Cytomegalovirus: a culprit or protector in multiple sclerosis? Marjan Vanheusden 1 , Piet Stinissen 1 , Bert A. ’t Hart 2, 3 , and Niels Hellings 1 1 Hasselt University, Biomedical Research Institute and Transnationale Universiteit Limburg, School of Life Sciences, 3590 Diepenbeek, Belgium 2 Biomedical Primate Research Centre, Department of Immunobiology, Rijswijk, The Netherlands 3 University of Groningen, Department of Neuroscience, University Medical Center, Groningen, The Netherlands Multiple sclerosis (MS) is a chronic disabling autoim- mune disease of the central nervous system (CNS). Cytomegalovirus (CMV), a b herpes virus, may have a detrimental or beneficial role in MS pathology. Accumu- lating evidence indicates that CMV contributes to MS disease via interplay of different mechanisms such as molecular mimicry, bystander activation, and epitope spreading. The activation and expansion of a specific T cell subset, CD4 + CD28 null T cells, via CMV infection could also contribute to MS pathology. Various additional observations also indicate a protective effect of CMV on autoimmune diseases. CMV immune evasion may mitigate the autoimmune reactions and proinflamma- tory milieu that contribute to MS. Hurdles in CMV and MS research In this article we focus on cytomegalovirus (CMV), a mem- ber of the b herpes family that establishes lifelong latent infections in 70% of the human population [1]. CMV infection was considered ‘innocent’ in immunocompetent persons, but evidence is now emerging about the large impact of CMV infection on the aging immune system. In addition, the possible involvement of CMV in a wide range of diseases is now being recognized, including in autoimmune diseases such as multiple sclerosis (MS). MS is a chronic disabling autoimmune disease of the CNS (Box 1). Autoreactive immune cells attack the CNS myelin, leading to demyelination, axonal injury, and ulti- mately neural cell loss. A wide range of symptoms can occur, including fatigue, muscle weakness, and visual dif- ficulties. MS is often preceded by clinically isolated syn- drome (CIS), where patients experience a first episode of neurologic symptoms, such as optic neuritis, without a second event. Another disease, namely acute disseminated encephalomyelitis (ADEM), is clinically and pathologically similar to MS, and often manifests after an infection [2]. The role of CMV in MS disease is disputed. Our own research, together with that of others, supports a detrimen- tal role of CMV, where the virus contributes to MS patholo- gy, whereas others believe that CMV is disease-limiting. We discuss here viral mechanisms that are suggestive for promotion of autoimmunity and we summarize evidence arguing in favor of and against CMV involvement in MS etiology and progression. Possible mechanisms of viral contribution to autoimmune disease There are several different mechanisms by which viruses such as CMV could drive autoreactive T cell activation and thus lead to autoimmune disease (Figure 1). Two hypothe- ses rely on the fact that potentially autoreactive T cells are already present in low numbers in each individual. These cells seem to escape negative selection in the thymus during normal T cell development (see Glossary) [3,4]. Opinion Glossary Brain atrophy: decreased brain volume. In MS this is due to the loss of neurons and axons. Cryptic epitopes: self-epitopes that are not easily accessible to the immune system. T cells specific for these cryptic epitopes are present because they are not deleted in the thymus by negative selection, and might become activated in the periphery if these epitopes are made available via systemic release. Heterologous immunity: established immunity to previously encountered viruses can alter responses to unrelated pathogens, thereby impacting upon the course and outcome of this new infection. Heterologous immunity may be beneficial by boosting protective responses, but can also result in severe immunopathology. Immunosenescence: age-dependent decrease in immunological competence, due to the ongoing deterioration of innate and adaptive immune responses. Inbred/SPF laboratory mouse strains: inbred strains are created by inbreeding (brother sister mating) to achieve genetic homozygosity. Specific pathogen- free (SPF) animals are, as their name implies, not contaminated with specific pathogens (in contrast to conventional animals) because they are maintained in facilities that incorporate barriers to prevent contamination. Mitogen or superantigen: microbial proteins (from e.g., viruses, bacteria) that strongly stimulate immune cells without prior antigen processing. They elicit massive T cell activation and release of numerous cytokines, resulting in systemic shock (e.g., toxic shock syndrome). By activating autoreactive T cells, superantigens could contribute to autoimmunity. Negative selection of T cells: in the thymus, this process deletes T cells that bind strongly with self-peptides, by inducing apoptosis. Thus, negative selection prevents the formation of mature self-reactive T cells that are capable of inducing autoimmunity. Even so, not all autoreactive T cells are removed. Those T cells with weak binding capacities can bypass the selection process and are present in the periphery of each individual. Upon activation (e.g., during infection), these cells could cause an autoimmune reaction. Oligoclonal expansion: expansion of a limited number of T cell clones, thus strongly skewing the T cell receptor (TCR) and T cell repertoire. White and gray matter lesions: lesions most frequently occur in the white matter, including areas within the spinal cord, the brainstem, the periventricular white matter of the cerebrum, and the optic nerves. However, lesions also arise within the cortex (gray matter). Differences between white- and gray-matter lesions are the amount of inflammation and disruption of the cytoarchitecture, which occur to a far lesser extent in gray-matter lesions. Nevertheless, neuronal and axonal pathology also arise in these gray-matter lesions. 1471-4914/ ß 2014 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.molmed.2014. 11.002 Corresponding author: Hellings, N. ([email protected]). Keywords: cytomegalovirus; multiple sclerosis. 16 Trends in Molecular Medicine, January 2015, Vol. 21, No. 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cytomegalovirus: a culprit or protectorin multiple sclerosis?Marjan Vanheusden1, Piet Stinissen1, Bert A. ’t Hart2,3, and Niels Hellings1
1 Hasselt University, Biomedical Research Institute and Transnationale Universiteit Limburg, School of Life Sciences,
3590 Diepenbeek, Belgium2 Biomedical Primate Research Centre, Department of Immunobiology, Rijswijk, The Netherlands3 University of Groningen, Department of Neuroscience, University Medical Center, Groningen, The Netherlands
Opinion
Glossary
Brain atrophy: decreased brain volume. In MS this is due to the loss of neurons
and axons.
Cryptic epitopes: self-epitopes that are not easily accessible to the immune
system. T cells specific for these cryptic epitopes are present because they are
not deleted in the thymus by negative selection, and might become activated in
the periphery if these epitopes are made available via systemic release.
Heterologous immunity: established immunity to previously encountered
viruses can alter responses to unrelated pathogens, thereby impacting upon
the course and outcome of this new infection. Heterologous immunity may be
beneficial by boosting protective responses, but can also result in severe
immunopathology.
