Cyclooxygenase-pathway participates in the regulation of regional cerebral blood flow in response to neuronal activation under normo- and hypercapnia R. A. Bakalova,T. Matsuura, I. Kanno Department of Radiology and Nuclear Medicine, Research Institute for Brain and Blood Vessels, Senshu-Kubota-Machi, Akita, Japan Summary The present study was designed to investigate whether cyclooxygenase products are involved in the regulation of the regional cerebral blood flow, evoked by somatosensory activation (evoked rCBF) under normo- and hypercapnia. Indomethacin (IMC) was used as cyclooxygenase inhibitor. It was applied intravenously (i.v.,10 mg/kg/h) in two experimental protocolsFbefore hypercapnia (i) and after hypercapnia (ii). Somatosensory activation was induced by electrical hind paw stimulation (5 Hz frequency, 5 s duration,1.5 mA).The evoked rCBF-response was measured in a-chloralose anesthetized rats using laser-Doppler flowmetry. IMC abolished completely the effect of hypercapnia on the baseline level of CBF.The drug reduced significantly evoked rCBF-response also.The inhibitory effect of IMC on evoked rCBF-response is better expressed under normocapnia (B70%) than that under hypercapnia (B40%). After IMC application, the normalized evoked rCBF curves peaked earlier as compared to that before its application (Po0.05), although the rise time of 0.5 s was nearly constant regardless of stimulus frequency. In conclusion, the results suggest a participation of IMC-sensitive and cyclooxygenase-dependent mechanisms in the regulation of evoked rCBF, induced by somatosensory stimulation. & 2002 Elsevier Science Ltd. All rights reserved. INTRODUCTION Two powerful physiological regulators of the cerebral circulation are described in norm. 1–3 K arterial CO 2 tension (PaCO 2 )Fa regulator of cerebral blood flow (CBF) at rest condition; and K neuronal activityFa regulator of CBF in discreetly activated regions of the cortex (rCBF) and thus providing energy metabolites for neurotransmission. Fundamental aspect of brain physiology are the mechanisms of coupling between regional neuronal activation and changes in rCBF, as well as between carbon dioxide tension and cerebrovascular tone at rest. Both coupling processes are highly complicated and include the combined action of many biochemical mediators. In relation to coupling between PaCO 2 and CBF, there is a commonly accepted hypothesis. Recent evidences suggest that one of the major mechanisms, underlying the hypercapnia-induced cerebrovascular vasodilation, is endothelium-derived and involves the following cascade of contiguous biochemical reactions (Scheme 1): 4,5 acti- vation of phospholipase A 2 and free arachidonate production, activation of cyclooxygenase (COX) and prostanoid synthesis, activation of adenylate and guany- late cyclases and formation of cyclic nucleotides (cAMP, cGMP), modulation of ion channels and smooth muscle relaxation. It is accepted that CO 2 ventilation causes not only an induction of COX-dependent cascade, but also nitric oxide (NO)-dependent cascade. 4–6 Some authors suppose that both cascades interact each other. 4,5 Probably, they are two alternative links from one and Prostaglandins, Leukotrienes and Essential Fatty Acids (2002) 67(6), 379^388 & 2002 Elsevier Science Ltd. All rights reserved. doi:10.1054/plef.2002.0445, available online at http://www.idealibrary.com on Correspondence to : Rumiana Bakalova, PhD, Natural Substance-Composed Materials Group, Institute for Structural and Engineering Materials, Independent Administrative Institution, National Institute of Advanced Industrial Science and Technology, Kyushu, 807-1, Shuku,Tosu, Saga-ken 841- 0052, Japan.Tel.: +81-942-81-3628; Fax: +81-942-81-3690; E-mail: [email protected] Received 11 January 2002 Accepted 4 July 2002 & 2002 Elsevier Science Ltd. All rights reserved. Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^388

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^388& 2002 Elsevier Science Ltd. All rights reserved.doi:10.1054/plef.2002.0445, availableonlineathttp://www.idealibrary.comon
Cyclooxygenase-pathway participatesin the regulation of regional cerebralblood flow in response to neuronalactivation under normo- andhypercapnia
R. A. Bakalova,T. Matsuura, I. Kanno
Department of Radiologyand Nuclear Medicine,Research Institute for Brain and Blood Vessels, Senshu-Kubota-Machi, Akita, Japan
Summary Thepresent study wasdesigned to investigatewhether cyclooxygenaseproducts are involved in the regulationof the regional cerebralblood flow, evokedby somatosensoryactivation (evoked rCBF) under normo- andhypercapnia.Indomethacin (IMC) wasusedas cyclooxygenase inhibitor. It wasapplied intravenously (i.v.,10mg/kg/h) in two experimentalprotocolsFbeforehypercapnia (i) andafter hypercapnia (ii). Somatosensoryactivationwas inducedbyelectricalhindpawstimulation (5 Hz frequency, 5 s duration,1.5 mA).The evoked rCBF-responsewasmeasured in a-chloraloseanesthetized ratsusinglaser-Doppler flowmetry. IMCabolished completely the effect of hypercapniaon thebaseline levelof CBF.The drugreducedsignificantlyevokedrCBF-responsealso.The inhibitoryeffect of IMConevokedrCBF-response isbetterexpressedundernormocapnia (B70%) than that underhypercapnia (B40%).After IMCapplication, thenormalizedevokedrCBFcurvespeakedearlierascompared to that before itsapplication (Po0.05), although therise timeof 0.5 swasnearlyconstant regardlessof stimulusfrequency.In conclusion, the results suggest a participationof IMC-sensitiveand cyclooxygenase-dependentmechanismsin theregulationof evokedrCBF, inducedby somatosensory stimulation. & 2002 Elsevier Science Ltd.All rights reserved.
