A aron Bronner, OD, began yesterday morning’s ses- sion, “Managing Uveitis with Flair,” with a goal of pro- viding “not just facts, but clini- cally useful information on uve- itis you can use today.” He spent the first few minutes dispelling the common mindset that the condition “is no big deal,” with some sobering numbers. Uveitis is causative in 10% to 15% of total blindness cases in the developed world, he said, and although many gradually regain vision, up to 20% are left legally blind. Don’t Disrespect the Disease So how do clinicians give uveitis the respect it deserves? By better understanding its sight-threatening implications, differentials and treat- ment options. Dr. Bronner dove into these topics with a brief primer on how cell and flare cause vision loss, and the long-term implications of ocular inflammation, includ- ing cataracts, glaucoma, cystoid macular edema and, less often, retinal detachment, epiretinal membrane and band keratopathy. After discussing the many as- sociated conditions, Dr. Bronner provided a few clinical pearls on managing uveitis patients. “If you aren’t comfortable with gonio, you shouldn’t manage uveitis patients,” Dr. Bronner said. “If you aren’t willing to dilate these patients, don’t manage uveitis.” Therapy Rundown Dr. Bronner then moved on to treatment protocols. The ultimate goal—eliminate inflammation—is simple, and he walked attendees through the common therapy DAILY FRIDAY , MARCH 2, 2018 O n Thursday morning, two leading experts in glaucoma treatment and surgery, James Thimons, OD, and Robert Noecker, MD, shared the stage to discuss why 2017 was one of the most exciting and innovative years in the recent history of glaucoma care. In the “Gear Up for Glaucoma” lecture, Dr. Thimons noted that two new drugs came out in 2017, the first time new drugs have been released in 21 years. The discussion delved deep into the next generation of therapeutics, the evolving science of surgical intervention, including mini- mally invasive glaucoma surgeries (MIGS), and the technologies optometrists can use for earlier detection and management of glaucoma. OCT for the OD “The earlier we can identify it, the earlier we can treat it, and there’s no question that earlier intervention in glaucoma does save sight over time,” said Dr. Thimons, making it essential that ODs not only have the technology in their offices to detect disease early, but that they’re also keen to use it. “OCT is the window to the brain and almost as good as MRI in the early identification of the disease state. It takes us to a completely different level of expertise,” added Dr. Thimons. Both doctors agreed that ganglion cell analysis through OCT is the frontier of early glaucoma diagnosis. “While it used to be state-of-the- art care, you look at the ubiquity of the OCT machine now—a clinically useful tool that we rely on for our clinical exams and for decision making—so yes, along with visual field testing, OCT testing has become standard of care,” said Dr. Noecker. Outside Office Hours From there, the discussion turned to a handful of newly approved technologies that are changing the face of glaucoma management, such as add- ing the potential for 24-hour intraocular pressure (IOP) monitoring into the approach to manage- ment. One device, the iCare home tonometer, allows doctors to have IOP data throughout the day, even beyond office hours. Catching Up to the Silent Thief WHAT’S INSIDE • The dynamic duo of Melton and Thomas wowed the crowd ..... 3 • Olympian Laurie Hernandez opened the exhibits ................ 3 • How to keep your cool during an ocular emergency ................. 4 • See what student and resident events are coming up .............5 • Don’t miss tomorrow’s special session on the anterior segment ................................ 7 • Want to learn about amniotic membranes? We’ve got you covered ................................... 8 • These pediatric pearls can make your practice more kid- friendly ................................. 18 • What OCT can do for your practice ................................ 22 New drugs, technologies and awareness can bring ODs to higher levels in diagnosing and treating glaucoma. Drs. Thimons and Noecker discussed innovations and new directions for glaucoma treatment. See GLAUCOMA, Page 21 See UVEITIS, Page 21 REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018 Topics covered in today’s OD courses, p.6 Special five-page guide to the exhibits, p.10 Tomorrow’s ‘What’s Brewing?’ series, p.18 All You Need to Know About Uveitis Attendees left this course with a comprehensive understanding of the many etiologies of the condition—and how to handle them. HLA-B27-associated uveitis can sometimes present with a secluded pupil, which has to be treated with a peripheral iridotomy (PI). “While the PI will most likely exacerbate the uveitis, you have to lower that pressure,” said Dr. Bronner.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Aaron Bronner, OD, began yesterday morning’s ses-sion, “Managing Uveitis
with Flair,” with a goal of pro-viding “not just facts, but clini-cally useful information on uve-itis you can use today.” He spent the fi rst few minutes dispelling the common mindset that the condition “is no big deal,” with some sobering numbers.
Uveitis is causative in 10% to 15% of total blindness cases in the developed world, he said, and although many gradually regain vision, up to 20% are left legally blind.
Don’t Disrespect the DiseaseSo how do clinicians give uveitis the respect it deserves? By better understanding its sight-threatening
implications, differentials and treat-ment options. Dr. Bronner dove into these topics with a brief primer on how cell and fl are cause vision loss, and the long-term implications of ocular infl ammation, includ-
ing cataracts, glaucoma, cystoid macular edema and, less often, retinal detachment, epiretinal membrane and band keratopathy.
After discussing the many as-sociated conditions, Dr. Bronner provided a few clinical pearls on managing uveitis patients. “If you aren’t comfortable with gonio, you shouldn’t manage uveitis patients,” Dr. Bronner said. “If you aren’t willing to dilate these patients, don’t manage uveitis.”
Therapy RundownDr. Bronner then moved on to
treatment protocols. The ultimate goal—eliminate infl ammation—is simple, and he walked attendees through the common therapy
DAILYFRIDAY , MARCH 2, 2018
On Thursday morning, two leading experts in glaucoma treatment and surgery, James Thimons, OD, and Robert Noecker, MD,
shared the stage to discuss why 2017 was one of the most exciting and innovative years in the recent history of glaucoma care.
In the “Gear Up for Glaucoma” lecture, Dr. Thimons noted that two new drugs came out in 2017, the fi rst time new drugs have been released in 21 years. The discussion delved deep into the next generation of therapeutics, the evolving science of surgical intervention, including mini-mally invasive glaucoma surgeries (MIGS), and the technologies optometrists can use for earlier detection and management of glaucoma.
OCT for the OD“The earlier we can identify it, the earlier we can treat it, and there’s no question that earlier intervention in glaucoma does save sight over time,” said Dr. Thimons, making it essential that
ODs not only have the technology in their offi ces to detect disease early, but that they’re also keen to use it. “OCT is the window to the brain and almost as good as MRI in the early identifi cation of the disease state. It takes us to a completely different level of expertise,” added Dr. Thimons.
Both doctors agreed that ganglion cell analysis through OCT is the frontier of early glaucoma diagnosis. “While it used to be state-of-the-art care, you look at the ubiquity of the OCT machine now—a clinically useful tool that we rely on for our clinical exams and for decision making—so yes, along with visual fi eld testing, OCT testing has become standard of care,” said Dr. Noecker.
Outside Offi ce Hours From there, the discussion turned to a handful of newly approved technologies that are changing the face of glaucoma management, such as add-ing the potential for 24-hour intraocular pressure (IOP) monitoring into the approach to manage-ment. One device, the iCare home tonometer, allows doctors to have IOP data throughout the day, even beyond offi ce hours.
Catching Up to the Silent Thief
WHAT’S INSIDE• The dynamic duo of Melton and
Thomas wowed the crowd .....3
• Olympian Laurie Hernandez opened the exhibits ................3
• How to keep your cool during an ocular emergency .................4
• See what student and resident events are coming up .............5
• Don’t miss tomorrow’s special session on the anterior segment ................................7
• Want to learn about amniotic membranes? We’ve got you covered ...................................8
• These pediatric pearls can make your practice more kid-friendly .................................18
• What OCT can do for your practice ................................22
New drugs, technologies and awareness can bring ODs to higher levels in diagnosing and treating glaucoma.
Drs. Thimons and Noecker discussed innovations
and new directions for glaucoma treatment.
See GLAUCOMA, Page 21
See UVEITIS, Page 21
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Topics covered in today’s OD courses, p.6
Special fi ve-page guide to the exhibits, p.10
Tomorrow’s ‘What’s Brewing?’ series, p.18
All You Need to Know About Uveitis Attendees left this course with a comprehensive understanding of the many etiologies of the condition—and how to handle them.
HLA-B27-associated uveitis can sometimes
present with a secluded pupil, which has to
be treated with a peripheral iridotomy (PI).
“While the PI will most likely exacerbate the
uveitis, you have to lower that pressure,”
said Dr. Bronner.
000_sd0318_FRI_final.indd 1000_sd0318_FRI_final.indd 1 3/1/18 5:59 PM3/1/18 5:59 PM

2018MEETINGSNASHVILLE, TNNashville Marriott at VanderbiltProgram Chair: Paul Karpecki, ODwww.reviewofoptometry.com/nashville2018
SAN DIEGO, CA**
San Diego Marriott Del MarProgrom Chair: Paul Karpecki, ODwww.reviewofoptometry.com/sandiego2018
ORLANDO, FLDisney’s Yacht & Beach ClubProgram Chair: Paul Karpecki, ODwww.reviewofoptometry.com/orlando2018
ARLINGTON, VAThe Westin Arlington GatewayProgram Chair: Paul Karpecki, ODwww.reviewofoptometry.com/arlington2018
APRIL 6-8, 2018
APRIL 26-29, 2018
MAY 17-20, 2018
NOVEMBER 2-4, 2018
NEW TECHNOLOGIES & TREATMENTS IN
Eye Care &
2018
REVIEW OF OPTOMETRY® EDUCATIONAL MEETINGS OF CLINICAL EXCELLENCE
Visit our website for the latest information:
www.reviewofoptometry.com/eventsemail: [email protected] | call: 866-658-1772
Review of Optometry® partners with Salus University for those ODs who are licensed in states that require university credit. See Review website for any meeting schedule changes or updates.
*Approval pending
Administered byReview of Optometry ®
OPTOMETRIC CORNEA, CATARACT AND REFRACTIVE SOCIETY
**15th Annual Education Symposium
Joint Meeting with NT&T in Eye Care
Earn up to
18-29 CE Credits*

3DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
In the second installment of their “Eye Care Update” lecture, op-tometry’s dynamic duo—Randall Thomas, OD, and Ron Melton,
OD—ran through selected hot topics revealed in both recent research and their very own offi ces.
“Our goal is to spend the year looking at the literature, fi ltering through it, incorporating the impor-tant concepts into our clinical prac-tice, trying them, making sure they work, and then bringing them to you so you too can take the pearls back to your practice early next week,” said Dr. Melton in the opening of their second Wednesday course.
The discussion focused on four take-home messages: (1) be prepared and confi dent for anything that may walk through the offi ce door, (2) rely less on antibiotics and referring out for non-surgical procedures, (3) pay attention to infl ammation because it’s telling you something and, (4) when in doubt, use steroids.
Saved by ShingrixThe pair started by addressing the big hitters of these long winter months: herpes simplex virus, herpes zoster
ophthalmicus and herpes simplex keratitis. They touched on Shingrix (GlaxoSmithKline), the new talk of the town in anti-shingle vaccinations. While Drs. Melton and Thomas playfully disagreed on whether the vaccine will truly replace Zostavax (Merck), they warned the audience that “shingles is going to become more and more common for about 20 to 30 more years, until fi nally it will fade away. That’s just the epide-miological reality,” said Dr. Thomas, so ODs “should be prepared.”
Science, Not Habit Building on their earlier morning discussions around the importance of using oral and topical steroids to treat infl ammation, Drs. Melton and Thomas called on new fi ndings from the Antibiotic Resistance Monitoring in Ocular Microorganisms study. As resistance to commonly prescribed antibiotics is an ever-growing con-cern, the doctors announced in no uncertain terms that ODs should be consciously prescribing on a case-by-case basis, rather than by habit.
“Every time you think about prescribing an antibiotic, even topical
ones,” said Dr. Thomas, “we would beg of you to stop because the chanc-es are, you’re wrong.” The epidemi-ology of acute red eye, he explained, “is one of infl ammation, so antibiot-ics will have very little utility here.” Let science guide your care. “Do not do things out of habit; follow the lit-erature and make scientifi cally sound prescribing decisions.”
These sentiments resurfaced as the doctors confronted the next leg of their discussion: differentiating between corneal ulcers and infi ltrates. As infi ltrates are more common and represent an underlying infl amma-tory condition, ocular steroids, often combined with an antibiotic, have become the preferred treatment ap-proach. The fast action of the steroid, Dr. Melton advised, will aid in pre-venting a secondary infection or the much less desirable corneal ulcer.
The Ungrateful DED Threading the theme of prioritiz-ing infl ammation into the second half of their discussion, Drs. Melton and Thomas proposed new ways to target dry eye disease (DED), which has become more widely accepted as
an infl ammatory condition. Dr. Thomas suggested that
everyone fi nd themselves a copy of a comprehensive supplement to the November 2017 Ophthamology, which highlights new global perspec-tives on treating DED. Both agree that the supplement is one of the most innovative pieces of this year’s literature. “Infl ammation is one of the major targets in treating DED,” read Dr. Thomas, “and breaking the cycle of infl ammation is crucial in improving symptoms.” Both doctors continued to cite key publications and case studies released over the last year that list various holistic methods (blinking exercises, warm compresses, fi sh oils, artifi cial tears) that patients can use to better address infl ammation and actively treat DED.
The lecturers concluded the session by reminding all ODs—new to the fi eld and veterans alike—of the great role and responsibility each takes on in their practice. Take a step back from the knee-jerk reaction to refer out, they said. You don’t have to be a genius to do this stuff, “you just have to have the courage to do what you know is right,” urged Dr. Thomas. “Tell your patients, ‘I am your eye doctor; if you ever have a problem, call me fi rst.’ So, now we’re growing instead of referring, and that’s how we grow as a profession.” •
Finding Room to GrowBy sticking to science and practicing with confidence, ODs can deliver for their patients and grow as a profession.
Drs. Melton and Thomas presented
part two of their “Eye Care Update”
series—and encouraged attendees to
ease up on referring. “You just have to
have the courage to do what you know
is right,” Dr. Thomas said.
Laurie Hernandez, 2016 Olympic gold medalist, addressed the crowd at
yesterday’s grand openng of the exhibit hall (top). She was then joined
by outgoing SECO president Lynn Hammonds, OD, for the ribbon cutting
ceremony (right). Ms. Hernandez is a spokesperson for Alcon’s Dailies
AquaComfort Plus contact lenses and its #InvisibleEdge campaign.
EXHIBIT HALL OPENING CEREMONY
000_sd0318_FRI_final.indd 3000_sd0318_FRI_final.indd 3 3/1/18 5:49 PM3/1/18 5:49 PM

Black humor enthusiasts are well aware of the Darwin Awards—an unoffi cial listing of the
dumbest ways people have injured themselves each year. Rich Mangan, OD, kept the crowd of his pre-lunch presentation “Be Prepared! Handling Ocular Emergencies” engaged with reminders that people often make risky choices; photos of ladders propped up on wheeled garbage cans, motorcyclists treating their moving vehicle like a La-Z-Boy and even a video of a marksman checking the barrel of his fi rearm only to have it nearly blow his nose off.
Dr. Mangan, who writes Review of Optometry’s Urgent Care column, even offered a collection of cases he’s witnessed that may offer an optomet-ric analog to the Darwins, such as patients who have stored soft contact lenses in pond water, shot themselves in the eye with paintball guns and even enucleated their own eyes. Call them the “Mangan Awards” per-haps, but the speaker also offered careful guidance on how attendees can treat these patients.
The fi rst step, Dr. Mangan said, is identifying whether or not your patient has a true ocular emergency, and if it needs to be treated immedi-ately (within a matter of hours), ur-gently (within a day), soon (within a week) or on an elective basis (within a month). Making that call begins with training staff to understand “the art of triage,” Dr. Mangan said. “It’s defi ned as sorting patients ac-cording to the urgency of their need for care.”
The presentation consisted of a
number of case examples to demon-strate how ODs can manage ocular emergencies.
You’re So Vein Patients with ocular trauma may not realize it, but some of their symptoms may indicate that they’re experienc-ing a central retinal artery occlusion. Fundus imaging, however, will reveal the damage to their vascular system. Be on the lookout for superfi cial opacifi cation or whitening of the retina in the posterior pole with a cherry-red spot in the center of the macula, Dr. Mangan said, and if you suspect it, act immediately. “When you go outside a four-hour win-dow, your prognosis is really, really poor,” he explained, but “it’s still recommended, even within a six- to eight-hour time frame, that you try to re-perfuse the eye.” Dr. Mangan said not to spend precious time taking a complete family history in these cases—treat fi rst. That intervention can include anything from orbital
massage to anterior paracentesis to a special Nd:YAG laser application. The goal here is to reduce the pres-sure on the eye.
Burn, Baby, Burn“There are some chemicals that can eat through a cornea, or the eye, in only fi ve minutes,” he warned. Alkali-based chemicals are more severe than acid-based ones, but Dr. Mangan said all contingencies, such as how much of the chemical got in the eye and how long ago it hap-pened, play a role. Sixty percent of these types of burns occur at work, but plenty of household items contain dangerous chemicals, and children are especially prone to this type of injury. For these cases, manage-ment needs to begin over the phone because “you want to start irrigation right away,” he said. Instruct the patient to fi nd a shower or even an outdoor hose. Don’t even try to take contact lenses out, he noted. Just keep irrigating. Also, don’t forget to ask patients to bring the container that held the chemical if they’re not sure what it was.
Once they arrive at the offi ce, refer to the Roper-Hall classifi cation of ocular surface burns to judge how to start treatment. “If it’s a basic substance or an alkali burn, you may want to avoid a topical glaucoma drop and use an oral instead,” Dr. Mangan said. And “if there’s any kind of limbal blanching, I think the patient will benefi t from a Prokera amniotic membrane (Bio-Tissue). Sometimes I’ll wait until three to fi ve days out from the burn and assess the
healing. If the healing is a little slow, I’ll turn to the Prokera.”
Not-so-gentle GiantIn cases of giant cell arteritis, if they’re in your chair, chances are they’ve already lost vision in at least one eye. “Clearly, if they’ve already had vision loss in one eye, this is a true ocular emergency,” Dr. Mangan said. And if there’s any doubt, get a blood test. “It’s urgent we get these patients started on steroids right away,” he said. Other treatments include obtaining a biopsy, but even that’s not 100% reliable. The Ameri-can College of Rheumatology offers a fi ve-point scoring system. If your patient has any three of these, you’re justifi ed in starting steroids:
• Older than 50 years of age.• A Westergren ESR greater than
50.• Temporal artery tenderness or
abnormality on exam.• New-onset headache.• Positive temporal artery biopsy.
Soft CellOne patient presented to Dr. Mangan complaining of a “pulling” sensation in his left eye when looking superior temporal. The diagnosis turned out to be periorbital cellulitis, an infec-tion usually caused by Staphylococ-cus or Streptococcus.
For patients with tenderness, proptosis and blurred vision, he said, ask if they’ve had any surgeries, such as lid and sinus surgeries (or a history of trauma), because patients who’ve undergone these can get infections even months to years later. Unlike with chemical burns, “you want to get as much of a history as you can” to uncover the cause of the infection.
Initial treatment will include an-tibiotics, but if the problem persists, patients may need to undergo a par-ticularly gory procedure that requires a surgeon to “push out the pus.” A video of this elicited uncomfortable groans, even from this room full of doctors. •
Emergency Protocols in OptometryWhen patients stick their noses—or eyes—where they don’t belong, ODs must act fast.
DAILY4
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Dr. Mangan presented urgent
cases from the strange to the scary
in yesterday’s course on ocular
emergencies.
‘Immediate Care’ Examples
• Chemical burn• Acute ocular trauma • Sudden vision loss• Severe pain• Brow pain with nausea/
vomiting
‘Urgent Care’ Examples
• Corneal abrasion • Foreign body• Flashes and fl oaters plus
vision change• Monocular patients• Postoperative patients
‘Obtain Care Soon’ Examples
• Recent-onset diplopia• Recent-onset ptosis• Distorted vision for less
than two weeks• Photophobia• Mild pain for 2-3 days
‘Elective Care’ Examples
• Dry, itchy, watering• Fluctuating vision for
weeks• Broken glasses• Mild redness• Lumps and bumps
000_sd0318_FRI_final.indd 4000_sd0318_FRI_final.indd 4 3/1/18 5:49 PM3/1/18 5:49 PM

REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
5DAILY
SECO Welcomes Students and ResidentsAbundant opportunities for the next generation of optometrists to learn and connect.
SECO is committed to the training and education of the next generation of opto-
metric professionals, and our growing student program show-cases that commitment.
Students and residents get free access to SECO’s world-renowned OD continuing education program, including Special Sessions and MedPro360. Residents may reserve space in courses ahead of time, and stu-dents may attend as long as space is available. Learning Labs are not included.
The Student Lunch Symposium on Saturday from 12–1:15pm is your chance to enjoy a free lunch while you hear from industry leaders Alcon, Johnson & John-son Vision, CooperVision and Hoya. You could win a $1,000
scholarship courtesy of SECO International just by attending.
The Student Party this year is joining with another exciting event at SECO, The Bad Habits–Eye Docs of Rock Charity Event benefi tting Optometry Cares. Students will have a special VIP Lounge area at the party with special seating, games and drink tickets courtesy of Hoya. The party is Friday from 9pm to midnight at the College Football Hall of Fame.
Pick up your $100 cash sti-pend, courtesy of SECO Interna-tional, on Saturday from 3–4pm in the student lounge inside the exhibit hall. You must bring your SECO badge and photo ID with you. Don’t be late!
Be sure to check out the new Student Escape Room Adventure
presented by VSP Global. Test your optometry knowledge as you work together searching the room to fi nd clues, solve riddles and crack codes to escape the room within the hour. Sign up in advance in the student lounge in the exhibit hall or at the link on AttendSECO.com.
Be sure to check out the return of SECO’s Multimedia Poster Presentations in the exhibit hall throughout the show.
Student-focused practice man-agement courses will be available on Saturday, March 3 at the Practice Management Education Theater brought to you by VSP Global in the exhibit hall. The topics are: Starting Cold Versus Buying a Practice and Student Debt: The Numbers Actually Work in Your Favor. •
SECO is happy to bring 2019’s conference to New Orleans Febru-
ary 20-24 for the fi rst SECO congress held outside of Atlanta in 60 years! Don’t miss out on this exciting new chapter. Visit booth #1633 to learn about everything there is to do in New Orleans. You can fi nd out about all of the great hotel options the city has to offer and book your room today.
We’ll be giving away New Orleans-themed prizes throughout the show, including a Grand Prize Giveaway for those who book their 2019 hotel reservations that includes:
• Two-night hotel stay from Star-wood
• $400 Delta airline voucher• $150 gift card to Arnaud’s Res-
taurant• All-inclusive Package Registration
for SECO 2019.The grand prize winner will be an-
nounced on Saturday at 4pm with free Bloody Marys. You must be present to win, so be sure to join us at booth #1633.
SECO Welcomes Students and ResidentsAbundant opportunities for the next generation of optometrists to learn and connect.
SECO is happy to bring 2019’s conference to New Orleans Febru-
ary 20-24 for the fi rst SECO congress held outside of Atlanta in 60 years! Don’t miss out on this exciting new chapter. Visit booth #1633 to learn about everything there is to do in New Orleans. You can fi nd out about all of the great hotel options the city has to offer, and book your room today.
We’ll be giving away New Orleans-themed prizes throughout the show, including a Grand Prize Giveaway for those who book their 2019 hotel reservations that includes:
• Two-night hotel stay from Star-wood
• $400 Delta airline voucher• $150 gift card to Arnaud’s Res-
taurant• All-inclusive package registration
for SECO 2019.The grand prize winner will be an-
nounced on Saturday at 4pm with free Bloody Marys. You must be present to win, so be sure to join us at booth #1633.
SECO Moves to New
Orleans for 2019
Learn more, book your hotel
and win prizes at booth #1633.
000_sd0318_FRI_final.indd 5000_sd0318_FRI_final.indd 5 2/28/18 1:55 PM2/28/18 1:55 PM
7DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Contiuned | FRIDAY, MARCH 2 OPTOMETRIC EDUCATION
SURGICAL PROCEDURES AND COMANAGEMENT
1–4pm Laser Learning Lab Lighthizer, Lewis, Walker Room A310
3–5pm Wet, Dry and Painful Eye Learning Lab Pate, Than, Elder, Clore Room A407
5–7pm High Tech Cataract Care Woodard Room A312
TEAM-CENTERED LEARNING (FOR ODs AND AOPs)
7–8am What’s Brewing? Controversies in Ocular Nutrition Gerson Room A311
10–11am MRSA: A Cause for Concern Mangan Room A313
10–11am Scleral Lenses Shovlin Room A311
1:30–2:30pm Managing Millennials in the Workplace Burns Room A315
2:30–3:30pm The New Customer Experience King Room A315
5–7pm Through the Eyes of Women: Caring for the Female Patient Than, Sclafani, Pate Room A311
5–7pm Seeing Stars: Concussions in Sports Weise Room A313
TECHNOLOGY
7–8am What’s Brewing? OCT Angiography Rixon Room A312
5–6pm 3D Printing in the Modern Dispensary Parker Room A304
Looking to brush up on your anterior seg-ment disease management skills? Then clear some space in your schedule for “Anterior
Segment Solutions.” In this Saturday morning Special Session course, Zaina Al-Mohtaseb, MD, assistant professor of ophthalmology at Baylor College of Medicine, will engage attend-ees in a detailed exploration of the ins and outs of the various anterior segment cases seen in clinical practice.
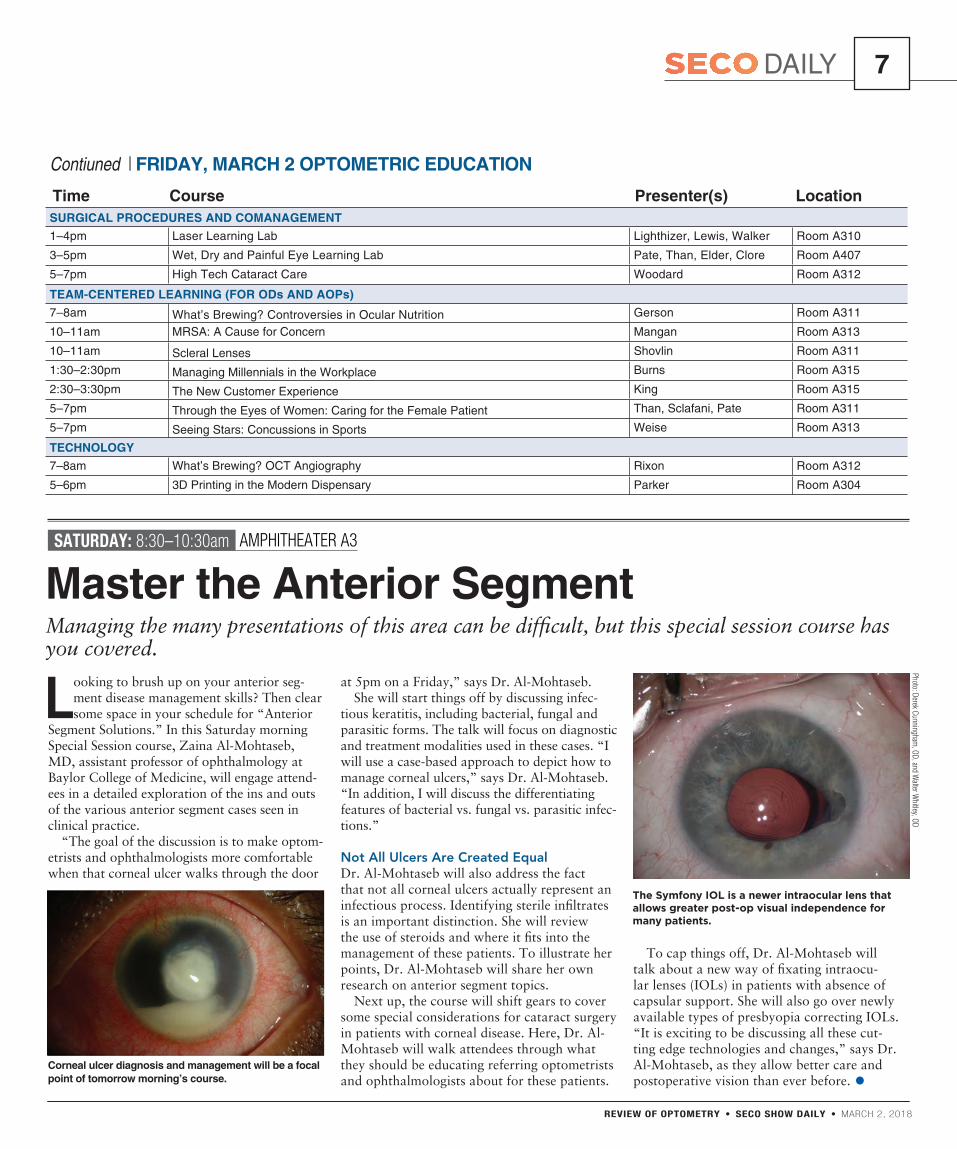
“The goal of the discussion is to make optom-etrists and ophthalmologists more comfortable when that corneal ulcer walks through the door
at 5pm on a Friday,” says Dr. Al-Mohtaseb.She will start things off by discussing infec-
tious keratitis, including bacterial, fungal and parasitic forms. The talk will focus on diagnostic and treatment modalities used in these cases. “I will use a case-based approach to depict how to manage corneal ulcers,” says Dr. Al-Mohtaseb. “In addition, I will discuss the differentiating features of bacterial vs. fungal vs. parasitic infec-tions.”
Not All Ulcers Are Created EqualDr. Al-Mohtaseb will also address the fact that not all corneal ulcers actually represent an infectious process. Identifying sterile infi ltrates is an important distinction. She will review the use of steroids and where it fi ts into the management of these patients. To illustrate her points, Dr. Al-Mohtaseb will share her own research on anterior segment topics.
Next up, the course will shift gears to cover some special considerations for cataract surgery in patients with corneal disease. Here, Dr. Al-Mohtaseb will walk attendees through what they should be educating referring optometrists and ophthalmologists about for these patients.
To cap things off, Dr. Al-Mohtaseb will talk about a new way of fi xating intraocu-lar lenses (IOLs) in patients with absence of capsular support. She will also go over newly available types of presbyopia correcting IOLs. “It is exciting to be discussing all these cut-ting edge technologies and changes,” says Dr. Al-Mohtaseb, as they allow better care and postoperative vision than ever before. •
Master the Anterior SegmentManaging the many presentations of this area can be diffi cult, but this special session course has you covered.
Corneal ulcer diagnosis and management will be a focal
point of tomorrow morning’s course.
SATURDAY: 8:30–10:30am AMPHITHEATER A3
The Symfony IOL is a newer intraocular lens that
allows greater post-op visual independence for
many patients.
Photo: D
erek Cunningham
, OD
, and Walter W
hitley, OD
Time Course Presenter(s) Location
000_sd0318_FRI_final.indd 7000_sd0318_FRI_final.indd 7 2/28/18 1:57 PM2/28/18 1:57 PM

7DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Continued | FRIDAY, MARCH 2 OPTOMETRIC EDUCATION
SURGICAL PROCEDURES AND COMANAGEMENT
1–4pm Laser Learning Lab Lighthizer, Lewis, Walker Room A310
3–5pm Wet, Dry and Painful Eye Learning Lab Pate, Than, Elder, Clore Room A407
5–7pm High Tech Cataract Care Woodard Room A312
TEAM-CENTERED LEARNING (FOR ODs AND AOPs)
7–8am What’s Brewing? Controversies in Ocular Nutrition Gerson Room A311
10–11am MRSA: A Cause for Concern Mangan Room A313
10–11am Scleral Lenses Shovlin Room A311
1:30–2:30pm Managing Millennials in the Workplace Burns Room A315
2:30–3:30pm The New Customer Experience King Room A315
5–7pm Through the Eyes of Women: Caring for the Female Patient Than, Sclafani, Pate Room A311
5–7pm Seeing Stars: Concussions in Sports Weise Room A313
TECHNOLOGY
7–8am What’s Brewing? OCT Angiography Rixon Room A312
5–6pm 3D Printing in the Modern Dispensary Parker Room A304
Looking to brush up on your anterior seg-ment disease management skills? Then clear some space in your schedule for “Anterior
Segment Solutions.” In this Saturday morning Special Session course, Zaina Al-Mohtaseb, MD, assistant professor of ophthalmology at Baylor College of Medicine, will engage attend-ees in a detailed exploration of the ins and outs of the various anterior segment cases seen in clinical practice.
“The goal of the discussion is to make optom-etrists and ophthalmologists more comfortable when that corneal ulcer walks through the door
at 5pm on a Friday,” says Dr. Al-Mohtaseb.She will start things off by discussing infec-
tious keratitis, including bacterial, fungal and parasitic forms. The talk will focus on diagnostic and treatment modalities used in these cases. “I will use a case-based approach to depict how to manage corneal ulcers,” says Dr. Al-Mohtaseb. “In addition, I will discuss the differentiating features of bacterial vs. fungal vs. parasitic infec-tions.”
Not All Ulcers Are Created EqualDr. Al-Mohtaseb will also address the fact that not all corneal ulcers actually represent an infectious process. Identifying sterile infi ltrates is an important distinction. She will review the use of steroids and where it fi ts into the management of these patients. To illustrate her points, Dr. Al-Mohtaseb will share her own research on anterior segment topics.
Next up, the course will shift gears to cover some special considerations for cataract surgery in patients with corneal disease. Here, Dr. Al-Mohtaseb will walk attendees through what they should be educating referring optometrists and ophthalmologists about for these patients.
To cap things off, Dr. Al-Mohtaseb will talk about a new way of fi xating intraocu-lar lenses (IOLs) in patients with absence of capsular support. She will also go over newly available types of presbyopia correcting IOLs. “It is exciting to be discussing all these cut-ting edge technologies and changes,” says Dr. Al-Mohtaseb, as they allow better care and postoperative vision than ever before. •
Master the Anterior SegmentManaging the many presentations of this area can be diffi cult, but this special session course has you covered.
Corneal ulcer diagnosis and management will be a focal
point of tomorrow morning’s course.
SATURDAY: 8:30–10:30am AMPHITHEATER A3
The Symfony IOL is a newer intraocular lens that
allows greater post-op visual independence for
many patients.
Photo: D
erek Cunningham
, OD
, and Walter W
hitley, OD
Time Course Presenter(s) Location
000_sd0318_FRI_final.indd 7000_sd0318_FRI_final.indd 7 2/28/18 3:36 PM2/28/18 3:36 PM

REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
DAILY8
The misunderstanding with amniotic membranes is the perception that “you
only use it on trainwrecks,” says Greg Caldwell, OD, of the bio-logic technology that eye care professionals can actually use for a variety of ocular wound healing purposes. By “trainwrecks,” he’s referring to corneas with severe conditions such as microbial ulcers or chemical burns. While amniotic membranes are highly regarded for their ability to treat these conditions, Dr. Caldwell
hopes this early morning course—“Get Comfortable With Amniotic Membranes in an Hour”—will dispel the myth that they’re limited to severe cases. “Amniotic mem-branes should be in every optom-etrist’s offi ce to rehab the cornea,” he says. Yes, they are useful for severe corneal defects, but they can also be used for conditions as common as dry eye.
In tomorrow morning’s course, Dr. Caldwell will talk about the differences between the two main types of amniotic membranes,
cryopreserved and dehydrated, the pros and cons of each, and how to identify when to use which type. He’ll explain the science behind the biological scaffolding that facilitates cellular adhesion and assists in cell migration and proliferation.
Amniotic membranes—which are derived from the submucosa of the placenta—provide an impres-sive regenerative platform. Their therapeutic capabilities include promoting stem cell expansion, suppressing pain and promoting cellular migration—all while ex-pediting recovery. The technology possesses natural growth factors and optimal scaffolding proper-ties within a complex extracellular matrix that are:
(1) Anti-scarring(2) Anti-angiogenic (3) Anti-infl ammatory That last point is key because, as
Dr. Caldwell’s course will explain, infl ammation is the “hallmark of all ocular surface disease.” If left uncontrolled, ocular infl ammation can lead to chronic pain and ir-ritation, delayed healing and more extensive tissue damage that may cause scarring and, eventually, even threaten the patient’s vision.
In addition to updating attend-ees on the benefi cial properties of amniotic membranes and the conditions they can be used to treat, the lecture will provide an overview of the various products available, tips on inserting and removing each one, a discussion of patient expectations and strategies to help attendees better under-stand the patient’s experience.
“It can be used on a herpes ulcer. It can be used for recurrent corneal erosions,” Dr. Caldwell explains. “This is an awareness lecture and, for those alreadyaware, it’s got tips to help doctors feel more comfortable with the procedure and helps guide them around any pitfalls they might en-counter.” As the procedure is rela-tively new to optometry, and not all states allow its use, it is prudent to be conservative until you gain confi dence and experience
The course will also review how to partner with a lab and a com-pounding pharmacy to develop the autologous serum.
Finally, the course will review the cost of and billing tips for the ProKera (BioTissue), AmbioDisk (IOP Ophthalmics) and BioDOptix (BioD) graft products. •
Get on Board with Amniotic Membranes This overview covers all you can do with this versatile technology.
SATURDAY: 6:30–7:30AM ROOM A313, LEVEL 3
Special Event Benefiting Optometry Cares - The AOA Foundation
SEE THE OPTOMETRY STARS AT SECO 2018SEE THE OPTOMETRY STARS AT SECO 2018
Friday, March 2 | 9:00 PM - MidnightCollege Football Hall of Fame
EYE DOCS OF ROCK
Thank You SponsorsPlus, a special lounge just for
optometry students,
presented by
Special Guest
Performers to be
announced!
Purchase raffle tickets for a chance
to win an iScan system courtesy of
Optovue!
Photos: Nathan Lighthizer, O
D
Amniotic membrane grafts (such as the Prokera Slim shown here) promote
epithelialization, decrease infl ammation and scarring, prevent new blood vessel
growth and improve comfort.
000_sd0318_FRI_final.indd 8000_sd0318_FRI_final.indd 8 2/28/18 1:58 PM2/28/18 1:58 PM

NEW TECHNOLOGIES & TREATMENTS IN
Eye Care
2018
REVIEW OF OPTOMETRY® EDUCATIONAL MEETINGS OF CLINICAL EXCELLENCE
OPTOMETRIC CORNEA, CATARACTAND REFRACTIVE SOCIETY
**Additional CE fees if attending both meetings. Agenda subject to change.See website for details: www.reviewofoptometry.com/SanDiego2018
Administered by
Review of Optometry®*Approval pending
Review of Optometry® partners with Salus University for those ODs who are licensed in states that require university credit
SAN DIEGOAPRIL 26-29, 2018
We invite you to attend a unique joint meeting
held at the San Diego Marriott Del Mar.
Review’s New Technologies & Treatments in Eye Care and
Optometric Cornea, Cataract and Refractive Society’s annual
meetings are combined to provide you with up to 29* COPE CE
credits in one weekend.
San Diego Marriott Del Mar11966 El Camino Real
San Diego, California 92130Phone: 858-523-1700
A limited number of rooms have been
reserved at $165 per night.
Please make reservations with the hotel
directly at 858-523-1700. For group
rate, mention “New Technologies and
Treatments in Eye Care”.
David Friess, OD, FAAOPresident, OCCRS
Paul M. Karpecki, OD, FAAOReview Program Chair
Program Chairs:
Three Ways to RegisterOnline: www.reviewofoptometry.com/sandiego2018Call: 866-658-1772 • E-mail: [email protected]
Convenient opportunities to register for one or both meetings.**
REGISTER ONLINE: WWW.REVIEWOFOPTOMETRY.COM/SANDIEGO2018
Earn up to
29 CE Credits*

10
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
DAILY
FREE CE IN THE PRESENTATION THEATERSIndustry support allows ODs and AOPs to earn credit for free!
Space is limited and participation is on a fi rst-come, fi rst-served
basis. Today’s schedule:
11am–12pm: • Workshop: Sutureless Amniotic Membranes How to Properly
Insert and Remove Them (Katena)
• The Evolution of Lenses – The Importance of Blocking Blue
Light (Essilor
1–3pm: • Cracking The Code: Clinical Case Management & Medical
Record Compliance Part 1
2–3pm: • Blue Light (Essilor)
4–5pm: • Winning the Online Game: Any Practice Can Be #1 Online
(iMatrix)
• Procuring Practice Buyers and Sellers (VSP)
• Practice of the Future (Essilor)
SHOW SPECIALSMany exhibitors are offering special deals. Check out the list in
the mobile app or on page 14.
EXHIBIT HALL IN-BOOTH EVENTSBe sure to visit these companies for special events today:
AcuityPro Software: Showing off a totally redesigned booth,
the company will also be randomly handing out International
Space Station hats while supplies last.
EyeMed Vision Care: Free charging pad for the fi rst 100
attendees to take a survey.
MacuLogix: Offering free copies of the most recent AMD
diagnostic and treatment guidelines, along with patient
management recommendations. Stop by and ask for the AMD Knowledge Base, a
collection of reading
essentials for the diagnosis
and treatment of AMD.
TLC Laser Eye Centers:
TLC will be hosting a
LASIK Wet Lab each
day. Today’s takes place
1–4pm. Attendees can
create a LASIK fl ap on a pig’s eye using the Alcon laser suite,
have Pentacam scans performed on their eyes and learn how to
interpret the results. Lecturers will review pre- and post-op care
protocols for LASIK and PRK. Upon completion, participants can
sign up for a chance to win a Fitbit.
NEW! STUDENT ESCAPE ROOM1pm, 2:45pm, 4:30pmStudents, test your optometry knowledge as you work together
searching the room to fi nd clues, solve riddles and crack codes
to accomplish the goal of escaping within the hour. Three rooms
will be running simultaneously with groups of 10 students each.
LEARNING LOUNGE, POSTERS & GOOGLE TALKSIn this informal educational environment, you can hear from
industry leaders on the latest in exciting trends. Plus, experience
the new Google Talks! Liz Austin from Google shares cutting-
edge strategies for fi nding new patients and growing your
business with Google. You can also fi nd the return of our
multimedia Poster Presentations.
EYESTYLES FASHION SHOW, 11:15–11:45amSee the latest eyewear trends and gain insight on how
showcasing the latest trends in frames can help maximize ROI
and customer experience in your practice. Experience it in the
Focal Point lounge this morning.
THE VIEWSee some of the world’s most exclusive frames in THE VIEW,
SECO’s Luxury Eyewear Pavilion.
EXHIBIT HALL EVENTS FOR FRIDAY, MARCH 2
OPENS: 10:45am CLOSES: 5pm
DAILY10
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
000_sd0318_FRI_final.indd 10000_sd0318_FRI_final.indd 10 2/28/18 1:58 PM2/28/18 1:58 PM

DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
11DAILY
Exhibitor Listing for SECO 2018 (as of February 26, 2018)
Attendees can visit Optometry’s Marketplace at SECO™ for free just by mentioning an exhibiting company they intend to visit during SECO 2018.
EXHIBITOR .............................. Booth EXHIBITOR............................... Booth EXHIBITOR .............................. Booth EXHIBITOR............................... Booth
4ECPs, a Preferred Premier Google Partner ............................1300A&A Optical ..................................1200ABS Smart Mirror ..........................1111ABB Optical Group ...........................332Acuity Pro/VisionScience Software ..1113Akorn .............................................800Alcon ..............................................429Allergan ........................................1220Allied Powers ..................................404Allure Eyewear ................................714American Academy of Optometry ....1725American Academy of Orthokeratology
and Myopia Control .....................1726American Board of Opticianry – National
Contact Lens Examiners ...............1718American Board of Optometry .........1724Applied Medical Systems .................301Art Optical Contact Lens ..................603Article One ....................................1337Aspex Eyewear Group ....................1201Association of Schools and Colleges of
Optometry ....................................127Avalon Eyewear ...............................437Avesis ..........................................1532Baumvision ...................................1137Bausch + Lomb ...............................818Beaver Visitec International ..............737Binocleuses ..................................1330Bio-Tissue ......................................310BlephEx ........................................1500Bruder Healthcare Company .............327Bushnell Outdoor Products .............1431CareCredit ....................................1600CatarActive3 ...................................235Centervue .....................................1619Chadwick Optical ............................209Clearlens ......................................1536ClearVision Optical/BluTech ...........1005Coburn Technologies .......................321Color My World by EyeChroma ..........504Community Low Vision Center ..........131Compulink Business Systems .........1313Contact Lens Spectrum (Pentavision) ..512CooperVision ...................................513Costa Sunglasses ............................627Crystal Practice Management ...........330Demandforce ................................1629Design Eyewear Group ...................1422DGH Technology ..............................320Digital Healthcare Professionals .......313Digital Heat Corporation ...................241Diopsys ..........................................633DM Med Group ..............................1614
Ear Technology Corporation ...........1625Eastern Ophthalmic Supply & Repair ..701EdgePro by GPN Technologies ..........715Edison Optics ................................1436E-Dr. Network/New Era ....................408Energeyes, the Association of Corporate-
Affiliated Optometrists .................1604Eschenbach Optik ..........................1115eSee Acuity...................................1528Essilor Instruments ..........................420Essilor of America ...........................419Eye Designs ....................................921Eyecare Business (Pentavision) ........514EyeCor by Nteon/Nteon Practice
Consultants ..................................506Eyefficient ......................................300EyeMed Vision Care .........................538EyePromise/ZeaVision ......................605Eyes of Faith Optical ......................1412Faniel Eyewear ..............................1328Fashion Optical Displays ..................507Gazal Eyewear ..............................1241Good-Lite .......................................401Hai Laboratories ..............................711Harvest Acuity .................................311Healthpod .......................................704Heidelberg Engineering ..................1505Heine USA.......................................611Hoya Vision Care ...........................1013Icare USA .......................................432i-dealoptics ..................................1427Identity Optical Lab .........................412IDOC ..............................................405iMatrix ................................ 1307, 1533ImprimisRx ...................................1428Innexus by Innereactive ...................308Integra Life Sciences .....................1401Interstate Optical .............................802Invision Magazine ..........................1723J & M Distribution .........................1615Jeunesse Innovations ....................1511Johnson & Johnson Vision..............1019Kasperek USA Optical ....................1405Katena ............................................533Keeler Instruments ........................1101Kentucky College of Optometry .........121Kingdom Eyewear ..........................1228Kio Yamato Optics .........................1340Konan Medical ..............................1207LA Eyeworks .................................1141Lacrivera ........................................609Lafont ............................................812LasikPlus ......................................1522Life Without Color ............................211
Lombart Instrument .........................738Luneau Technology USA (AIT, Briot,
WECO, LPO, Visionix) ............. 424, 426Luxottica Group ...............................621M&S Technologies ...........................414MacuLogix ....................................1515Mad Vision ....................................1139Marco Ophthalmic .........................1029Marcolin USA Eyewear .....................913Maui Jim Sunglasses .......................833MaximEyes by First Insight .............1331MaxiVision (MedOp Health) .............1325Medi Lazer ......................................215Modern Optical International ............500Morel Eyewear ..............................1432My Vision Express ...........................326MyEyeDr .......................................1327National Academy of Opticianry ......1720National Board of Examiners in Optometry ..................................1513National Vision Retail .....................1507National Vision ..............................1304Natural Ophthalmics ........................315NCI Vision Systems ..........................536Nerdwax .........................................245New York Eye ..................................713Nidek ...........................................1215Nouveau .........................................931Nova Southeastern University College of Optometry .................................123NovaBay Pharmaceuticals ................438Novartis Pharmaceuticals .................137Oasis Medical ...............................1214Oculus ............................................836Ocusoft ........................................1109Optical Academy Alliances ...............440Opticwash ......................................339Optikam Tech..................................328Opto Multimedia ..............................400Optometric Architects ......................607Optometric Management (Pentavision) .................................510Optometric Protector Plan ................410Optometry Times (UBM) .................1729Optos ...........................................1301Optovue ........................................1521Orgreen + Goldsmith .....................1240Orion Vision Group .........................1610Ottica Veneta ................................1229OWP USA ......................................1430Passion to Heal, Me to We ................128Patch .............................................645Pharmanex ...................................1310Practice Director EHR ....................1621
Presenta Nova .................................338Professional Eye Care Associates of
America ........................................304Proof Eyewear .................................322Quantel Medical ............................1433Quidel Corporation...........................641Q-Vision Optics ...............................407Reichert .......................................1419Remote Area Medical .....................1737Review of Optometry .....................1411RevolutionEHR.................................411RightEye .........................................220Santinelli International ...................1204ScienceBased Health .....................1414Shire ..............................................501Shwood Eyewear ...........................1426Signet Armorlite ..............................314SingleCare ......................................305Solutionreach ..................................323Southern College of Optometry .......1210State Optical Co. ...........................1321Studio Optyx .................................1437Sun Ophthalmics .............................201Suppleyes .......................................309TearScience ....................................433TelScreen .......................................318The Gideons International ................739The Lens Butler ...............................205The McGee Group ............................827TLC Laser Eye Centers .....................537Topcon Medical Systems .................727US Optical ....................................1501UAB School of Optometry .................120Ultra Palm Optical (Cazal, Caviar, Goliath) ......................................1329United States Air Force ....................129Uppercut Consulting ........................303Villa Eyewear ................................1338Vital Tears ......................................838Vmax Vision ....................................601Volk Optical ..................................1103VOSH International ........................1727VSI, a division of Enhanced Medical
Services .....................................1525VSP Global/VSP Optics Group/Eyefinity/
Marchon/Altair ..............................805Walman Instruments ........................927Walman Optical .............................1026Wal-Mart Health and Wellness ........1212Weave ............................................639Williams Group ................................706Wolters Kluwer ................................543X-Cel Specialty Contacts ................1032Zeiss ..............................................700
000_sd0318_FRI_final.indd 11000_sd0318_FRI_final.indd 11 2/28/18 1:59 PM2/28/18 1:59 PM
12
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
ocal Point Loung :Fashio
Presentation Theater #1
Learning Lounge
Exhibits InfoBooth
PosterPresentations
SECO 20199
1005
20'
30'
ClearVisionOptical /BluTech
1013
20'
20'
HOYAVisionCare
1019
40'
40'
Johnson &Johnson
Vision
1026
30'
Wal
man
1029
20'
30'
MARCOOphthalmic 1032
X-CelSpeci10320
1101
KeelerInstru
1103
1109
OCuSOFT
1111
A.B.S.Smart
1113
AcuityPro /
1115
Eschenbach
1200
20'
A&
A O
ptic
al
1201
30'
Asp
ex E
yew
ear
Gro
up0'
1204
Santitinelli
1207
Kon
anM
edic
al
1210
Southern
1212
Wal-Mart
1214
OASIS
1215
NidekInc.
1220
30'
20'
Allergan
1300
20'
4ecp
s, A
Pref
erre
d
1301
20'
20'
Optos,Inc.
1304
30'
Nat
iona
l Vis
ion,
Inc.
1307
20'
20'
iMatrix
1310
1313
Com
pulin
kB
usin
ess
1321
SEC
OIn
tern
a1325
MaxiVision
1327
MyEyeDr
1329
UltraPalm
1331
20'
Max
imEy
esby
Firs
t
1337
SECOIntern
1401
Integra Life
1405
20'
20'
KasperekUSA Optical
1411
20'
30'
Review ofOptometry
1412
Eyesof
1414
ScienceBas
1419
Rei
cher
t, In
c
1422
Des
ign
Eyew
ear
1426
Shwood
1427
1428
ImprimisR
1430
OWPUSA
1431
Bushnell
1432
MorelEyew143241433
Quantel
1436
Edison
1437
STUDIO
1441
51'2''Remote Area Medical
1500
BlephEx
1501
U.S.Optica1 01
1505
Heidelberg5055
1507
National
1511
Jeunesse
1513
National
1515
MacuLogix
1518
Visioneering
1520
Ophthalmic
1521
21'2''Optovue
1522
1525
VSI, adivision ofEnhanced
1528
1530
FoxFire
1532
Avesis
1533
1536
CLEARLEN
1600
CareCredit
1604
20'
Ener
geye
s,Th
e
1610
OrionVision
1612PatientPop6122
1614
DMMed
1615
J & MDistri
1619
Centervue
1621
Practice
1625
EarTechn
1627
1629
Demandfor
17141715
1718
American
1719
AirForce
1720
National
1721
ArmedForce
1723
INVISION
1724
American
1725
American
1726
American
1727
VOSHIntern
1728
FirstVision
1729
Optometry17299
913
23'
20'
MarcolinU.S.A.
Eyewear Corp.
921
23'
20'
Eye Designs,LLC
927
20'
Wal
man
Inst
rum
ent
931
20'
Nou
veau
1129
1131
1133
FACEA
1137
Baumvision
1139
MADVision
1141
L.A.EYEW
1228
Kingdom
1229
OtticaVenet
1240
Orgreen +
1241
GazalEyew12412
1328
FanielEyewe13283
1330
Binocleuses
1338
VillaEyewe
1340
KioYamat
SECO 2019Find out about our move to New Orleans for next year’s conference. Register today! Prizes will be given out, too—ask for details at the booth!
DAILY12
Today’s Free CE in Theater 1 11am–12pm: Workshop: Sutureless Amniotic Membranes How to Properly Insert and Remove Them (Katena)
1–3pm: Cracking The Code: Clinical Case Management & Medical Record Compliance Part 1
4–5pm: Winning the Online Game: Any Practice Can Be #1 Online (iMatrix)
ENTRANC
E X H I B I T H A L L M A P A N
Industry’s PerspectiveStop by the Learning Lounge to hear industry executives discuss trends in eye care.
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
000_sd0318_FRI_final.indd 12000_sd0318_FRI_final.indd 12 2/28/18 1:59 PM2/28/18 1:59 PM

REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
DAILY
ounge::o
EscapeRoom Adventure
9137
20'
20'
NovartisPharmaceuti
cals
201
20'Su
nO
phth
alm
ic20
'2
205
TheLens
209
Chadwick
211
LifeWitho
213
TalentCare
215
MediLazer
219
Miraflex
220
RightEye200221
Kentucky21
222
Global expo
223
UABScho
226
Adit
227
NovaSouth
228
Passion to
229
United
230
Associatio
231
Communit
233
235
CatarActiv
241
245
Nerdwax
300
20'
Eyef
ficie
nt,
LLC
301
Applied
303
Uppercut
304
Professional
305
SingleCare
308
Innexus by308309
Suppleyes,
3090
310
20'
Bio
-Tis
sue
311
Harvest
313
DigitalHealth
314
SignetArmor
315
Natural
318
TelScreen
320
DGHTechn
321
Coburn
322
ProofEyewe
323
20'
Solu
tionr
each
326
MyVision
327
Bruder
328
OPTIKAM
330
Crystal
332
ABBOptica3323
338339
opticwash
344
400
20'OPT
OM
ultim
edia
401
20'
Goo
d-Li
te
404
AlliedPower
405
IDOC407
Patch408
E-dr.Netwo
410
SECOIntern
411
30'
Rev
olut
ionE
HR
412
Identity22
414
M&STechn
419
Essilor ofAmerica
420
20'Es
silo
rIn
stru
men
ts
424
Luneau
426
429
Alcon
432433
20'TearScience
437
Avalon
438
NovaBay
439
440
21'2''Optical
441
Wolters
500
20'Mod
ern
Opt
ical
0'
501
20'
20'
Shire
504
ColorMy044
506
EyeCOR by
507
20'
20'
FashionOptical
Displays
510
Optometri
512
Contact513
CooperVision 514
Eyecare
533
20'Katena
536
NCIVision537
20'20
'TLC Laser
Eye Centers 538
20'
EyeM
edVi
sion
Car
e
601
VmaxVision
603
ArtOptica
605
EyePromise/
607
Optometric
609
Lacrivera
611
621
31'4''
20'
LuxotticaGroup
627
20'
20'
CostaSunglasse
s
633
21'2''Diopsys
639
Weave
641
QuidelCorpo641
700
20'Ze
iss
701
East
ern
Oph
thal
mic 704
Healthpod040
706
Williams
711
HAILabo
713
NewYork
714
AllureEyewe
715
EDGEPro by
727
20'
40'
TopconMedicalSystems
737
Beaver
738
20'
Lom
bart
Inst
rum
ent
739
TheGideo
800
Akorn, Inc.
802
805
20'
60'
VSP Global /VSP Optics
Group /Eyefinity /Marchon /
Altair 812
20'La
font
818
40'
30'
Bausch +Lomb
827
20'
20'
TheMcGeeGroup
833
20'Maui Jim
836
Oculus
838
VitalTears
2020
20
13
Today’s Free CE in Theater 211am–12pm: The Evolution of Lenses – The Importance of Blocking Blue Light (Essilor)
2–3pm: Blue Light (Essilor)
4–5pm: Procuring Practice Buyers and Sellers (VSP)
NCE
A N D S P E C I A L E V E N T S
Today’s Free CE in Theater 34–5pm: Practice of the Future (Essilor)
Escape Rooms Students, test your optometry knowledge as you work together searching the room to fi nd clues, solve riddles and crack codes within one hour. Three rooms will be running simultaneously with groups of 10 students each.
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
EyeStyles Fashion ShowToday at 11:15am, see the latest eyewear trends and gain insight on how showcasing the latest trends in frames can help maximize ROI and customer experience in your practice.
000_sd0318_FRI_final.indd 13000_sd0318_FRI_final.indd 13 2/28/18 1:59 PM2/28/18 1:59 PM

