D-Thyroxine Reduces Lipoprotein(a) Serum Concentration in Dialysis Patients CHRISTIANE BOMMER,* EGON WERLE,* INGEBORG WALTERSACK,* CHRISTINE KELLER,* FRANK GEHLEN,* CHRISTOPH WANNER, MATTHIAS NAUCK, WINFRIED MARZ HEINRICH WIELAND and JURGEN BOMMER* *Medizjnjsche Universit#{228}tsklinik, Heidelberg, Germany; Medizinische Universit#{228}tsklinik, Wiirzburg, Germany; and Medizinische Universit#{228}tsklinik, Freiburg, Germany. Abstract. Uremia raises lipoprotein(a) (Lp(a)) serum concen- tration and the risk of arteriosclerosis in dialysis patients. The treatment of high Lp(a) levels is not satisfactory today. The decrease of Lp(a) in hypothyroid patients on L-I4 therapy raised the question of whether dextro-thyroxine (D-thyroxine) reduces not only serum cholesterol, but also Lp(a) serum concentration. In a single-blind placebo-controlled study, the influence of 1)-thyroxine therapy on Lp(a) serum concentration was evaluated in 30 hemodialysis patients with elevated Lp(a) serum levels. Lp(a) was quantified in parallel by two methods, i.e., rocket immunoelectrophoresis and nephebometry, and apo(a) isoforms were determined by a sensitive immunobbot- ting technique. Regardless of the apo(a) isoforms, 6 mg/d D-thyroxine reduced elevated Lp(a) levels significantly by 27 ± 13% in 20 dialysis patients (P < 0.001) compared with 10 control subjects (-9.9 ± 8.4%). In parallel, D-thyroxine therapy significantly lowered total cholesterol (P < 0.001), LDL cholesterol (P < 0.001), and LDL cholesterollHDL cho- lesterob ratio (P < 0.01); raised 14 and 13 serum levels; and suppressed thyroid-stimulating hormone secretion without causing clinical symptoms of hyperthyroidism in any of the patients. D-Ihyroxine reduces elevated serum Lp(a) concentra- tion in dialysis patients. The effect in nondialysis patients can be expected but remains to be proven. (I Am Soc Nephrol 9: 90-96, 1998) Arteriosclerosis is accelerated in patients with end-stage renal disease (ESRD) ( 1 ). Various risk factors may be involved in the pathogenesis of arteriosclerosis in ESRD patients, such as hypertension, impaired glucose tolerance, decreased HDL, and increased serum levels of triglycerides and also of lipopro- tein(a) (Lp(a)). During the past 10 yr, Lp(a) has been recog- nized as an independent risk factor for coronary, cerebral, and peripheral arteriosclerosis in the healthy population and also in dialysis patients. In a prospective study, Cressman and cob- leagues noted a significantly higher plasma level of Lp(a) in dialysis patients with complications due to arteriosclerosis compared with patients without such complications (2). Today, treatment of elevated Lp(a) plasma concentrations is not satisfactory. A low-cholesterol diet (3), chobestyramine (4), and ()hydroxy-(f3)methyl glutaryl-CoA reductase inhibitors (5-7) did not reduce Lp(a) plasma levels. Niacin therapy was followed by a significant decrease of Lp(a) bevels, but was poorly tolerated due to its side effects (8). Gemfibrozib (2 X 600 mg) reduced Lp(a) bevels by 27% in hyperchobesterolemic patients (9). N-Acetylcysteine also mildly reduced plasma 1ev- els of Lp(a) (10). Furthermore, sex hormones may influence Received February 17, 1997. Accepted July 16. 1997. Correspondence to Dr. lUrgen Bommer. 1 Medizin. Universithtsklinik Heidel- berg, Bergheimer Strasse 56, D-69 115 Heidelberg. Germany. 1046-6673/090i-0090$03.00/0 Journal of the American Society of Nephrobogy Copyright 0 1998 by the American Society of Nephrology Lp(a) plasma concentrations. The use of estrogen as contracep- tive (1 1), as postmenopausal hormone therapy (12), or for treat- ment of men with prostatic cancer was followed by a decrease of serum Lp(a) levels (13). Recently, bifibrol, a new lipid-lowering agent, has also been shown to lower Lp(a) concentrations by approximately 30% (14). Recent clinical observations indicated that treatment with the thyroid hormones levo-triiodothyronine (L-13) or levo- thyroxine (L-14) reduces cholesterol concentrations and also Lp(a) levels in hypothyroid patients (15-18). This raised the question of whether dextro-thyroxine (D-thyroxine), which does not have significant general metabolic effects as L-thy- roxine, but does lower serum cholesterol levels, is able to reduce Lp(a) serum concentrations. Therefore, we studied the effect of D-thyroxine on serum lipids and Lp(a) in dialysis patients with elevated Lp(a) serum concentrations. Materials and Methods Patients A total of 39 (13 women, 26 men) chronic hemodialysis patients with a basal Lp(a) concentration of more than 250 mgIL were enrolled in the study. The mean age was 58.8 ± I I .0 yr (mean ± SD), and the duration of dialysis therapy was 71 .2 ± 79.7 mo. All of the patients were routinely dialyzed for 5 h 3 times a week using Gambro AK1O (Gambro, Lund, Sweden) or Fresenius MTS 2008 C or 4008 C machines (Fresenius, Bad Homburg, Germany), and GFSI5 M, GFS l5H (Gambro, Hechingen, Germany), F6, F60, F50 diaiyzers (Frese- nius) or Renak l5U dialyzers (Kawasumi, Shmagawa KU, Tokyo,

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

D-Thyroxine Reduces Lipoprotein(a) Serum Concentration in
Dialysis Patients
CHRISTIANE BOMMER,* EGON WERLE,* INGEBORG WALTER�SACK,*
CHRISTINE KELLER,* FRANK GEHLEN,* CHRISTOPH WANNER,�MATTHIAS NAUCK,� WINFRIED MARZ� HEINRICH WIELAND� and
JURGEN BOMMER*
*Medizjnjsche Universit#{228}tsklinik, Heidelberg, Germany; �Medizinische Universit#{228}tsklinik, Wiirzburg, Germany;
and Medizinische Universit#{228}tsklinik, Freiburg, Germany.