INTRODUCTION
Two powerful physiological regulators of the cerebralcirculation are described in norm.1–3
K arterial CO2 tension (PaCO2)Fa regulator of cerebralblood flow (CBF) at rest condition; and
K neuronal activityFa regulator of CBF in discreetlyactivated regions of the cortex (rCBF) and thusproviding energy metabolites for neurotransmission.
Fundamental aspect of brain physiology are themechanisms of coupling between regional neuronal
Correspondence to:Rumiana Bakalova,PhD,Natural Substance-ComposedMaterials Group, Institute for Structural and Engineering Materials,Independent Administrative Institution,National Institute of AdvancedIndustrial Science and Technology,Kyushu, 807-1, Shuku,Tosu,Saga-ken 841-0052, Japan.Tel.: +81-942-81-3628; Fax: +81-942-81-3690;E-mail: [email protected]
Received 11January 2002Accepted 4 July 2002
& 2002 Elsevier Science Ltd. All rights reserved. Prost
activation and changes in rCBF, as well as between carbondioxide tension and cerebrovascular tone at rest. Bothcoupling processes are highly complicated and includethe combined action of many biochemical mediators.
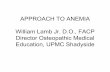
In relation to coupling between PaCO2 and CBF, thereis a commonly accepted hypothesis. Recent evidencessuggest that one of the major mechanisms, underlyingthe hypercapnia-induced cerebrovascular vasodilation, isendothelium-derived and involves the following cascadeof contiguous biochemical reactions (Scheme 1):4,5 acti-vation of phospholipase A2 and free arachidonateproduction, activation of cyclooxygenase (COX) andprostanoid synthesis, activation of adenylate and guany-late cyclases and formation of cyclic nucleotides (cAMP,cGMP), modulation of ion channels and smooth musclerelaxation. It is accepted that CO2 ventilation causes notonly an induction of COX-dependent cascade, but alsonitric oxide (NO)-dependent cascade.4–6 Some authorssuppose that both cascades interact each other.4,5
Probably, they are two alternative links from one and
aglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^388

HYPERCAPNIA
PHOSPHOLIPASE A2
activation
FREE ARACHIDONATE
CYCLOOXYGENASE activation
PROSTANOIDS
ADENYLATE CYCLASEactivation
cAMP
NITRIC OXIDE SYNTHASEactivation
NITRIC OXIDE
GUANYLATE CYCLASEactivation
cGMP
MODULATION OF Ca2+- AND ATP-DEPENDENTK+-CHANNELS*
RELAXATION OF SMOOTH MUSCLES OF CEREBRALVESSELS
VASODILATION
*N
ITR
IC O
XID
E-D
EP
EN
DE
NT
CA
SCA
DE
? ?
Inhibitors
*
PROTEIN KINASE G activation*and/or suppression of
ENDOTHELIN release*
Cross-talk betweenmetabolising systems
PR
OST
AN
OID
-DE
PE
ND
EN
T C
ASC
AD
E
↓
↓
↓
↓
↓
↓
↓
Scheme 1 Hypotheticalendothelium-derivedmechanism(s) for the regulation of cerebralblood flowbyhypercapnia. (?) The triggersignal(s) by whichhypercapnia stimulates cerebralprostanoid and NO syntheses is unknown. (*) Possible sitesof interaction betweenbothpathwaysFNOSdependent and COX dependent.
380 Bakalova et al.
the same regulatory chain (Scheme 1). The accent of thepresent study is on the COX-dependent branch. Theobservations that many COX inhibitors completelyabolish CBF response to hypercapnia4,6 indicate that thispathway really takes important place in CBF regulation atrest condition.
Despite considerable research over many decades, themechanism(s) underlying the coupling between neuronalactivity and rCBF is still unclear. There are many opinionsabout the relationships between biochemical mediatorsas well as many obscurities about a trigger mechanism(s)of function/flow couple.7,8,3
It was found that neuronal activity causes depolariza-tion-induced enhancement in phospholipase A2 activityby K+.9 This process has resulted in a production of freearachidonate and subsequent COX activation. It wasfound also that COX products are produced by activatedneurons, astrocytes, and, probably, by perivascularnerves.10,11,6 Nevertheless, their role in the couplingbetween neuronal activity and rCBF is less investigatedand obscure.
In the early 1990s, COX was demonstrated to exist astwo distinct isoforms.12 COX-1 is constitutively expressedas a ‘housekeeping’ enzyme in most tissues. In contrast,COX-2 can be upregulated by various agents, includingcytokines and growth factors, and can be expressed in
Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^
many brain disorders.13 Recently, it was found that theselective COX-2 inhibitor NS-398 attenuates the increasein rCBF evoked by neuronal activation, whereas thehypercapnic vasodilation is not affected by this com-pound.14 On the other hand, a selective COX-1 inhibitorSC-560 reduces the resting CBF and attenuates the CBFincrease, produced by hypercapnia, but the drug does notaffect the increase in somatosensory blood flow, producedby neuronal stimulation.15
The results, mentioned above, suggest that COX-isoenzymes and their products may play a more complexphysiological role in the function/flow coupling than wasexpected.
It was observed that a neuronal activation applied aftera brief hypercapnia16 as well as a combined application ofgraded neuronal activation and continuous hypercap-nia17 resulted in a synergistic increase in absoluteresponse of rCBF in somatosensory cortex. It is wellknown that both coupling processes have common targetsites on smooth muscles of cerebral vesselsFion chan-nels.18,19 It is not excluded COX-dependent cascade totake part in this synergism also.
