Daily Shame and Hostile Irritability in Adolescent Girls With Borderline Personality Disorder Symptoms Lori N. Scott, Stephanie D. Stepp, Michael N. Hallquist, Diana J. Whalen, Aidan G. C. Wright, and Paul A. Pilkonis University of Pittsburgh Recent theoretical and empirical work suggests that adults with borderline personality disorder (BPD) have difficulty regulating both shame and anger, and that these emotions may be functionally related in clinically relevant ways (e.g., Schoenleber & Berenbaum, 2012b). The covariation of shame with anger-related emotions has important clinical implications for interventions targeting shame and uncon- trolled anger in BPD. However, no studies have examined shame, anger, and their covariation in adolescents who may be at risk for developing BPD. Therefore, this study focuses on associations between BPD symptoms and patterns of covariation between daily experiences of shame and anger- related affects (i.e., hostile irritability) in a community sample of adolescent girls using ecological momentary assessment. Multilevel models revealed that girls with greater BPD symptoms who reported greater mean levels of shame across the week also tended to report more hostile irritability, even after controlling for guilt. Additionally, examination of within-person variability showed that girls with greater BPD symptoms reported more hostile irritability on occasions when they also reported greater concurrent shame, but this was only the case in girls of average socioeconomic status (i.e., those not receiving public assistance). Unlike shame, guilt was not associated with hostile irritability in girls with greater BPD symptoms. Results suggest that shame may be a key clinical target in the treatment of anger-related difficulties among adolescent girls with BPD symptoms. Keywords: borderline personality disorder, ecological momentary assessment, hostility, irritability, shame Symptoms of borderline personality disorder (BPD) are usually recognizable by adolescence and are associated with a host of poor long-term outcomes (Chanen & McCutcheon, 2013; Winograd, Cohen, & Chen, 2008). Although prevalence rates are similar across men and women in the general population, studies indicate higher rates of BPD among adolescent girls and young women in clinical and forensic settings, and greater distress and impairment in women with BPD as compared with their male counterparts (APA, 2013; Grant et al., 2008; Rosler, Retz, Yaqoobi, Burg, & Retz-Junginger, 2009). In addition, research has shown that BPD symptoms peak during mid-adolescence, between ages 14 and 17 (Bornovalova, Hicks, Iacono, & McGue, 2009). Research on the early manifestations and characteristics of BPD symptoms during mid-adolescence, especially in girls, is therefore critical in the effort to develop targeted prevention and treatment strategies (Chanen & McCutcheon, 2013). Although BPD is associated with a range of negative affects, recent theoretical and empirical work suggests that adults with BPD have particular difficulties regulating shame and anger- related emotions (Berenson et al., 2011; Gratz et al., 2010; Line- han, 1993). Moreover, several authors have suggested that anger- related affects may be elicited in the context of intense shame among individuals with BPD, perhaps as a defensive attempt to deflect attention away from the shamed self and direct blame to others (Bateman & Fonagy, 2004; Schoenleber & Berenbaum, 2012b; Velotti, Elison, & Garofalo, 2014). According to these theorists, shame could be a prime driver of anger-related emotions and thus may be an important clinical target in the treatment of anger and aggression in those with BPD. However, little empirical work has examined emotional dys- function, let alone patterns of dysregulation and covariation of specific emotional states, among adolescents with emerging BPD symptoms. This is a significant gap considering that proneness to intense shame and anger is associated with poor outcomes and higher likelihood of future self-harm and suicide attempts in adults with BPD (Brodsky, Groves, Oquendo, Mann, & Stanley, 2006; Brown, Linehan, Comtois, Murray, & Chapman, 2009; Rusch et Lori N. Scott, Stephanie D. Stepp, and Michael N. Hallquist, Department of Psychiatry, University of Pittsburgh School of Medicine; Diana J. Whalen and Aidan G. C. Wright, Department of Psychology, University of Pittsburgh; Paul A. Pilkonis, Department of Psychiatry, University of Pittsburgh School of Medicine. Diana J. Whalen is now at the Department of Psychiatry, Washington University. This research and the efforts of the authors were supported by grants from the National Institute of Mental Health (K01 MH086713, PI: Stepp; R01 MH56630, PI: Loeber; R01 MH056888, PI: Pilkonis; K01 MH101289, PI: Scott; F32 MH097311, PI: Scott; F31 MH093991, PI: Whalen; K01 MH097091, PI: Hallquist), the National Institute on Drug Abuse (R01 DA012237, PI: Chung), and by funding from the Office of Juvenile Justice and Delinquency Prevention, the FISA Foundation and the Falk Fund. Correspondence concerning this article should be addressed to Stephanie D. Stepp, Western Psychiatric Institute and Clinic, 3811 O’Hara Street, Pittsburgh, PA 15213. E-mail: [email protected] This document is copyrighted by the American Psychological Association or one of its allied publishers. This article is intended solely for the personal use of the individual user and is not to be disseminated broadly. Personality Disorders: Theory, Research, and Treatment © 2015 American Psychological Association 2015, Vol. 6, No. 1, 53– 63 1949-2715/15/$12.00 http://dx.doi.org/10.1037/per0000107 53

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Daily Shame and Hostile Irritability in Adolescent Girls With BorderlinePersonality Disorder Symptoms
Lori N. Scott, Stephanie D. Stepp, Michael N. Hallquist, Diana J. Whalen,Aidan G. C. Wright, and Paul A. Pilkonis
University of Pittsburgh
Recent theoretical and empirical work suggests that adults with borderline personality disorder (BPD)have difficulty regulating both shame and anger, and that these emotions may be functionally related inclinically relevant ways (e.g., Schoenleber & Berenbaum, 2012b). The covariation of shame withanger-related emotions has important clinical implications for interventions targeting shame and uncon-trolled anger in BPD. However, no studies have examined shame, anger, and their covariation inadolescents who may be at risk for developing BPD. Therefore, this study focuses on associationsbetween BPD symptoms and patterns of covariation between daily experiences of shame and anger-related affects (i.e., hostile irritability) in a community sample of adolescent girls using ecologicalmomentary assessment. Multilevel models revealed that girls with greater BPD symptoms who reportedgreater mean levels of shame across the week also tended to report more hostile irritability, even aftercontrolling for guilt. Additionally, examination of within-person variability showed that girls with greaterBPD symptoms reported more hostile irritability on occasions when they also reported greater concurrentshame, but this was only the case in girls of average socioeconomic status (i.e., those not receiving publicassistance). Unlike shame, guilt was not associated with hostile irritability in girls with greater BPDsymptoms. Results suggest that shame may be a key clinical target in the treatment of anger-relateddifficulties among adolescent girls with BPD symptoms.
Keywords: borderline personality disorder, ecological momentary assessment, hostility, irritability,shame
Symptoms of borderline personality disorder (BPD) are usuallyrecognizable by adolescence and are associated with a host of poorlong-term outcomes (Chanen & McCutcheon, 2013; Winograd,Cohen, & Chen, 2008). Although prevalence rates are similaracross men and women in the general population, studies indicatehigher rates of BPD among adolescent girls and young women inclinical and forensic settings, and greater distress and impairmentin women with BPD as compared with their male counterparts(APA, 2013; Grant et al., 2008; Rosler, Retz, Yaqoobi, Burg, &
Retz-Junginger, 2009). In addition, research has shown that BPDsymptoms peak during mid-adolescence, between ages 14 and 17(Bornovalova, Hicks, Iacono, & McGue, 2009). Research on theearly manifestations and characteristics of BPD symptoms duringmid-adolescence, especially in girls, is therefore critical in theeffort to develop targeted prevention and treatment strategies(Chanen & McCutcheon, 2013).
Although BPD is associated with a range of negative affects,recent theoretical and empirical work suggests that adults withBPD have particular difficulties regulating shame and anger-related emotions (Berenson et al., 2011; Gratz et al., 2010; Line-han, 1993). Moreover, several authors have suggested that anger-related affects may be elicited in the context of intense shameamong individuals with BPD, perhaps as a defensive attempt todeflect attention away from the shamed self and direct blame toothers (Bateman & Fonagy, 2004; Schoenleber & Berenbaum,2012b; Velotti, Elison, & Garofalo, 2014). According to thesetheorists, shame could be a prime driver of anger-related emotionsand thus may be an important clinical target in the treatment ofanger and aggression in those with BPD.
However, little empirical work has examined emotional dys-function, let alone patterns of dysregulation and covariation ofspecific emotional states, among adolescents with emerging BPDsymptoms. This is a significant gap considering that proneness tointense shame and anger is associated with poor outcomes andhigher likelihood of future self-harm and suicide attempts in adultswith BPD (Brodsky, Groves, Oquendo, Mann, & Stanley, 2006;Brown, Linehan, Comtois, Murray, & Chapman, 2009; Rusch et
Lori N. Scott, Stephanie D. Stepp, and Michael N. Hallquist, Departmentof Psychiatry, University of Pittsburgh School of Medicine; Diana J.Whalen and Aidan G. C. Wright, Department of Psychology, University ofPittsburgh; Paul A. Pilkonis, Department of Psychiatry, University ofPittsburgh School of Medicine.
Diana J. Whalen is now at the Department of Psychiatry, WashingtonUniversity.