Abstract. Uremia raises lipoprotein(a) (Lp(a)) serum concen-
tration and the risk of arteriosclerosis in dialysis patients. The
treatment of high Lp(a) levels is not satisfactory today. The
decrease of Lp(a) in hypothyroid patients on L-I4 therapy
raised the question of whether dextro-thyroxine (D-thyroxine)
reduces not only serum cholesterol, but also Lp(a) serum
concentration. In a single-blind placebo-controlled study, the
influence of 1)-thyroxine therapy on Lp(a) serum concentration
was evaluated in 30 hemodialysis patients with elevated Lp(a)
serum levels. Lp(a) was quantified in parallel by two methods,
i.e., rocket immunoelectrophoresis and nephebometry, and
apo(a) isoforms were determined by a sensitive immunobbot-
ting technique. Regardless of the apo(a) isoforms, 6 mg/d
D-thyroxine reduced elevated Lp(a) levels significantly by
27 ± 13% in 20 dialysis patients (P < 0.001) compared with
10 control subjects (-9.9 ± 8.4%). In parallel, D-thyroxine
therapy significantly lowered total cholesterol (P < 0.001),
LDL cholesterol (P < 0.001), and LDL cholesterollHDL cho-
lesterob ratio (P < 0.01); raised 14 and 13 serum levels; and
suppressed thyroid-stimulating hormone secretion without
causing clinical symptoms of hyperthyroidism in any of the
patients. D-Ihyroxine reduces elevated serum Lp(a) concentra-
tion in dialysis patients. The effect in nondialysis patients can
be expected but remains to be proven. (I Am Soc Nephrol 9:
90-96, 1998)
Arteriosclerosis is accelerated in patients with end-stage renal
disease (ESRD) ( 1 ). Various risk factors may be involved in
the pathogenesis of arteriosclerosis in ESRD patients, such as
hypertension, impaired glucose tolerance, decreased HDL, and
increased serum levels of triglycerides and also of lipopro-
tein(a) (Lp(a)). During the past 10 yr, Lp(a) has been recog-
nized as an independent risk factor for coronary, cerebral, and
peripheral arteriosclerosis in the healthy population and also in
dialysis patients. In a prospective study, Cressman and cob-
leagues noted a significantly higher plasma level of Lp(a) in
dialysis patients with complications due to arteriosclerosis
compared with patients without such complications (2).
Today, treatment of elevated Lp(a) plasma concentrations is
not satisfactory. A low-cholesterol diet (3), chobestyramine (4),
and (�)hydroxy-(f3)methyl glutaryl-CoA reductase inhibitors
(5-7) did not reduce Lp(a) plasma levels. Niacin therapy was
followed by a significant decrease of Lp(a) bevels, but was
poorly tolerated due to its side effects (8). Gemfibrozib (2 X
600 mg) reduced Lp(a) bevels by 27% in hyperchobesterolemic
patients (9). N-Acetylcysteine also mildly reduced plasma 1ev-
els of Lp(a) (10). Furthermore, sex hormones may influence
Received February 17, 1997. Accepted July 16. 1997.
Correspondence to Dr. lUrgen Bommer. 1 Medizin. Universithtsklinik Heidel-
berg, Bergheimer Strasse 56, D-69 1 15 Heidelberg. Germany.
1046-6673/090i-0090$03.00/0Journal of the American Society of Nephrobogy
Copyright 0 1998 by the American Society of Nephrology
Lp(a) plasma concentrations. The use of estrogen as contracep-
tive (1 1), as postmenopausal hormone therapy (12), or for treat-
ment of men with prostatic cancer was followed by a decrease of
serum Lp(a) levels (13). Recently, bifibrol, a new lipid-lowering
agent, has also been shown to lower Lp(a) concentrations by
approximately 30% (14).
Recent clinical observations indicated that treatment with
the thyroid hormones levo-triiodothyronine (L-13) or levo-
thyroxine (L-14) reduces cholesterol concentrations and also
Lp(a) levels in hypothyroid patients (15-18). This raised the
question of whether dextro-thyroxine (D-thyroxine), which
does not have significant general metabolic effects as L-thy-
roxine, but does lower serum cholesterol levels, is able to
reduce Lp(a) serum concentrations. Therefore, we studied the
effect of D-thyroxine on serum lipids and Lp(a) in dialysis
patients with elevated Lp(a) serum concentrations.
Materials and MethodsPatients
A total of 39 (13 women, 26 men) chronic hemodialysis patientswith a basal Lp(a) concentration of more than 250 mgIL were enrolled
in the study. The mean age was 58.8 ± I I .0 yr (mean ± SD), and theduration of dialysis therapy was 71 .2 ± 79.7 mo. All of the patients
were routinely dialyzed for 5 h 3 times a week using Gambro AK1O
(Gambro, Lund, Sweden) or Fresenius MTS 2008 C or 4008 C
machines (Fresenius, Bad Homburg, Germany), and GFSI5 M, GFS
l5H (Gambro, Hechingen, Germany), F6, F60, F50 diaiyzers (Frese-
nius) or Renak l5U dialyzers (Kawasumi, Shmagawa KU, Tokyo,

D-Thyroxine Lowers Serum Lipoprotein(a) 91
Japan), with a diabysate flow of 500 mi/mm and a blood flow of 240
to 300 mb/mm with a double-needle technique. The dialysis devices
and procedure were kept constant throughout the study period, and
urea reduction rates were consistently >60% and varied only by ± 3%
in the single patient. The underlying renal diseases were giomerulo-
nephritis (n = 15), analgesic nephropathy (n = 4), diabetic nephro-
pathy (n = 6). obstructive nephropathy (“ = 2). amyboidosis (,z 1),
tuberculosis (a = I ), polycystic kidney disease (n = 3), nephroscle-
rosis (ii = 3), and unknown (n 4). Euthyroidism was documented
by the serum concentrations of thyroid-stimulating hormone (TSH),
total thyroxine. and triiodothyronine in all patients during the placebo
period preceding the D-thyroxine treatment. Median values (andranges) were within the normal range: TSH, 1.24 (0.02 to 3.0) mUlL;
total thyroxine, 77. 1 (45 to 132) nmollL; and total triiodothyronine.