In the present study, we try to give at least a partialexplanation about the possible participation of hypercap-nia as a trigger signal for activation of COX-dependentpathway in the regulation of somatosensory blood flow
388 & 2002 Elsevier Science Ltd. All rights reserved.

Neuronal activity, rCBF, cyclooxygenase 381
during neuronal stimulation. Using laser-Doppler flow-metry (LDF), we estimated the effect of a non-selectiveCOX-inhibitorFindomethacin (IMC)Fon the rCBF-response in somatosensory cortex of a-chloraloseanesthetized rats, evoked by electrical hind paw stimula-tion under normo- and hypercapnia.
MATERIALS AND METHODS
Animal preparation
All experiments were conducted in accordance with theguidelines of the Physiological Society of Japan and wereapproved by the Animal Care and Use Committee of theResearch Institute for Brain and Blood Vessels, Akita,Japan.
Twenty Sprague–Dawley male rats (403.5723.4 g,mean7SD) were used to investigate the effect of IMCand hypercapnia, applied separately or in combination,on the evoked rCBF in response to hind paw stimulation.The rats were divided into two groups:
K nine rats (408.9725.7 g, mean7SD) were used inexperimental protocol A (Fig. 1A), and
K eleven rats (397.5720.5 g, mean7SD) were used inexperimental protocol B (Fig. 1B).
Preparation
Experiment 1
Anaesthesia
Stabilization Stimulation
Normocapnia
Equili-bration
20 min
Preparation
IMCsingle i.v. injection
(10 mg/kg b.w.)
Experiment 1
Anaesthesia
Stabilization Stimulation
Normoc
IMCi.v. i(10 m
20 min
Protocol A
Protocol B
Fig. 1 Experimentalprotocols.Experimentswere carried out about 3 hbefore andafter IMC intravenous (i.v.) infusion (10mg/kg/h) duringnormosuccessivestimuliof 5 Hz frequency (5 sduration,1.5mA)wereappliedatB: normocapnia-IMC-hypercapnia.
& 2002 Elsevier Science Ltd. All rights reserved. Prost
The rats were anesthetized with halothane (3% forinduction and 1% during surgery) in 30% O2 and 70%N2O, using a face mask. Subcutaneous 2% lidocaine wasused before incision to prevent vasospasm duringcatheter insertion. Polyethylene catheters were used tocannulate the tail artery and the left femoral vein forblood-pressure monitoring, blood sampling for gas ana-lysis, and i.v. administration of anesthetic and IMC. Aftertracheotomy, a-chloralose (56 mg/kg, i.v.) was adminis-tered, and halothane and nitrous oxide administrationwas discontinued. Anesthesia was maintained with a-chloralose (44 mg/kg/h, i.v.), and muscle relaxation withpancronium bromide (0.7 mg/kg/h, i.v.). The body tem-perature was monitored with a rectal probe and main-tained at about 37.01C using a heating pad (MuromachiKikai Co. Ltd, MK-900, Japan).
The rat was ventilated by respirator (Harvard Appara-tus, M-683, USA) throughout the experimental period,with a mixture of air and oxygen to achieve physiologicalarterial blood levels of O2 and CO2 tension (PaO2 andPaCO2, respectively). Under normocapnia, PaCO2 levelswere maintained in the range 35–40 mmHg and PaO2
levels - in the range 110–130 mmHg, by regulating thestroke volume of ventilation and the fractional concen-tration of oxygen in the gas inspired, respectively.
IMCsingle i.v. injection
(10 mg/kg b.w.)
Hypercapnia
Experiment 2
Stimulation
IMCi.v. infussion(10 mg/kg/h)
Experiment 3
Stimulation20 min 10 min
Experiment 4
Stimulation
apnia Hypercapnia
Equili-bration
nfussiong/kg/h)
Experiment 2
Stimulation10 min
Experiment 3
Stimulation
20 min
Experiment
Hind paw stimulation - 1.5 mA, 5 Hz
Blood gassample
Blood gassample
5 sec 60 sec
Stim.1 Stim.2 Stim.20
after the preparation of the animal.The evoked rCBF wasmeasured- andhypercapnia (2.5%CO2 ventilation).At eachexperiment, 2060 sintervals.Protocol A: normocapnia-hypercapnia-IMC.Protocol
aglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^388

382 Bakalova et al.
The animals were fixed in a stereotactic frame, and theparietal bone was thinned to translucency at the leftsomatosensory cortex using a dental drill (an area of3�3 mm2, centered at 2.5 mm caudal and 2.5 mm lateralto the bregma). To ensure a stable physiological conditionof the animal, measurements were performed 3 h after thepreparation of the parietal bone.
For hypercapnic ventilation, approximately 2.5% CO2
was mixed with the gas administered under normocapnia.An equilibration time of 20 min was the time at which thebaseline of rCBF reached a peak value after 2.5% CO2-ventilation.20
LDF measurement and hind paw stimulation
Changes in evoked rCBF were measured by LDF (TDF-LN1, Unique Medical, Japan). The tip diameter of the LDFprobe was 0.55 mm (Probe LP-N, Unique Medical, Japan).LDF measures red blood cell’s behavior in the capillarybased on the Doppler effect with laser light (wavelengthof 780 nm). The frequency shift of the scattered radiationis caused by moving red blood cells in the blood vessels.The sampling volume of LDF measurement was about1 mm3.21 A time constant of 0.1 s was used to detect theLDF signal. The LDF probe was positioned to the thinnedskull (over the somatosensory area of the hind paw)perpendicular to the brain surface. It was attached to thethinned parietal bone and then finely positioned using amicromanipulator to obtain the maximum signal changeduring stimulation (15–20% at a frequency of 5 Hz,current of 1.5 mA, duration of 5 s), avoiding areas withlarge blood vessels.
