Cyclooxygenase-1 derived prostaglandins are involved in the maintenance of renal function in rats with cirrhosis and ascites 1 Marta Lo´pez-Parra, * ,1 Joan Cla`ria, 1 Anna Planaguma`, 1 Esther Titos, 5 Jaime L. Masferrer, 5 B. Mark Woerner, 5 Alane T. Koki, 2 Wladimiro Jime´ nez, 4 Rosario Altuna, 3 Vicente Arroyo, 2 Francisca Rivera & 3 Joan Rode´s 1 DNA Unit, Hospital Clı´nic, Institut d’Investigacions Biome`diques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Barcelona 08036, Spain; 2 Hormonal Laboratory, Hospital Clı´nic, Institut d’Investigacions Biome`diques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Barcelona 08036, Spain; 3 Liver Unit, Hospital Clı´nic, Institut d’Investigacions Biome`diques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Barcelona 08036, Spain; 4 Pharmacia Spain, Barcelona 08190, Spain and 5 Pharmacia Research and Development, St Louis, Missouri, MO 63167, U.S.A. 1 The maintenance of renal function in decompensated cirrhosis is highly dependent on prostaglandins (PGs). Since PG synthesis is mediated by cyclooxygenase-1 and -2 (COX-1 and COX-2), the present study was designed to examine which COX isoform is involved in this phenomenon. 2 Renal COX-1 and COX-2 protein expression and distribution were analysed by Western blot and immunohistochemistry in nine rats with carbon tetrachloride-induced cirrhosis and ascites and 10 control animals. The eects of placebo and selective COX-1 (SC-560) and COX-2 (celecoxib) inhibitors on urine flow (V), urinary excretion of sodium (U Na V) and PGE 2 (U PGE2 V), glomerular filtration rate (GFR), renal plasma flow (RPF), the diuretic and natriuretic responses to furosemide and renal water metabolism were assessed in 88 rats with cirrhosis and ascites. 3 COX-1 protein levels were found to be unchanged in kidneys from cirrhotic rats. In contrast, these animals showed enhanced renal COX-2 protein expression which was focally increased in the corticomedullary region. Although U PGE2 V was equally reduced by SC-560 and celecoxib, only SC- 560 produced a significant decrease in U Na V, GFR and RPF and a pronounced impairment in the diuretic and natriuretic responses to furosemide in rats with cirrhosis and ascites. Neither SC-560 nor celecoxib aected renal water metabolism in cirrhotic rats. 4 These results indicate that despite abundant renal COX-2 protein expression, the maintenance of renal function in cirrhotic rats is mainly dependent on COX-1-derived prostaglandins. British Journal of Pharmacology (2002) 135, 891 – 900 Keywords: Experimental cirrhosis; renal COX expression; selective COX inhibition; renal function Abbreviations: Celecoxib, 4-[5-(4-methylphenyl)-3-(trifluoromethyl)-1H-pyrazol-1-yl]; GFR, glomerular filtration rate; NSAIDs, nonsteroidal anti-inflammatory drugs; PG, prostaglandin; RPF, renal plasma flow; SC-560, [5-(4-chlorophenyl)- 1-(4-methoxyphenyl)-3-trifluoromethylpyrazole); V, urine flow; U PGE2 V, urinary PGE 2 excretion; U Na V, urinary sodium excretion Introduction Non-steroidal anti-inflammatory drugs (NSAIDs) are among the most widely prescribed class of pharmaceutical agents world-wide, having broad clinical utility in treating pain, fever and inflammation (Payan & Katzung, 1995). Despite a relatively low incidence of renal side eects in healthy subjects, administration of NSAIDs to patients with unbalanced eective arterial blood volume, such as decom- pensated cirrhosis, represents a major clinical problem since renal function in these patients is critically dependent on prostaglandins (PGs) (Arroyo et al., 1983; 1986; Dunn, 1984). In fact, acute PG inhibition with NSAIDs in patients with cirrhosis