Ear Technology CorporationBooth 1625
New-to-the-industry hearing products designed for the optical channel include TuneAmp, which is affordable, easy to use and easy to sell. TuneAmp is already sold by many opticians in Europe, but SECO is the fi rst showcase for our products in the US. Great opportunity to add revenue and profi t to the practice. Stop by and let us show you how it easy it can be!
Eyes of Faith OpticalBooth 1412
New styles: Integrity and Trust (both available in ophthalmic and sun). New colors: hickory smoke (for the Honor line), scarlet (for the Beauty line), choc-full-of-color (for the Alive line).
Villa Eyewear Booth 1388
The Blackfi n Spring/Summer 2018 collection includes the new Bonita Bay, Ocean Ridge, Elliott Key and Marrowstone frames.
CooperVisionBooth 513
CooperVision Introduces MyDay toric daily dispos-able contact lenses that incorporate the Biofi nity toric design and material, offering the healthy advan-tages of silicone hydrogel, uncompromised comfort and handling, and excellent lens stability and visual acuity.
EyeChromaBooth 504
EyeChroma is a brand new company. SECO is our fi rst trade show. We are bringing the fi rst profes-sional kit of color-enhancing glasses to help color-blind patients see a much more vibrant world The kit includes our fi ve most successful lens coatings proven to be successful for the vast majority of color blind patients.
ImprimisRx Booth 1428
Preservative-free cyclosporine 0.1%/chondroitin sulfate compounded ophthalmic emulsion is now available for only $99.99 for your patient’s fi rst three bottles. No prior authorizations, no coupons and no pharmacy callbacks to deal with.
LacriveraBooth 609
The new FlexFit punctal occluder by Lacrivera offers a fresh approach in bringing greater value to your dry eye practice. The FlexFit nose technol-ogy, designed to collapse when inserted, allows for simple sizing, easy insertion, superior retention and excellent patient comfort. Available in four sizes and in sterile preloaded or non-sterile bulk packages.
MarcoBooth 1029
Visit Marco to see our newest products: TS-310 refractive tabletop workstation, LM-7 Series lens-meters and the new Ultra M Series slit lamps.
Kingdom EyewearBooth 1228
We are pleased to debut the Casanova Occhiali, Taxi and Dolce Vita collections of hand-enameled and cloisonné eyewear designs for the fi rst time at SECO, only in the VIEW.
Acuity Pro SoftwareBooth 1113
Offering several specials on software, including $100 off Acuity Pro Version 9 license key ($995) or $50 off Version 9 upgrade licenses. Included is a USB Acuity Pro license key and installation, remote control/receiver, mouse pad, HOTV/hot key card and pair of red/blue glasses. You can also place orders directly from the website and take advantage of the show specials by using coupon codes UPGRADE2018 or LICENSE2018.
eSee Acuity Booth 1528
Stop by booth 1528 to enter a raffl e for a free all-in-one digital acuity chart. Just drop on by with no purchase or gimmicks!
Eschenbach Optik Booth 1115
Buy three, get one free—a $1,595 value! Our new Visolux Digital XL FHD is an advanced portable video magnifi er that features a 12-inch touch screen display. With magnifi cation from 2x to 22x, dynamic line scrolling, FHD camera and HDMI and USB ports, it’s ideal for patients who need extra magnifi cation.
EyeMed Vision Care Booth 538
Stop by booth 538 to see for yourself how being part of our net-work leads to profi t potential and loyalty from EyeMed members. On Thursday from 1–4pm, speak one-on-one with EyeMed’s president Lukas Ruecker.
Eyes of Faith OpticalBooth 1412
Receive a 30% discount on your 30-piece order and keep your boards refreshed. Fifteen ready-for-spring styles ship in March, 15 sizzling styles for summer ship in May.
Kasperek USA OpticalBooth 1405
Leave the booth with your premium in hand! Mix and match from the following collections: Glen Lane, Pure-T, Pure-T Max, Camelot, Pure Color, Cc: Two is One or Pure Comfort. Five frames earns you a $100 Visa gift card. For 17 frames, receive an iPad or Apple Watch. And pick any 28 frames to receive an iPad Pro.
LacriveraBooth 609
• FlexFit punctal plugs: sterile preloaded $49/pair & nonsterile bulk $265/10 pair box.• VeraPlug punctal plugs: sterile preloaded $40/pair & nonsterile bulk $250/10 pair box.• Vera90 Extended Wear (60 to 180 days): $100/10 pair box. • VeraC7 collagen plugs: $45/60 plugs.
Lombart InstrumentBooth 738
• Haag-Streit BI 900 slit lamp $11,599 (was $13,691) and free BC/BD tonometer!• Haag-Streit Octopus perimeter: up to $15,000 trade-in.• Topcon 3D OCT-1 Maestro: Up to $15,000 trade-in, free Lombart table and large table top, free remote installation of review software, free ongoing remote training. Limited offer: fi ve-year leasing special $1,099/mo for 60 months, includes fi ve-year service coverage.• Topcon Aladdin HW 3.0 biometer: up to $12,500 trade-in, $2,000 mail-in rebate, free CAS training ($1,500 value), free Lombart table and small top, free IOL confi guration setup.• Reichert Ocular Response Analyzer G3: 0% fi nancing for 24 months; monthly payment $677.• Lane promotions (incl. 2nd-year warranty): premium lane pack-age $28,990 ($3,277 savings), digital refraction package $29,485 ($4,595 savings), value lane package $13,995 ($2,585 savings).
Natural OphthalmicsBooth 315
Ongoing education plus 15% show discount promo on all orders. Natural products for dry eye and allergy will increase revenue, bring referrals to your offi ce and meet patients’ needs.
MaximEyes, by First Insight Booth 1331
Attend a 10-minute MaximEyes EHR demo in Booth 1331 and get a $10 Starbucks gift card. Must be a practicing doctor or practice decision-maker.
Modern Optical International Booth 500
Buy 20 frames, get 20 free! Modern Optical is family owned and has been a proud supporter of independent eye care since 1974. Restrictions apply on free frames.
Professional Eye Care Associates of America Booth 304
Promotion for new members: join by March 15, 2018 and your next three months of PECAA membership are free!
New Product Launches
Exhibit Hall Show Specials
DAILY14
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
000_sd0318_FRI_final.indd 14000_sd0318_FRI_final.indd 14 2/28/18 2:00 PM2/28/18 2:00 PM

15DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
The fi elds of low vision and vision rehabilitation have remained a misunderstood
niche for years. For patients, the term low vision opens a Pandora’s box of emotions, send-ing fear, confusion and even panic into the exam room; for optometrists, the extensive time investment and management pro-cess of low vision patients is often daunting.
While ODs seek comfort in know-ing they can refer these cases to the nearest low vision specialist, that
luxury cannot last. The growing num-ber of those in need of care from such a small number of specialists is simply unsustainable.
In his course, “Low Vision Care for the Primary Care Practitioner,” Scott Gartner, OD,
provides a glimpse into the current state of low vision care and what optometry needs to do to ensure all Americans in need of low vision exams, management and assistive devices receive them—their daily independence often depends on it.
“I want to communicate how and when the primary care optometrist can perform many of the basic low vision needs, like prescribing higher power reading lenses and a few special low vision devices, allowing a patient to function and perform their daily living tasks better,” says Dr. Gartner.
During the course, he will walk through the array of testing nec-essary to choose the best device for correction, and will discuss the abundance of new technolo-gies available for everyday use. He will also touch on new clini-cal procedures available for some outstanding cases. He says he hopes it becomes easier to identify those who are in need of moderate man-agement, as opposed to those who should be referred to a specialist.
This past year, the AOA released several articles and statements that serve to emphasize the importance of integrating vision rehabilitation into your practice.
“That understanding is a big milestone for the entire eye care fi eld,” says Dr. Gartner. “It reveals
that low vision and vision rehabili-tation should be on every doctor’s mind when taking a patient’s his-tory.”
His lecture touches on the ques-tions that all ODs should be asking patients—and how to interpret the answers.
“I never want to hear that patients with macular degeneration or glaucoma are being told that
there is nothing left to do to save their eyesight, because it’s not true,” says Dr. Gartner. “For low vision specialists, those diagnoses, for example, are just the starting point for low vision rehabilitation.”
Knowing what to ask, what to look for, when to refer and to whom are skills all ODs should learn, refi ne and regularly integrate into their practices. •
High Hopes for Low VisionHold up your end of the bargain for these patients.
SATURDAY: 3:30–5:30pm ROOM A304, LEVEL 3
Andrew Bartlett, MDAlabama Vision Center, Birmingham, Ala
In his SECO 2018 Special Session, “Cornea Update,” Dr. Bartlett will
be teaming up with Joseph Shovlin, OD, to give attendees a refresher
course on all things cornea. “I’m hopeful attendees will take away the
signifi cant advancements that modern corneal transplantation techniques
can offer,” says Dr. Bartlett. “I also promise to do my best to keep people
from falling asleep and to be as entertaining as the SECO ethics commit-
tee allows.”
Dr. Bartlett comes from a family legacy of medical vision achievements
and currently practices at the Alabama Vision Center in Birmingham, Ala.
After receiving his undergraduate degree from the University of Alabama,
he attended the University of Alabama at Birmingham School of Medicine.
For his ophthalmology residency, Dr. Bartlett went to Texas Tech
University. He also completed a Cornea and External Disease fellowship
at Eye Consultants of Atlanta.
His specialties include cataract surgery, LASIK and corneal transplan-
tation (specifi cally, Descemet’s membrane endothelial keratoplasty and
Descemet’s stripping automated endothelial keratoplasty).
SPEAKER SPOTLIGHT
Dr. Bartlett’s SECO course schedule includes:
• Cornea UpdateSunday 9–11am, Amphitheater A3
• View the complete Schedule of Events, explore all of the offered courses and get a detailed map of the exhibit hall.
• Keep your pulse on the most popular sessions and events by accessing the Activity Feed which will highlight photos, ratings, comments and more.
• Receive announcements and obtain the most up-to-date event information.
• Get your course handouts at your fi ngertips.
• Tap into your competitive side! Earn points and achievements to win prizes.
WHY USE THE SECO 2018 MOBILE APP?
Visit the Apple App
Store or Google Play
store and search for
SECO 2018.
“I never want to hear
that patients with
macular degeneration
or glaucoma are being
told that there is nothing
left to do to save their
eyesight, because it’s not
true,” says Dr. Gartner.
000_sd0318_FRI_final.indd 15000_sd0318_FRI_final.indd 15 2/28/18 2:00 PM2/28/18 2:00 PM

DAILY16
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
NEW TECHNOLOGIES & TREATMENTS IN
Eye Care &&
E
2018
REVIEW OF OPTOMETRY® EDUCATIONAL MEETINGS OF CLINICAL EXCELLENCE
NashvilleApril 6-8, 2018
Paul Karpecki, OD, FAAO Program Chair
Eric Schmidt, OD, FAAO
Doug Devries, OD
Alan Kabat, OD, FAAO
Nashville Marriott at Vanderbilt University2555 West End Avenue Nashville, TN 37203 Reservations: 615-321-1300 DISCOUNTED RATE: $249 per night
Program Faculty
Earn up to
19 CE Credits*
Administered by
Review of Optometry®*Approval pending
Review of Optometry® partners with Salus University for those ODs who are licensed in states that require university credit.
THREE WAYS TO REGISTER online: www.reviewofoptometry.com/nashville2018 email: [email protected] phone: 1-866-658-1772Registration cost: $495
See event website for agenda and up-to-date information.
Continuing Education with Examination (CEE/TQ) Courses at SECO 2018Date Start End Course # Title COPE
Friday, March 2 1:30pm 3:30pm 139 OCT in Glaucoma - Green Isn't Always Clean 20-609693
Friday, March 2 1:30pm 3:30pm 141 Referral Center Grand Rounds 20-609695
Friday, March 2 1:30pm 3:30pm 143 AMD - Current Concepts and Future Directions 20-637056
Friday, March 2 5pm 7pm 146 Narrow Minded: The Management of Angle Closure 20-610353
Friday, March 2 5pm 7pm 149 Modern Day Diabetes 20-609703
Friday, March 2 5pm 7pm 515 Seeing Stars: Concussions in Sports 20-609717
Saturday, March 3 6:30am 8:30am 154 The Pressure is On: Managing Challenging Cases in Glaucoma 20-638342
Saturday, March 3 6:30am 8:30am 156 "What's Brewing?" All About Dry Eye & MGD 20-609705
Saturday, March 3 12:30pm 2:30pm 159 Get Going with Glaucoma 20-638344
Saturday, March 3 12:30pm 2:30pm 161 Neuro-Ophthamology of MS 20-609699
Saturday, March 3 12:30pm 2:30pm 162 New Drugs and Bugs 2018 20-609697
Saturday, March 3 3:30pm 5:30pm 164 Glaucoma Update: New Tools and Treatment Options 20-609709
Saturday, March 3 3:30pm 5:30pm 166 Anterior Segment Surgery Update 20-638460
Saturday, March 3 3:30pm 5:30pm 169 From Outdated to Updated: A Review of Key Clinical Trials in Eyecare 20-609713
Saturday, March 3 5:30pm 7:30pm 529 Digging Into Dry Eye 20-609723
Sunday, March 4 12pm 2pm 530 Lunch Course: How Do You Mend a Broken Cornea? 20-609725
000_sd0318_FRI_final.indd 16000_sd0318_FRI_final.indd 16 2/28/18 2:00 PM2/28/18 2:00 PM

17DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Prepare Your Practice for Red EyeDetermining if a case is urgent and knowing what to do is imperative.
FRIDAY: 1–2pm ROOM A403, LEVEL 3
If your staff seems to panic every time a red eye emergency calls the offi ce, this Friday afternoon course
will help ease everyone’s minds. In “Red Eye Emergencies: What Do You Do?” Kris Kerestan-Garbig, OD, of Garbig Family Eye Care in Wilder, KY, will teach attendees about the crucial role front offi ce staff and optometric assistants play in managing red eye-related emer-gencies. Additionally, she will go over the most common presenting signs, symptoms, causes and treat-ment options for red eye cases.
Dr. Kerestan-Garbig will start things off by going over how to properly train your staff to begin these evaluations during the initial phone call. Here, she will go over some common things patients will
say, including “I’m afraid I have pink eye,” and “My eyes are so red and itchy, I can hardly stop rubbing them.”
Next, she will list what to look for in urgent cases that need immedi-ate attention and differentiate them
from cases that can wait. According to Dr. Kerestan-Garbig, must-see patients include those with redness associated with:
• Sudden or severe pain and discomfort
• Bleeding in or around the eye• Ocular trauma from:
– Sports injury– Auto accident– Blow to the eye– Fingernail scratch– Paper cut– Curling iron burn– Chemical burn
• Foreign body in the eye• Extreme discomfort and sensi-
tivity to light• Sudden change in vision or loss
of vision• Copious matter or discharge
Non-urgent cases, meanwhile, include redness not associated with ocular trauma or foreign body injury, involve mild pain or discom-fort that has been present for several days to a week, have no bleeding and little to no light sensitivity, change in vision or discharge.
Beyond that, Dr. Kerestan-Garbig will cover the signs, symptoms and treatment of many of the most com-mon red eye lid conditions, including internal and external hordeolum, chalazion, blepharitis, meibomiani-tis, trichiasis and eye lid trauma.
To fi nish things up, Dr. Kerestan-Garbig will bring things full circle with a quiz for attendees. Here, participants must identify a number of cases based on clinical images and the list of associated symptoms. •
After attending this course, blepharitis
mangement will be a breeze.
FRIDAY: 5–7pm ROOM A311, LEVEL 3
Caring for Her EyesLearn about the ocular differences that may affect the care of female patients.
Tonight, Tammy Than, OD, Louise Sclafani, OD, and Caroline Pate, OD, will teach
attendees about sex-related differenc-es in patients’ ocular structures and functions in their lecture “Through the Eyes of Women: Caring for the Female Patient.”
The development and severity of many ophthalmic conditions can vary between sexes, ranging from ocular surface disease to optic neuropathies, the presenters say. To help attendees better prepare for this, the presenters will go over the specifi c ocular needs of the female patient at different life stages—all the while placing empha-sis on the diagnosis and management.
First up, Dr. Sclafani will begin with basic statistical differences be-tween female and male eyes, as well as some conditions women common-
ly present with, including macular holes, Graves’ disease, myasthenia gravis, rheumatoid arthritis, systemic lupus erythematosus, Sjögren’s syn-drome and rosacea.
After this, she will touch on some complications that could affect this patient population. Eating disor-ders and ocular complications such as episcleral capillary aneurysms, subconjunctival hemorrhages, night photosensitivity and decreased tear production are all issues to consider here, and Dr. Sclafani will go over each in detail.
Next, Dr. Pate will address how to best care for pregnant patients. Top-ics pertaining to this patient popula-tion will include corneal changes, dry eye, refractive changes, intraocular pressure, optic nerves, central serous retinopathy, hypertension, pre-
eclampsia and diabetes. Dr. Pate will cover what to look for in these cases and how to approach treatment before wrap-ping things up with some case examples.
The discussion will then shift back to Dr. Sclafani, who’ll address hormonal infl uences on the glaucoma popula-tion. This section will start off with several case examples leading into key consid-erations to answer the question, “Is there a difference in the prevalence of glaucoma between men and women?” To get to an answer, Dr. Sclafani will cover glaucoma and pregnancy, the protective role of endogenous estrogen, exogenous hor-
mones and the maturing patient. The session will conclude with a
talk on systemic medications with oc-ular side effects and how they affect female patients. Here, the presenters will discuss the possible ocular side effects of drugs such as hydroxychlo-roquine/chloroquine, topiramate, tamoxifen and more. •
Sex can infl uence the severity of various ocular
conditions. Tonight’s presenters will let you in on
the etiology of this patient’s ocular concern.
000_sd0318_FRI_final.indd 17000_sd0318_FRI_final.indd 17 2/28/18 2:01 PM2/28/18 2:01 PM

DAILY18
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Head-borne Low Vision Devices6:30–7:30am, room A304
This course provides an overview of the newest low vision technology for head born display devices which enable the legally blind to actually see and/or hear their visual world. These devices empower individuals with various eye conditions to become more independent as they engage in their various activities of daily living. The benefi ts and disadvantages of each will be discussed. Case studies will be used to demonstrate the device including patient videos. Scott Gartner, OD
Vision Therapy: The Top 10 Tools in Action6:30–7:30am, room A316
Vision therapy has the power to change a patient’s life for the better. Vision therapy can be used to treat issues with binocular vision, accommodative, strabismus, amblyopia and acquired brain injury successfully. While there are upwards of 200+ therapy activities, this lecture will focus on the most common, the top 10. Marc Taub, OD
Get Comfortable with Amniotic Membranes in an Hour6:30–7:30am, room A313
In offi ce and sutureless amniotic membrane (AM) is emerging as an excellent alternative due to promising clinical outcomes to treat a variety of ocular surface conditions rapidly and effectively. This course will review what is an amniotic membrane, the various types of AMs, clinical applications, patient experience, insertion and removal.Gregory Caldwell, OD
Creative Techniques for Finding Your Next New Team Member6:30–7:30am, room A315
When adding to your team it is more important to determine if the new addition will fi t into the offi ce culture than for them to have optometric skills. How do you fi nd the best candidate for the position? Where do you fi nd the best candidate for the position available in your offi ce? This course will help you locate hire and keep the best person for your establishment. Carole Burns, OD
All About Dry Eye & MGD6:30–8:30am, room A312
We hear a lot about the new “disruptive” technology. Does disruptive equal better? Some topics discussed: meibography, intranasal stimulation, tear osmolarity, risk assessment. DEWS II: disruptive or disrupting? Milton Hom, OD
What’s Brewing? CoursesSATURDAY SATURDAY: 8–9am ROOM A403, LEVEL 4
Pediatrics PearlsKids can be tricky to examine and treat. This session will give advice you can integrate today.
Not every OD is used to a squirming, curious six-year-old in their chair. So, when a pediatric patient walks through the door, how can you be prepared? Katherine K. Weise, OD, director of pediatric optometry
service at the University of Alabama at Birmingham, will provide Saturday morning’s attendees with a roadmap for success with these patients.
To begin her 8am lecture, “I’ve Got a Kid In My Chair…Now What?” Dr. Weise will discuss the main differences between an adult and pediatric visit, starting with techniques on taking the history. Unlike an adult patient, kids should generally follow a developmental curve, and abnormal development is a red fl ag. Other pediatric-specifi c history questions include prenatal, delivery and perinatal risk factors, family and school placement and guardianship. Each one of these can impact the child’s visual development, and Dr. Weise will share how to record the history and sleuth out what is at play.
Children may not have an extensive history but, Dr. Weise says, they won’t sit still for long, so the trick is getting to the point quickly.
Dr. Weise will then delve into conditions more common in the pediatric population that might be infl uencing any suspicious fi ndings. Cerebral palsy, for example, has a high rate of secondary eye problems, according to Dr. Weise. Other developmental delays, such as Down syndrome, often have asso-ciated eye signs, including poor accommodation, eye lid abnormalities, retinal disorders, optic atrophy and media opacities.
Finally, with the history out of the way, Dr. Weise will turn her attention to testing. She will cover visual acuity, alignment, strabismus screening with both an ophthalmoscope and with a cover test, stereo testing, pupil testing, extra-ocular muscles and confrontation visual fi elds—all with a pediatric twist.
For fundus exams, Dr. Weise doesn’t mess around. “If you go to a doctor who doesn’t use dilating drops on kids, you need to choose another doc-tor,” she emphasizes. Of course, you should consider skipping it if the drops will harm the child (i.e., subluxated lens, narrow angles or systemic or neuro condition that would contraindicate drops); if the child is tired and would per-form better when fresh; or if parents refuse. For the last one, it’s the clinician’s job to convince them with education, according to Dr. Weise.
No pediatric discussion is complete without a refresher on myopia, and Dr. Weise will spend a few minutes discussing myopia risk factors, prevalence and control options. She will wrap up the session with a brief look at an OD’s worst nightmare: pediatric ocular emergencies. Attendees will walk away with a comprehensive understanding of how to take a pediatric history, what to look out for, and how to handle the most common pediatric conditions. •
A child in the chair can be a real challenge. For one, they rarely stop moving.
Dr. Weise will share some tips on getting a good look at this patient’s eyes
even as he squirms and fi dgets.
000_sd0318_FRI_final.indd 18000_sd0318_FRI_final.indd 18 2/28/18 2:35 PM2/28/18 2:35 PM

19DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Published in partnership with Allergan.
SECO CHAMPION SPOTLIGHT
© 2018 Allergan. All rights reserved. All trademarks are the property of their respective owners. AOT72080_v2 01/18 180013
000_sd0318_FRI_final.indd 19000_sd0318_FRI_final.indd 19 2/28/18 2:41 PM2/28/18 2:41 PM

Orlando, FloridaMay 17-20, 2018
Join Review of Optometry’s New Technologies & Treatments in Eye CareMay 17-20, 2018 in Orlando at Disney’s Yacht & Beach Club. Earn up to 18* COPE CE credits including interactive workshops!**
TQ/CEE approval is pending for optometrists licensed in Florida or other states requiring “Transcript Quality” courses for re-licensure. Please see agenda on event website for specifi c courses.
EARLY BIRD SPECIAL: $495
Registration cost: $595 after March 23, 2018.
Get your discounted park tickets by Friday, March 9 th.
DISNEY’S YACHT & BEACH CLUB1700 Epcot Resorts Boulevard
Orlando, Florida 32830Phone: 407-934-7000
See website for updated hotel accommodations.
NEW TECHNOLOGIES & TREATMENTS IN
Eye Care &
2018
REVIEW OF OPTOMETRY® EDUCATIONAL MEETINGS OF CLINICAL EXCELLENCE
Paul Karpecki, OD, FAAOProgram Chair
Douglas Devries, OD Mark Dunbar, OD, FAAO Murray Fingeret, OD, FAAO
FACULTY
g
3 3 WAWAYS TO REGISTERYS TO REGISTERonline: www.reviewofoptometry.com/Orlando2018
email: [email protected] | phone: 866-658-1772
Earn up to
18 CE Credits*
**Separate registration required. Review of Optometry® partners with Salus University for those ODs who are licensed in states that require university credit. See event website for complete details.
Administered by
Review of Optometry® *Approval pending