This research and the efforts of the authors were supported by grantsfrom the National Institute of Mental Health (K01 MH086713, PI: Stepp;R01 MH56630, PI: Loeber; R01 MH056888, PI: Pilkonis; K01MH101289, PI: Scott; F32 MH097311, PI: Scott; F31 MH093991, PI:Whalen; K01 MH097091, PI: Hallquist), the National Institute on DrugAbuse (R01 DA012237, PI: Chung), and by funding from the Office ofJuvenile Justice and Delinquency Prevention, the FISA Foundation and theFalk Fund.
Correspondence concerning this article should be addressed to StephanieD. Stepp, Western Psychiatric Institute and Clinic, 3811 O’Hara Street,Pittsburgh, PA 15213. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Personality Disorders: Theory, Research, and Treatment © 2015 American Psychological Association2015, Vol. 6, No. 1, 53–63 1949-2715/15/$12.00 http://dx.doi.org/10.1037/per0000107
53

al., 2008; Welch & Linehan, 2002). In addition, both shame andanger are relevant to the fundamental difficulties with identity andrelatedness that are believed by many to lie at the core of person-ality disorders (Bender, Morey, & Skodol, 2011; Skodol et al.,2011).
Shame-Proneness and Shame-Aversion in BPD
Shame is characterized by a feeling that one is inherently a bador defective person (Lewis, 2000). Thus, shame involves a generaland global negative evaluation of the whole self, which is closelyaligned with the negative self-representations and self-conceptsreported in those with BPD (Butler, Brown, Beck, & Grisham,2002; Jovev & Jackson, 2004). A large body of research suggeststhat shame can be distinguished from guilt, a related yet distinctemotion characterized by feeling bad about specific actions orbehaviors that are inconsistent with one’s moral values (Lewis,2000). Both shame and guilt involve negative self-evaluations, andare therefore often referred to as self-conscious emotions, butseveral studies have demonstrated that shame is more stronglyassociated with maladaptive behaviors and psychopathology thanguilt (Bennett, Sullivan, & Lewis, 2010; Fergus, Valentiner,McGrath, & Jencius, 2010; Tangney, Wagner, & Gramzow, 1992).In fact, many studies have shown that guilt is unrelated or eveninversely related to problem behaviors after controlling for shame(Fergus et al., 2010; Tangney, Wagner, Fletcher, & Gramzow,1992; Tangney, Wagner, & Gramzow, 1992).
A number of theorists and researchers have discussed shame asa central emotion in BPD (Linehan, 1993; Rizvi, Brown, Bohus, &Linehan, 2011; Rusch et al., 2007; Schoenleber & Berenbaum,2012a). Rusch and colleagues (2007) found that adult BPD pa-tients scored higher than healthy controls or patients with socialphobia on both explicit and implicit measures of shame. Anotherstudy found that adult BPD patients reacted to negative evaluationin the laboratory with greater increases in shame, but not otheremotions, relative to a clinical group without personality disorder(Gratz et al., 2010). In the first published study to our knowledgethat has examined shame in relation to BPD symptoms in childrenor adolescents, Hawes, Helyer, Herlianto, and Willing (2013)found that the identity disturbance component of BPD features wasassociated with an implicit measure of shame-prone self-concept,but only among girls (ages 10–14). One study also found thatalthough BPD symptoms in undergraduate students were posi-tively associated with shame-proneness, they were negatively as-sociated with guilt-proneness (Schoenleber & Berenbaum, 2012a),supporting distinctions between shame and guilt in their associa-tion with BPD. The same study also found that students withgreater BPD symptoms reported high levels of shame aversion,that is, experiencing shame as particularly painful and intolerable.
Anger-Related Emotions in BPD
Anger-related emotions, including irritability and hostility, arecentral components of emotion dysregulation in BPD and mayserve as precursors to the development of the disorder (Carlotta,Borroni, Maffei, & Fossati, 2013; Crowell, Beauchaine, & Line-han, 2009; Stepp, Burke, Hipwell, & Loeber, 2012). For instance,research suggests that uncontrolled anger and affective instabilityare the most predictive criteria for distinguishing between adoles-
cents with and without a BPD diagnosis (Becker, Grilo, Edell, &McGlashan, 2002). In addition, higher levels of anger, aggression,and impulsivity differentiated adolescent inpatients with BPDfrom those with major depressive disorder, and were associatedwith more suicidality in those with BPD (Horesh, Orbach, Gothelf,Efrati, & Apter, 2003). In a longitudinal study, adolescents whofailed to show a normative reduction in hostility and exhibitedincreases in impulsive behaviors across ages 13 to 17 were at anincreased risk for Cluster B personality disorders (Kobak, Zajac, &Smith, 2009). These findings underscore the importance of exam-ining anger-related emotions in adolescents who may be at risk forthe development of BPD, as these difficulties are among theearliest of BPD-related traits to emerge and are prognostic of poorlong-term outcomes.
Associations Between Shame andAnger-Related Emotions
Not only are shame and anger prominent emotional experiencesin BPD, but some authors have suggested that shame and angermay be functionally related in clinically important ways (Schoen-leber & Berenbaum, 2012b; Velotti et al., 2014). Beyond the BPDliterature, social psychologists have written extensively on thepotential for shame to evoke simultaneous anger and aggression(e.g., Gilligan, 1997; Lutwak, Panish, Ferrari, & Razzino, 2001;Tangney, Wagner, Fletcher, & Gramzow, 1992). In various sam-ples across developmental stages (i.e., childhood through adult-hood), shame has been shown to generate hostile and aggressivebehaviorial responses (Bennett, Sullivan, & Lewis, 2005; Scheel etal., 2013; Thomaes, Bushman, Stegge, & Olthof, 2008), whereasguilt has been associated with constructive responses to anger suchas cognitive reappraisals and nonhostile corrective actions (Tang-ney, Wagner, Hill-Barlow, Marschall, & Gramzow, 1996).
Although no studies currently exist with adolescents, recentevidence suggests that shame has a particularly strong associationwith anger and aggression in adults with BPD. For instance,shame-proneness has been associated with anger and hostility, aswell as chronic suicidal ideation, suicide attempts, and self-injurious behavior in adult BPD patients (Brodsky et al., 2006;Brown et al., 2009; Rizvi et al., 2011; Rizvi & Linehan, 2005;Rusch et al., 2007, 2008; Welch & Linehan, 2002). Moreover, arecent study found that adults with BPD reacted to shame induc-tion in the laboratory with greater increases in anger and moresustained anger than depressed patients or healthy controls (Scheelet al., 2013), implying that BPD may be associated with thesimultaneous co-occurrence of anger with shame. It has beensuggested that externalized anger is one of several maladaptivestrategies for avoiding or deflecting intense shame, and thatindividuals with BPD symptoms may be more likely to instan-taneously convert shame to anger-related affects because oftheir tendency toward shame-aversion, that is, experiencingshame as intolerable (Schoenleber & Berenbaum, 2012a). Thus,anger may co-occur with shame among individuals with BPD,perhaps as a defensive attempt to deflect attention away fromthe shamed self and direct blame to others (Schoenleber &Berenbaum, 2012b).
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
54 SCOTT ET AL.

Goals and Hypotheses of the Current Study
In summary, experiences of shame and anger, and the momen-tary covariation of shame and anger-related emotions, are clini-cally significant but understudied aspects of BPD, and are there-fore the focus of the current study. Using ecological momentaryassessment (EMA) of affective experiences across a 1-week pe-riod, we examined individual differences in BPD symptoms as apotential moderator of associations between experiences of shameand anger-related emotions (operationalized as a composite ofirritability and hostility, referred to hereafter as hostile irritability)in daily life after controlling for experiences of guilt. The use ofEMA is a significant improvement over previous studies of shameand angry affects in BPD by providing intensive repeated mea-sures that allow for the disentangling of between-person differ-ences in dispositional affect (i.e., mean levels over the course ofthe week) and within-person fluctuations or variability in affectivestates. In addition, the diverse community sample provides signif-icant variability in race and socioeconomic status (SES), which areoften not explored in clinical studies but may have importantimplications for culturally sensitive theory and practice. We ex-amined the covariation between concurrent reports of affects ratherthan time-lagged relationships because clinical theory and pastresearch suggest that shame can instantaneously or very quicklylead to angry affects, suggesting a momentary co-occurrence ofthese affective experiences rather than time-lagged relationships(Bennett et al., 2005; Scheel et al., 2013; Thomaes et al., 2008).
In accordance with the theoretical and empirical literature re-viewed above, our hypotheses were as follows: (a) Between-person differences in mean levels of shame over the course of theweek (i.e., dispositional shame or shame-proneness), and not guilt,will be positively associated with hostile irritability, but onlyamong those with greater BPD symptoms; and (b) Within-personmomentary reports of shame, and not guilt, will be positivelyassociated with contemporaneous reports of hostile irritability, butonly among those with greater BPD symptoms. In addition, con-sidering the diverse study sample and previous studies demonstrat-ing associations between sociodemographic factors such as lowSES and anger, aggression, and psychopathology (Conger et al.,1994; Evans, 2004; Evans & English, 2002), we also took theopportunity to explore race and SES as potential moderators ofthese hypothesized relationships.