Immunosenescence: age-dependent decrease in immunological competence,
due to the ongoing deterioration of innate and adaptive immune responses.
Inbred/SPF laboratory mouse strains: inbred strains are created by inbreeding
(brother � sister mating) to achieve genetic homozygosity. Specific pathogen-
free (SPF) animals are, as their name implies, not contaminated with specific
pathogens (in contrast to conventional animals) because they are maintained
in facilities that incorporate barriers to prevent contamination.
Mitogen or superantigen: microbial proteins (from e.g., viruses, bacteria) that
strongly stimulate immune cells without prior antigen processing. They elicit
massive T cell activation and release of numerous cytokines, resulting in
systemic shock (e.g., toxic shock syndrome). By activating autoreactive T cells,
superantigens could contribute to autoimmunity.
Negative selection of T cells: in the thymus, this process deletes T cells that
bind strongly with self-peptides, by inducing apoptosis. Thus, negative
selection prevents the formation of mature self-reactive T cells that are capable
of inducing autoimmunity. Even so, not all autoreactive T cells are removed.
Those T cells with weak binding capacities can bypass the selection process
and are present in the periphery of each individual. Upon activation (e.g.,
during infection), these cells could cause an autoimmune reaction.
Oligoclonal expansion: expansion of a limited number of T cell clones, thus
strongly skewing the T cell receptor (TCR) and T cell repertoire.
Multiple sclerosis (MS) is a chronic disabling autoim-mune disease of the central nervous system (CNS).Cytomegalovirus (CMV), a b herpes virus, may have adetrimental or beneficial role in MS pathology. Accumu-lating evidence indicates that CMV contributes to MSdisease via interplay of different mechanisms such asmolecular mimicry, bystander activation, and epitopespreading. The activation and expansion of a specific Tcell subset, CD4+CD28null T cells, via CMV infection couldalso contribute to MS pathology. Various additionalobservations also indicate a protective effect of CMVon autoimmune diseases. CMV immune evasion maymitigate the autoimmune reactions and proinflamma-tory milieu that contribute to MS.
Hurdles in CMV and MS researchIn this article we focus on cytomegalovirus (CMV), a mem-ber of the b herpes family that establishes lifelong latentinfections in �70% of the human population [1]. CMVinfection was considered ‘innocent’ in immunocompetentpersons, but evidence is now emerging about the largeimpact of CMV infection on the aging immune system.In addition, the possible involvement of CMV in a widerange of diseases is now being recognized, including inautoimmune diseases such as multiple sclerosis (MS).
MS is a chronic disabling autoimmune disease of theCNS (Box 1). Autoreactive immune cells attack the CNSmyelin, leading to demyelination, axonal injury, and ulti-mately neural cell loss. A wide range of symptoms canoccur, including fatigue, muscle weakness, and visual dif-ficulties. MS is often preceded by clinically isolated syn-drome (CIS), where patients experience a first episode ofneurologic symptoms, such as optic neuritis, without asecond event. Another disease, namely acute disseminatedencephalomyelitis (ADEM), is clinically and pathologicallysimilar to MS, and often manifests after an infection [2].
The role of CMV in MS disease is disputed. Our ownresearch, together with that of others, supports a detrimen-tal role of CMV, where the virus contributes to MS patholo-gy, whereas others believe that CMV is disease-limiting.
1471-4914/
� 2014 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.molmed.2014.
11.002
Corresponding author: Hellings, N. ([email protected]).Keywords: cytomegalovirus; multiple sclerosis.
16 Trends in Molecular Medicine, January 2015, Vol. 21, No. 1
We discuss here viral mechanisms that are suggestive forpromotion of autoimmunity and we summarize evidencearguing in favor of and against CMV involvement in MSetiology and progression.
Possible mechanisms of viral contribution toautoimmune diseaseThere are several different mechanisms by which virusessuch as CMV could drive autoreactive T cell activation andthus lead to autoimmune disease (Figure 1). Two hypothe-ses rely on the fact that potentially autoreactive T cells arealready present in low numbers in each individual. Thesecells seem to escape negative selection in the thymusduring normal T cell development (see Glossary) [3,4].
White and gray matter lesions: lesions most frequently occur in the white
matter, including areas within the spinal cord, the brainstem, the periventricular
white matter of the cerebrum, and the optic nerves. However, lesions also arise
within the cortex (gray matter). Differences between white- and gray-matter
lesions are the amount of inflammation and disruption of the cytoarchitecture,
which occur to a far lesser extent in gray-matter lesions. Nevertheless, neuronal
and axonal pathology also arise in these gray-matter lesions.

Box 1. Disease course and types of MS
Patients often present to the clinic with a first episode of neurologic
symptoms, and are diagnosed with clinically isolated syndrome
(CIS) until a second event occurs. After this second event, the
McDonald criteria are fulfilled and the diagnosis is changed to
clinically definite MS. With this second event we imply either a
second clinical attack or secondary lesions that are disseminated in
time and space, established via MRI.
The majority of MS patients (85%) develop RRMS disease with a
duration ranging from several years to decades. In most patients,
the episodes of recovery (remissions) gradually become less
frequent and finally disappear completely, while their symptoms
become more pronounced and their disability worsens. At this stage
the disease converts to the secondary progressive (SP) phase.
In a minority of patients (10%), those with primary progressive MS
(PPMS), the disease is progressive from onset.
A relatively rare (5%) form of MS, progressive relapsing MS,
consists of steadily worsening of the disease, but also comprises
relapses. In some cases there is no recovery, although in other cases
there is. Thus the periods between relapses involve continuing
progression of the disease instead of remission as in RRMS.
The lesions in RRMS are usually located in the white matter
around ventricles and blood vessels, and are characterized by
sharply edged focal areas of inflammation with a variable degree of
demyelination, remyelination, and axonal injury. Lesions in pro-
gressive MS are also found in the gray matter and are characterized
by intensive demyelination with little inflammation but pronounced
degeneration of oligodendrocytes and neurons.