and ascites is associated with a significant impairment in renal hemodynamics, sodium excretion, free water clearance and renal response to furosemide and spironolactone (Boyer et al., 1979; Zipser et al., 1979; Arroyo et al., 1983; 1986; Planas et al., 1983; Mirouze et al., 1983; Pe´ rez-Ayuso et al., 1984; Dunn, 1984). Thus, in clinical practice, patients with decompensated cirrhosis cannot be treated with NSAIDs on a long term basis because of the high risk of developing renal failure and refractory ascites. Cyclooxygenase (COX) is the key enzyme in the formation of PGs from arachidonate and is the major therapeutic target for NSAIDs (Vane, 1971). Two isoforms of COX, designated COX-1 and COX-2, have been identified (Kujubu et al., 1991, Masferrer et al., 1992; Hla & Neilson, 1992). COX-1 is ubiquitous and has been previously linked to the cytoprotective eects of PGs in the gut as well as to the integrity of platelet function. Conversely, COX-2 is undetectable in most tissues, but its expression can be induced by a variety of stimuli related to inflammatory response (Herschman, 1996). Conventional NSAIDs inhibit COX-1 and COX-2 and this feature British Journal of Pharmacology (2002) 135, 891 – 900 ª 2002 Nature Publishing Group All rights reserved 0007 – 1188/02 $25.00 www.nature.com/bjp *Author for correspondence; E-mail: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cyclooxygenase-1 derived prostaglandins are involved in themaintenance of renal function in rats with cirrhosis and ascites
1Marta Lo pez-Parra, *,1Joan ClaÁ ria, 1Anna PlanagumaÁ , 1Esther Titos, 5Jaime L. Masferrer,5B. Mark Woerner, 5Alane T. Koki, 2Wladimiro Jime nez, 4Rosario Altuna, 3Vicente Arroyo,2Francisca Rivera & 3Joan Rode s
1DNA Unit, Hospital ClõÂ nic, Institut d'Investigacions BiomeÁ diques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona,Barcelona 08036, Spain; 2Hormonal Laboratory, Hospital ClõÂ nic, Institut d'Investigacions BiomeÁ diques August Pi i Sunyer(IDIBAPS), Universitat de Barcelona, Barcelona 08036, Spain; 3Liver Unit, Hospital ClõÂ nic, Institut d'InvestigacionsBiomeÁ diques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Barcelona 08036, Spain; 4Pharmacia Spain, Barcelona08190, Spain and 5Pharmacia Research and Development, St Louis, Missouri, MO 63167, U.S.A.
1 The maintenance of renal function in decompensated cirrhosis is highly dependent onprostaglandins (PGs). Since PG synthesis is mediated by cyclooxygenase-1 and -2 (COX-1 andCOX-2), the present study was designed to examine which COX isoform is involved in thisphenomenon.
2 Renal COX-1 and COX-2 protein expression and distribution were analysed by Western blot andimmunohistochemistry in nine rats with carbon tetrachloride-induced cirrhosis and ascites and 10control animals. The e�ects of placebo and selective COX-1 (SC-560) and COX-2 (celecoxib)inhibitors on urine ¯ow (V), urinary excretion of sodium (UNaV) and PGE2 (UPGE2V), glomerular®ltration rate (GFR), renal plasma ¯ow (RPF), the diuretic and natriuretic responses to furosemideand renal water metabolism were assessed in 88 rats with cirrhosis and ascites.
3 COX-1 protein levels were found to be unchanged in kidneys from cirrhotic rats. In contrast,these animals showed enhanced renal COX-2 protein expression which was focally increased in thecorticomedullary region. Although UPGE2V was equally reduced by SC-560 and celecoxib, only SC-560 produced a signi®cant decrease in UNaV, GFR and RPF and a pronounced impairment in thediuretic and natriuretic responses to furosemide in rats with cirrhosis and ascites. Neither SC-560nor celecoxib a�ected renal water metabolism in cirrhotic rats.