21DAILY
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
escalation of a strong steroid, periocular injection, vitreal steroid implants and, for severe cases, im-mune modulators. “When Humira was fi rst approved for uvieitis, everyone was excited and wonder-ing if they should add it to their common therapy,” he said. “But we shouldn’t. It’s a very powerful drug, and should only be for severe cases. It comes with a lot of side effects.”
Clinicians can also consider nonsteroidal anti-infl ammatory drugs (NSAIDs), which research now shows may be useful for some recurrent acute anterior uveitis cases, he said.
Dr. Bronner concluded the treat-ment portion of the lecture noting three common treatment errors to avoid: “not using cycloplegics in anterior disease, not fully control-ling infl ammation and being impa-tient with steroid taper,” he said. “These will get you into trouble.”
Diagnostic TroubleWhile treatment is straightforward,
Dr. Bronner said, diagnosing is not. “Really, you need to rely on the intersection between the clinical picture and patient setting,” he said. “Labs just aren’t sensitive enough.” On the other hand, the patient’s age, sex, race and other medical diagnoses are crucial to understanding their uveitis presen-tation and can go a long way to whittling down the differential list to make testing more useful.
“Uveitis can present with a laundry list of clinical fi ndings,” Dr. Bronner added. “Not all fi ndings present with each etiology. Knowing what is common for each etiology is the key to honing the differential.”
Differentials GaloreDr. Bronner then spent the second half of the lecture running through those many etiologies, careful to include the usual clinical fi ndings.
Everything from juvenile idiopathic arthritis, Behcet’s disease, herpetic disease and postoperative retained lens fragments to sarcoidosis tattoos
and tuberculosis are all on the uveitis differential list. Dr. Bronner helped attendees get through the material by providing clinical pearls after each etiology. He concluded the lecture with an etiology “that’s mostly discussed as a curiosity, but it’s not all that uncommon,” he said. He sees as many as one patient a year with Fuchs’ heterochromic iridocyclitis—
and he can’t treat them with steroids as you would a usual uveitis patient. “You have to treat the hypertension here, and then the cataract as soon as it forms.”
Dr. Bronner provided a fi nal reminder before dismissing the lecture: “Don’t rely on labs—the clinical picture and patient setting are more helpful every time.” •
All You Need to Know About Uveitis
NSAIDs in Uveitis Treatment For clinicians looking for a therapy that bridges the gap between peri-ocular agents and long-term immune modulators, research suggests oral nonsteroidal anti-infl ammatory drugs (NSAIDs) may be surprisingly useful. Although NSAIDs have never been a part of the uveitis treatment protocol, Dr. Bronner discussed a small study from Massachusetts Eye and Ear that showed a reduction in uveitis episode recurrences by more than 63% in 44 patients with recurrent acute anterior uveitis.
The patients were on the maximum dose for each specifi c NSAID trialed for a at least six to 12 months prior to showing any reduction, and periocu-lar steroid was used to control acute fl are-ups. The researchers preferred COX selective celecoxib, unless cost was an issue for the patient.
While this is an off-label use, it may actually be very useful in optometric practice, Dr. Bronner said. “Of course, as with all long-term medications, controversy still exists, given the risk and reward balance of long-term NSAIDs in these eyes.”
Continued from Page 1
OD and MD Experts Address How to ‘Gear Up for Glaucoma’Continued from Page 1
Knowing that peak IOPs do not occur between the hours of 9am and 5pm, optometrists can now tap into possible missing links that could radically alter the management approach, the speakers said.
Dr. Thimons, who has rented the home tonom-eter to more than 45 of his patients since its FDA approval last spring, has found the data output for late evening and early morning pressure read-ings to be fascinating. “I’d say 30% to 40% of these patients have a 5mm Hg difference between my highest IOP recording and what they found off-offi ce hours from the device,” he said. Dr. Noecker said he does receive the occasional late-night call from patients who panic after seeing a high reading in the middle of the night; however, he said this can be avoided by simply engaging in a few extra minutes of patient education around IOP results.
Hysteresis Hysteria For the last fi ve years, Drs. Thimons and Noecker
have been using the Ocular Response Analyzer (Reichert) to assess corneal hysteresis to further inform the direction for glaucoma management. “This provides the type of information that really yields high return in looking at prediction for progression within existent glaucoma patients,” said Dr. Thimons.
According to Dr. Noecker, when he doesn’t have the corneal hysteresis reading, he really misses it. “It’s a step up from pachymetry, a more sophisticated measure and more reliable, so in some ways, I use it to see how good a job we’re doing; you can see the hysteresis rise when you treat appropriately,” said Dr. Noecker. Because visibly positive feedback can be rare in many of these interventions, this data adds a necessary slice of positivity to the process.
New Digs: MIGS In the fi nal part of the presentation, Drs. Noecker and Thimons explored some of the latest, real-time results trickling in from the use of the newest
drugs on the market—Rhopressa (Aerie Pharma-ceuticals) and Vyzulta (Bausch + Lomb)—as well as the newest frontiers in MIGS. Dr. Noecker said that in combining two or three MIGS for one patient, he has come across impressively positive results. And while he’s seen varying success with lowering IOP across these procedures, the greatest triumph lies in the breadth of options.
According to Dr. Thimons, glaucoma treatment was once “drops and laser and then trabeculec-tomy, with a gigantic space in between.” Now, however, we “have minimally eight, maybe 10 procedures in the middle of that, each of which gives you a different risk pattern, a different IOP endpoint that you can drive to, and we’re seeing remarkable results, like patients dropping into the low teens and staying there for years without drops.”
In closing, the message was clear: thanks to new technologies and surgical procedures, we are on the horizon of revolutionizing the course of glaucoma. •
000_sd0318_FRI_final.indd 21000_sd0318_FRI_final.indd 21 3/1/18 5:59 PM3/1/18 5:59 PM

DAILY22
REVIEW OF OPTOMETRY • SECO SHOW DAILY • MARCH 2, 2018
Chances are, you’ve had patients ask you about their headaches. These can include migraine, facial pain syndromes and pain
related to cranial neuropathies, orbital and ocular disease and sometimes, they can be indicative of bigger medical emergencies, so diagnosis and man-agement become crucial.
In tonight’s course (part of the Snap Chat series), attendees will learn about the most common head-ache cases as well as some of the most troubling. Richard B. Mangan, OD, will be looking for heavy audience participation while providing clinical pearls that will aid in the differentiation of benign head pain disorders and more serious disorders.
Name that HeadacheThroughout the course, Dr. Mangan will address the many different types of headaches, including tension headaches, cluster headaches, migraines,
rebound headaches, infl ammatory headaches, sinus headaches and brain tumor headaches.
Within each section, he will start with a review of the headache’s typical presentation. For ex-ample, tension headaches are “characterized by gradual onset, bilateral, non-throbbing, aching pain over the frontal and temporal regions, which often spreads to the occipital,” says Dr. Mangan.
Finding ReliefManaging headaches can be tricky, as it usually calls on the practitioner to decide whether behavior modifi cation or abortive or prophylactic treatment would be more appropriate.
In addition to the many types of headache pre-sentations that exist, Dr. Mangan will discuss what each could indicate, including giant cell arteritis, infectious meningitis, pseudotumor cerebri, brain tumors and stroke.
Finishing up, Dr. Mangan will give attendees a crash “Radiology 101” course for headache cases. “Computerized tomography is today’s preferred imaging modality to exclude intracranial patholo-gy, especially in acute cases,” says Dr. Mangan. •
The speakers in “Understanding and Interpreting the OCT in Retina and Glaucoma”
on Thursday morning made a con-vincing case for the importance of using optical coherence tomography (OCT) in clinical eye care practice for diagnosing, following and man-aging retina and glaucoma-related conditions.
Noting the fi rst scientifi c description of OCT in the Journal of Science in 1991, the speakers said OCT is now widely embraced by optometrists and ophthalmologists. Its widespread use is being driven by increased demand for eye care due to an aging population, yielding a growing number of cases involving macular degeneration, diabetic retinopathy, retinal vascular disease and glaucoma.
“What an opportunity for optometry to get involved in medical eye care,” said Mark Dunbar, OD, director of optometric services at Bascom Palmer Eye Institute, “by having an OCT to keep these patients in your chair longer.”
Qualities of a Good OCTDr. Dunbar said his experience with various retinal OCT devices and software packages revealed that they all were “very good.” He pointed out that “a B-scan is a B-scan” and that—on both ends of the economic spectrum—all OCT offerings he has tried offer high defi nition, three- to fi ve-micron images that pick up key features of
abnormality and pathology. Though OCT software programs for glaucoma
are unique, Dr. Dunbar said the differences boil down to subjective factors and personal prefer-ences. But he pointed out that all the devices do a “great job” of detecting retinal nerve fi ber layer thinning and evaluating the ganglion cell complex. Since the hardware is similar across platforms, software that is patient friendly, com-petitively priced and fi ts the needs of clinicians are important purchasing considerations.
When it comes to OCT selection, Jeffry D. Gerson, OD, an optometrist at Grin Eye Care in
Leawood, Kan., compared the process to buying different tiers of contact lenses from companies offering “good, better and best” options. “For most patients, the ‘good’ works out just fi ne,” Dr. Gerson said.
Confi dence FactorDuring the comprehensive presentation, featuring 245 slides, in which Drs. Dunbar and Gerson gave tips for OCT interpretation of retinal and glauco-ma conditions, the speakers urged clinicians not to make OCT interpretation more complicated than it needs to be. With any kind of imaging technol-ogy, especially when dealing with anatomy, there can be an “intimidation factor,” they noted. Dr. Dunbar told the story of a friend and colleague who purchased an OCT several years ago.
“He went through all of those insecurities: ‘Is this technology too advanced for me? Am I smart enough to fi gure it out?’” Dr. Dunbar said. A year later, the friend’s confi dence with OCT was high. “It really changed his life and how he practices,” Dr. Dunbar said. “So don’t get caught up in the minutia.”•
FRIDAY: 5–6pm ROOM A316, LEVEL 3
Making a Case for OCT How imaging technology can change the way you practice.
Take the Pain Out of Managing HeadachesPractitioners should be prepared to get to the bottom of these cases. This course can help.
This CT scan shows a parietal ischemic stroke.
“What an opportunity for optometry to get involved in medical eye care,” said Dr. Dunbar, “by having an OCT to keep these patients in your chair longer.”
000_sd0318_FRI_final.indd 22000_sd0318_FRI_final.indd 22 3/1/18 5:50 PM3/1/18 5:50 PM

NEW
SECO2018_CooperVision.indd 1SECO2018_CooperVision.indd 1 2/27/18 5:54 PM2/27/18 5:54 PM

Straight. Forward. Technology.For Straightforward Scleral Lens Fitting.
MicroVault™ TechnologyFully vaults the lens over elevations
that might interfere with a proper landing.
5000 sag4800 sag (standard)
4600 sag
SmartCurve™ TechnologySimplify your fitting.
Modify only those parameters that need to change.
Indicated for Ocular Surface DiseaseIncluding Dry Eye
®/TM are trademarks of Bausch & Lomb Incorporated or its affiliates. © Bausch & Lomb Incorporated. ALZN.0056.USA.17
To learn more, call or visit:
800-253-3669 • www.bauschsvp.com
For irregular corneas• Vaults the cornea and limbus to fit a wide range of corneas
• Lens diameters of 16.0 mm and 17.0 mm
• Prolate and oblate designs for a variety of corneal shapes
For regular corneas• Smaller diameters of 14.8 mm and 15.4 mm for regular corneas
• Single profile prolate design
Assistance from FCLSA* trained fitting consultants
* Fellow of Contact Lens Society of America
Scleral lens technology to help you… and your patients.
SECO2018_BL Specialty.indd 1SECO2018_BL Specialty.indd 1 2/27/18 5:53 PM2/27/18 5:53 PM
Related Documents