Opinion Trends in Molecular Medicine January 2015, Vol. 21, No. 1
One hypothesis suggests the direct triggering of auto-reactive T cells by infectious pathogens which expressantigenic epitopes that structurally resemble epitopes ofself-antigens [5]. A well-known example of this molecularmimicry is the T cell crossreaction between the MS relatedautoantigen myelin basic protein and Epstein–Barr virus(EBV) [6]. A second hypothesis, proposed by ‘t Hart et al., isa variation of the molecular mimicry paradigm, namely a‘delayed molecular mimicry’ model in which latent chronicinfections create a repertoire of long-living virus-specificmemory T cells. These cells can be reactivated at anymoment in time when they encounter molecular mimicrymotifs present in self-antigens that are shed from injuredtissues [7]. Another hypothesis entails bystander activa-tion, and comprises a variety of antigen-nonspecific theo-ries. First, cytokines produced by virus-specific immunecells could lead to the accidental activation of autoreactiveT cells. Second, host cell destruction by viral infection leadsto the release of cryptic epitopes, including self-antigensthat normally are not accessible to the immune system.Finally, a mitogen or superantigen, released from theinfectious pathogen, could lead to polyclonal lymphocyteactivation [3,8]. Thus, the inflammatory setting of a viralinfection could elicit the activation and clonal expansion ofautoreactive T cells, resulting in autoimmune disease[9]. McCoy et al. suggest a combination of both aforemen-tioned hypotheses: viral epitopes crossreact with self-anti-gens (molecular mimicry) to prime genetically susceptibleindividuals. After this priming a non-specific immunologicchallenge, leading to cytokine production (bystander ef-fect), could provoke autoimmunity [10].
Another process closely linked to molecular mimicryand bystander activation is epitope spreading. After theinitial reaction to a pathogen, antigens released from‘primary lesions’ in the target tissue will prime an
expanding range of potentially autoreactive T cells asa consequence of T cell receptor (TCR) diversity[11,12]. This cascade of self-recognition events providesa continuous inflammatory state that leads to chronicautoimmunity [13]. Delogu et al. suggest that the threeprocesses are linked, thus adding epitope spreading tothe McCoy et al. hypothesis. Molecular mimicry wouldoccur early in the development of autoimmunity, whereasbystander activation and epitope spreading occur lateron, exacerbating the autoimmune responses [9].
The hypotheses of ‘t Hart et al. and McCoy et al. alsocomply with the so-called ‘fertile field’ concept described byFujinami et al. [14]. The fertile field concept states thatexposure to a potential immunogen is normally withoutconsequence, but that under particular circumstances (e.g.,viral infection) the immunological environment changes,leading to a dysregulated immune reaction. Thus the viralinfection would create a fertile field in which immuneresponses to antigens could develop. Primed autoreactiveT cells (by viral infections) also create a fertile field becauselater events might trigger the expansion and activation ofthese cells leading to autoimmune disease.
Evidence in favor for the involvement of CMV in MSdiseaseThe interaction of environmental and genetic factors isthought to play a dominant role in the etiology of MS. It isenvisaged that some environmental factors (e.g., viruses)are potential triggers of the disease, while others (e.g.,vitamin D or smoking) may also influence the diseasecourse. Several observations support a viral trigger forMS or ADEM. Many viruses are associated with encepha-lomyelitis, axonal damage, and other demyelinating pro-cesses [15,16].
Animal models
Most animal models used in translational MS research arebased on inbred/SPF (specific pathogen free) laboratorystrains of mice and rats. A minority of the research is basedon non-human primates, man’s closest kin in nature.
Rodents. In several mouse models, viral infection elicitsan MS-like disease. Examples include Theiler’s murineencephalomyelitis virus (TMEV), mouse hepatitis virus(MHV), Semliki Forest virus (SFV), and canine distempervirus (CDV) (Box 2). These models provide compellingevidence for a possible viral cause, or at least as part ofthe multifactorial and complex etiology of MS [7,17].
One of the most convincing mechanisms via which CMVcould play a role in MS is molecular mimicry. Crossreac-tivity between hCMV981–1003 and myelin oligodendrocyteglycoprotein (MOG) residues 35–55 (MOG35–55) in Lewisrats was found [18]. Furthermore, sensitization of the ratsagainst MOG35–55 triggered CMV981–1003-specific lympho-cytes, leading to clonal expansion and migration towardsthe spleen. This study provides further evidence of the‘delayed molecular mimicry’ theory.
In another animal model, SJL/J mice were primed withvaccinia virus encoding proteolipid protein and were subse-quently challenged with murine CMV (mCMV) [14]. Thesemice developed white-matter lesions and had impaired
17
TRENDS in Molecular Medicine
(A) Molecular mimicry
CMV APC
Viral an�gens
Auto T cell
Auto T cell
(C) Epitope spreading
Auto T cell
Auto T cell Auto T cell
Auto T cellAPC
APC APC
Inflammatorymilieu
Myelinsheath
Self an�gens
Neuron
Secondaryself an�gens
Auto B cell
T cell CMV
CNS
(B) Bystander ac�va�on
An�bodies
Pro-inflammatorycytokines
B cell
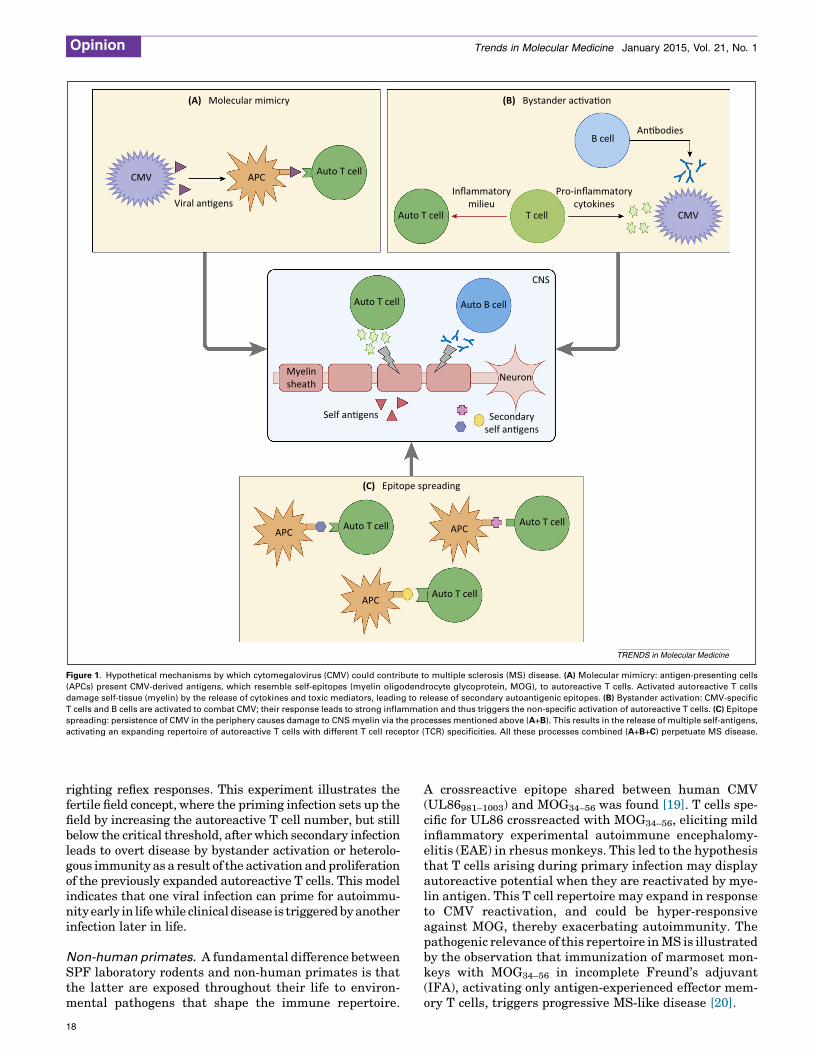
Figure 1. Hypothetical mechanisms by which cytomegalovirus (CMV) could contribute to multiple sclerosis (MS) disease. (A) Molecular mimicry: antigen-presenting cells
(APCs) present CMV-derived antigens, which resemble self-epitopes (myelin oligodendrocyte glycoprotein, MOG), to autoreactive T cells. Activated autoreactive T cells
damage self-tissue (myelin) by the release of cytokines and toxic mediators, leading to release of secondary autoantigenic epitopes. (B) Bystander activation: CMV-specific
T cells and B cells are activated to combat CMV; their response leads to strong inflammation and thus triggers the non-specific activation of autoreactive T cells. (C) Epitope
spreading: persistence of CMV in the periphery causes damage to CNS myelin via the processes mentioned above (A+B). This results in the release of multiple self-antigens,
activating an expanding repertoire of autoreactive T cells with different T cell receptor (TCR) specificities. All these processes combined (A+B+C) perpetuate MS disease.