Method
Participants and Recruitment Procedures
One hundred fourteen 16-year-old girls with a wide range ofBPD symptoms were recruited from the ongoing Pittsburgh GirlsStudy (PGS) for a substudy on girls’ personality development. Theongoing PGS involves an urban community sample of four agecohorts of girls who were ages 5 to 8 at the first assessment in2000/2001 and have been followed with annual assessments sincethat time. The PGS sample was identified by oversampling fromlow-income neighborhoods, such that neighborhoods in which atleast 25% of families were living at or below poverty level werefully enumerated and a random selection of 50% of households inall other neighborhoods were enumerated. Of the 2,875 eligiblefamilies who were contacted to determine interest in study partic-
ipation, 2,450 families (85%) agreed to participate in the PGS andprovided informed consent (see Keenan et al., 2010 for furtherdetails on PGS study design).
One hundred fourteen girls were selected from the larger PGSfor participation in the current substudy in 2010–2012 (girls incohort 7 in 2010, cohort 6 in 2011, and cohort 5 in 2012). Toobtain a sample with a high degree of variability in core symptomsof BPD, girls were recruited based on their self reports on theAffective Instability subscale of the Personality Assessment In-ventory (PAI-AI; Morey, 1991), which assesses a core symptom ofBPD and was administered as part of the main PGS annualassessment battery. Approximately one third of girls who wererecruited for the current substudy screened high on affective in-stability (scores �11 on the PAI-AI), and the remainder of thesample was randomly selected from girls endorsing low to mediumlevels of affective instability (scores �11). This sampling strategywas intended to produce a sample with a wide range of BPDsymptoms (affective instability as well as associated symptomsconsistent with BPD such as impulsivity, chaotic interpersonalrelationships, intense and inappropriate anger, self-harm, and iden-tity disturbance).
Of the 114 girls who were recruited for this substudy, 89completed diagnostic interviews for personality disorders and a7-day EMA protocol. Thus, 89 girls are included in the currentanalyses. The 89 girls who participated did not significantly differfrom the 25 who did not participate in terms of race, SES, PAI-AIscores, or number of BPD symptoms. Reflecting the demographiccharacteristics of the PGS, this sample was racially and socioeco-nomically diverse (67% African American, 33% Caucasian; 53%of families reported receiving some form of public assistance inthe last year, e.g., WIC, food stamps, welfare, temporary assistancefor needy families).
Assessment Procedures and Measures
Participants completed semistructured interviews for Axis I andII disorders in the laboratory, followed by a 1-week cellularphone–based EMA protocol in their home environments. All studyprocedures were approved by the University Institutional ReviewBoard. Participants were compensated for their participation.
Assessment of BPD symptoms. BPD symptoms were as-sessed dimensionally using the Structured Clinical Interview forDiagnostic and Statistical Manual of Mental Disorders, fourthedition (DSM–IV) Personality Disorders (SIDP-IV; Pfohl, Blum,& Zimmerman, 1997), a semistructured interview with establishedreliability and validity for assessing the presence and severity ofpersonality disorders in adolescents. Interviewers were postbacca-laureat, masters, or doctoral-level clinicians who were trained toreliability by the corresponding author (SDS). The nine itemscorresponding to individual DSM-5 diagnostic criteria for BPDwere rated on a 0–3 scale (0 � not present, 1 � subthreshold, 2 �present, 3 � strongly present). Per DSM-5 (APA, 2013) guidelinesfor the diagnosis of personality disorder in adolescence, symptomswere only rated “present” if they were present for at least the pastyear and judged to be pervasive, persistent, and unlikely to belimited to developmental stage or an episode of another disorder.The nine BPD items were summed to yield a dimensional score forBPD symptoms, which was used as a continuous measure of BPDsymptoms.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
55SHAME, HOSTILITY, IRRITABILITY, AND BPD SYMPTOMS

Twenty-two participants’ SIDP-IV interviews (25% of the an-alyzed sample) were videotaped and rated by at least one addi-tional independent rater for calculation of interrater reliability. Thenumber of raters per case ranged from 2 to 6 (n � 14 cases had 2raters, 4 had 3 raters, 2 had 4 raters, and the remaining 2 had 5 and6 raters). ICC’s were calculated based on one-way random effectmodels for the unequal number of raters per case, and demon-strated excellent interdiagnostician agreement for BPD dimen-sional scores (ICC � .91). The distribution of BPD criteria thatwere met above clinical threshold (i.e., items scored �2) is pre-sented in Table 1. The prevalence of diagnosable BPD in thecurrent study sample (4.5%) is within the range found in othercommunity adolescent samples (e.g., 3–6%; Chabrol et al., 2004;Zanarini et al., 2003). Consistent with previous studies with ado-lescent samples (e.g., Becker et al., 2002; Zanarini et al., 2011),intense anger and affective instability were the most frequentlymet BPD criteria in this sample.
Ecological momentary assessment of affect. After comple-tion of diagnostic interviews, participants were given modified,answer-only cellular telephones to use during the EMA protocol.Based on their reported wake and sleep times and activity sched-ules, participants were scheduled to receive a maximum of fourcalls from research staff per day over the course of seven days(maximum of 28 calls across the week). Because of some partic-ipants’ afterschool activities and work schedules, there was indi-vidual variability in the number of planned calls per day, as furtherdescribed below. At each call, participants were asked questionsabout their current mood, activities, and location. For mood items(Happy, Sad, Nervous, Excited, Scared, Ashamed, Irritable, Hos-tile, Guilty, Alert), girls were asked to rate how they had beenfeeling in the last 15 minutes on a 5-point Likert scale (1 � veryslightly or not at all; 5 � extremely). Similar procedures have beensuccessfully used in previous EMA studies with child and adoles-cent samples (e.g., Primack et al., 2011; Silk et al., 2011). As withthese previous studies, participants could not take calls during
school hours. However, previous studies have been limited toevening and weekend assessments, and we improved on this byincluding a morning call. On school days, call 1 was before school,and calls 2 through 4 were after school up until 10:00 p.m. Onweekends, call 1 was within an hour of the girl’s reported awak-ening time, and calls 2 through 4 were scheduled at equal intervalsacross the day until 10:00 p.m. If a participant missed the first call,second and third attempts to reach the participant were made, eachin 10-min intervals.
Although 93 girls agreed to participate in the EMA protocol,data were excluded from three girls who completed fewer thanseven calls over the course of the week (i.e., less than one call perday on average) and from one girl who did not complete diagnosticinterviews, leaving a sample of 89 girls who were included in thisreport. The current analyses included 1569 phone calls (M � 17.81successful calls per person; SD � 4.06; Range � 7–27). The meannumber of planned phone calls per person was 20.67 (SD � 3.82)and the compliance rate (i.e., percentage of planned calls that weresuccessful) was 86.31% (SD � 12.37%; Median � 90.5%Range � 35% to 100%). Neither the number of calls planned norindividual compliance rates were significantly associated with anystudy variables (rs � .15, ns), nor did these factors emerge assignificant covariates in any of the models tested. As expectedconsidering the inability to assess girls during school or workhours, there was wide variability in the time lags between assess-ments (M � 8.84 hrs, SD � 8.84, Range � 0.17–70.53 hrs). Forthe majority of assessments (78%), girls reported being at home atthe time of assessment. Reported activities included media use(28%); family, peer, or school-related activities (24%); personalcare or eating (18%); chores, shopping, outdoor activities, ortransportation (18%); and either sleeping or doing “nothing”(12%).
The current analysis uses participants’ ratings on four emotionsthat directly pertain to our study hypotheses: Ashamed, Guilty,Irritable, and Hostile. Ratings of irritability and hostility werehighly correlated, r � .65, p � .001 and loaded on the same factorin an exploratory factor analysis (EFA). Bivariate correlations alsosuggested that hostility and irritability were related to other studyvariables in similar ways (e.g., with shame, rs � .45 and .48,which did not significantly differ, z � 0.39, ns; and with guilt, rs �.39 and .33, z � 0.72, ns). Ratings of hostility and irritability weretherefore combined into a single “hostile irritability” score bycalculating the mean of these ratings for each person at eachoccasion. Models were also tested with hostility and irritability asseparate dependent variables, and results were generally the sameacross these constructs, supporting their combination to streamlineanalyses and results. Although ratings of shame and guilt were alsohighly correlated, r � .77, p � .001, they loaded on separatefactors in an EFA and showed differential relationships with otherstudy variables (e.g., shame was significantly associated with BPDsymptoms, r � .29, p � .01, but guilt was not, r � .09, ns, andthese correlations differed significantly from one another, z �2.82, p � .005; and shame was more strongly associated withhostile irritability, r � .52, than was guilt, r � .38, z � 2.20, p �.05). These findings are consistent with previous research suggest-ing distinctions between shame and guilt in their associations withpsychopathology (Bennett et al., 2010; Fergus et al., 2010; Tang-ney, Wagner, & Gramzow, 1992). Shame and guilt were thereforetreated as separate constructs, allowing us to examine their differ-
Table 1Distribution of BPD Symptoms Met Above Threshold in StudySample (n � 89)
Symptom n %
BPD criterion1. Efforts to avoid abandonment 2 2.22. Unstable relationships 8 9.03. Identity disturbance 3 3.44. Impulsivity 11 12.45. Suicide/self-harm behavior 4 4.56. Affective instability 25 28.17. Chronic emptiness 11 12.48. Intense anger 33 37.19. Paranoid/dissociative 9 10.1
BPD symptom counts (# criteria)0 47 52.81 11 12.42 13 14.63 7 7.94 7 7.95 4 4.5
Note. Criteria were counted as present (i.e., above threshold) based onitem scores � 2 on the Structured Clinical Interview for DSM–IV Person-ality Disorders (SIDP-IV; Pfohl, Blum, & Zimmerman, 1997).
