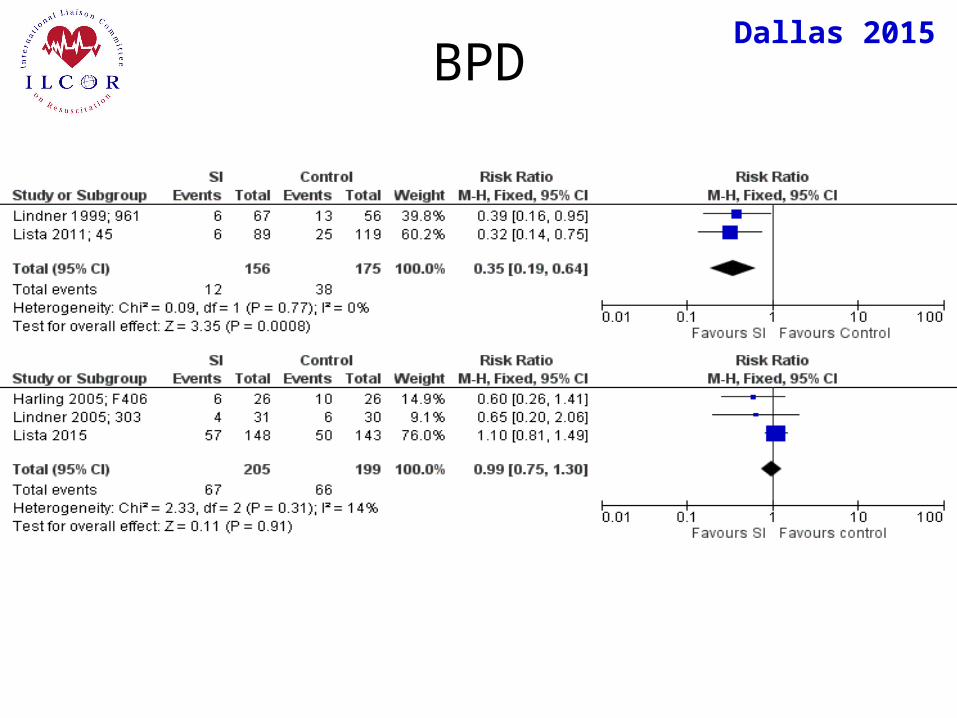
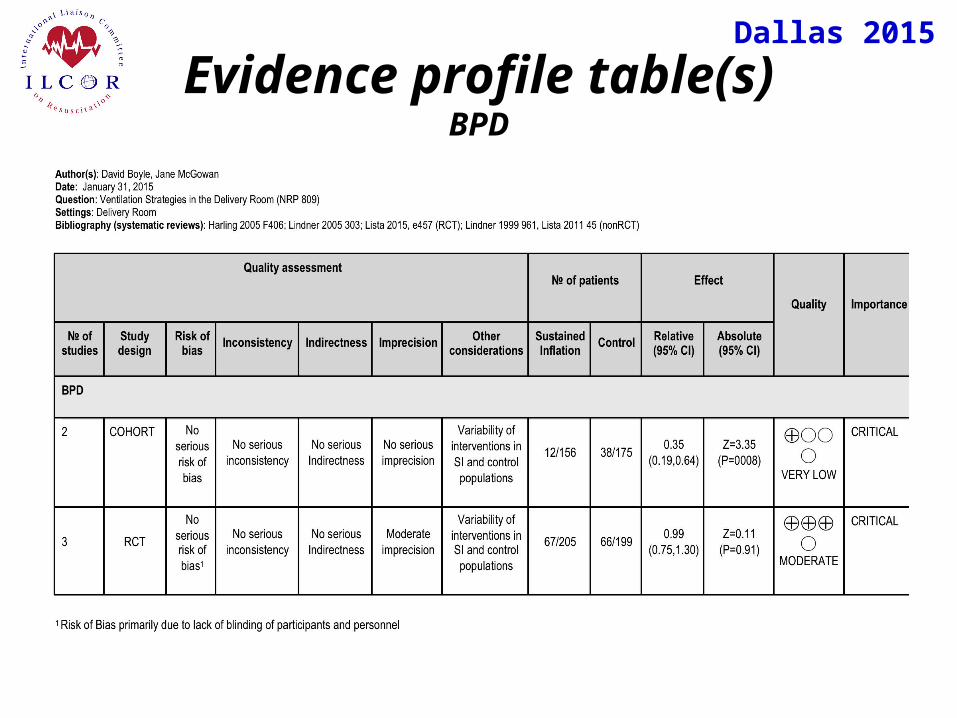
For the critical outcome of BPD, moderate quality evidence (downgraded for moderate imprecision and other considerations) from three RCTs enrolling 404 patients showed no benefit (Harling 2005 F406; Lindner 2005 303; Lista 2015 e457). Very low quality evidence (downgraded for other considerations) from two cohort studies enrolling 331 patients showed significant benefit (Lindner 1999 961, Lista 2011 45).