1.75 (1 .32 to 2.67) nmollL. Medication of patients included subcuta-
neous or intravenous recombinant human erythropoietin, intravenous
iron gluconate, and orally vitamins, calcium salts, or aluminum-containing phosphate binders, sedatives, digitalis, nitrates, and an-
tidiabetics, but no antilipid therapy other than D-thyroxine. The treat-
ment was kept constant except for minor modifications, which have
no known effect on lipid metabolism. Twelve of the 30 evaluated
patients were continuously treated with antihypertensive drugs. In
only one patient was metoprolol treatment ( I X 50 mg) stopped after
5 wk of the D-thyroxine treatment.
Study Drug Therapy
In this randomized single-blind study, the patients were subdividedinto two groups: control subjects (ii 13) and the D-T4 group (‘1
26). The D-T4 group was further subdivided into D-T4 group 1 (ii =
15), with a placebo period of4 wk, and D-T4 group 2 (n = 11), with
a placebo period of 8 wk, before n-thyroxine treatment was started.
D-Thyroxine (Dynothel#{174}, Fa. Henning, Berlin, Germany) treatmentwas started with 2 mg/d, increased every 4 wk by 2 mg to a maximum
of 6 mg/d. The daily dosage of the medication was organized in
separate pilibox compartments to ensure correct and timely adminis-
tration of the medication. The D-thyroxine therapy was followed by a
b2-wk washout period without further medication. Nine patients were
excluded from the final evaluation: three control subjects for relapse
of vasculitis, decompensating diabetes, or transfer to another dialysis
center; three patients in the D-T4 group 1 for septicemia, tuberculosis,
or noncompliance; and three patients in the D-T4 group 2 due toocclusive bowel disease or obvious noncompliance, and one patient
who refused to continue the study because of itching during the
placebo phase.
During the 32 wk of the study, laboratory tests were performed
before and at 4-wk intervals during the phases of placebo and D-
thyroxine treatment. During the final washout period, measurements
were done after 6 and I 2 wk. The study was conducted in accordancewith the guidelines proposed in the Declaration of Helsinki. The study
protocol was approved by the Ethics Committee ofthe Medical Centerof the University of Heidelberg, and written informed consent was
obtained from the patients.
Assessment of Efficacy
Blood was taken just before a hemodialysis session. Serum and
plasma (heparinized) were refrigerated at 4#{176}Cor frozen at -21#{176}C.All
measurements were done within the next week except for the deter-
mination ofT3, T4, and TSH, which were measured simultaneously at
the end ofthe study after storage at - 2 1#{176}C.The quantification method
of thyroxine and triiodothyronine did not differentiate between the
dextro and levo isoforms.
Lp(a) was measured by two different methods, rocket electrophore-sis and nephebometry. in two different laboratories in Heidelberg and
Freiburg. During the electroimmunodiffusion test (Immuno AG, Vi-enna Austria), Lp(a) formed a rocket-like precipitation in the anti-apo(a) antibody-loaded agarose gel. The length of that rocket-like
precipitation corresponds to the concentration of the Lp(a). Nephelo-
metrically. Lp(a) was determined with polyclonal antibodies (Inkstar,
Stillwater. MN) on a Behring Nephelometer (Behring. Marburg. Ger-
many) as described in detail by Nauck et a/. (19). apo(a) isoform
determination was performed on whole serum, using a sensitive
immunoblotting technique described previously (20) and modified as
follows. Briefly. 12 pA of serum was mixed with 100 pA of samplebuffer containing 5% sodium dodecyl sulfate. 2% mercaptoethanol.and 2% bromphenol blue. After 10 mm of boiling in a waterbath, the
reduced samples were applied to a 4% polyacrylamide electrophoresis
gel and run for approximately 2 h at 30 mA. After electrotransfer of
the proteins to Immobilon polyvinyldifluoride transfer membranes(Millipore, Bedford, MA). membranes were blocked with 3% bovine
serum albumin, incubated with a polyclonal anti-apo(a) antibody
(Immuno AG), and detected with the anti-sheep IgG (Fc) alkaline
phosphatase method. A standard of a defined isoform pool (B, S I , S3,
S4, >54) was used on each gel.
The functional thrombin-coagulable fibrinogen was quantified with
the Clauss method (Bioniatic Sarstedt, NOmbrecht, Germany). Totalcholesterol and triglycerides were measured enzymatically (Boehr-
inger. Mannheim, Germany). VLDL cholesterol (VLDL-C), LDL
cholesterol (LDL-C), and HDL cholesterol (HDL-C) were analyzed
with a combined ultracentrifugation and precipitation technique (2 1).
The “pure” LDL cholesterol, corrected for the content of Lp(a) in theLDL, was calculated as: ‘�pure” LDL LDL-C - 0.3 X Lp(a) (22).
Aspartate aminotransferase, alanine aminotransferase, urea, creati-
nine, and uric acid were measured by the Chem- I chemistry analyzer
(Bayer Technicon. Munich, Germany). C-reactive protein was mea-sured by rate nephelometry with the Array 360 analyzer (Beckman,
Munich, Germany).