Electrical hind paw stimulation was performed with twoneedle electrodes inserted subdermally into the righthind paw contralateral to the LDF probe. A currentstimulus of 1.5 mA (0.1 ms pulse) was applied at 5 Hzfrequency and 5 s duration. At each experiment, 20successive stimuli were applied at 60 s intervals. Thesestimulus parameters did not cause any changes in thesystemic arterial blood pressure and heart rate duringstimulation.22,20
The rCBF response to somatosensory stimulation wasinvestigated before and after IMC application underdifferent gas conditionsFnormo and hypercapnia. Theorder of application of IMC and CO2 as well as the orderof hind paw stimulation is given in Figure 1.
IMC application
IMC (Sigma Chem. Co.) was first dissolved in 50 ml sodiumbicarbonate/saline solution (NaHCO3, 0.13 g/100 ml, pH7.4) and after that was added to 950ml saline solution. Ithas been demonstrated that in this concentration, thesolvent has no effect on CBF, cerebral oxygen consump-
Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^
tion, local cerebral glucose utilization, arterial bloodgases, mean arterial blood pressure (MABP), or bodytemperature.6
IMC was applied intravenously (0.5 ml single injectionof 10 mg/kg b.w.) and 20 min after that there was infusionwith 10 mg/kg b.w./h. The rate of infusion was 1 ml/h. Thetime protocols of IMC application were selected, based onthe preliminary experiments about dose- and time-dependent effects of IMC on the increase of evoked rCBFin somatosensory area of the cortex after hind pawstimulation.
Two distinct protocols of IMC application were used, i.e.,hypercapnia followed by IMC administration (Fig. 1A), andIMC administration followed by hypercapnia (Fig. 1B). As itis supposed that the cerebrovascular effects of hypercapniamight be long lasting,16 the use of both protocols is moresuited to distinguish the effect of IMC when the drug isadministered before and after hypercapnia.
Analyzed parameters
Arterial blood pressure was monitored during the experi-ments and MABP was calculated as the average at threetime points (i.e., before, during and immediately aftereach stimulation). Arterial blood samples were seriallycollected before and immediately after each step ofexperiment and analyzed for blood gas values (Fig. 1).
The LDF signal and arterial blood pressure wererecorded continuously on MacLab data acquisition soft-ware (AD Instruments, Australia) and the outputs wereaccumulated 20 times. Data were digitized at 40 Hz andsaved on a disk for off-line analysis. The rise time and thetermination time of the evoked rCBF were defined as thetimes at the intersection of the extrapolated lines, whichwere drawn on the response curve from 90 to 10% of thepeak, with the baseline. The peak time was the time atwhich the response curve of evoked rCBF reached themaximum height.22 The LDF signal was normalizedtowards the baseline level as percent changes from thebaseline. The response magnitude was calculated as anintegral of the response curve from the rise time to thetermination time.
Values were statistically analyzed by ANOVA, usingStudent’s t-test or Bonferrony test, and are presented asmean7SD.
RESULTS
Protocol A (hypercapnia - IMC application)
As shown in Table 1A, the physiological variables werewithin the normal ranges throughout the experimentalperiod under normocapnia in the absence of IMC.Ventilation with 2.5% CO2 for 20 min caused a significant
388 & 2002 Elsevier Science Ltd. All rights reserved.

Table 1 Physiologicalvariables
Condition MABP (mmHg) pH PaCO2 (mmHg) PaO2 (mmHg)
(A) Protocol A(n=9)a Beforehypercapnia 104.1379.00 7.4170.04 34.9872.83 125.45710.10
*** *** ***After hypercapnia 87.7578.01 7.1570.04 68.5375.64 126.7478.33
* *ns
After hypercapnia+IMC 76.6376.91 7.1170.03 69.4574.84 130.06713.60(B) Protocol B
(n=8)a Before IMC 103.8977.29 7.4070.03 37.2272.82 124.27710.68
*** ns nsAfter IMC 85.2274.02 7.3970.03 36.1871.91 128.48710.28
ns *** ***After IMC+hypercapnia 81.1174.54 7.1370.05 66.6775.12 129.92712.55aThenumberof rats; mean7SD.*Po0.05, **Po0.01, ***Po0.001.IMCFindomethacin.
*** *** ***
****** ***
Fig. 2 Baseline levelof CBFobtainedbefore andafter IMCapplicationunder normo- andhypercapnia.Thevalue of baselineobtainedunder normocapnia in theabsence of IMCwas consideredto be100%. (A) Protocol A (9 rats): normocapnia-hypercapnia-IMC. (B) Protocol B (11rats): normocapnia-IMC-hypercapnia.*Po0.05; **Po0.01; ***Po0.001.
Neuronal activity, rCBF, cyclooxygenase 383
reduction in arterial pH, a significant elevation in thelevel of PaCO2, and a significant decrease in MABP(Po0.001) (Table 1A). Subsequent i.v. infusion of IMC(10 mg/kg/h) lead to an additional significant decrease inarterial pH and MABP. Presumably, the decrease in pH is aresult of continuous hypercapnia and is not a result ofIMC application. IMC did not influence PaCO2 levelsunder hypercapnia. PaO2 level was unaffected by CO2
ventilation as well as by IMC application.The hind paw stimulation did not cause any change in
MABP during stimulation before and after CO2 ventila-tion as well as after IMC application.