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
56 SCOTT ET AL.
ential effects on hostile irritability. Because shame, guilt, andhostile irritability ratings were positively skewed, they were log-transformed before analysis.
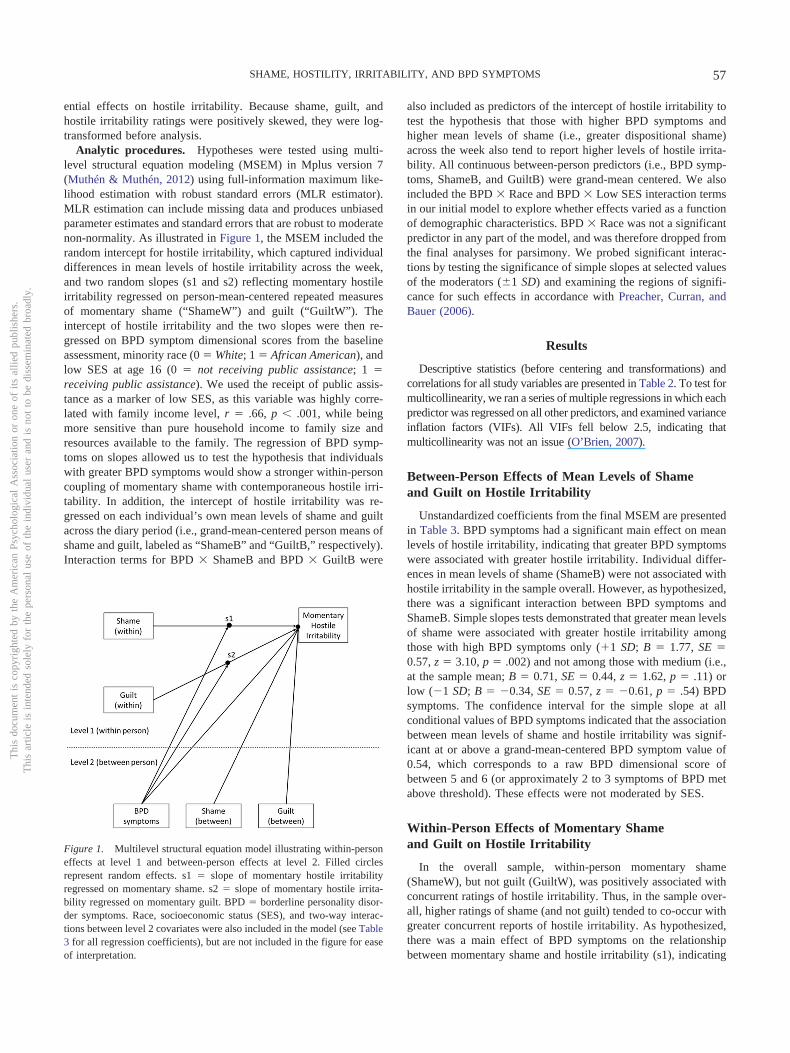
Analytic procedures. Hypotheses were tested using multi-level structural equation modeling (MSEM) in Mplus version 7(Muthén & Muthén, 2012) using full-information maximum like-lihood estimation with robust standard errors (MLR estimator).MLR estimation can include missing data and produces unbiasedparameter estimates and standard errors that are robust to moderatenon-normality. As illustrated in Figure 1, the MSEM included therandom intercept for hostile irritability, which captured individualdifferences in mean levels of hostile irritability across the week,and two random slopes (s1 and s2) reflecting momentary hostileirritability regressed on person-mean-centered repeated measuresof momentary shame (“ShameW”) and guilt (“GuiltW”). Theintercept of hostile irritability and the two slopes were then re-gressed on BPD symptom dimensional scores from the baselineassessment, minority race (0 � White; 1 � African American), andlow SES at age 16 (0 � not receiving public assistance; 1 �receiving public assistance). We used the receipt of public assis-tance as a marker of low SES, as this variable was highly corre-lated with family income level, r � .66, p � .001, while beingmore sensitive than pure household income to family size andresources available to the family. The regression of BPD symp-toms on slopes allowed us to test the hypothesis that individualswith greater BPD symptoms would show a stronger within-personcoupling of momentary shame with contemporaneous hostile irri-tability. In addition, the intercept of hostile irritability was re-gressed on each individual’s own mean levels of shame and guiltacross the diary period (i.e., grand-mean-centered person means ofshame and guilt, labeled as “ShameB” and “GuiltB,” respectively).Interaction terms for BPD � ShameB and BPD � GuiltB were
also included as predictors of the intercept of hostile irritability totest the hypothesis that those with higher BPD symptoms andhigher mean levels of shame (i.e., greater dispositional shame)across the week also tend to report higher levels of hostile irrita-bility. All continuous between-person predictors (i.e., BPD symp-toms, ShameB, and GuiltB) were grand-mean centered. We alsoincluded the BPD � Race and BPD � Low SES interaction termsin our initial model to explore whether effects varied as a functionof demographic characteristics. BPD � Race was not a significantpredictor in any part of the model, and was therefore dropped fromthe final analyses for parsimony. We probed significant interac-tions by testing the significance of simple slopes at selected valuesof the moderators (�1 SD) and examining the regions of signifi-cance for such effects in accordance with Preacher, Curran, andBauer (2006).
Results
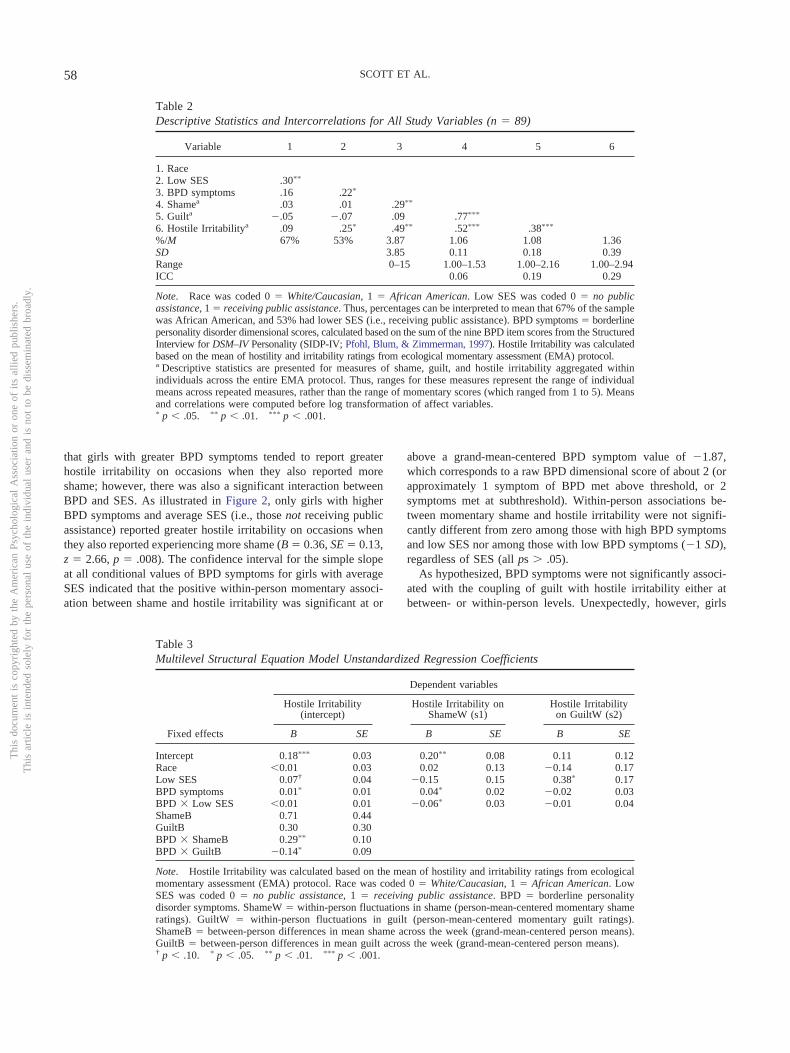
Descriptive statistics (before centering and transformations) andcorrelations for all study variables are presented in Table 2. To test formulticollinearity, we ran a series of multiple regressions in which eachpredictor was regressed on all other predictors, and examined varianceinflation factors (VIFs). All VIFs fell below 2.5, indicating thatmulticollinearity was not an issue (O’Brien, 2007).
Between-Person Effects of Mean Levels of Shameand Guilt on Hostile Irritability
Unstandardized coefficients from the final MSEM are presentedin Table 3. BPD symptoms had a significant main effect on meanlevels of hostile irritability, indicating that greater BPD symptomswere associated with greater hostile irritability. Individual differ-ences in mean levels of shame (ShameB) were not associated withhostile irritability in the sample overall. However, as hypothesized,there was a significant interaction between BPD symptoms andShameB. Simple slopes tests demonstrated that greater mean levelsof shame were associated with greater hostile irritability amongthose with high BPD symptoms only (�1 SD; B � 1.77, SE �0.57, z � 3.10, p � .002) and not among those with medium (i.e.,at the sample mean; B � 0.71, SE � 0.44, z � 1.62, p � .11) orlow (�1 SD; B � �0.34, SE � 0.57, z � �0.61, p � .54) BPDsymptoms. The confidence interval for the simple slope at allconditional values of BPD symptoms indicated that the associationbetween mean levels of shame and hostile irritability was signif-icant at or above a grand-mean-centered BPD symptom value of0.54, which corresponds to a raw BPD dimensional score ofbetween 5 and 6 (or approximately 2 to 3 symptoms of BPD metabove threshold). These effects were not moderated by SES.