Statistical Analysis
Mean values and SEM (±SD) or median values and ranges are
given unless otherwise stated. In the control group and the total group
of D-thyroxine-treated patients, the changes of serum concentration of
lipids and other parameters during the study period were analyzed by
the Wilcoxon matched-pairs signed rank test, if the Friedman two-wayANOVA was significant.
In Caucasian populations, serum Lp(a) concentrations show noGaussian distribution but do show a skewed distribution. In the
Kolmogorov-Smirnov test of normal distribution, normal Gaussian
distribution was also not given in all other laboratory data. possibly
due to the limited number of control subjects and D-thyroxine-treatedpatients. Therefore, the individual serum concentrations of Lp(a) and
other variables assessed during the u-thyroxine treatment period and
washout period were compared with the mean of the two concentra-
tions found during the preceding placebo period. By this method, the
percent changes were calculated for each single laboratory result and
analyzed by the Kruskal-Wallis ANOVA by ranks. Furthermore, at
different points in time, the percent changes of lipids and other
laboratory results in D-thyroxine-treated patients were compared with
those in control patients by the Wilcoxon rank sum test.
ResultsAs measured by electroimmunodiffusion test, mean Lp(a)
decreased significantly from 47.4 ± 22.9 to 34.2 ± 16.6 mg/dl

92 Journal of the American Society of Nephrology
Table 1. Lipids and body weight in D-thyroxine-treated patients and control subjects”
Category Preceding Placebo I 2 wk D-T4 16 wk D-T4 Washout
Lp(a) rocket (mg/dl)
controls 52.2 ± 8.9 (49.3) 47.5 ± 8.0 (40.0) 48.3 ± 9.7 (45.5) 48.2 ± 8.4 (43.5)
D-14 47.4 ± 5.1 (42.5) 34.2 ± 4.0 (335)b 34.2 ± 3.7 (33#{149}5)b 41.4 ± 4.4 (43.5)
Lp(a) nephebometry (mg/db)
controls 52.5 ± 10 (45.8) 49.3 ± 10.5 (35) 57.3 ± 13.3 (49.0) 53.7 ± 6.3 (51.5)
D-14 46.9 ± 4.7 (38.8) 38.7 ± 5.2 (31.0)c 41.2 ± 5.1 (33.0)c 50.7 ± 5.0 (46)
Total cholesterol (mg/dl)
controls 180.7 ± 10.5 (177) 186.1 ± 10.3 (178) 183.6 ± 12 (189) 178.3 ± 10.2 (175)
D-14 192.6 ± 8.5 (195) 163.1 ± 8.3 (162)b 161.1 ± 8.5 (157)b 190 ± 7.4 (185.5)
VLDL-C (mg/dl)
controls 40.2 ± 5.7 (41.5) 49.2 ± 5.3 (53.8) 44.0 ± 6.3 (43.5) 38.3 ± 4.7 (41.5)
D-14 27.8 ± 3.4 (27.0) 23.9 ± 3.6 (24.0) 23.2 ± 3.6 (19#{149}5)d 26.2 ± 3.4 (23.0)
LDL-C (mg/db)
controls 116±9.1 (115.5) 111 ±9.6 (104) 113±8.2 (119) 118.7±9.5 (114.5)
D-I4 128.8 ± 7.4 (130) 103 ± 5.1 (102)C 101 ± 5.1 (985)b 127.8 ± 6.6 (123.5)
“Pure” LDL-C (mg/dl)
controls 100.3 ± 10.2 (101) 96.4 ± 10.1 (93.0) 98.9 ± 9.6 (86) 103.1 ± 10.4 (102)
D-14 114.5 ± 7.9 (117) 93 ± 5.6 (93)L� 90.3 ± 5.5 (86)L� 113 ± 7.4 (100)
HDL-C (mg/dl)
controls 25.4 ± 1.3 (25.0) 26.4 ± 1.3 (26.5) 26.0 ± 1.0 (25.5) 25.7 ± 1.1 (26.0)
D-4 36.2 ± 3.2 (33.3) 36.3 ± 3.7 (32.5) 37.7 ± 3.5 (35.0) 35.6 ± 2.0 (35.0)
LDL-C/HDL-C ratio
controls 4.69 ± 0.4 (4.64) 4.26 ± 0.4 (3.86) 4.44 ± 0.4 (4.57) 4.61 ± 0.4 (4.37)
D-14 3.98 ± 0.4 (4.02) 3.23 ± 0.3 (3.1 1)b 2.93 ± 0.2 (2.91)” 3.80 ± 0.3 (3.86)
Body weight (kg)
controls 64.2 ± 3.7 (64.2) 64.4 ± 3.7 (66.0) 64.6 ± 3.7 (66.0) 64.1 ± 4.2 (64.5)
D-14 69.4 ± 2.5 (68.6) 69.3 ± 2.5 (68.5) 69.6 ± 2.6 (68.8) 69.5 ± 2.7 (68.8)
a Data given as mean ± SEM (median), significantly different compared with preceding placebo period. Wilcoxon matched-pairs signed
rank test.hp <0.001.
ep < 0.01.d p < 0.05.
under 6 mg/d D-thyroxine therapy (Table 1 , Figure 1). This
decrease by 27 ± I 3% is significant compared with the control
patients (P < 0.01). A relevant change of the Lp(a) bevels was
not found in the control group (52.2 ± 28.3 mg/dl at the
beginning, and 48.3 ± 30.6 mg/dl (-9.9% ± 8.4%) after 16
wk of the treatment period. During the next washout period,
Lp(a) serum concentrations reincreased and were similar to
those found in control patients.