4 These results indicate that despite abundant renal COX-2 protein expression, the maintenance ofrenal function in cirrhotic rats is mainly dependent on COX-1-derived prostaglandins.British Journal of Pharmacology (2002) 135, 891 ± 900
Keywords: Experimental cirrhosis; renal COX expression; selective COX inhibition; renal function
Abbreviations: Celecoxib, 4-[5-(4-methylphenyl)-3-(tri¯uoromethyl)-1H-pyrazol-1-yl]; GFR, glomerular ®ltration rate; NSAIDs,nonsteroidal anti-in¯ammatory drugs; PG, prostaglandin; RPF, renal plasma ¯ow; SC-560, [5-(4-chlorophenyl)-1-(4-methoxyphenyl)-3-tri¯uoromethylpyrazole); V, urine ¯ow; UPGE2V, urinary PGE2 excretion; UNaV, urinarysodium excretion
Introduction
Non-steroidal anti-in¯ammatory drugs (NSAIDs) are amongthe most widely prescribed class of pharmaceutical agents
world-wide, having broad clinical utility in treating pain,fever and in¯ammation (Payan & Katzung, 1995). Despite arelatively low incidence of renal side e�ects in healthy
subjects, administration of NSAIDs to patients withunbalanced e�ective arterial blood volume, such as decom-pensated cirrhosis, represents a major clinical problem since
renal function in these patients is critically dependent onprostaglandins (PGs) (Arroyo et al., 1983; 1986; Dunn,1984). In fact, acute PG inhibition with NSAIDs in patientswith cirrhosis and ascites is associated with a signi®cant
impairment in renal hemodynamics, sodium excretion, freewater clearance and renal response to furosemide andspironolactone (Boyer et al., 1979; Zipser et al., 1979;
Arroyo et al., 1983; 1986; Planas et al., 1983; Mirouze et al.,1983; Pe rez-Ayuso et al., 1984; Dunn, 1984). Thus, in
clinical practice, patients with decompensated cirrhosiscannot be treated with NSAIDs on a long term basisbecause of the high risk of developing renal failure and
refractory ascites.Cyclooxygenase (COX) is the key enzyme in the
formation of PGs from arachidonate and is the major
therapeutic target for NSAIDs (Vane, 1971). Two isoformsof COX, designated COX-1 and COX-2, have beenidenti®ed (Kujubu et al., 1991, Masferrer et al., 1992; Hla& Neilson, 1992). COX-1 is ubiquitous and has been
previously linked to the cytoprotective e�ects of PGs inthe gut as well as to the integrity of platelet function.Conversely, COX-2 is undetectable in most tissues, but its
expression can be induced by a variety of stimuli related toin¯ammatory response (Herschman, 1996). ConventionalNSAIDs inhibit COX-1 and COX-2 and this feature
British Journal of Pharmacology (2002) 135, 891 ± 900 ã 2002 Nature Publishing Group All rights reserved 0007 ± 1188/02 $25.00
www.nature.com/bjp
*Author for correspondence; E-mail: [email protected]

accounts for both therapeutic and side e�ects (Warner et al.,1999). Recently, selective COX-2 inhibitors have beendeveloped to e�ectively inhibit COX-2-dependent in¯amma-
tion while sparing physiologic PG production (Seibert et al.,1994; Marnett & Kalgutkar, 1999). These novel compoundscould potentially be the NSAIDs of choice in patients inwhom, as occurs in cirrhosis with ascites, renal function is
critically dependent on PGs.To address the renal-damaging e�ects of NSAIDs in liver
disease, we have previously used rats with carbon tetra-
chloride (CCl4)-induced cirrhosis, an experimental modelthat closely reproduces the systemic and renal abnormalitiesseen in human cirrhosis (ClaÁ ria & Jime nez, 1999). In fact,
CCl4-induced cirrhotic rats also show increased renal PGsynthesis and develop renal failure after receiving conven-tional NSAIDs such as aspirin (Ros et al., 1995) and
ketorolac (Bosch-Marce et al., 1999). Interestingly, we haverecently shown that renal function in these animals remainsuna�ected by the administration of SC-236 (a research pre-clinical compound with high selectivity for COX-2 (Bosch-
Marce et al., 1999)), suggesting that the renal side-e�ects ofconventional NSAIDs in cirrhosis are secondary to COX-1inhibition. Given that a selective COX-1 inhibitor was not
available in that study, the current investigation was aimedto unequivocally establish which COX isoform is responsiblefor the synthesis of PGs involved in the maintenance of
renal function in decompensated cirrhosis. To this end, we®rst analysed COX-1 and COX-2 protein expression anddistribution by Western blot and immunohistochemistry,
respectively, in kidneys from rats with CCl4-inducedcirrhosis and ascites. In these animals, we next comparedthe e�ects of a selective COX-1 inhibitor (SC-560) withthose of a selective COX-2 inhibitor (celecoxib) on renal
hemodynamics and renal sodium handling. Subsequently, weassessed the e�ects of these COX inhibitors on the diureticand natriuretic response to furosemide, and ®nally char-
acterized which COX isoform is involved in the regulationof renal water metabolism in cirrhotic rats.
Methods
Materials
125I-Iothalamate, speci®c PGE2 EIA and the ECL systemwere from Amersham Pharmacia (Buckinghamshire, U.K.).