Ventilation with 2.5% CO2 for 20 min resulted in asignificant increase in the baseline of CBF above thenormocapnic levels (Po0.001). The mean baseline levelof CBF under hypercapnia was about 90% higher thanthat under normocapnia (Fig. 2A). After IMC application(10 mg/kg/h) the mean baseline of CBF decreased andreturned to the normocapnic level. There was nosignificant difference between baseline levels of CBF 30and 50 min after beginning of IMC application.
The normalized response magnitude of rCBF at 5 Hzstimulation under hypercapnia was slightly greater thanthose under normocapnia, but the difference was notstatistically significant (Fig. 3A). Intravenous applicationof IMC (10 mg/kg/h) during hypercapnia resulted in asignificant reduction of the normalized response magni-tude of evoked rCBF as compared to that before IMCapplication under both, normo- and hypercapnic condi-tions (Po0.05). In this case, the response magnitude ofevoked rCBF decreased by about 35% as compared to thenormocapnic value, and about 55% as compared tohypercapnic value in the absence of IMC.
Stimulation at 5 Hz using a fixed duration of 5 s yieldedV-shaped response curves of evoked rCBF in somatosen-sory cortex (Fig. 4). The time parameters of the evokedrCBF were calculated under normo- and hypercapnia, as
& 2002 Elsevier Science Ltd. All rights reserved. Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^388

Fig. 3 Normalized responsemagnitudesof rCBF, evokedbysomatosensory stimulation, obtained before andafter IMCapplicationunder normo- andhypercapnia. (A) Protocol A (9 rats):normocapnia-hypercapnia-IMC. (B) Protocol B (11rats):normocapnia-IMC-hypercapnia. *Po0.05; **Po0.01;***Po0.001.
Fig. 4 Normalizedevoked rCBFcurves at somatosensorystimulation before andafter IMCapplicationunder normo- andhypercapnia.The response curveswerenormalized to thebaselinelevelandaveragedby thenumberofanimalsused. (A) Protocol A (9rats): normocapnia-hypercapnia-IMC. (B) Protocol B (11rats):normocapnia-IMC-hypercapnia.Y-axisFLDF signal in% ofbaseline, X-axisFstimulation period in seconds.
384 Bakalova et al.
well as before and after IMC application (Table 2A). Therise time of 0.55 s and peak time were nearly constant inall experimental conditions. After hypercapnia, theevoked rCBF response at 5 Hz stimulation peaked a bitlater and returned to the baseline level more slowly thanthat under normocapnia (Po0.01) (Fig. 4A, Table 2A). Thesubsequent application of IMC decreased significantlythe termination time under hypercapnia and restored it tothe normocapnic level. There were negligible variationsin all time parameters between 30 and 50 min after IMCapplication, so the data have been pooled together in thepresentation of the results in Table 2.
Protocol B (IMC application-hypercapnia)
Physiological variables measured during experimentalprotocol B are listed in Table 1B. They were within the
Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^
normal ranges throughout normocapnia before IMCapplication. Intravenous infusion of IMC (10 mg/kg b.w./h) during normocapnia lead to a significant decrease inMABP (Po0.001) and did not affect PaO2, PaCO2 and pH.Ventilation with 2.5% CO2 after IMC application did notcause additional changes in MABP, but it caused asignificant reduction in arterial pH and a significantelevation in the level of PaCO2 in comparison with thevalues under normocapnia. Hypercapnia did not affectPaO2 level.
The hind paw stimulation did not cause any change inMABP during stimulation before and after IMC applica-tion as well as before and after CO2 ventilation.
IMC application (10 mg/kg/h, i.v.) during normocapniacaused a significant decrease in the baseline level ofCBFFabout 20% than that before IMC application(Po0.05) (Fig. 2B). Subsequent 2.5% CO2 ventilation leadto a slight increase in the baseline CBF.
IMC (10 mg/kg/h) reduced significantly the normalizedresponse magnitude of evoked rCBF at 5 Hz stimula-tionFabout 70% in comparison with normocapnia(Po0.001). Subsequent CO2 ventilation did not causeadditional changes in the response magnitude of the
388 & 2002 Elsevier Science Ltd. All rights reserved.

Table 2 Timeparametersof the rCBFresponse curves
Condition Rise time (s) Peak time (s) Termination time (s)
(A) Protocol A(n=9)a Beforehypercapnia 0.5170.20 4.7970.38 9.4970.39
**After hypercapnia 0.5870.22 5.4470.66 13.7871.67
**After hypercapnia+IMC 0.6770.29 5.1871.01 9.6871.13
(B) Protocol B(n=8)a Before IMC 0.5570.21 4.6070.55 8.3770.88
*After IMC 0.5870.22 3.6170.97 7.2372.00
**After IMC+hypercapnia 0.5770.24 5.2571.00 9.6671.94
aThenumberof rats; mean7SD.*Po0.05, **Po0.01, ***Po0.001.IMCFindomethacin.
ns
ns
Neuronal activity, rCBF, cyclooxygenase 385
evoked rCBF as compared to that under normocapniaafter IMC application. The response magnitude of theevoked rCBF under hypercapnia stayed significantly lowthan that under normocapnia before IMC applica-tionFthe decrease was about 70% (Po0.001).