When Lp(a) was measured by nephelometry, D-thyroxifle
therapy reduced mean Lp(a) levels from 46.9 ± 21.2 to 38.7 ±
23.3 mg/dl after week 12 and to 41.2 ± 22.6 mg/L after week 16
of therapy (lable 1 ). This is a significant decrease of 20.3 ± I 7.1
and 13 ± 17%, respectively (P < 0.05), compared with the
control patients in whom Lp(a) bevels did not change significantly
(52.5 ± 3 1 .6 mg/db before and 49.3 ± 33.3 mg/dl after week 12,
and 57.3 ± 41 .9 mg/L after week 16 of the treatment period).
After the final washout period, Lp(a) levels were not different in
previously D-thyroxine-treated and control patients.
In parallel, total cholesterol levels decreased from 192.0 ±
37.9 to 161.1 ± 38 mg/dl (16.3 ± 10.5%, P < 0.01) (Figure 2)
during maximal D-thyroxine therapy and remained stable in the
control subjects (180.7 ± 33.3 mg/db versus 183.6 ± 38.02
mg/dl) (Table 1 ). LDL cholesterol remained stable in the
control subjects and decreased from 1 28.8 ± 33. 1 mg/dl to
101 ± 22.8 mg/dl (20.7 ± 10.4%, P < 0.01) (Figure 3) during
D-thyrOxifle therapy. The “pure” LDL was constant in the
control group but decreased in the D-thyroxine-treated patients,
from 1 14.5 ± 35.5 to 90.3 ± 24.7 (P < 0.01) (lable 1). HDL
cholesterol bevels did not change markedly in the control
patients (25.4 ± 4.3 mg/dI versus 26.0 ± 3. 1 mg/dl) or D-
thyroxine-treated patients (36.2 ± 14.1 mg/db versus 37.7 ±
15.2 mg/dI). Furthermore, the LDL cholesterol/HDL chobes-
terol ratio did not change in the control patients (4.7 ± 1.4
versus 4.5 ± I .2) but decreased significantly in the D-thyrox-
me-treated patients, from 4.0 ± 1 .6 to 2.9 ± 1 .0 (23 ± 14.5%,
P < 0.01). The VLDL cholesterol also decreased under D-
thyroxine therapy, from 27.8 ± 15.4 to 23.2 ± 16.3 mg/dl
(19.8 ± 42.2%, P < 0.05). The decrease of serum triglyceride
levels (from 166 ± 76 to 138.5 ± 69.3 mg/dl) agreed with the
fall of VLDL cholesterol levels, but was not significant.

weeks
weeks
u-Thyroxine Lowers Serum Lipoprotein(a) 93
15%
10%
5%
C �o,(� _�,o
� -15%
-25%
-30%
-35%
Lp(a) Rocket Electrophoresis
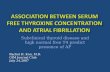
Figure 1. Changes of lipoprotein(a) (Lp(a)) serum concentration expressed as percentage of the mean Lp(a) level during the preceding placebo
period in the individual patients (mean ± SEM). Control subjects (S), D-T4 group I (U), D-T4 group 2 (A), and all D-T4-treated patients (X).Significant difference of the percent changes between control subjects and all D-T4 patients at the different points of time. *P < 0.05; **� < 0.01
(Wilcoxon rank sum test).
10%
5%
-10%e0 .iroIQ__ R310
-20%
-25%
Cholesterol
Figure 2. Changes of total serum cholesterol concentration expressed as percentage of the mean total cholesterol level during the preceding
placebo period in the individual patients (mean ± SEM). For symbols and significance, see Figure 1.
D-Ihyroxrne therapy increased serum concentrations of 14
from 90.5 ± 25.5 to 147.5 ± 40.8 ng/ml (P < 0.001 ) and of 13
from 1.8 ± 0.4 to 4.1 ± 1.2 ng/mb (P < 0.001) and decreased
ISH serum concentrations from 1 . 1 ± 0.8 mUlL to <0.01
mUlL (P < 0.001). All other variables, including C-reactive
protein, albumin, total protein, and fibrinogen concentration,
remained unaffected in control and D-thyroxine-treated patients
throughout the study period.
Body weight (Table 1) or predialytic pulse rate and BP did
not change markedly. Other clinical symptoms of hyperthy-
roidism were not found in any of the patients in response to the
D-thyroxine therapy. During the preceding placebo period, one
patient reported mild paroxysmal tachycardia, with heart rates
up to 100 beats/mm for 6 d, which stopped spontaneously.
DiscussionIn agreement with previous reports, D-thyroxine therapy
reduced serum levels of total cholesterol, LDL cholesterol,
and, to a lesser extent, VLDL cholesterol (23,24). The decrease
of LDL cholesterol was also evident if the LDL cholesterol was

5%
0%i
-5%
-1
-1
*
pre 4
** **
weeks22 28
94 Journal of the American Society of Nephrology
wC)C
0
Cw
wa-
LDL-C holesterol
8 12 16
Figure 3. Changes of serum LDL cholesterol concentration expressed as percentage of the mean LDL cholesterol level during the preceding
placebo period in the individual patients (mean ± SEM). For symbols and significance. see Figure 1.