Dallas 2015Proposed Consensus on Science statements
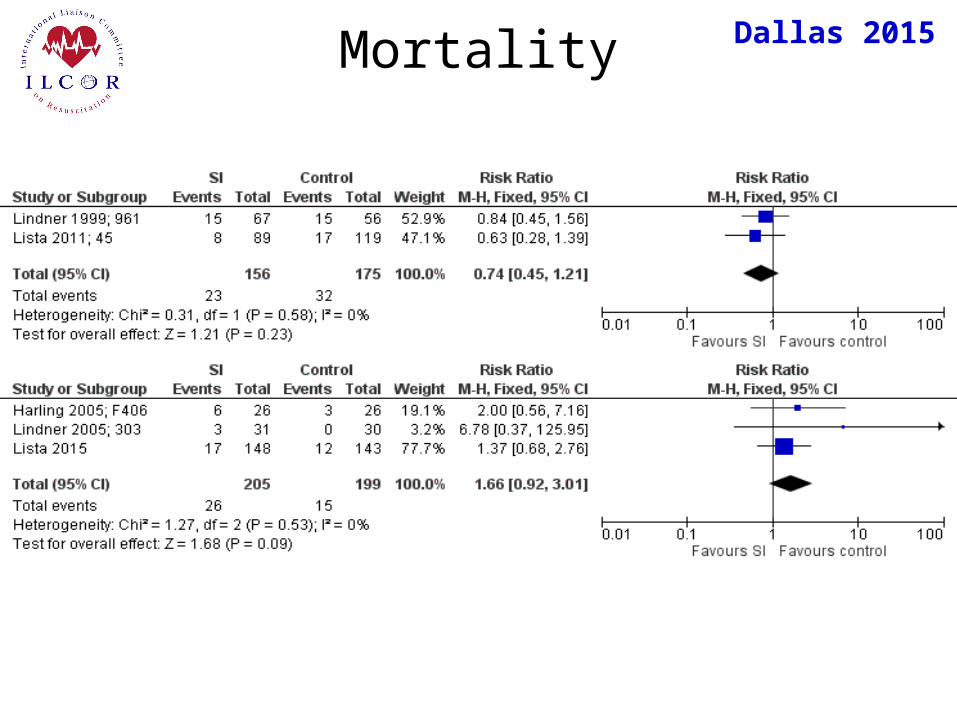
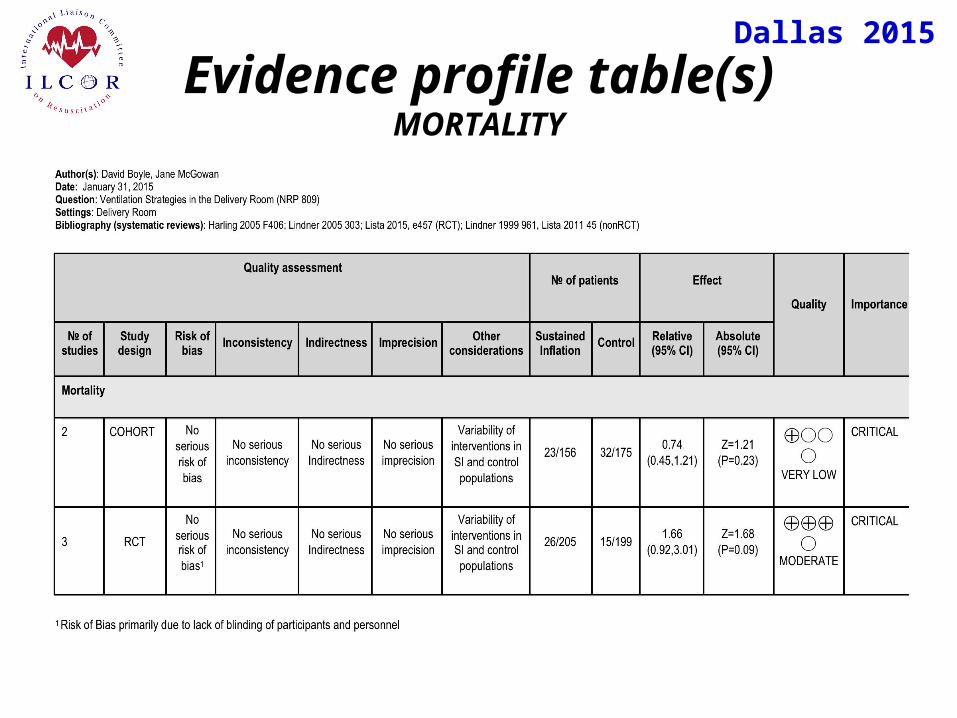
For the critical outcome of mortality, moderate quality evidence (downgraded for other considerations) from 3 RCTs enrolling 404 newborns, and very low quality evidence (downgraded for other considerations) from two cohort studies with a total of 331 patients showed no benefit (Harling 2005 F406; Lindner 2005 303; Lista 2015 e457; Lindner 1999 961, Lista 2011 45).