The rise time and termination time were nearlyconstant in all experimental conditions (Fig. 4B, Table2B). During normocapnia, after IMC application, theevoked rCBF curve peaked earlier as compared to thatbefore IMC application (Po0.05). The subsequent hyper-capnia restored the peak time to the value, characteristicof normocapnia before IMC application.
DISCUSSION AND CONCLUSIONS
Participation of COX-dependent cascade in the regulation ofhypercapnia-induced changes in CBFat rest condition
It has been found that the changes in the baseline level ofCBF response, measured by LDF, are indicative ofcerebrovascular tone at rest condition.20 The presentstudy shows that the baseline level increased significantlyduring hypercapnia and the subsequent application ofIMC abolished completely this effect. In contrast, IMC,applied under normocapnia, slightly reduced the baselineCBF (Po0.05) and the subsequent CO2 ventilation didnot affect it additionally (Fig. 2A). These results suggestthat IMC in concentration that effectively inhibit cerebralCOX and prostanoid synthesis in the brain,6 completelyabolishes hypercapnia-induced cerebral vasodilation.Applying before hypercapnia it completely suppressesthe effect of CO2 on cerebrovascular tone. Theseobservations confirm the hypothesis that the vasodilativeeffect of CO2 at rest condition is realized mainly throughIMC-sensitive and therefore COX-dependent pathway.4,5
Obviously, at rest condition, COX-products are the mainmediator of the relationship between high PaCO2 andCBF (Scheme 1).
& 2002 Elsevier Science Ltd. All rights reserved. Prost
However, as shown in Figure 2B, when hypercapnia isapplied after IMC, the baseline level of CBF slightlyincreases. This shows that COX-dependent pathway is notsingle in the regulation of hypercapnia-induced vasodila-tion. According to recent data, cerebral vasodilation tohypercapnia in rats at rest condition is inhibited by eitherCOX- and NOS-inhibitors.4 However, based on the results,mentioned above, as well as based on previouslypublished data,4,6 it appears that mainly the IMC-sensitive part is functionally connected with cerebralvascular relaxation by high PaCO2 at rest condition.
As the participation of NO-dependent pathway in theregulation of hypercapnia-induced vasodilation is aknown fact,7,4 the following question arises: What isthe possible effect of IMC on guanylate cyclase andcGMP-synthesisFa most likely site of interactionbetween COX- and NOS-dependent pathways of regula-tion of the relationship between hypercapnia and CBF(Scheme 1)?
It has been observed that hypercapnia causes anelevation of cortical cGMP that is not sensitive to NOS-inhibitors, but is significantly attenuated by IMC.5 A COX-dependent increase in cGMP could result from directactivation of guanylate cyclase by prostanoids.23 Theincrease in cortical cGMP during hypercapnia could alsobe an indirect consequence of elevated cAMP as a resultof cross-talk between cyclic nucleotide metabolizingsystems on the level of their synthesis and degrada-tion.24,5 It has been established also that prostacyclin,applied directly after i.v. infusion of IMC, facilitates therelease of NO and also potentiates its action in thecoronary vessels.25 Therefore, part of the hypercapnia-induced increase in cortical guanylate-cyclase activity isIMC sensitive and under COX control. Regardless ofthe possible increase in NOS activity by hypercapnia, theIMC probably blocks also NO-dependent cascade byinhibition of guanylate cyclase and suppression of cGMPproduction.
aglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^388

386 Bakalova et al.
The trigger signal(s) by which hypercapnia activatescerebral COX and prostanoid synthesis at rest conditionis not known. Two possible candidates are proposed:(i) arterial and intracellular decrease in pH under hyper-capnia,26,16,27 and (ii) subsequent elevation in free Ca2+,27
both causing activation of phospholipase A2 and releaseof free arachidonateFa substrate for COX.
It is also assumed that pH decrease during hypercapniahas a direct effect on cyclic nucleotide synthesis invascular tissue and/or cerebral cells (neurons and glia).5
However, based on the fact that IMC blocks completelythe cerebral vasodilatory response to hypercapnia,despite the long-lasting changes in pH (Fig. 2, Table 1),it appears that the direct effect of H+ on guanylate andadenylate cyclases is disputable.
In the present study, we hypothetize that, at restcondition, hypercapnia causes cerebral vasodilationmainly through activation of COX cascade and that themost likely trigger signal for this process is pH-dependentactivation of phospholipase A2 and release a freearachidonare, excluding a direct effect of H+ on cyclicnucleotide synthesis, as well as excluding a directvasodilative effect of CO2 on cerebral vessels.
Participation of COX-dependent cascade and CO2 in theregulation of the coupling between neuronalactivityandrCBF
The present study produces several findings, suggesting aparticipation of COX-dependent pathway in the regula-tion of rCBF, evoked by neuronal stimulation in somato-sensory cortex during normo- and hypercapnia:
(a) We demonstrated that IMC (10 mg/kg/h, i.v.) reducessignificantly evoked rCBF under normocapnia (Fig. 3B).In this case, its inhibitory effect is about 70%,indicating that IMC-sensitive and COX-dependentpathway is a major mechanism for regulation of therelationship between neuronal activity and rCBF.
(b) In the absence of IMC, the hypercapnia causes a slightincrease in normalized response magnitude of evokedrCBF (Fig. 3A). The hypercapnia results also in asignificant increase in absolute response magnitudeof rCBF, evoked by somatosensory stimulation.17,16
However, applied after IMC, the hypercapnia does notaffect evoked rCBF (Fig. 3B). The results suggest thatthe effect of CO2 on the evoked rCBF is completelyIMC sensitive and probably COX dependent as in thecase of rest condition. This suggestion also doubts adirect vasodilative effect of H+ and CO2 duringneuronal activity.