PAH was obtained from Merck & Co (West Point, PA,U.S.A.). Sep-Pack C18 cartridges and HPLC columns werefrom Waters (Milford, MA, U.S.A.). Furosemide was from
Hoechst Marion Roussel (Seguril1, Barcelona, Spain). MBFwas from Strecks Laboratories (Omaha, NE, U.S.A.).Immobilon-P PVDF membranes were from Millipore (Bed-
ford, MA, U.S.A.). Tween 80, aprotinin, leupeptin, pepstatinA and phenylmethylsulphonyl ¯uoride were purchased fromSigma Chemical Co (St Louis, MO, U.S.A.). Ketorolac,COX-1 and COX-2 protein standards, COX-1 (murine)
monoclonal antibody and COX-2 (murine) polyclonal anti-body (Western blot) were from Cayman Chemical Company(Ann Arbor, MI, U.S.A.). Polyclonal rabbit anti-human
COX-2 serum and anti-ovine COX-1 monoclonal antibodywere from Oxford Biomedical Research (Oxford, MI,U.S.A.). Selective COX-1 (SC-560) and COX-2 (celecoxib)
inhibitors were provided by Pharmacia Research andDevelopment (St Louis, MO, U.S.A.).
Induction of cirrhosis in rats
The study was performed in 97 rats with cirrhosis and ascites.Cirrhosis was induced by CCl4 inhalation in adult male
Wistar rats (Charles-River, Saint Aubin les Elseuf, France)initially weighing 160 ± 180 g, following a method describedelsewhere (ClaÁ ria & Jime nez, 1999). Cirrhotic rats were
obtained from a group of 136 animals submitted to thecirrhosis induction protocol. Thirty-nine of these animalscould not be included in the study for several reasons: 24 rats
died before the development of ascites and/or impairment ofrenal water excretion, seven rats died before completing theexperimental procedures and eight rats did not develop
ascites and/or impairment to renal water excretion. Animalswere maintained at the University of Barcelona animalfacility and were fed ad libitum with standard chow anddistilled water containing phenobarbital (0.3 g l71) as drink-
ing ¯uid. Cirrhotic rats were studied after the development ofascites, usually between 12 and 18 weeks of CCl4 adminis-tration.
Western blot analysis of COX-1 and COX-2 proteinexpression in renal tissue
Protein expression for COX-1 and COX-2 was assessed inrenal tissue samples isolated from six cirrhotic rats with
ascites and from seven control animals. Animals wereanaesthetized with an i.m. injection of ketamine (50 mg kg71)and the kidneys were rapidly dissected and stored in liquidnitrogen. Frozen tissues (150 ± 180 mg) were homogenized in
30 mM Tris/HCl pH 7.4, 100 mM phenylmethylsulphonyl¯uoride, containing protease inhibitors (1 mg ml71 each):leupeptin, pepstatin A and aprotinin. The homogenate was
centrifuged at 10006g for 10 min and the supernatant wastaken and subjected to a ®nal centrifugation step at100,0006g for 70 min. Total protein concentration was
determined by the Bradford Protein Assay. Aliquots fromeach sample containing equal amounts of protein (30 ± 50 mg)were resuspended in SDS-containing Laemmli sample bu�erand heated at 1008C for 5 min, electrophoresed on 10 ± 12%
SDS-polyacrylamide gels and transferred overnight to PVDFmembranes. The e�ciency of the transfer was visualized byPonceau staining. The blots were subsequently blocked for
6 h with 50 mM Tris/HCl pH 7.4 and 100 mM NaCl (TBS)containing 5% nonfat dry milk and 0.5% Tween 20, followedby incubation (1 : 1000 dilution) for 16 h with antisera speci®c
for either COX-1 or COX-2. After washing three times for5 min each with 0.1% Tween 20 in TBS, the blots wereincubated for 1 h at room temperature with 1 : 2000 dilution
of sheep anti-mouse or donkey anti-rabbit secondaryantibodies conjugated to horseradish peroxidase. Bands werevisualized by an enhanced chemiluminescence (ECL) detec-tion system.