Opinion Trends in Molecular Medicine January 2015, Vol. 21, No. 1
righting reflex responses. This experiment illustrates thefertile field concept, where the priming infection sets up thefield by increasing the autoreactive T cell number, but stillbelow the critical threshold, after which secondary infectionleads to overt disease by bystander activation or heterolo-gous immunity as a result of the activation and proliferationof the previously expanded autoreactive T cells. This modelindicates that one viral infection can prime for autoimmu-nity early in life while clinical disease is triggered by anotherinfection later in life.
Non-human primates. A fundamental difference betweenSPF laboratory rodents and non-human primates is thatthe latter are exposed throughout their life to environ-mental pathogens that shape the immune repertoire.
18
A crossreactive epitope shared between human CMV(UL86981–1003) and MOG34–56 was found [19]. T cells spe-cific for UL86 crossreacted with MOG34–56, eliciting mildinflammatory experimental autoimmune encephalomy-elitis (EAE) in rhesus monkeys. This led to the hypothesisthat T cells arising during primary infection may displayautoreactive potential when they are reactivated by mye-lin antigen. This T cell repertoire may expand in responseto CMV reactivation, and could be hyper-responsiveagainst MOG, thereby exacerbating autoimmunity. Thepathogenic relevance of this repertoire in MS is illustratedby the observation that immunization of marmoset mon-keys with MOG34–56 in incomplete Freund’s adjuvant(IFA), activating only antigen-experienced effector mem-ory T cells, triggers progressive MS-like disease [20].

Box 2. Viral animal models of MS
Many studies have examined the interaction between viruses and
immune-mediated CNS disease in vivo by inoculating mice with
different viral strains.
Theiler’s murine encephalomyelitis virus (TMEV)
TMEV, a single-stranded virus of the Picornaviridae family, is a natural
enteric mouse pathogen that can replicate and persist within the CNS.
Intracerebral injection of mice causes paralysis, encephalomyelitis,
and demyelination, a pathology similar to MS [61,62]. Some strains
cause a biphasic illness, starting with acute encephalomyelitis after
which a relapse can occur [63]. The chronic phase leads to slowly
progressive disability and consists of demyelination, remyelination,
inflammation, and axonal damage [64].
Mouse hepatitis virus (MHV)
MHV is a natural mouse pathogen that infects all cell types within
the CNS. Intracerebral or intranasal inoculation leads to a robust
immune response against CNS myelin, resulting in an influx of
immune cells that largely clear the virus, although low-level viral
infection persists. Infected mice develop a major symptomatic
episode with inflammation and demyelination of brain and spinal
cord leading to ataxia, hind-limb paresis, and paralysis [61,64].
Relapses can follow and lesion repair and remyelination may occur
[61,63].
Semliki Forest virus (SFV)
SFV is a neurotropic alphavirus or togavirus that induces a
demyelinating encephalomyelitis that is associated with the induc-
tion of T and B cell autoimmunity against CNS myelin. SFV is
inoculated in the periphery (intraperitoneally), but can cross the
BBB, infecting neurons and oligodendrocytes and inducing myelin
damage [62]. In mice, the virus is largely cleared from the CNS by
6 days post-infection, after which remyelination can take place [61].
Neurotropic strains of the canine distemper virus (CDV)
CDV is a single-stranded RNA morbillivirus which can cause
demyelinating leukoencephalitis in dogs and other carnivores.
Infection in dogs occurs mainly via the oro-nasal route, after which
infected immune cells can cross the BBB and cause CNS damage
[65]. Mice used in experiments are infected by intracranial injection.
The virus persists and leads to multifocal, inflammatory demyeli-
nating lesions similar to MS plaques [64].
Sindbis virus (SV)
SV is a togavirus or alphavirus. Mice infected intracerebrally with a
neuroadapted strain develop acute encephalomyelitis, experimental
autoimmune encephalomyelitis (EAE)-like paralysis, and demyeli-
nation [61,66].
Opinion Trends in Molecular Medicine January 2015, Vol. 21, No. 1
Human studies
CMV causes a chronic latent infection that can be reacti-vated under conditions of inflammation or reduced immu-nity as a result of stress, medication, or pregnancy. Thispattern of latency and reactivation resembles, and maytherefore underlie, the relapsing–remitting form of MS(RRMS) [15]. MS relapses are often associated with commonviral infections [21]. Furthermore, long-acting viruses, suchas CMV, could encourage modest immunological changes,eventually resulting in autoimmune demyelination [22].