(c) The inhibitory effect of IMC on evoked rCBF is betterexpressed when IMC is applied before hypercapniathan that after hypercapnia (Fig. 4A). Applied afterhypercapnia, IMC reduces evoked rCBF to about 40%
Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^
and its inhibitory effect is time dependent. It is betterexpressed 50 min after beginning of IMC applicationthan 30 min after that (Fig. 4). Probably, the combinedapplication of hypercapnia and neuronal activityinduces not only prostanoid synthesis, but also asynthesis of many other vasodilating substances (nitricoxide, adenosine, Ca2+, etc.). It takes a time forutilization of these substances and manifestation ofreal effect of IMC on the rCBF, evoked by neuronalstimulation.
The results, mentioned above, suppose the followingpossibilities, explaining the effect of IMC on the evokedrCBF: (i) a participation of COX-dependent pathway in theregulation of rCBF, induced by neuronal stimulation,and/or (ii) direct effect of IMC on neuronal activity insomatosensory cortex. The second possibility is not likelybecause it is reported that IMC (up to 30 mg/kg b.w., i.v.)does not affect oxygen consumption and regionalcerebral glucose utilization under neuronal activation inthe brain.6 It may be concluded that IMC reduces evokedrCBF in somatosensory cortex, through inhibition ofCOX-dependent pathway.
At least two possible trigger signals for COX-activationand prostanoid synthesis by neuronal activity may behypothesized:
K depolarization-induced enhancement in phospholipaseA2 activity by K+; and/or
K regional CO2 increase and long-lasting pH changes in adiscreetly activated region of the cortex,
both leading to the production of free arachidonate andsubsequent COX activation, as well as to the release ofother vasodilators.9,2
About depolarization-induced enhancement in phos-pholipase A2 activity by K+ there are many experimentalevidences.10,28 However, about local hypercapnia as aresult of accelerated aerobic glucose metabolism duringneurotransmission there are many Con and Pro opinions.Nevertheless, the hypothesis about regional hypercapniaas a possible trigger signal for activation of COX-dependent pathway of evoked rCBF regulation duringneuronal activity is likely and has not been excluded.
Recently specific prostanoid receptors are characterizedon the smooth muscles of cerebral vasculature.29 Themechanism of regulation of the evoked rCBF duringsomatosensory stimulation by COX products is probablyreceptor mediated. It is not excluded IMC to act also as areceptor–antagonist. It has been observed that IMC-sensitive CO2 reactivity of cerebral vessels is restored byvasodilator prostacyclin,30 what doubts the interactionbetween IMC and prostanoid receptors. Nevertheless, thispossibility needs verification.
388 & 2002 Elsevier Science Ltd. All rights reserved.

Neuronal activity, rCBF, cyclooxygenase 387
Our results demonstrated also that IMC, in a doseapplied (10 mg/kg b.w./h, i.v.), does not inhibit completelyevoked rCBF response in somatosensory area duringneuronal stimulation, in contrast to rest condition (Figs. 2and 3). This observation suggests that the neuronalactivity unlock also another pathway for rCBF regulation.The extension of termination time of the evoked rCBFcurves by hypercapnia, as well as the shortening of peaktime by IMC (Table 2), suggests that CO2 and IMCinfluence predominantly the second part of the evokedrCBF curve (Fig. 4). Presumably, CO2 and COX productstake part in the regulation of evoked rCBF later thanother vasodilating substances.
It has to be noted also that some authors assumed thatCOX products cannot be generally responsible forvascular dilation in the brain because the COX inhibitorshave no effect on the circulatory response to hypoxia aswell as some of them tend to vasodilate the blood vesselsin vitro.11,6 The lack of effect of COX inhibitors onhypoxia-induced cerebral vasodilation is not surprisingbecause COX is an oxygen-dependent enzyme. Still theexact mechanism(s) of participation of COX pathway inthe regulation of cerebrovascular tone by neuronalactivity remains to be clarified.
ACKNOWLEDGEMENTS
The technical assistance of Mr. Y. Ito of the ResearchInstitute for Brain and Blood Vessels, Akita, Japan, isgratefully acknowledged. This study was supported, inpart, by the STA Postdoctoral Research Fellowship fromThe Japan Science and Technology Agency.
REFERENCES
1. Brian J. E. Jr., Faraci F. M., Heistad D. D. Recent insights into theregulation of cerebral circulation. Clin Exp Pharmacol Physiol1996; 23(6–7): 449–457.
2. Magistretti P. J., Pellerin L., Rothman D. L., Shulman R. G. Energyand demand. Science 1999; 283(5401): 496–497.
3. Villringer A., Dirnagl U. Coupling of brain activity and cerebralblood flow: basis of functional neuroimaging. Cerebrovasc BrainMetab Rev 1995; 7: 240–276.
4. Heinert G., Nye P. C. G., Paterson D. J. Nitric oxide andprostaglandin pathways interact in the regulation of hypercapniccerebral vasodilation. Acta Physiol Scand 1999; 166: 183–193.
5. Parfenova H., Shibata M., Zuckerman S., Mirro R., Leffler C. W.CO2 and cerebral circulation in newborn pigs: cyclic nucleotidesand prostanoids in vascular regulation. Am J Physiol 1994; 266:H1494–H1501.
6. Pickard J. D. Role of prostanoids and arachidonic acid derivativesin the coupling of cerebral blood flow to cerebral metabolism.J Cereb Blood Flow Metab 1981; 1: 361–384.