Immunohistochemical analysis of COX-1 and COX-2protein distribution in renal tissue
Localization of COX-1 and COX-2 expression was assessedin renal tissue isolated from three cirrhotic rats with ascites
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al892

and three control rats. Animals were anaesthetized with ani.m. injection of ketamine (50 mg kg71) and sacri®ced. Thekidneys were rapidly resected and cut to the appropriate size
to facilitate e�cient ®xative penetration of the molecularbiology ®xative (MBF). MBF is an aqueous bu�ered solutioncontaining organic and inorganic salts, supplemented with abacteriostatic and fungistatic agent and provides excellent
preservation of tissue structure and COX antigenicity. Tissueswere ®xed for 24 h at 48C, transferred to 70% ethanol,embedded in para�n, sectioned at 5 mm onto Fisher Gold
SuperFrost Plus glass slides and ®nally, depara�nized inxylene and re-hydrated in descending alcohols. Tissues werethen blocked for endogenous peroxidase (3% H2O2 in
MeOH) and avidin/biotin (Avidin Biotin Blocking Kit SP-2001, Vector Laboratories, Burlingame, CA, U.S.A.). Sec-tions were permeabilized in TNB-BB (0.1 M Tris pH 7.5,
0.015 M NaCl, 0.5% blocking agent, 0.3% Triton-X, 0.2%saponin), and incubated overnight at 48C with polyclonalrabbit anti-human COX-2 serum diluted to 2.5 mg ml71
(Oxford Biomedical Research). COX-1 was immunolocalized
with the anti-ovine monoclonal antibody (diluted to1 mg ml71) (Oxford Biomedical Research). Immunoreactivecomplexes were detected using tyramide signal ampli®cation
(TSA-indirect, NEN Life Science), and were visualized withthe peroxidase substrates AEC or DAB. Control sectionswere treated with isotype-matched controls, or were pre-
incubated with 100 fold excess of human recombinant COX-1or COX-2 protein. To ensure rigid inter-slide consistency allslides were stained simultaneously on an autoimmunostainer.
Pathological changes were described by a licensed pathologistfollowing preparation of standard hematoxylin and eosinstaining.
Drug administration studies
Study 1 The goal of this study was to investigate the e�ects
of selective COX-1 (SC-560) and COX-2 (celecoxib)inhibitors on renal function in conscious rats with cirrhosisand ascites. For this purpose, 28 rats with cirrhosis and
ascites were anaesthetized with an i.m. injection of ketamine(50 mg kg71) and prepared with a PVC-50 catheter in the leftfemoral artery for hemodynamic measurements and bloodcollection, a double-lumen PVC-100 catheter in the right
jugular vein for the infusion of substances, and a PVC-50tube in the bladder for urine collection. The femoral arterycatheter was connected to a highly sensitive transducer and a
multichannel recorder (MX4P and MT4, Lectromed Ltd,Jersey, Channel Islands, U.K.) to register pulsatile meanarterial pressure (MAP) and heart rate (HR), while the
jugular vein catheter was continuously perfused with Ringersolution (0.5 ml h71). Catheters were connected to a swivel(Harvard Apparatus, South Natick, MA, U.S.A.) and
animals were placed in rectangular cages with no restrictionof movement. Twenty-four hours later, a priming dose of 125I-Iothalamate (0.37 mCi) and para-aminohippurate (PAH)(3 mg) was given through the jugular vein, followed by a
constant infusion (2 ml h71) of a Ringer solution containing125I-Iothalamate (0.37 mCi ml71) and PAH (3 mg ml71).Animals were equilibrated for 1 h and after two baseline
20-min urine collection periods received 1 ml kg71 of 2%Tween 80 in Dulbecco's Phosphate Bu�ered Saline (DPBS)containing the following: Group 1 (n=8): Placebo; Group 2
(n=10): Selective COX-1 inhibitor, SC-560 (20 mg kg71, i.v.);Group 3 (n=10): Selective COX-2 inhibitor, celecoxib(20 mg kg71, i.v.).
The dose of SC-560 was selected from previous studiesdemonstrating inhibition of constitutive PG synthesis ineuvolemic rats (Smith et al., 1998; Wallace et al., 2000;Gretzer et al., 2001). The dose of celecoxib was selected from
previous studies reporting complete inhibition of PGsynthesis in the rat carrageenan footpad and airpouch modelsof in¯ammation (Smith et al., 1998; Wallace et al., 2000).
Moreover, by using the zymosan-induced in¯ammationmodel in rats, Niederberger et al. (2001) have recentlyreported that celecoxib retains its anti-in¯ammatory e�cacy
at doses of up to 100 mg kg71.Subsequently, four 20-min urine collection periods were
performed and changes in MAP, HR, urine volume (V),
urinary sodium excretion (UNaV), glomerular ®ltration rate(GFR) and renal plasma ¯ow (RPF) were recorded duringthe entire period. At the midpoint of each clearance period, a0.5 ml blood sample was obtained. Urinary PGE2 excretion
(UPGE2V) was measured under baseline conditions andduring the fourth 20-min urine collection period followingthe administration of COX inhibitors.