The most prevalent exposure routes to CMV are sexualcontact or contact with urine or saliva from infected per-sons. CMV mainly targets cells of the myeloid lineage (e.g.,macrophages, dendritic cells) and replicates in the sali-vary glands and in brain tissue [15]. The virus can crossthe blood–brain barrier (BBB) directly or indirectly as aviral load in cells [22]. Because CMV is present in the CNS,it could damage local cells and tissues [15]. Indeed, CMVhas been found in demyelinating plaques and the cerebro-spinal fluid (CSF) of MS patients [16,22], and causes
demyelination mainly in the CNS of immunocompromisedhosts [7,17]. Moreover, enrichment of EBV- and CMV-specific CD8+ T cells among T cells isolated from chronicinflammatory lesions of MS brain was reported [23].
Epidemiological studies. Epidemiological data support-ing a role of CMV in MS pathology are scarce. It wasshown that that CMV DNA and CMV-specific IgG anti-body titers are higher in MS patients compared to healthycontrols, indicating a role of CMV in MS [21]. Otherresearchers investigated a cohort of CIS patients, andfound that CMV seropositivity was associated with re-duced time to relapse and a higher number of relapses.CMV seropositivity was further associated with progres-sion to clinically definite MS [24,25]. Another study per-formed on the same cohort of CIS patients found thatanti-CMV positivity was associated with greater totaldeep gray-matter atrophy and whole-brain atrophy[26]. Newly diagnosed MS patients were examined viaserological testing for a panel of viruses including CMV[22]. They found that early CMV infection occurred in86% of the MS patients, indicating that early CMV infec-tions may affect the development of MS.
CMV infection and disease exacerbations. Many viralinfections are associated with exacerbations of MS[10]. Disease exacerbations in RRMS patients occur 2–3-fold more frequently during or immediately after a viralinfection [27,28].
CMV infection has also been implicated in worsening ofautoimmune diseases or in the progression of ADEM toclinically definite MS [16]. CMV infection leads to celldeath and could therefore enhance autoimmunity as aresult of the release of self-antigen from degeneratingtissue [8]. Reactivation of CMV during ongoing MS couldtrigger the release of free virus in interstitial and cerebralfluids of the CNS. It is possible that autoreactive T cells(molecular mimicry) will migrate towards this regionand induce demyelination. Our own research suggeststhat CMV exacerbation may indirectly lead to diseaseaggravation by the induction or expansion of cytotoxicCD4+CD28null T cells via repeated antigenic stimulation[29]. These cells have an inflammation-seeking/proinflam-matory effector-memory phenotype and are attracted toMS lesions via a fractalkine gradient [30,31]. Furthermore,at least a subpopulation of CD4+CD28null T cells proliferateand expel cytotoxic granules upon stimulation withMS-related autoantigens, and may therefore contributeto MS pathology [32,33]. The fact that CD4+CD28null Tcells are mostly found in CMV-seropositive persons [34]hints at the involvement of CMV in the expansion of thisoligoclonal subpopulation. Indeed, primary infection withCMV induces brisk expansion of CD4+CD28null T cells, buttheir appearance in the peripheral blood occurs only aftercessation of viral replication [35].
Evidence contra CMV involvement in MSOther studies are indicative for a protective effect of CMVon autoimmune diseases. CMV infection is associated withanti-inflammatory activities, which could lead to a lesssevere course of the disease [8]. Furthermore, CMV
19

Box 3. Immune-evasion mechanisms of CMV
Particular viruses have devised ways to evade the host immune
system, allowing them to replicate, disseminate and persist
throughout life, occasionally reactivating but mostly being latently
present. CMV commits a large portion of its genome to modulating
recognition by the immune system. It encodes multiple immune-
evasion proteins during the course of infection that target different
arms of the immune system [67,68].
Adaptive immunity
Expression of major histocompatibility complex (MHC) class I or II
molecules on the surface of CMV-infected cells is downregulated,
reducing antigen presentation [68]. MHC class I molecules are
degraded or retained in the endoplasmic reticulum by various viral
proteins [1,67]. MHC class II molecules are also degraded, and their
upregulation is disrupted by CMV-specific genes [67]. In addition, a
viral homolog of the immunomodulatory cytokine interleukin 10 (IL-
10), which is expressed during latency, has been shown to down-
regulate expression of MHC class I and II molecules, inhibit
proliferation of peripheral blood mononuclear cells, and inhibit the
production of inflammatory cytokines [67].
Innate immunity
The lack of surface MHC class I molecules makes the infected cell
prone to lysis by natural killer (NK) cells. However, CMV can evade NK
cell lysis by expressing MHC class I homologs, or by upregulating
expression of the host HLA-E which binds to an inhibitory NK
receptor. Thus, infected cells escape detection and subsequent lysis
by NK cells. Furthermore, CMV glycoproteins can directly bind to and
sequester NK-activating ligands, minimizing their surface expression
and preventing activating NK receptor signaling [67,68]. In addition,
selective, allele-specific degradation of MHC class I leads to protection
against both CTL-mediated and NK-mediated cell lysis [68]. Another
strategy of CMV immune evasion may be to restrict the differentiation
of CD34+ progenitor cells to dendritic cells (DCs), which are potent
antigen-presenting cells (APCs) [1,68].
Opinion Trends in Molecular Medicine January 2015, Vol. 21, No. 1
encodes multiple factors that trigger immunomodulatoryor evasion mechanisms (Box 3), which can decrease theimmune response in MS patients [21,36].
Animal models
In the TMEV mouse model of MS, mCMV infection 2 weeksbefore TMEV infection leads to a better disease outcomecompared to TMEV alone. These mice showed better motorperformance, and less T cell infiltration in the brain,suggesting an immunomodulatory effect of mCMV infec-tion in the TMEV model [36]. It should be noted that onlythe brain and not spinal cord tissue was examined, andTMEV is present in both compartments, which could havebiased the results.
Human studies
An association between CMV-specific antibody titers andbetter clinical outcome was observed in a cohort of 140 MSpatients. CMV-positive MS patients had a higher age atdisease onset, and displayed less brain atrophy as mea-sured by magnetic resonance imaging (MRI) [37]. A case–control study comparing Swedish MS patients and healthycontrols with reported data via meta-analysis indicatedthat CMV positivity reduces the risk of developing MS[38]. It should be noted that this effect was only seen in themeta-analysis of the retrospective studies, and that onlytwo of 11 studies were significantly associated with MS,rendering the overall statistical value insignificant. Thedisadvantage of such retrospective studies is the time
20
interval between onset of symptoms and collection of se-rum sample for virus analysis. In the Swedish study themean time-interval was 5 years, during which timepatients could have seroconverted. This can obviouslyinfluence the results.