Dallas 2015Proposed Consensus on Science statements
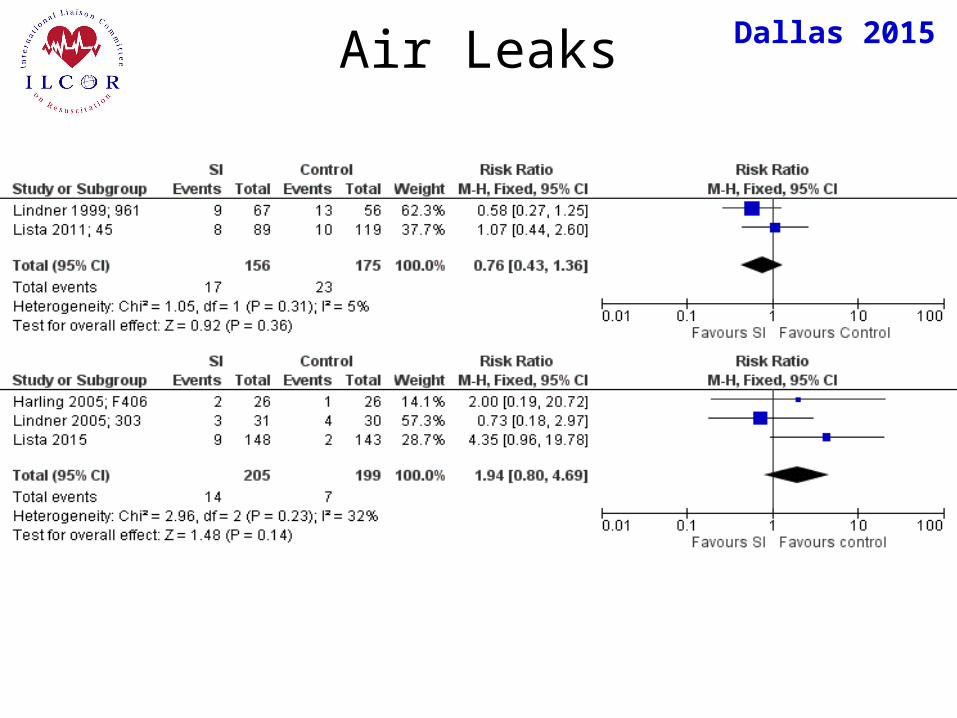
For the critical outcome of air leak, low quality evidence (downgraded for imprecision and other considerations) from three RCTs enrolling 404 newborns (Harling 2005 F406; Lindner 2005 303; Lista 2015 e457) and very low quality of evidence (downgraded for imprecision and other considerations) from two cohort studies with a total of 331 patients (Lindner 1999 961, Lista 2011 45) showed no effect.