Within-Person Effects of Momentary Shameand Guilt on Hostile Irritability
In the overall sample, within-person momentary shame(ShameW), but not guilt (GuiltW), was positively associated withconcurrent ratings of hostile irritability. Thus, in the sample over-all, higher ratings of shame (and not guilt) tended to co-occur withgreater concurrent reports of hostile irritability. As hypothesized,there was a main effect of BPD symptoms on the relationshipbetween momentary shame and hostile irritability (s1), indicating
Figure 1. Multilevel structural equation model illustrating within-personeffects at level 1 and between-person effects at level 2. Filled circlesrepresent random effects. s1 � slope of momentary hostile irritabilityregressed on momentary shame. s2 � slope of momentary hostile irrita-bility regressed on momentary guilt. BPD � borderline personality disor-der symptoms. Race, socioeconomic status (SES), and two-way interac-tions between level 2 covariates were also included in the model (see Table3 for all regression coefficients), but are not included in the figure for easeof interpretation.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
57SHAME, HOSTILITY, IRRITABILITY, AND BPD SYMPTOMS
that girls with greater BPD symptoms tended to report greaterhostile irritability on occasions when they also reported moreshame; however, there was also a significant interaction betweenBPD and SES. As illustrated in Figure 2, only girls with higherBPD symptoms and average SES (i.e., those not receiving publicassistance) reported greater hostile irritability on occasions whenthey also reported experiencing more shame (B � 0.36, SE � 0.13,z � 2.66, p � .008). The confidence interval for the simple slopeat all conditional values of BPD symptoms for girls with averageSES indicated that the positive within-person momentary associ-ation between shame and hostile irritability was significant at or
above a grand-mean-centered BPD symptom value of �1.87,which corresponds to a raw BPD dimensional score of about 2 (orapproximately 1 symptom of BPD met above threshold, or 2symptoms met at subthreshold). Within-person associations be-tween momentary shame and hostile irritability were not signifi-cantly different from zero among those with high BPD symptomsand low SES nor among those with low BPD symptoms (�1 SD),regardless of SES (all ps � .05).
As hypothesized, BPD symptoms were not significantly associ-ated with the coupling of guilt with hostile irritability either atbetween- or within-person levels. Unexpectedly, however, girls
Table 2Descriptive Statistics and Intercorrelations for All Study Variables (n � 89)
Variable 1 2 3 4 5 6
1. Race2. Low SES .30��
3. BPD symptoms .16 .22�
4. Shamea .03 .01 .29��
5. Guilta �.05 �.07 .09 .77���
6. Hostile Irritabilitya .09 .25� .49�� .52��� .38���
%/M 67% 53% 3.87 1.06 1.08 1.36SD 3.85 0.11 0.18 0.39Range 0–15 1.00–1.53 1.00–2.16 1.00–2.94ICC 0.06 0.19 0.29
Note. Race was coded 0 � White/Caucasian, 1 � African American. Low SES was coded 0 � no publicassistance, 1 � receiving public assistance. Thus, percentages can be interpreted to mean that 67% of the samplewas African American, and 53% had lower SES (i.e., receiving public assistance). BPD symptoms � borderlinepersonality disorder dimensional scores, calculated based on the sum of the nine BPD item scores from the StructuredInterview for DSM–IV Personality (SIDP-IV; Pfohl, Blum, & Zimmerman, 1997). Hostile Irritability was calculatedbased on the mean of hostility and irritability ratings from ecological momentary assessment (EMA) protocol.a Descriptive statistics are presented for measures of shame, guilt, and hostile irritability aggregated withinindividuals across the entire EMA protocol. Thus, ranges for these measures represent the range of individualmeans across repeated measures, rather than the range of momentary scores (which ranged from 1 to 5). Meansand correlations were computed before log transformation of affect variables.� p � .05. �� p � .01. ��� p � .001.
Table 3Multilevel Structural Equation Model Unstandardized Regression Coefficients
Fixed effects
Dependent variables
Hostile Irritability(intercept)
Hostile Irritability onShameW (s1)
Hostile Irritabilityon GuiltW (s2)
B SE B SE B SE
Intercept 0.18��� 0.03 0.20�� 0.08 0.11 0.12Race �0.01 0.03 0.02 0.13 �0.14 0.17Low SES 0.07† 0.04 �0.15 0.15 0.38� 0.17BPD symptoms 0.01� 0.01 0.04� 0.02 �0.02 0.03BPD � Low SES �0.01 0.01 �0.06� 0.03 �0.01 0.04ShameB 0.71 0.44GuiltB 0.30 0.30BPD � ShameB 0.29�� 0.10BPD � GuiltB �0.14� 0.09
Note. Hostile Irritability was calculated based on the mean of hostility and irritability ratings from ecologicalmomentary assessment (EMA) protocol. Race was coded 0 � White/Caucasian, 1 � African American. LowSES was coded 0 � no public assistance, 1 � receiving public assistance. BPD � borderline personalitydisorder symptoms. ShameW � within-person fluctuations in shame (person-mean-centered momentary shameratings). GuiltW � within-person fluctuations in guilt (person-mean-centered momentary guilt ratings).ShameB � between-person differences in mean shame across the week (grand-mean-centered person means).GuiltB � between-person differences in mean guilt across the week (grand-mean-centered person means).† p � .10. � p � .05. �� p � .01. ��� p � .001.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
58 SCOTT ET AL.

with low SES showed a stronger within-person association ofmomentary guilt (and not shame) with concurrent hostile irritabil-ity, regardless of BPD symptoms. Simple slopes tests revealed thatmomentary guilt was only significantly associated with hostileirritability for girls with low SES (B � 0.49, SE � 0.21, z � 2.27,p � .02), and not among girls with average SES (B � 0.11, SE �0.12, z � 0.92, p � .36).
In a supplemental analysis, we examined whether results dif-fered if BPD dimensional scores were calculated without includingthe “intense anger” criterion. This step allowed us to explorewhether the coupling of shame with hostile irritability is onlystronger among those with anger-related BPD symptoms, orwhether these results generalize to other BPD symptoms such asaffective instability or impulsivity. All results and substantiveinterpretations remained the same in this supplemental analysis,suggesting that shame is positively associated with hostile irrita-bility among those with greater non–anger-related BPD symptomssuch as affective instability and impulsivity. However, the associ-ation between low SES and overall hostile irritability becamesignificant (B � 0.07, SE � 0.04, z � 1.97, p � .05), whereas itwas not significant in the above results (p � .06). Further detailsfrom this analysis are available upon request from the first author.
Discussion
We examined whether BPD symptoms in a diverse communitysample of adolescent girls predicted associations between experi-ences of shame and anger-related emotions (i.e., hostile irritability)in daily life. Results generally supported hypothesized associationsbetween shame and anger-related affects in those with greater BPDsymptoms and demonstrated important distinctions between shameand guilt in this regard. Specifically, consistent with our hypoth-eses, mean levels of shame, and not guilt, over the course of the
week were associated with greater hostile irritability, but only ingirls with high levels BPD symptoms. In addition, as hypothesized,girls with greater BPD symptoms tended to report more hostileirritability on occasions when they also reported experiencingmore shame, but not on occasions when they reported more guilt.However, the within-person coupling of momentary shame withhostile irritability was only found among those girls with greaterBPD symptoms and average SES (i.e., those not receiving publicassistance). This within-person link between shame and hostileirritability emerged among girls of average SES with as few as onesymptom of BPD met above threshold, or two symptoms at sub-threshold.
Our finding that shame, and not guilt, was associated withhostile irritability in girls with higher BPD symptoms is consistentwith studies that have demonstrated negligible or even negativeassociations between guilt and psychopathology or anger-relatedemotions after controlling for shame (Tangney, Wagner, Fletcher,& Gramzow, 1992; Tangney, Wagner, & Gramzow, 1992). How-ever, this is the first study to our knowledge to examine themomentary within-person associations between shame, guilt, andangry affects using intensive repeated measures. Our results extendprevious findings by demonstrating that the within-person momen-tary covariation of shame and guilt with anger-related emotions inadolescent girls depends on their level of BPD symptoms and SES,such that momentary shame (but not guilt) is associated withsimultaneous anger-related emotions only in girls with greaterBPD symptoms and average SES.
Consistent with recent literature reviews suggesting that shameconfers greater vulnerability to angry reactivity and aggression(e.g., Schoenleber & Berenbaum, 2012b; Velotti et al., 2014), ourresults imply that shame and anger-related emotions may be func-tionally related in adolescent girls with BPD symptoms, even in
Figure 2. Within-person associations between momentary shame and concurrent momentary hostile irritability(log-transformed) as a function of borderline personality disorder (BPD) symptoms and socioeconomic status(SES). Lines represent model-estimated simple slopes at �1 SD and �1 SD from the mean of BPD symptomsand at low (i.e., receiving public assistance) and average (i.e., not receiving public assistance) SES levels. Theassociation between momentary shame (within-person deviations from individual means) and hostile irritabilityis only significant (i.e., different from zero, p � .05) among girls with high BPD symptoms and average SES(solid black line).
