D. C. Mikulecky Faculty Mentoring Program Virginia Commonwealth Univ. 03/22/22

D. C. Mikulecky Faculty Mentoring Program Virginia Commonwealth Univ. 10/6/2015.
Dec 30, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

D. C. MikuleckyFaculty Mentoring ProgramVirginia Commonwealth Univ.
04/19/23
Water balanceElectrolyte balancePlasma volumeAcid-base balanceOsmolarity balanceExcretionHormone secretion
04/19/23

KidneysBlood supply: Renal arteries and
veinsUreterUrinary bladderUrethra
04/19/23

04/19/23
Bowman’sCapsule
Glomerulus
Proximal ConvolutedTubule
Distal ConvolutedTubule
Loop of Henle
Cortex
MedullaArtery
Vein
Peritubular Capillaries
CollectingDuct

Glomerular Filtration: Filtering of blood into tubule forming the primitive urine
Tubular Reabsorption: Absorption of substances needed by body from tubule to blood
Tubular Secretion: Secretion of substances to be eliminated from the body into the tubule from the blood
04/19/23

04/19/23
GF
TR
TA
Urine Excreted
Efferent ArterioleAfferentArteriole
Glomerulus
KidneyTubule
Peritubular Capillary

First step in urine formation180 liters/day filteredEntire plasma volume filtered 65
times/dayProteins not filtered
04/19/23

04/19/23
Glomerular CapillaryBlood Pressure + 55
Plasma Colloid Osmotic Pressure
-30
15
10
Bowman’s CapsuleHydrostatic Pressure
-
Net Filtration Pressure +

Water: 99% reabsorbed
Sodium: 99.5% reabsorbed
Urea: 50% reabsobed
Phenol: 0% reabsorbed
04/19/23
By passive diffusion
By primary active transport: Sodium
By secondary active transport: Sugars and Amino Acids
04/19/23

04/19/23
Lumen
Plasma
Cells

04/19/23
Lumen
Plasma
Cells
PUMP: Na/K ATPase
Sodium
Potassium
Chloride
Water

Stimulates Sodium Reabsorption in distal and collecting tubules
Naturetic peptide inhibits In absence of Aldosterone, 20mg of
sodium/day may be excretedAldosterone can cause 99.5%
retention
04/19/23

04/19/23
Fall in NaCl, extracellular fluid volume, arterial blood pressure
JuxtaglomerularApparatus
ReninLiver
Angiotensin
+
Angiotensin Angiotensin Aldosterone
Lungs
ConvertingEnzyme
AdrenalCortex
IncreasedSodiumReabsorption
HelpsCorrect
ACE Inhibitors (Angiotensin Converting Enzyme): Cause loss of salt---> water follows
Atrial Naturetic Peptide (ANP) also inhibits sodium reabsorption
Osmotic diuretics: Are not reabsorbed
04/19/23
They are actively transported across the apical cell membranes of the epithelial cells
Their active transport depends on the sodium gradient across this membrane
All other steps are passive
04/19/23