7. Dirnagl U., Niwa K., Lindauer U., Villringer A. Coupling of cerebralblood flow to neuronal activation: role of adenosine and nitricoxide. Am J Physiol 1994; 267: H297–H301.
& 2002 Elsevier Science Ltd. All rights reserved. Prosta
8. Faraci F. M., Sobey C. G. Role of potassium channels in regulationof cerebral vascular tone. J Cereb Blood Flow Metab 1998; 18:1047–1063.
9. Howard M. J., Insel P. A. Elevated extracellular K+ enhancesarachidonic acid release in MDCK-D1 cells. Am J Physiol 1990;259: C224–C231.
10. Golanov E. V., Reis D. J. Nitric oxide and prostanoids participatein cerebral vasodilation elicited by electrical stimulation of therostral ventrolateral medulla. J Cereb Blood Flow Metab 1994; 14:492–502.
11. Lipsky P. E., Brooks P., Crofford L. J., DuBois R., Graham D.,Simon L. S., van de Putte L. B., Abramson S. B. Unresolved issuesin the role of cyclooxygenase-2 in normal physiological processesand disease. Arch Intern Med 2000; 160(7): 913–920.
12. Hawkey C. J. COX-2 inhibitors. Lancet 1999; 353: 307–314.13. Ek M., Engblom D., Saha S., Blomqvist A., Jakobsson P.-J.,
Ericsson-Dahlstrand A. Pathway across the blood–brain barrier.Nature 2001; 410: 430–431.
14. Niwa K., Araki E., Morham S. G., Ross M. E., Iadecola C.Cyclooxygenase-2 contributes to functional hyperemia inwhisker-barrel cortex. J Neurosci 2000; 20(2): 763–770.
15. Niwa K., Haensel C., Ross M. E., Iadecola C. Cyclooxygenase-1participates in selected vasodilator response of the cerebralcirculation. Circulation Res 2001; 88: 600–607.
16. Schmitz B., Bottiger B. W., Hossmann K. -A. Brief hypercapniaenhances somatosensory activation of blood flow in rat. J CerebBlood Flow Metab 1996; 16: 1307–1311.
17. Bakalova R., Matsuura T., Kanno I. Frequency dependence oflocal cerebral blood flow induced by somatosensory hind pawstimulation in rat under normo- and hypercapnia. Jpn J Physiol2001; 51(2): 201–208.
18. Li P. L., Zou A. P., Campbell W. B. Regulation of potassiumchannels in coronary arterial smooth muscle by endothelium-derived vasodilators. Hypertension 1997; 29: 262–267.
19. Robertson B. E., Schubert R., Hescheler J., Nelson M. T. cGMP-dependent protein kinase activates Ca2+-activated K+ channels incerebral artery smooth muscle cells. Am J Physiol 1993; 265:C299–C303.
20. Matsuura T., Fujita H., Kashikura K., Kanno I. Evoked localcerebral blood flow induced by somatosensory stimulation isproportional to the baseline flow. Neurosci Res 2000; 38: 341–348.
21. Nilsson G. E., Tenland T., Oberg P. A. Evaluation of a laser-Doppler flowmeter for measurement of tissue blood flow. IEEETrans Biochem Eng 1980; 27: 597–604.
22. Matsuura T., Fujita H., Seki C., Kashikura K., Kanno I. CBF-changeevoked by somatosensory activation measured by laser-Dopplerflowmetry: independent evaluation of RBC velocity and RBCconcentration. Jpn J Physiol 1999; 49: 289–296.
23. Kanba S., Sasakawa N., Nakaki T., Kanba K.-S., Yagi G., Kato R.,Richelson E. Two possibly distinct prostaglandin E1 receptors inN1E-115 clone: one mediating inositol triphosphate formation,cyclic GMP formation, and intracellular calcium mobilization andthe other mediating cyclic AMP formation. J Neurochem 1991; 57:2011–2015.
24. Jiang H., Colbran J. L., Francis S. H., Corbin J. D. Direct evidencefor cross-activation of cGMP-dependent protein kinase by cAMPin pig coronary arteries. J Biol Chem 1992; 267(2): 1015–1019.
25. Shimokawa H., Flavahan N. A., Lorentz R. R., Vanhoutte P. M.Prostacyclin releases endothelium-derived relaxing factor andpotentiates its action in coronary artery of the pig. Br J Pharmacol1988; 95: 1197–1203.
26. Busija D. W., Heistad D. D. Factors involved in the physiologicalregulation of the cerebral circulation. Rev Physiol Biochem 1984;101: 162–211.
glandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^388

388 Bakalova et al.
27. Wagerle L. C., Mishra O. P. Mechanism of CO2 response incerebral arteries of the newborn pig: role of phospholipase,cyclooxygenase, and lipoxygenase pathways. Circ Res 1988; 62:1019–1026.
28. Sobey C. G., Heistad D. D., Faraci F. M. Potassium channelsmediate dilation of cerebral arterioles in response toarachidonate. Am J Physiol 1998; 275: H1606–H1612.
Prostaglandins, Leukotrienes and Essential FattyAcids (2002) 67(6), 379^
29. Narumiya S. Prostanoid receptors and signal transduction. ProgBrain Res 1996; 113: 231–241.
30. Suzuki H., Ikezaki H., Hong D., Rubinstein I. PGH(2)-TxA(2)-receptor blockade restores vasoreactivity in a new rodentmodel of genetic hypertension. J Appl Physiol 2000; 88(6):1983–1988.
388 & 2002 Elsevier Science Ltd. All rights reserved.
Related Documents