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
59SHAME, HOSTILITY, IRRITABILITY, AND BPD SYMPTOMS

those with BPD symptoms at subthreshold levels. Perhaps due tofeatures such as rejection sensitivity and a fragile sense of self,individuals with BPD can be particularly prone to intense shamewhile also experiencing shame as highly intolerable and threaten-ing to their sense of self and relatedness to others (Velotti et al.,2014). Thus, they might be more likely to externalize blame andreact angrily in efforts to regulate shame and regain a sense ofcontrol. Although it is possible that shame may emerge as aconsequence of being more hostile and irritable (e.g., feeling badabout being grumpy), previous research suggests that anger-relatedemotions co-occur simultaneously with shame, as opposed tooccurring as a consequence of shame (Bennett et al., 2005; Scheelet al., 2013; Thomaes et al., 2008; Velotti et al., 2014). Nonethe-less, the temporal relationships between shame and anger shouldbe explored in future studies with more frequent daily measure-ments of affect with shorter and less variable time lags betweenassessments.
Although the effects of SES observed in this study were nothypothesized, they warrant discussion and interpretation. It is note-worthy that the predicted relationship between momentary shame andhostile irritability only emerged among girls with high BPD symp-toms and average SES. As shown in Figure 2, girls with high BPDsymptoms and low SES reported high levels of hostile irritabilityregardless of their concurrent levels of shame. There may be a ceilingeffect for the high-BPD and low SES girls, whose hostile irritabilityis so high that there is little room to increase as a function of shame.These results may imply that the additive combination of BPD symp-toms with poverty represents a high degree of cumulative risk (e.g.,see Evans, Li, & Whipple, 2013) that predisposes adolescent girls tohigher levels of hostile irritability, independent of shame. Previousresearch has documented associations between economic adversityand exposure to hostility, aggression, and violence both at home andin the community, which in turn influences the development ofadjustment problems in children, including hostile and aggressivebehavior (e.g., Conger et al., 1994; Evans & English, 2002). BPDsymptoms may further compound this risk by virtue of higher traitanger and aggression, thereby predisposing these girls to higher levelsof hostile irritability for reasons that are independent of concurrentlevels of shame. There may also be aspects of living in an average tohigh SES environment, such as invalidation of the child’s emotions orbehaviors that do not meet familial expectations (Linehan, 1993), thatcould promote experiences of shame in those with BPD symptoms.This is an interesting possibility to explore in future studies.
As hypothesized, BPD symptoms did not predict a stronger cou-pling of guilt with hostile irritability, but we unexpectedly found thatlow SES was associated with a stronger within-person coupling ofmomentary guilt with hostile irritability, regardless of BPD level. Thiscontrasts with findings from previous studies indicating that guilt isnot associated with anger or aggression after controlling for shame(for review, see Velotti et al., 2014). However, one study has foundthat shame-free guilt is linked to higher internalizing and externalizingsymptoms in early adolescent girls but not boys (Ferguson, Stegge,Miller, & Olsen, 1999). The authors suggest that this may be attrib-utable to a gender paradox, that is, as compared with boys, girls tendto receive harsher consequences from their environment and to ex-press more remorse and regret for their delinquent behavior. Perhapsgirls living in poverty may try to cover or regulate this guilt withanger-related emotions; conversely, they might feel guilty for actingin an irritable or hostile manner. Alternatively, girls with limited
family resources may differ in their level of understanding, interpre-tation, and daily usage of words like “shame” and “guilt” as a resultof differences in emotion socialization and/or education, obscuringdistinctions between these constructs in their self reports. Althoughwe can only speculate about these potential explanations, they suggestthat SES deserves further investigation in studies of BPD in the effortto develop more culturally sensitive prevention strategies.
The current study fills important gaps in previous research byexamining not only mean levels of affective experiences but alsomomentary patterns of covariation between self-conscious and anger-related affects in relation to BPD symptoms. The assessment of dailyaffective experiences using EMA methodology is ideal for examiningthese within-person processes with greater ecological validity thanlaboratory-based assessment on a single occasion. On a related note,the intensive repeated measures of affect allowed us to use a statisticalapproach that improves upon past studies by disaggregating between-and within-persons effects so that relations between both trait andstate levels of shame and angry emotions could be examined. Further,the diverse adolescent community sample is advantageous and novelbecause BPD-related pathology has generally been understudied inadolescents with sociodemographic risk factors such as low SES.Although this introduces heterogeneity and statistical power may belimited to detect moderation effects, the diverse sample allowed us toexplore whether the hypothesized relations between shame and anger-related emotions in adolescents with BPD symptoms differed acrossracial and socioeconomic strata.
On the other hand, this study has several limitations that should benoted. The inability to assess girls during school and work hoursrestricts ecological validity, and these are social contexts in whichadolescent girls may have been most prone to experiencing intenseshame and anger-related emotions. There were also insufficient as-sessments in close enough succession to one another to examine thetemporal sequence of affective experiences. To establish whethershame precedes angry affects, or vice versa, it would be necessary tosample affective experiences at a much higher frequency and resolu-tion (i.e., several assessments within minutes of each other). Further-more, we relied on single items to assess complex affective constructs,and it is unclear how girls understood or interpreted these emotionwords when making their ratings. This is common in EMA studies(Scollon, Kim-Prieto, & Diener, 2003; Stone & Shiffman, 1994), inwhich it is necessary to reduce the number of items to alleviateparticipant burden and increase compliance with intensive repeatedmeasures. However, this limitation may be mitigated by recent evi-dence for the validity and reliability of single-item measures (Doll-inger & Malmquist, 2009; Hoeppner, Kelly, Urbanoski, & Slaymaker,2011), and the consistency of our results distinguishing betweenshame and guilt with previous studies using multiple-item measuresof these constructs suggests that our measures have validity. Finally,given the adolescent community sample of only girls, these resultsmay not generalize to males, adults, or to treatment-seeking individ-uals with a diagnosis of BPD.
Despite these limitations, there are several implications of theseresults for clinical assessment and interventions. First, our resultssuggest that shame could be a key clinical target for interventionsaimed at preventing or reducing angry or aggressive behavior inadolescent girls with BPD symptoms. Clinicians should be aware ofthe possibility that hostility, irritability, or other anger-related emo-tions might mask underlying experiences of intense shame, or atleast co-occur with them. Angry emotions may be more notice-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
60 SCOTT ET AL.

able on the surface, whereas shame could be hidden and may gounnoticed, especially in the context of hostile behavior. Carefulassessment of shame experiences, particularly in those whodemonstrate angry or hostile affects, may be warranted toadequately validate and directly target intense shame. Accuratevalidation of such underlying shame experiences may help tomitigate angry affects and allow for the introduction of moreadaptive ways of coping with shame. Clinical interventions thatare designed to target shame, such as compassion focusedtherapy (Gilbert, 2011), elements of dialectical behavior ther-apy (e.g., opposite action, mindfulness, and acceptance; Rizvi etal., 2011), and some relational or object relations approaches(Stadter, 2011), may be particularly helpful in reducing theintensity of shame and maladaptive reactions to experiences ofshame, including anger and aggression directed at self or others(Velotti et al., 2014). Finally, our results suggest that theseaffective processes may operate differently in girls from low-SES backgrounds, highlighting the importance of consideringthe influence of family level adversity in research and clinicalassessment.
References
American Psychiatric Association [APA]. (2013). Diagnostic and statisti-cal manual of mental disorders (5th ed.). Arlington, VA: Author.
Bateman, A., & Fonagy, A. (2004). Psychotherapy for borderline person-ality disorder: Mentalization-based treatment. Oxford, UK: Oxford Uni-versity Press.
Becker, D. F., Grilo, C. M., Edell, W. S., & McGlashan, T. H. (2002).Diagnostic efficiency of borderline personality disorder criteria in hos-pitalized adolescents: Comparison with hospitalized adults. The Ameri-can Journal of Psychiatry, 159, 2042–2047. http://dx.doi.org/10.1176/appi.ajp.159.12.2042
Bender, D. S., Morey, L. C., & Skodol, A. E. (2011). Toward a model forassessing level of personality functioning in DSM-5, part I: A review oftheory and methods. Journal of Personality Assessment, 93, 332–346.http://dx.doi.org/10.1080/00223891.2011.583808
Bennett, D. S., Sullivan, M. W., & Lewis, M. (2005). Young children’sadjustment as a function of maltreatment, shame, and anger. Child Mal-treatment, 10, 311–323. http://dx.doi.org/10.1177/1077559505278619
Bennett, D. S., Sullivan, M. W., & Lewis, M. (2010). Neglected children,shame-proneness, and depressive symptoms. Child Maltreatment, 15,305–314. http://dx.doi.org/10.1177/1077559510379634
Berenson, K. R., Downey, G., Rafaeli, E., Coifman, K. G., & Paquin, N. L.(2011). The rejection-rage contingency in borderline personality disor-der. Journal of Abnormal Psychology, 120, 681–690. http://dx.doi.org/10.1037/a0023335
Bornovalova, M. A., Hicks, B. M., Iacono, W. G., & McGue, M. (2009).Stability, change, and heritability of borderline personality disorder traitsfrom adolescence to adulthood: A longitudinal twin study. Developmentand Psychopathology, 21, 1335–1353.