corrected for the Lp(a) content in the LDL fraction (“pure”
LDL cholesterol). In the present study, D-thyroxine therapy
with a maximum dose of 6 mg/d reduced elevated Lp(a) bevels
in uremic patients, and Lp(a) reincreased during the washout
period after 1)-thyroxine treatment. Progressing renal failure is
commonly accompanied by an increase of the Lp(a) serum
concentration. Some reports indicated that, in contrast to other
factors such as growth hormone (25), hypothyroidism (17,18),
or low estrogen levels ( 12,26), uremia induces a specific in-
crease of high molecular Lp(a) isoforms (27) that is reversed
after kidney transplantation (28). In our study, D-thyroxine
reduced Lp(a) in dialysis patients regardless of the molecular
weight of apo(a) isoforms. loday, it is possible to differentiate
34 Lp(a) phenotypes (29). The apo(a) phenotyping method
used in the current study distinguishes six apo(a) isoforms and
thus breaks down the larger number of apo(a) alleles into the
groups originally described by Utermann et al. (30,3 1 ). How-
ever, this is not a relevant limitation of our study, which
included only 30 patients. Given the tremendous heterogenicity
of the apo(a) locus, a phenotyping method with higher resolu-
tion would have revealed different phenotypes in almost all of
the individuals studied. Obviously, analysis of such data would
have required post hoc stratification, and the information
gained by a more sophisticated phenotyping method would not
have been used. When our patients were subdivided into two
groups of Lp(a) phenotypes, i.e., �S2 (B, 51, 52, high molec-
ubar Lp(a)), and >52 (53, 54, >54, low molecular Lp(a))
(27,28), the mean percent reduction of Lp(a) bevels under
D-thyrOxine therapy was identical in both groups. Repeated
determination of apo(a) phenotypes did not indicate a relevant
change in size of Lp(a) in the individual patients during D-
thyroxine therapy. In good agreement with these findings,
antithyroid therapy was followed by a comparable increase of
Lp(a) in hyperthyroid patients with high or low molecular
weight apo(a) phenotypes as well (32).
The question of the optimal and most reliable method of
quantifying serum concentrations of Lp(a) is under continuing
discussion. In the present study, the reduction of Lp(a) was
documented by two different, highly validated methods of
Lp(a) quantification, performed in two separate laboratories.
Thus, it is unlikely that the method of Lp(a) measurement was
influenced by changes of Lp(a) structure or size during the
study period.
The daily dosage of medication was organized in separate
piblbox compartments, so that each patient could always be
certain of taking the tablets. Furthermore, the increase of 14
and 13 serum levels, as well as the complete suppression of
ISH secretion in all D-thyroxine-treated patients, indicated
good compliance. Significant adverse effects such as symp-
toms of hyperthyroidism were not observed during D-thyroxine
therapy, using a very pure D-thyroxine preparation with an
L-I4 content of <0. 1 %.
The mechanism of Lp(a) reduction under D-thyroxine re-
mains unknown. L-Ihyroxine or L-trnodothyronine seems to
induce a higher expression and activity of LDL receptors
followed by enhanced LDL cholesterol catabolism (33). In
cultured fibrobbasts, 13 increases the number of LDL receptors
and the degradation rate of LDL cholesterol (34). A determi-
nant role of LDL receptors in the catabolism of Lp(a) has been
postulated, but is not proven. The Lp(a) kinetics after LDL
apheresis (35) and the fractional catabolic rate of Lp(a) in
subjects with familial hypercholesterolemia suggest that in vivo
Lp(a) is not markedly cleared by an LDL receptor-mediated
mechanism.
Ihe rather constant Lp(a) serum concentration under HMG-
CoA reductase inhibitor therapy followed by upregubation of

n-Thyroxine Lowers Serum Lipoprotein(a) 95
LDL receptors and decrease of LDL serum concentration also
points to some differences in the metabolism of LDL and
Lp(a). In our patients, D-thyroxine therapy reduced both Lp(a)
and LDL cholesterol by an average of approximately 20%. The
individual decreases of Lp(a) and LDL cholesterol did not
correlate significantly but varied markedly from patient to
patient.
In patients exhibiting the same apo(a) isoform, different
production rates of apo(a) may be more important for the
serum levels of Lp(a) than different rates of Lp(a) catabolism
(36). In patients with nephrotic syndrome, Lp(a) serum con-
centration is increased, but normalized when proteinuria dis-
appeared (37). In patients with liver diseases, plasma levels of
apo(a) significantly correlated with the microsomal function
and synthetic capacity of the liver, as indicated by the levels of
serum albumin and coagulation factor activities. In rats, tn-
iodothyronine may suppress apo B messenger RNA (38). De-
Bruin et al. postulated that thyroid hormones directly suppress
synthesis and secretion of the apo(a) moiety of Lp(a) in hu-
mans and animals ( 1 8). Additional studies are needed to clarify
the mechanism of decreasing plasma levels of Lp(a) under
L-14 and D-thyroxine therapy.
Serum levels of L-triiodothyronine and L-thyrOxine tend to
be lower in dialysis patients compared with healthy control
subjects, and in some patients low 13 syndrome is found
(39-41). In the present study, however, hypothyroidism can be
excluded by normal ISH serum levels. Furthermore, a signif-
icant effect of L-thyroxine is unlikely. The D-thyroxine prepa-
ration used contains <0. 1 % L-isoforms. Therefore, the maxi-
mal dose of 6 mg of n-thyroxine included <6 pg of L-14 and
a very small amount of L-I3. Any significant metabolic effect
cannot be attributed to the small amounts of L-I4 and L-13.
Similar doses of that D-thyrOxifle preparation were used in
patients with hyperthyroidism due to pituitary resistance to
thyroid hormones. In such patients, D-thyroxine suppresses
ISH secretion, and the symptoms of hyperthyroidism disap-
pear (42). Hamon et al. treated hypothyroid children after total
thyroidectomy plus radioiodine ablation for thyroid cancer I 0 d
with 24 mg of D-thyroXifle per day. The cholesterol bevels
decreased markedly, and the authors recommended that “the
ban on D-thyroxine could be reevaluated since purer prepara-
tions are available” (43).
In conclusion, the study presented here showed that D-
thyroxine can significantly reduce serum concentration of
Lp(a). Additional studies are required to prove the long-term
effect of o-thyroxine therapy in dialysis patients and the effect
in nondialysis patients, and to evaluate the benefits of lowering
the Lp(a) serum concentration, such as reduced risk of artenio-
sclerosis in patients with elevated Lp(a). Ihe clarification of
the mechanism by which D-thyroxine reduces Lp(a) levels may
help to determine combinations of drugs with different mech-
anisms that lower Lp(a) levels more effectively.