04/19/23
Renal threshold (300mg/100 ml)
Plasma Concentration of Glucose
GlucoseReabsorbedmg/min
Filtered Excreted
Reabsorbed
Protons (acid/base balance)
Potassium
Organic ions
04/19/23
04/19/23
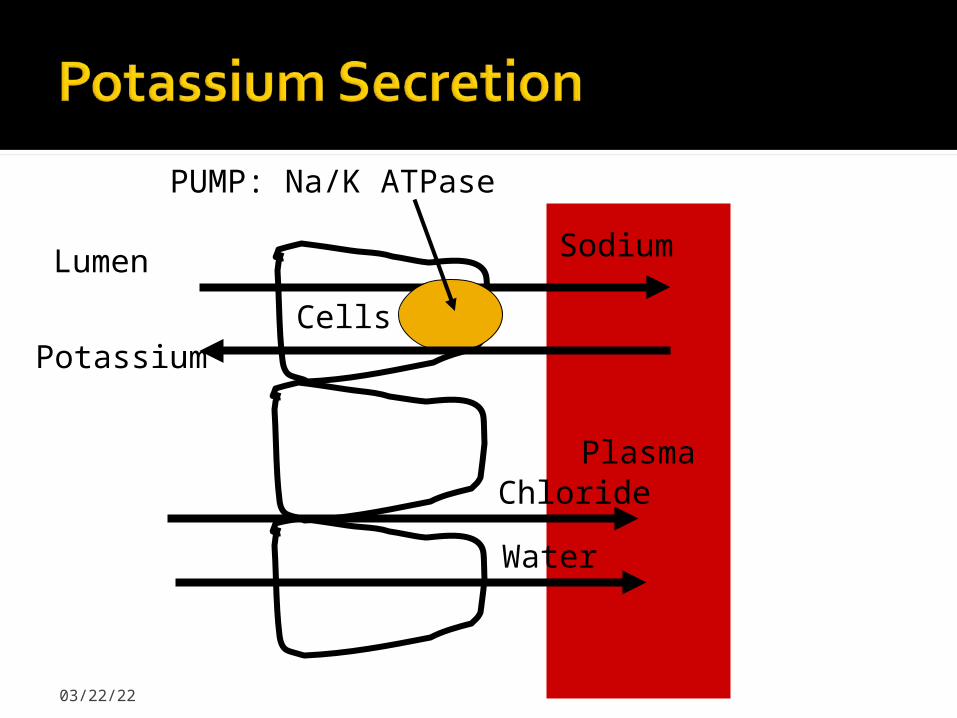
Lumen
Plasma
Cells
PUMP: Na/K ATPase
Sodium
Potassium
Chloride
Water

04/19/23
Fall in sodium
ECF Volume
Blood Pressure
Increased PlasmaPotassium
Increased Aldosterone secretion
Increased TubularPotassium Secretion
Increased UrinaryPotassium Secretion
Increased TubularSodium Reabsorption
Fall in Urinary
Sodium Excretion

Glucose and Amino Acids67% of Filtered SodiumOther Electrolytes65% of Filtered Water50% of Filtered UreaAll Filtered Potassium
04/19/23
Variable Proton secretion for acid/base regulation
Organic Ion secretion
04/19/23

Variable Sodium controlled by Aldosterone
Chloride follows passively
Variable water controlled by vasopressin
04/19/23
Variable Proton for acid/base regulation
Variable Potassium controlled by aldosterone
04/19/23
Variable water reabsorption controlled by vasopressin
Variable Proton secretion for acid/base balance
04/19/23

Medullary countercurrent system
Vasopressin
04/19/23

Osmotic gradient established by long loops of Henle
Descending limb
Ascending limb
04/19/23

Highly permeable to water
No active sodium transport
04/19/23
Actively pumps sodium out of tubule to surrounding interstitial fluid
Impermeable to water
04/19/23

04/19/23
300
450
600
750
900
1050
1200
1200
From ProximalTubule
To DistalTubule
Cortex
Medulla300
450
600
750
900
1050
1200
1200
100
250
400
550
700
850
1000
1000
ActiveSodiumTransport
PassiveWaterTransport
Long Loopof Henle

04/19/23
From DistalTubule
Cortex
Medulla300
450
600
750
900
1050
1200
1200
300
400
550
700
850
1000
1100
1200
Interstitial Fluid
CollectingDuct
PoresOpen
Passive Water Flow

04/19/23
From DistalTubule
Cortex
Medulla300
450
600
750
900
1050
1200
1200
100
100
100
100
100
100
100
100
Interstitial Fluid
CollectingDuct
PoresClosed
No Water FlowOut of Duct

Acute: Sudden onset, rapid reduction in urine output - usually reversible
Chronic: Progressive, not reversible
Up to 75% function can be lost before it is noticeable
04/19/23

Gravity and peristaltic contractions propel the urine along the ureter
Parasympathetic stimulation contracts the bladder and micturition results if the sphincters (internal and external urethral sphincters) relax
The external sphincter is under voluntary control
04/19/23

Bladder filling reflexively contracts the bladder
Internal Sphincter mechanically opens
Stretch receptors in bladder send inhibitory impulses to external sphincter
Voluntary signals from cortex can override the reflex or allow it to take place
04/19/23
Related Documents