Brodsky, B. S., Groves, S. A., Oquendo, M. A., Mann, J. J., & Stanley, B.(2006). Interpersonal precipitants and suicide attempts in borderlinepersonality disorder. Suicide and Life-Threatening Behavior, 36, 313–322. http://dx.doi.org/10.1521/suli.2006.36.3.313
Brown, M. Z., Linehan, M. M., Comtois, K. A., Murray, A., & Chapman,A. L. (2009). Shame as a prospective predictor of self-inflicted injury inborderline personality disorder: A multi-modal analysis. Behaviour Re-search and Therapy, 47, 815–822. http://dx.doi.org/10.1016/j.brat.2009.06.008
Butler, A. C., Brown, G. K., Beck, A. T., & Grisham, J. (2002). Assess-ment of dysfunctional beliefs in borderline personality disorder. Behav-
iour Research and Therapy, 40, 1231–1240. http://dx.doi.org/10.1016/S0005-7967(02)00031-1
Carlotta, D., Borroni, S., Maffei, C., & Fossati, A. (2013). On the rela-tionship between retrospective childhood ADHD symptoms and adultbpd features: The mediating role of action-oriented personality traits.Comprehensive Psychiatry, 54, 943–952. http://dx.doi.org/10.1016/j.comppsych.2013.03.025
Chabrol, H., Montovany, A., Ducongé, E., Kallmeyer, A., Mullet, E., &Leichsenring, F. (2004). Factor structure of the borderline personalityinventory in adolescents. European Journal of Psychological Assess-ment, 20, 59–65. http://dx.doi.org/10.1027/1015-5759.20.1.59
Chanen, A. M., & McCutcheon, L. (2013). Prevention and early interven-tion for borderline personality disorder: Current status and recent evi-dence. The British Journal of Psychiatry, 202, s24–s29. http://dx.doi.org/10.1192/bjp.bp.112.119180
Conger, R. D., Ge, X., Elder, G. H., Jr., Lorenz, F. O., & Simons, R. L.(1994). Economic stress, coercive family process, and developmentalproblems of adolescents. Child Development, 65, 541–561. http://dx.doi.org/10.2307/1131401
Crowell, S. E., Beauchaine, T. P., & Linehan, M. M. (2009). A biosocialdevelopmental model of borderline personality: Elaborating and extend-ing Linehan’s theory. Psychological Bulletin, 135, 495–510. http://dx.doi.org/10.1037/a0015616
Dollinger, S. J., & Malmquist, D. (2009). Reliability and validity ofsingle-item self-reports: With special relevance to college students’alcohol use, religiosity, study, and social life. Journal of General Psy-chology, 136, 231–242. http://dx.doi.org/10.3200/GENP.136.3.231-242
Evans, G. W. (2004). The environment of childhood poverty. AmericanPsychologist, 59, 77–92. http://dx.doi.org/10.1037/0003-066X.59.2.77
Evans, G. W., & English, K. (2002). The environment of poverty: Multiplestressor exposure, psychophysiological stress, and socioemotional ad-justment. Child Development, 73, 1238–1248. http://dx.doi.org/10.1111/1467-8624.00469
Evans, G. W., Li, D., & Whipple, S. S. (2013). Cumulative risk and childdevelopment. Psychological Bulletin, 139, 1342–1396. http://dx.doi.org/10.1037/a0031808
Fergus, T. A., Valentiner, D. P., McGrath, P. B., & Jencius, S. (2010).Shame- and guilt-proneness: Relationships with anxiety disorder symp-toms in a clinical sample. Journal of Anxiety Disorders, 24, 811–815.http://dx.doi.org/10.1016/j.janxdis.2010.06.002
Ferguson, T. J., Stegge, H., Miller, E. R., & Olsen, M. E. (1999). Guilt,shame, and symptoms in children. Developmental Psychology, 35, 347–357. http://dx.doi.org/10.1037/0012-1649.35.2.347
Gilbert, P. (2011). Shame in psychotherapy and the role of compassionfocused therapy. In R. L. Dearing & J. P. Tangney (Eds.), Shame in thetherapy hour (pp. 325–354). Washington, DC: American PsychologicalAssociation. http://dx.doi.org/10.1037/12326-014
Gilligan, J. (1997). Violence: Reflections on a national epidemic. NewYork, NY: Vintage Books.
Grant, B. F., Chou, S. P., Goldstein, R. B., Huang, B., Stinson, F. S., Saha,T. D., . . . Ruan, W. J. (2008). Prevalence, correlates, disability, andcomorbidity of DSM–IV borderline personality disorder: Results fromthe Wave 2 National Epidemiologic Survey on Alcohol and RelatedConditions. Journal of Clinical Psychiatry, 69, 533–545. http://dx.doi.org/10.4088/JCP.v69n0404
Gratz, K. L., Rosenthal, M. Z., Tull, M. T., Lejuez, C. W., & Gunderson,J. G. (2010). An experimental investigation of emotional reactivity anddelayed emotional recovery in borderline personality disorder: The roleof shame. Comprehensive Psychiatry, 51, 275–285. http://dx.doi.org/10.1016/j.comppsych.2009.08.005
Hawes, D. J., Helyer, R., Herlianto, E. C., & Willing, J. (2013). Borderlinepersonality features and implicit shame-prone self-concept in middlechildhood and early adolescence. Journal of Clinical Child and Adoles-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
61SHAME, HOSTILITY, IRRITABILITY, AND BPD SYMPTOMS
cent Psychology, 42, 302–308. http://dx.doi.org/10.1080/15374416.2012.723264
Hoeppner, B. B., Kelly, J. F., Urbanoski, K. A., & Slaymaker, V. (2011).Comparative utility of a single-item versus multiple-item measure ofself-efficacy in predicting relapse among young adults. Journal of Sub-stance Abuse Treatment, 41, 305–312. http://dx.doi.org/10.1016/j.jsat.2011.04.005
Horesh, N., Orbach, I., Gothelf, D., Efrati, M., & Apter, A. (2003).Comparison of the suicidal behavior of adolescent inpatients with bor-derline personality disorder and major depression. Journal of Nervousand Mental Disease, 191, 582–588. http://dx.doi.org/10.1097/01.nmd.0000087184.56009.61
Jovev, M., & Jackson, H. J. (2004). Early maladaptive schemas in person-ality disordered individuals. Journal of Personality Disorders, 18, 467–478. http://dx.doi.org/10.1521/pedi.18.5.467.51325
Keenan, K., Hipwell, A., Chung, T., Stepp, S., Stouthamer-Loeber, M.,Loeber, R., & McTigue, K. (2010). The Pittsburgh Girls Study: Over-view and initial findings. Journal of Clinical Child and AdolescentPsychology, 39, 506–521. http://dx.doi.org/10.1080/15374416.2010.486320
Kobak, R., Zajac, K., & Smith, C. (2009). Adolescent attachment andtrajectories of hostile–impulsive behavior: Implications for the develop-ment of personality disorders. Development and Psychopathology, 21,839–851.
Lewis, M. (2000). Self-conscious emotions: Embarrassment, pride, shame,and guilt. In M. Lewis & J. Haviland-Jones (Eds.), Handbook of emo-tions (2nd ed., pp. 623–636). New York, NY: Guilford Press.
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderlinepersonality disorder. New York, NY: Guilford Press.
Lutwak, N., Panish, J. B., Ferrari, J. R., & Razzino, B. E. (2001). Shameand guilt and their relationship to positive expectations and anger ex-pressiveness. Adolescence, 36, 641–653.
Morey, L. C. (1991). Personality assessment inventory: Professional man-ual. Odessa, FL: Psychological Assessment Resources.
Muthén, B. O., & Muthén, L. K. (2012). Mplus user’s guide (7th ed.). LosAngeles, CA: Author.
O’Brien, R. M. (2007). A caution regarding rules of thumb for varianceinflation factors. Quality & Quantity: International Journal of Method-ology, 41, 673–690. http://dx.doi.org/10.1007/s11135-006-9018-6
Pfohl, B., Blum, N., & Zimmerman, M. (1997). Structured interview forDSM–IV personality. Washington, DC: American Psychiatric Press.