ReferencesI . Kronenberg F: Lipoprotein(a) in renal disease: What we have,
what we need, what we can forget. Nephro/ Dial Transplant 10:
766-769, 1995
2. Cressman MD, Heyka Ri. Paganini EP. O’Neil I. Skibinski CI,
Hoff HF: Lipoprotein(a) is an independent risk factor for cardio-
vascular disease in hemodialysis patients. Circulation 86: 475-482, 1992
3. Masarei IRL, Rouse IL, Lynch WI, Robertson K, Vandongen R,
Beilin U: Effect of lacto-ovo-vegetarian diet on serum concen-
trations of cholesterol, triglyceride. HDL-C. HDL-2-C, HDL-
3-C, and Lp(a). Am J C/in Nutr 40: 468-479, 1984
4. Vessby B, Kostner 0, Lithell H. Thomis I: Diverging effects of
cholestiramine on apolipoprotein B and lipoprotein Lp(a). At/i-
erosclerosis 44: 61-71, 1982
5. Thiery I. Armstrong VW, Schleefl. Creutzfeld C, Creutzfeld W,
Seidel D: Serum lipoprotein Lp(A) concentrations are not influ-
enced by an HMG-CoA reductase inhibitor. K/in Wochenschr 66:
462-463, 1988
6. Ramires JAF, Mansur AP, Solimene MC, Maranhao R, Chamone
D, da Luz P. Pileggi F: Effect of gemfibrozil versus lovastatin onincreased serum iipoprotein(a) levels of patients with hypercho-
lesterolemia. mt J Cardio/ 48: 1 15-120, 1995
7. Dabbongeville J, Fruchart IC, Pfister F, Bard JM: Effect of
fluvastatin on plasma apolipoprotein-B-containing particles. in-
cluding lipoprotein(a). J Intern Med 236: 95-101, 1994
8. Gurakar A, Hoeg IM. Kostner GM, Papadopoulos NM, Brewer
HB: Levels of lipoprotein (a) decline with neomycin niacin
treatment. Atherosclerosis 57: 293-301, 1985
9. Jones PH, Pownali HI, Patsch W, Herd IA, Farmer IA, Payton-Ross C, Kimball KT, Gotto AM, Morrisett ID: Effect of gemfi-
brozil on levels of lipoprotein(a) in Type II hyperlipoproteinemic
subjects. J Lipid Res 37: 1298-1308, 1996
10. Gavish D, Breslow IL: Lipoprotein(a) reduction by N-acetylcys-
teine. Lance,’ 337: 203-204, 1991
I 1 . KuhI H, Mhrz W, Iung-Hoffmann C, Weber I, Siekmeier R,Groj3 W: Effect on lipid metabolism of a biphasic desogestrel-
containing oral contraceptive: Divergent changes in apolipopro-
tein B and E and transient decrease in Lp(a). C’o�itracep!ion 47:
69-83, 1993
12. Hanggi W. Riesen W, Birkhaeuser MH: Postmenopausal hor-
mone replacement therapy with tibolone decreases serum Ii-poprotein(a). Eur J Cliii Chem C/in Bioche,n 3 1 : 645-650, 1993
13. Henriksson P. Angelin B, Berglund L: Hormonal regulation of
serum Lp(a) levels: Opposite effects after estrogen treatment and
orchidectomy in males with prostatic carcinoma. J C/in Invest
89: 1166-1171, 1992
14. Locker P. Iungbluth GL, Francom SF, Hughes GS Ir, for the
Lifibrol Study Group: Lifibrol: A novel lipid-lowering drug for
the therapy of hypercholesterolemia. C/i,: Phar,nacol Ther 57:
73-88, 1995
15. Dullaart RPF. van Doormaal II, Hoogenberg K, Sluiter WI:Triiodothyronine rapidly lowers plasma lipoprotein(a) in hypo-
thyroid subjects. Net/i J Med 46: 179-184, 1995
16. Pazos F, Alvarez I, Rubies-Prat I, Varela C, Lasuncion MA:
Long-term thyroid replacement therapy and levels of lipopro-
tein(a) and other lipoproteins. J Clin Endocrinol Metab 80:562-566, 1995
17. Engler H, Riesen WF: Effect of thyroid function on concentra-
tions of lipoprotein(a). C/in Chem 39: 2466-2469, 1993
18. De Bruin TW, Van Barlingen H, Van Linde-Sibenius Trip M,
Van Vuurst De Vries AR, Akveld MI. Erkelens DW: Lipopro-tein(a) and apolipoprotein B plasma concentrations in hypothy-
roid. euthyroid and hyperthyroid subjects. J Cliii Endocrinol
Metab 76: 121-126, 1993
19. Nauck M, Winkier K, Wittmann C. Mayer H, Luley C, M#{228}rzW,

96 Journal of the American Society of Nephrology
Wieland H: Direct determination of lipoprotein(a) cholesterol by
ultracentrifugation and agarose gel electrophoresis with enzy-
matic staining for cholesterol. C/in Chem 41 : 73 1-738, 1995
20. Wanner C, Rader D, Banens W, Kramer I, Brewer HB, Scholl-
meyer P. Wieland H: Elevated plasma lipoprotein(a) in patients
with nephrotic syndrome. Ann Intern Med 1 19: 263-269, 1993
21. Kohimeier M: Lipoproteinanalyse mit Ultrazentrifuge. Arzt/ Lab
32: 46-52, 1990
22. Li KM. Wilcken DE, Dudman NPB: Effect of serum lipopro-
tein(a) on estimation of low-density lipoprotein cholesterol by
the Friedewald formula. C/in Chern 40: 571-573, 1994
23. Rakow AD, Kl#{246}rHU, Kilter E, Ditschuneit HH, Ditschuneit H:
Treatment of type II hyperlipoproteinemia with D-thyroxine.Atherosc/erosis 24: 369-380, 1976