The possible involvement of CMV in pediatric MS in acohort of early pediatric MS patients and age-matchedcontrol subjects was analyzed. It was observed thatCMV infection acquired during childhood reduced the riskof developing MS or CIS in subjects up to 18 years of age.However, the control group comprised, next to healthyindividuals, ADEM patients and patients with other neu-rological conditions, which could have biased their findings[39].
The relationship between aging and CMV, and thetransition to progressive MSThe biological factor that is most strongly associated withprogressive MS is age. This notion has led to the hypothesisthat age-associated changes in the immune system, aphenomenon known as immunosenescence, may underliethe conversion of RRMS to progressive disease [40]. Ofparticular relevance are herpes viruses causing lifelongchronic latent infection, such as CMV and EBV. Observa-tions in the aging immune system illustrate the substan-tial impact that these viruses, in particular CMV, have onthe immune repertoire [41–43]. For current knowledge onhow CMV impacts upon immune aging see [44]. As aconceptual basis, we propose the existence of two distinctcompartments in the immune repertoire: an outward-di-rected compartment that deals with pathogens outside thebody, and an inward-directed compartment that deals withpathogens inside the body. Studies in the extremely old(>90 years) show decreased immunocompetence of theoutward compartment, impairing the response to vaccina-tion, while the inward compartment displays oligoclonalexpansion of highly reactive T cell specificities (Figure 2)[45]. This oligoclonal expansion combined with a decreasein age-dependent thymic output results in a dysregulationof the total T cell compartment, and thus may underlie theage-associated development of chronic inflammation inautoimmune disorders such as MS and rheumatoid arthri-tis (RA) [40].
The main cause of progressive MS is thought to be theaccumulating degeneration of neurons and oligodendro-cytes, and this may not have an immunological basis.Indeed, in contrast to lesions in the white matter, T cellsand antibody deposition is rare in gray-matter lesions.However, activation of microglia and the presence of im-mune cell infiltrates in adjacent meninges is prominent[46]. The presence of T cell and macrophage infiltrates isonly evident in early but not chronic gray-matter lesions[47], suggesting a role of the immune system during arestricted episode in progressive disease.
A new EAE model in marmosets has now been devel-oped, which is induced by immunization with MOG34–56 inIFA [20]. The model shares essential pathological charac-teristics with progressive MS that are not present in RRMS[48,49], including prominent demyelination of the corticalgray matter [50,51] and the expression of markers formitochondrial dysfunction (our unpublished observations).

Box 4. Outstanding questions
� Which exact mechanisms underlie the role of viruses in auto-
immune diseases? How do viruses contribute to the development
or exacerbation of autoimmune diseases?
� Is CMV involved in MS disease? If so, does it have a positive or
negative influence on MS disease?
� Which in vivo model would be the best to study the role of CMV in
MS?
Ado
lesc
ent
Middle-aged/old
Inward
OutwardVery old
TRENDS in Molecular Medicine
Figure 2. Changes in two distinct immune repertoire compartments throughout
life. The pathogen-educated immune system deals with pathogens in the
environment and those causing chronic latent infections (indicated by ).
Studies in aging individuals show that distinct immune compartments may be
involved in the defense against these outward and inward threats. Inflation of the
outward compartment (blue ring) impairs the capacity of elderly to respond
against vaccination. By contrast, the inward compartment (yellow ring) is
characterized by oligoclonal expansion of immune specificities against chronic
latent infections. The differently sized balls represent clones of different specificity.
Based on studies in the non-human primate we hypothesize that T cells driving
chronic inflammation (red color) are recruited from this inward compartment [45].
Opinion Trends in Molecular Medicine January 2015, Vol. 21, No. 1
Unraveling the immunopathogenic process that gives riseto MS-like pathology and disease in this model revealed acentral role of CD3+CD56+CD28� cytotoxic T cells, whichspecifically recognize a mimicry motif shared betweenMOG and UL86 (CMV peptide) [19,50]. A similar type ofT cell is present in the human anti-CMV repertoire [52]and in MS lesions [53]. Cytotoxic T lymphocytes (CTLs)depend on presentation of their specific antigen from Bcells infected with lymphocryptovirus (LCV), a subgroup ofprimate-specific g-herpes viruses of which EBV is thehuman representative. Thus, development of the pri-mate-specific autoimmune pathway requires the involve-ment of at least two herpes viruses, both of which havebeen implicated in MS-like disease [40]. Conceptually,chronic latent infection with CMV creates a progressivelyexpanding repertoire of CTLs, which display their enceph-alitogenic potency when they encounter MOG released byprimary demyelination of CNS lesions. LCV infection pre-sumably renders B cells capable of activating these strong-ly pathogenic T cells [54].
Concluding remarksThe role of CMV in MS pathology remains controversial,and may be detrimental or beneficial (Box 4). A recentmeta-analysis on 1341 MS patients and 2042 healthy con-trols did not yield a conclusive result on the relationshipbetween CMV infection and the occurrence of MS becauseno significantly enhanced risk (expressed as an odds ratio)was found [55]. Further studies are warranted to define arole of CMV as either culprit or protector. Future studies
should take into account the different forms and stages ofMS-like diseases, as well as the age of onset. The marmosetmodel suggests that CMV may have a stronger impactduring late-stage disease than in the early phase. Further-more, the epidemiologic studies should be interpreted withcare because they have some limitations. Owing to (possi-bly rapid) changes in the health and environmental statusof some subjects (e.g., viral infections), the conclusionsderived from previous analyses may not reflect the actualstatus (e.g., viral titers or status). Furthermore, case–control studies may prove an association, but they donot demonstrate causation. Retrospective studies shouldbe examined critically because they could be influenced byconfounding factors and bias due to missing or unknowninformation.
We strongly believe that CMV plays a role in MSpathology and disease progression; however, CMV infec-tion or reactivation by itself is not sufficient to induce MSdisease. The combined effects of CMV infection with ge-netic and immune triggers should be investigated in fur-ther detail. It has already been shown that the synergy ofviral (e.g., herpes simplex virus 1) and immune triggerscan elicit MS-like pathology, while the virus alone had noeffect [56]. Furthermore, EAE induction combined withviral infection accelerated or exacerbated disease as aresult of enhanced immune cell infiltration and polariza-tion of the adaptive immune response [27,57,58]. Next tothese triggers, another virus implicated in MS disease,such as EBV, could also play an added role. In marmosetEAE, EBV and CMV are both necessary for the develop-ment of the primate-specific autoimmune pathway, asalready discussed. In humans, seropositivity for CMVand EBV is associated with significantly increasedwhole-brain atrophy [24].