Preacher, K. J., Curran, P. J., & Bauer, D. J. (2006). Computational toolsfor probing interactions in multiple linear regression, multilevel model-ing, and latent curve analysis. Journal of Educational and BehavioralStatistics, 31, 437–448. http://dx.doi.org/10.3102/10769986031004437
Primack, B. A., Silk, J. S., DeLozier, C. R., Shadel, W. G., DillmanCarpentier, F. R., Dahl, R. E., & Switzer, G. E. (2011). Using ecologicalmomentary assessment to determine media use by individuals with andwithout major depressive disorder. Archives of Pediatrics & AdolescentMedicine, 165, 360 –365. http://dx.doi.org/10.1001/archpediatrics.2011.27
Rizvi, S. L., Brown, M. Z., Bohus, M., & Linehan, M. M. (2011). The roleof shame in the development and treatment of borderline personalitydisorder. In R. L. Dearing & J. P. Tangney (Eds.), Shame in the therapyhour (pp. 237–260). Washington, DC: American Psychological Associ-ation; US. http://dx.doi.org/10.1037/12326-010
Rizvi, S. L., & Linehan, M. M. (2005). The treatment of maladaptiveshame in borderline personality disorder: A pilot study of “oppositeaction.” Cognitive and Behavioral Practice, 12, 437–447. http://dx.doi.org/10.1016/S1077-7229(05)80071-9
Rösler, M., Retz, W., Yaqoobi, K., Burg, E., & Retz-Junginger, P. (2009).Attention deficit/hyperactivity disorder in female offenders: Prevalence,psychiatric comorbidity and psychosocial implications. European Ar-
chives of Psychiatry and Clinical Neuroscience, 259, 98–105. http://dx.doi.org/10.1007/s00406-008-0841-8
Rüsch, N., Lieb, K., Göttler, I., Hermann, C., Schramm, E., Richter, H., . . .Bohus, M. (2007). Shame and implicit self-concept in women withborderline personality disorder. The American Journal of Psychiatry,164, 500–508. http://dx.doi.org/10.1176/appi.ajp.164.3.500
Rüsch, N., Schiel, S., Corrigan, P. W., Leihener, F., Jacob, G. A.,Olschewski, M., . . . Bohus, M. (2008). Predictors of dropout frominpatient dialectical behavior therapy among women with borderlinepersonality disorder. Journal of Behavior Therapy and ExperimentalPsychiatry, 39, 497–503. http://dx.doi.org/10.1016/j.jbtep.2007.11.006
Scheel, C. N., Schneid, E.-M., Tuescher, O., Lieb, K., Tuschen-Caffier, B.,& Jacob, G. A. (2013). Effects of shame induction in borderline per-sonality disorder. Cognitive Therapy and Research, 37, 1160–1168.
Schoenleber, M., & Berenbaum, H. (2012a). Aversion and proneness toshame in self- and informant-reported personality disorder symptoms.Personality Disorders: Theory, Research, and Treatment, 3, 294–304.http://dx.doi.org/10.1037/a0025654
Schoenleber, M., & Berenbaum, H. (2012b). Shame regulation in person-ality pathology. Journal of Abnormal Psychology, 121, 433–446. http://dx.doi.org/10.1037/a0025281
Scollon, C., Kim-Prieto, C., & Diener, E. (2003). Experience sampling:Promises and pitfalls, strengths and weaknesses. Journal of HappinessStudies, 4, 5–34. http://dx.doi.org/10.1023/A:1023605205115
Silk, J. S., Forbes, E. E., Whalen, D. J., Jakubcak, J. L., Thompson, W. K.,Ryan, N. D., . . . Dahl, R. E. (2011). Daily emotional dynamics indepressed youth: A cell phone ecological momentary assessment study.Journal of Experimental Child Psychology, 110, 241–257. http://dx.doi.org/10.1016/j.jecp.2010.10.007
Skodol, A. E., Bender, D. S., Morey, L. C., Clark, L. A., Oldham, J. M.,Alarcon, R. D., . . . Siever, L. J. (2011). Personality disorder typesproposed for DSM-5. Journal of Personality Disorders, 25, 136–169.http://dx.doi.org/10.1521/pedi.2011.25.2.136
Stadter, M. (2011). The inner world of shaming and ashamed: An objectrelations perspective and therapeutic approach. In R. L. Dearing & J. P.Tangney (Eds.), Shame in the therapy hour (pp. 45–68). Washington,DC: American Psychological Association. http://dx.doi.org/10.1037/12326-002
Stepp, S. D., Burke, J. D., Hipwell, A. E., & Loeber, R. (2012). Trajectoriesof attention deficit hyperactivity disorder and oppositional defiant dis-order symptoms as precursors of borderline personality disorder symp-toms in adolescent girls. Journal of Abnormal Child Psychology, 40,7–20. http://dx.doi.org/10.1007/s10802-011-9530-6
Stone, A. A., & Shiffman, S. (1994). Ecological momentary assessment (EMA) inbehavioral medicine. Annals of Behavioral Medicine, 16, 199–202.
Tangney, J. P., Wagner, P., Fletcher, C., & Gramzow, R. (1992). Shamedinto anger? The relation of shame and guilt to anger and self-reportedaggression. Journal of Personality and Social Psychology, 62, 669–675.http://dx.doi.org/10.1037/0022-3514.62.4.669
Tangney, J. P., Wagner, P., & Gramzow, R. (1992). Proneness to shame,proneness to guilt, and psychopathology. Journal of Abnormal Psychol-ogy, 101, 469–478. http://dx.doi.org/10.1037/0021-843X.101.3.469
Tangney, J. P., Wagner, P. E., Hill-Barlow, D., Marschall, D. E., &Gramzow, R. (1996). Relation of shame and guilt to constructive versusdestructive responses to anger across the lifespan. Journal of Personalityand Social Psychology, 70, 797–809. http://dx.doi.org/10.1037/0022-3514.70.4.797
Thomaes, S., Bushman, B. J., Stegge, H., & Olthof, T. (2008). Trumpingshame by blasts of noise: Narcissism, self-esteem, shame, and aggres-sion in young adolescents. Child Development, 79, 1792–1801. http://dx.doi.org/10.1111/j.1467-8624.2008.01226.x
Velotti, P., Elison, J., & Garofalo, C. (2014). Shame and aggression:Different trajectories and implications. Aggression and Violent Be-havior, 19, 454 – 461. http://dx.doi.org/10.1016/j.avb.2014.04.011
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
62 SCOTT ET AL.

Welch, S. S., & Linehan, M. M. (2002). High-risk situations associatedwith parasuicide and drug use in borderline personality disorder. Journalof Personality Disorders, 16, 561–569. http://dx.doi.org/10.1521/pedi.16.6.561.22141
Winograd, G., Cohen, P., & Chen, H. (2008). Adolescent borderlinesymptoms in the community: Prognosis for functioning over 20 years.Journal of Child Psychology and Psychiatry, 49, 933–941. http://dx.doi.org/10.1111/j.1469-7610.2008.01930.x
Zanarini, M. C., Frankenburg, F. R., Hennen, J., & Silk, K. R. (2003). The
longitudinal course of borderline psychopathology: 6-year prospectivefollow-up of the phenomenology of borderline personality disorder. TheAmerican Journal of Psychiatry, 160, 274–283. http://dx.doi.org/10.1176/appi.ajp.160.2.274
Zanarini, M. C., Horwood, J., Wolke, D., Waylen, A., Fitzmaurice, G., &Grant, B. F. (2011). Prevalence of DSM–IV borderline personality dis-order in two community samples: 6,330 English 11-year-olds and 34,653American adults. Journal of Personality Disorders, 25, 607–619. http://dx.doi.org/10.1521/pedi.2011.25.5.607
Correction to Clark and Ro (2014)
In the article “Three-Pronged Assessment and Diagnosis of Personality Disorder and Its Conse-quences: Personality Functioning, Pathological Traits, and Psychosocial Disability” by Lee AnnaClark and Eunyoe Ro (Personality Disorders: Theory, Research, and Treatment, 2014, Vol. 5,No. 1, pp. 55–69. doi: 10.1037/per0000063), there was an error in the results. Under thesubheading, Personality Traits—Functioning Relations, on page 63, the second, third, andfourth paragraph have been revised. Starting from the fourth sentence in the second paragraph thetext should read, “The two-factor solution reflected, broadly speaking, Internalizing functioningand traits, including traits marking N/NA versus PA/E and Well being/Positive functioning versuslow basic and self functioning (e.g., TCI Harm Avoidance, SIPP Identity, MDPF Non-coping vs.PWB Life-and-Self Satisfaction, SNAP Positive Temperament, WHOQOL Health) for the firstfactor, and Externalizing traits, including both Disinhibition and Agreeableness/Antagonism (e.g.,SNAP Disinhibition vs. TCI Cooperativeness) with only two functioning scales (SIPP SocialConcordance and Responsibility) for the second. In the three-factor solution, the second factor ofthe two-factor solution (primarily trait scales, except for three SIPP interpersonal functioningscales) formed the second factor, whereas the large Internalizing factor split into a bipolar factorwith more positive traits (e.g., TCI Persistence, IPIP FFM Altruism) on one end and Interpersonal(Personality) Dysfunction on the other, which formed the third factor, and a first large Internal-izing factor characterized by N/NA and the remaining functioning measures.
In the four-factor solution, clearer factors began to emerge: The first factor was formed fromfunctioning scales marking Well-Being versus Self Pathology and trait scales reflecting N/NA.Functioning scales marking Poor Social/Interpersonal Functioning and trait measures of Agree-ableness and Sociability comprised the second factor. Self-focused traits with a range ofdisinhibition and positive but unusual perceptivity content (e.g., SNAP Impulsivity, TCI Self-transcendence, respectively) formed the third factor and the basic functioning scales broke off toform the core of the fourth factor along with two “compulsivity” scales (SNAP Workaholism andPropriety) versus positive functioning (e.g., WHOQOL Health). Thus, the first two factorsblended functioning and personality-trait scales, whereas the latter two were, respectively, a purepersonality-trait factor and a (mostly) functioning factor.
At the five-factor level, the first, second, and fourth factors remained largely the same, whereasthe third factor broke into a more focused disinhibition trait factor and another trait factor that wasloaded most strongly with two scales each from the previous second and fourth factors thatreflected rigidity (e.g., SNAP Propriety) and goal engagement (e.g., TCI Persistence) along withthe positive, unusual perceptivity content from the third factor.”
http://dx.doi.org/10.1037/per0000103
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
63SHAME, HOSTILITY, IRRITABILITY, AND BPD SYMPTOMS
Related Documents