24. Schwandt P, Weisweiler P: The effects of D-thyroxine on ii-
poprotein lipids and apolipoproteins in primary type Ila hyper-
lipoproteinemia. Atherosclerosis 35: 301-306, 1980
25. Eden 5, Wiklund 0, Oscarsson I, Rosen T, Bengtsson BA:
Growth hormone treatment of growth hormone-deficient adultsresults in a marked increase in Lp(a) and HDL cholesterol
concentrations. Arteriosc/er Thromb 13: 296-301, 1993
26. Soma M, Fumagalli R, Paoletti R, Meschia M, Carena Maini M,
Crosignani P: Plasma Lp(a) concentration after oestrogen and
progestogen in postmenopausab women [Letter]. Lancet 37: 612,
I 99127. Dieplinger H, Lackner C, Kronenberg F, Sandholzer C, Lhotta K,
Hoppichler F, Graf H, Konig P: Elevated plasma concentrations
of lipoprotein(a) in patients with end-stage renal disease are not
related to the size polymorphism of apolipoprotein(a). J C/in
invest 91: 397-401, 1993
28. Kronenberg F, Konig P, Lhotta K, Ofner D, Sandholzer C,
Margreiter R. Dosch E, Utermann 0, Dieplinger H: Apolipopro-
tein(a) phenotype-associated decrease in lipoprotein(a) plasma
concentrations after renal transplantation. Arteriosc/er Thromb
14: 1399-1404, 1994
29. Marcovina SM, Zhang ZH, Gaur VP, Aibers II: Identification of
34 apolipoprotein(a) isoforms: Differential expression of apoli-
poprotein(a) alleles between American blacks and whites. Bio-
chem Biophys Res Commun 191 : I 192-b 196, 1993
30. Utermann G, Duba C, Menzel HI: Genetics of the quantitative
Lp(a) lipoprotein trait. II. Inheritance of Lp(a) glycoprotein phe-notypes. Hu,n Genet 78: 47-50, 1988
3 1 . Utermann G, Kraft HG, Menzel HI, Hopferwieser 1, Seitz C:Genetics of the quantitative Lp(a) lipoprotein trait. I. Relation of
Lp(a) glycoprotein phenotypes to Lp(a) lipoprotein concentra-
tions in plasma. Hu,n Genet 78: 41-46, 1988
32. Kbausen IC, HegedUs L, Hansen PS, Nielsen FE, Gerdes LU,
Faergeman 0: Apolipoprotein(a) phenotypes and lipoprotein(a)
concentrations in patients with hyperthyroidism. J Mo/ Med 73:
41-46, 1995
33. Staels B, Van Tol A, Chan L, Will H, Verhoeven G, Auwerx I:
Alterations in thyroid status modulate apolipoprotein, hepatic
triglyceride bipase and low density lipoprotein receptor in rats.
Endocrinology I 27: 1 144-1 152, 1990
34. Chait A, Bierman EL, Albers II: Regulatory role of triiodothy-
ronine in the degradation of low density lipoprotein by cultured
human skin fibroblasts. J C/in Endocrino/ Metab 48: 887-889,
I 979
35. Armstrong VW, Schleff I, Thiery J, Muche R, Schuff-Werner P.
Eisenhauer T, Seidel D: Effect of HELP-LDL-apheresis on Se-
rum concentrations of human lipoprotein(a): Kinetic analysis of
posttreatment return to baseline levels. Ear J C/in Invest 19:235-240, 1989
36. Rader DI, Cain W, Zech LA, Usher D, Brewer HB Ir: Variation
in lipoprotein(a) concentrations among individuals with the same
apobipoprotein(a) isoform is determined by the rate of lipopro-
tein(a) production. J C/in Invest 91: 443-447, 1993
37. Gansevoort KF, Heeg IE. Dikkeschei FD, de Zeeuw D, de long
PE, Duliart RP: Symptomatic antiproteinunic treatment decreasesserum lipoprotein(a) concentration in patients with glomerular
proteinuria. Nephro/ Dia/ Transplant 9: 244-250, 1994
38. Davidson NO, Powell LM, Wallis SC, Scott I: Thyroid hormone
modulates the introduction of a stop codon in rat liver apoli-
poprotein B messenger RNA. J Bio/ Chem 263: 13482-13485,
I988
39. Lim VS, Zavala DC, Flanigan Ml, Freeman RM: Blunted pe-
ripheral tissue responsiveness to thyroid hormone in uremic
patients. Kidney Int 31: 808-814, 1987
40. Gardner DF, Mars DR. Thomas RG, Bumrungsup C, Misbin RI:
Iodine retention and thyroid dysfunction in patients on hemodi-
abysis and continuous ambulatory peritoneal dialysis. Am J Kid-
ne�’ Dis 6: 471-476, 1986
41. Pagliacci MC, Pelicci 0, Grignani F, Giammartino C, Fedeli L,
Carobi C, Buoncnistiani U, Nicoletti I: Thyroid function tests in
patients undergoing maintenance dialysis: Characterization of
the “Low-T4 Syndrome” in subjects on regular hemodialysis and
continuous ambulatory peritoneal dialysis. Nephron 46: 225-
230, 1987
42. Dorey F, Strauch G. Gayno IP: Thyreotoxicosis due to pituitary
resistance to thyroid hormones. Successful control with D-Thy-
roxine: A study in three patients. C/in Endocrino/ Oxf32: 221-
228, 1990
43. Hamon P, Dingeon B, hang N-S. Orgiazzi I: Purified D-thyrox-
me in athyreotic patients. Lancet 34 1 : 1477, 1993
Related Documents