Because we reason that CMV plays a role in MS disease,we propose that vaccine or antiviral drug strategies tomanage CMV responses should be taken into considerationas part of managing MS patients. These benefits mayextend beyond MS because CMV infection is also implicat-ed in arteriosclerosis, vascular disease, and immune aging[44,59,60].
References1 Hanley, P.J. and Bollard, C.M. (2014) Controlling cytomegalovirus:
helping the immune system take the lead. Viruses 6, 2242–22582 Karussis, D. (2014) The diagnosis of multiple sclerosis and the various
related demyelinating syndromes: a critical review. J. Autoimmun. 48–49, 134–142
3 Benoist, C. and Mathis, D. (2001) Autoimmunity provoked by infection:how good is the case for T cell epitope mimicry? Nat. Immunol. 2, 797–801
4 Enouz, S. et al. (2012) Autoreactive T cells bypass negative selectionand respond to self-antigen stimulation during infection. J. Exp. Med.209, 1769–1779
21

Opinion Trends in Molecular Medicine January 2015, Vol. 21, No. 1
5 Fujinami, R.S. et al. (1983) Molecular mimicry in virus infection:crossreaction of measles virus phosphoprotein or of herpes simplexvirus protein with human intermediate filaments. Proc. Natl. Acad.Sci. U.S.A. 80, 2346–2350
6 Lang, H.L. et al. (2002) A functional and structural basis for TCR cross-reactivity in multiple sclerosis. Nat. Immunol. 3, 940–943
7 ‘t Hart, B.A. et al. (2009) Multiple sclerosis – a response-to-damagemodel. Trends Mol. Med. 15, 235–244
8 Halenius, A. and Hengel, H. (2014) Human cytomegalovirus andautoimmune disease. Biomed. Res. Int. 2014, 472978
9 Delogu, L.G. et al. (2011) Infectious diseases and autoimmunity. J.Infect. Dev. Ctries 5, 679–687
10 McCoy, L. et al. (2006) Multiple sclerosis and virus induced immuneresponses: autoimmunity can be primed by molecular mimicry andaugmented by bystander activation. Autoimmunity 39, 9–19
11 Tuohy, V.K. et al. (1999) Regression and spreading of self-recognitionduring the development of autoimmune demyelinating disease. J.Autoimmun. 13, 11–20
12 Wilkin, T. (1989) Autoimmunity: attack, or defence? (The case for aprimary lesion theory). Autoimmunity 3, 57–73
13 Tuohy, V.K. and Kinkel, R.P. (2000) Epitope spreading: a mechanismfor progression of autoimmune disease. Arch. Immunol. Ther. Exp.(Warsz) 48, 347–351
14 Fujinami, R.S. et al. (2006) Molecular mimicry, bystander activation, orviral persistence: infections and autoimmune disease. Clin. Microbiol.Rev. 19, 80–94
15 Olival, G.S. et al. (2013) Multiple sclerosis and herpesvirus interaction.Arq. Neuropsiquiatr. 71, 727–730
16 Smyk, D.S. et al. (2014) Acute disseminated encephalomyelitisprogressing to multiple sclerosis: are infectious triggers involved?Immunol. Res. 60, 16–22
17 Cermelli, C. and Jacobson, S. (2000) Viruses and multiple sclerosis.Viral Immunol. 13, 255–267
18 Zheng, M.M. and Zhang, X.H. (2014) Cross-reactivity between humancytomegalovirus peptide 981–1003 and myelin oligodendrogliaglycoprotein peptide 35–55 in experimental autoimmuneencephalomyelitis in Lewis rats. Biochem. Biophys. Res. Commun.443, 1118–1123
19 Brok, H.P. et al. (2007) The human CMV-UL86 peptide 981–1003shares a crossreactive T-cell epitope with the encephalitogenic MOGpeptide 34–56, but lacks the capacity to induce EAE in rhesusmonkeys. J. Neuroimmunol. 182, 135–152
20 Jagessar, S.A. et al. (2010) Induction of progressive demyelinatingautoimmune encephalomyelitis in common marmoset monkeys usingMOG34-56 peptide in incomplete freund adjuvant. J. Neuropathol. Exp.Neurol. 69, 372–385
21 Sanadgol, N. et al. (2011) Prevalence of cytomegalovirus infection andits role in total immunoglobulin pattern in Iranian patients withdifferent subtypes of multiple sclerosis. New Microbiol. 34, 263–274
22 Djelilovic-Vranic, J. and Alajbegovic, A. (2012) Role of early viralinfections in development of multiple sclerosis. Med. Arch. 66, 37–40
23 Scotet, E. et al. (1999) Frequent enrichment for CD8 T cells reactiveagainst common herpes viruses in chronic inflammatory lesions:towards a reassessment of the physiopathological significance of Tcell clonal expansions found in autoimmune inflammatory processes.Eur. J. Immunol. 29, 973–985
24 Horakova, D. et al. (2013) Environmental factors associated withdisease progression after the first demyelinating event: results fromthe multi-center SET study. PLoS ONE 8, e53996
25 Weinstock-Guttman, B. et al. (2013) Interactions of serum cholesterolwith anti-herpesvirus responses affect disease progression in clinicallyisolated syndromes. J. Neuroimmunol. 263, 121–127
26 Zivadinov, R. et al. (2014) Humoral responses to herpesviruses areassociated with neurodegeneration after a demyelinating event:results from the multi-center set study. J. Neuroimmunol. 273, 58–64
27 Rainey-Barger, E.K. et al. (2013) Virus-induced CD8+ T cells acceleratethe onset of experimental autoimmune encephalomyelitis: implicationsfor how viral infections might trigger multiple sclerosis exacerbations. J.Neuroimmunol. 259, 47–54
28 Buljevac, D. et al. (2002) Prospective study on the relationship betweeninfections and multiple sclerosis exacerbations. Brain 125, 952–960
29 Thewissen, M. and Stinissen, P. (2008) New concepts on thepathogenesis of autoimmune diseases: a role for immune homeostasis,
22
immunoregulation, and immunosenescence. Crit. Rev. Immunol. 28,363–376
30 Broux, B. et al. (2012) CX(3)CR1 drives cytotoxic CD4+CD28� T cellsinto the brain of multiple sclerosis patients. J. Autoimmun. 38,10–19
31 Pinto-Medel, M.J. et al. (2012) The CD4+T-cell subset lacking expressionof the CD28 costimulatory molecule is expanded and shows a higheractivation state in multiple sclerosis. J. Neuroimmunol. 243, 1–11