For the important outcome of Apgar score, there was no difference between groups in any studies reviewed (Harling 2005 F406; Lindner 2005 303; Lindner 1999 961, Lista 2011 45).
Dallas 2015Proposed Consensus on Science statements
In a small case series of 9 asphyxiated term infants, a prolonged initial inflation of 5 seconds produced a 2-fold increase in functional residual capacity compared with historic controls (Vyas 1981 635).Very low quality evidence from one cohort study (Lindner 1999 961) demonstrated that the need for intubation in the delivery room was significantly lower in infants who received a sustained inflation compared to conventional management.No human studies evaluated time to HR >100 beats per minute, FiO2 in the delivery room, or need for chest compressions in the delivery room (i.e., “bystander CPR”).

Dallas 2015Proposed Consensus on Science statements
Animal studies of the effects of sustained inflation on alveolar recruitment have shown mixed results. Studies in preterm lambs (Sobotka 2011 56; Klingenberg 2013 F222) and preterm rabbits (te Pas 2009 295) showed more uniform lung inflation and better lung compliance if animals received a sustained inflation prior to initiation of mechanical ventilation; however, another study in preterm lambs, showed no benefit after an initial SI (Klopping-Ketelaars 1994 43), and an additional study showed that step-wise increases in PEEP resulted in better overall lung mechanics than treatment with an initial sustained inflation (Tingay 2014 288).
Dallas 2015Proposed Consensus on Science statements
Comparison across studies (RCTs and cohort) was complicated by variation across studies in the duration of the initial sustained inflation (from 5-20 seconds) as well as the initial peak inspiratory pressure (20-30 cm H2O). In addition, investigators used different interface devices to deliver the sustained inflations (endotracheal tube, face mask, nasopharyngeal tube). Three studies repeated the initial SI once (Lindner 1999 961, Lista 2011 451; Lista 2015 e457), one at a higher PIP (Lindner 1999 961); one study repeated the SI twice, increasing the PIP on second application (Lindner 2005 303). Therefore all studies were downgraded for “other considerations”.No studies compared the efficacy of a single sustained inflation to multiple sustained inflations.
Dallas 2015Draft Treatment Recommendations
We suggest an initial sustained inflation (>5 seconds duration) should not be used as routine care for preterm infants without spontaneous respirations immediately after birth, but may be considered. (Weak recommendation, Moderate quality of evidence)
Dallas 2015Draft Treatment Recommendations
Dallas 2015
Knowledge Gaps
Further studies are essential to determine the optimal pressure and duration of sustained inflation that would allow the establishment of FRC while minimizing the risk of barotrauma in the newly born infant, as well as the long-term morbidity. Randomized, controlled trials are needed to determine the optimal duration of initial sustained inflations, the appropriate peak inflation pressure, and the number of inflations that should be administered. Specific research requiredLarger studies in animal models-SI vs PPV, different durations of SIRCT of PPV vs SI using standard devicesFurther studies are need to determine the optimal pressure and duration of sustained inflation that would allow the establishment of FRC while minimizing the risk of barotrauma in the newly born infant. Early outcome measures, e.g., time to heart rate >100 beats per minutePopulation likely to benefit
Dallas 2015Final Comments
One additional human RCT is pending publication (ClinicalTrials.gov #NCT01739114); completed October 2014, estimated enrollment 186.
One RCT identified (Pediatrics Aug--2007; 120 (2): 322-9. A randomized, controlled trial of delivery-room respiratory management in very preterm infants.. te Pas, Arjan B; Walther, Frans J) was excluded from the final analysis due to methodologic variability - use of different interface devices between control and experimental groups (NP tube and T-piece ventilator vs mask and self-inflating bag) as well as enrollment of subjects at multiple time points after delivery. DWB/JEM
Related Documents