32 Broux, B. et al. (2012) Pathogenic features of CD4+CD28� T cells inimmune disorders. Trends Mol. Med. 18, 446–453
33 Markovic-Plese, S. et al. (2001) CD4+CD28� costimulation-independent T cells in multiple sclerosis. J. Clin. Invest. 108,1185–1194
34 Thewissen, M. et al. (2007) CD4+CD28null T cells in autoimmune disease:pathogenic features and decreased susceptibility to immunoregulation.J. Immunol. 179, 6514–6523
35 van Leeuwen, E.M. et al. (2004) Emergence of a CD4+CD28� granzymeB+, cytomegalovirus-specific T cell subset after recovery of primarycytomegalovirus infection. J. Immunol. 173, 1834–1841
36 Pirko, I. et al. (2012) CMV infection attenuates the disease course in amurine model of multiple sclerosis. PLoS ONE 7, e32767
37 Zivadinov, R. et al. (2006) Positivity of cytomegalovirus antibodiespredicts a better clinical and radiological outcome in multiplesclerosis patients. Neurol. Res. 28, 262–269
38 Sundqvist, E. et al. (2014) Cytomegalovirus seropositivity is negativelyassociated with multiple sclerosis. Mult. Scler. 20, 165–173
39 Waubant, E. et al. (2011) Common viruses associated with lowerpediatric multiple sclerosis risk. Neurology 76, 1989–1995
40 ‘t Hart, B.A. et al. (2013) Chronic autoimmune-mediated inflammation:a senescent immune response to injury. Drug. Discov. Today 18,372–379
41 Cicin-Sain, L. et al. (2011) Cytomegalovirus-specific T cell immunity ismaintained in immunosenescent rhesus macaques. J. Immunol. 187,1722–1732
42 Sylwester, A.W. et al. (2005) Broadly targeted human cytomegalovirus-specific CD4+ and CD8+ T cells dominate the memory compartments ofexposed subjects. J. Exp. Med. 202, 673–685
43 Willis, E.L. et al. (2014) The effects of age and cytomegalovirus onmarkers of inflammation and lymphocyte populations in captivebaboons. PLoS ONE 9, e107167
44 Sansoni, P. et al. (2014) New advances in CMV and immunosenescence.Exp. Gerontol. 55, 54–62
45 ‘t Hart, B.A. et al. (2014) Improvement of preclinical animal models forautoimmune-mediated disorders via reverse translation of failedtherapies. Drug. Discov. Today 19, 1394–1401
46 Popescu, B.F. and Lucchinetti, C.F. (2012) Meningeal and cortical greymatter pathology in multiple sclerosis. BMC Neurol. 12, 11
47 Lucchinetti, C.F. et al. (2011) Inflammatory cortical demyelination inearly multiple sclerosis. N. Engl. J. Med. 365, 2188–2197
48 Bradl, M. and Lassmann, H. (2009) Progressive multiple sclerosis.Semin. Immunopathol. 31, 455–465
49 Lassmann, H. et al. (2012) Progressive multiple sclerosis: pathologyand pathogenesis. Nat. Rev. Neurol. 8, 647–656
50 Jagessar, S.A. et al. (2012) Unravelling the T-cell-mediatedautoimmune attack on CNS myelin in a new primate EAE modelinduced with MOG34-56 peptide in incomplete adjuvant. Eur. J.Immunol. 42, 217–227
51 Kap, Y.S. et al. (2011) Effects of early IL-17A neutralization on diseaseinduction in a primate model of experimental autoimmuneencephalomyelitis. J. Neuroimmune Pharmacol. 6, 341–353
52 Mazzarino, P. et al. (2005) Identification of effector-memory CMV-specific T lymphocytes that kill CMV-infected target cells in anHLA-E-restricted fashion. Eur. J. Immunol. 35, 3240–3247
53 Zaguia, F. et al. (2013) Cytotoxic NKG2C+ CD4 T cells targetoligodendrocytes in multiple sclerosis. J. Immunol. 190, 2510–2518
54 ‘t Hart, B.A. et al. (2013) The primate EAE model points at EBV-infected B cells as a preferential therapy target in multiple sclerosis.Front. Immunol. 4, 145
55 Pakpoor, J. et al. (2013) Cytomegalovirus and multiple sclerosis risk. J.Neurol. 260, 1658–1660
56 Dumitrascu, O.M. et al. (2014) A comparative study of experimentalmouse models of central nervous system demyelination. Gene Ther. 21,599–608

Opinion Trends in Molecular Medicine January 2015, Vol. 21, No. 1
57 Casiraghi, C. et al. (2012) Gammaherpesvirus latency accentuatesEAE pathogenesis: relevance to Epstein–Barr virus and multiplesclerosis. PLoS Pathog. 8, e1002715
58 Jerusalmi, A. et al. (2003) Effect of intranasal administration ofSemliki Forest virus recombinant particles expressing reporter andcytokine genes on the progression of experimental autoimmuneencephalomyelitis. Mol. Ther. 8, 886–894
59 Cheng, J. et al. (2009) Cytomegalovirus infection causes an increase ofarterial blood pressure. PLoS Pathog. 5, e1000427
60 Nerheim, P.L. et al. (2004) Enhanced cytomegalovirus infectionin atherosclerotic human blood vessels. Am. J. Pathol. 164,589–600
61 Mecha, M. et al. (2013) Viral models of multiple sclerosis:neurodegeneration and demyelination in mice infected withTheiler’s virus. Prog. Neurobiol. 101–102, 46–64
62 van der Star, B.J. et al. (2012) In vitro and in vivo models of multiplesclerosis. CNS Neurol. Disord. Drug Targets 11, 570–588
63 Tselis, A. (2011) Evidence for viral etiology of multiple sclerosis. Semin.Neurol. 31, 307–316
64 Pachner, A.R. (2011) Experimental models of multiple sclerosis. Curr.Opin. Neurol. 24, 291–299
65 Lempp, C. et al. (2014) New aspects of the pathogenesis of caninedistemper leukoencephalitis. Viruses 6, 2571–2601
66 Irani, D.N. and Prow, N.A. (2007) Neuroprotective interventionstargeting detrimental host immune responses protect mice fromfatal alphavirus encephalitis. J. Neuropathol. Exp. Neurol. 66, 533–544
67 Jackson, S.E. et al. (2011) Human cytomegalovirus immunity andimmune evasion. Virus Res. 157, 151–160
68 Noriega, V. et al. (2012) Diverse immune evasion strategies by humancytomegalovirus. Immunol. Res. 54, 140–151
23
Related Documents







![The Culprit [2]](https://static.cupdf.com/doc/110x72/56816247550346895dd28534/the-culprit-2.jpg)