Sodium and potassium concentrations in plasma and urinesamples were measured by ¯ame photometry (IL 943,Instrumentation Laboratory, Lexington, MA, U.S.A.) and
serum osmolality by the osmometric depression of thefreezing point in an Advanced Instruments Osmometer(model 3MO, Needham, MA, U.S.A.). GFR and RPF were
estimated from 125I-Iothalamate and PAH clearance respec-tively, using the standard formula: CIothalamate=urinary 125Icounts6V/plasma 125I counts and CPAH=urinary PAHconcentration6V/plasma PAH concentration. The radio-
activity of 125I-Iothalamate samples was counted in anautomatic scintillation counter (Wallac, Turku, Finland).PAH was determined by RP ±HPLC as described (Decosterd
et al., 1997) with modi®cations. Brie¯y, 2 ml of plasma orurine in MeOH (®nal volume 25 ml) were injected into a RP ±HPLC system which consisted of a Waters integrated system
controller (model 600E) equipped with a 996 PhotodiodeArray Detector (DAD) and Millennium HPLC analysissoftware (Waters, Milford, MA, U.S.A.). For analysis ofPAH, a HPLC column (either a Kromasil 100 C18 (5 mm,
4.66250 mm) or a Tracer Extrasil ODS2 (5 mm,4.66250 mm) was eluted with a linear gradient of MeOH:ci-trate-citric acid pH 3.9 (from 1 : 99 to 15 : 85, v v71 over
15 min) at a ¯ow rate of 1.0 ml min71. The spectrophoto-metric UV-VIS DAD was set at 273 nm. PGE2 levels in urinewere measured by speci®c EIA after extraction of samples on
Sep-Pack C18 cartridges.
Study 2 The aim of this study was to investigate the e�ect
of SC-560 and celecoxib on the renal diuretic and natriureticresponses to furosemide in rats with cirrhosis and ascites.Twenty-six rats with cirrhosis and ascites were prepared asdescribed in Study 1 and received placebo (n=6), the selective
COX-1 inhibitor SC-560 (20 mg kg71, i.v.) (n=10) or theselective COX-2 inhibitor celecoxib (20 mg kg71, i.v.)(n=10). Sixty minutes later, they received an i.v. injection
of furosemide (5 mg kg71) and changes in V, UNaV, GFRand RPF were recorded during four 20-min urine collectionperiods. In an additional group of 13 rats with cirrhosis and
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al 893

ascites, the e�ects of increasing doses of SC-560 (10 and30 mg kg71, i.v) and celecoxib (10 and 30 mg kg71, i.v,) onthe diuretic and natriuretic response to furosemide were also
evaluated.
Study 3 The aim of this study was to investigate the e�ect ofSC-560 and celecoxib on renal water metabolism in rats with
cirrhosis and ascites. Renal water metabolism was estimated incirrhotic rats resting in metabolic cages, as follows: two hoursafter removing water and food, a water load (50 ml kg71) was
administered via a gastric tube inserted under light etheranaesthesia. Immediately afterwards, the animals were re-introduced into their metabolic cages where each spontaneous
urine void was individually collected for a total period of 3 h.The renal ability of these animals to excrete free water wasestablished by measuring the minimum urinary osmolality
(mUOsm) from the osmometric depression of the freezingpoint of each spontaneously voided sample and by gravime-tically measuring the percentage (%) of the water loadexcreted during the 3-h urine collection period. After a 24-h
period, animals received 1 ml kg71 of 2% Tween 80 in 0.5%carboxymethylcellulose containing the following treatmentsand doses selected from Smith et al. (1998), Wallace et al.
(2000), Gretzer et al. (2001) and Niederberger et al. (2001).Group 1 (n=6): Placebo; Group 2 (n=7): SC-560 (30 mgkg71, p.o.); Group 3 (n=8): celecoxib (30 mg kg71, p.o.).
Twenty minutes after receiving the drug, the animals weresubmitted to a second oral water load of 50 ml kg71 and thepercentage of water load excreted and the mUOsm were
again determined during the 3-h period following the wateradministration (see above).At the end of each study, tissue specimens were obtained
from the middle liver lobe of each animal, ®xed in 10%
bu�ered formalin and stained with hematoxylin-eosin,reticulin and Masson's trichrome for histological examina-tion.
Statistical analysis of the results was performed by one-wayANOVA, Newman-Keuls and paired and unpaired Student'st-tests, as appropriate. Data are expressed as mean+s.e.m.
and were considered signi®cant at a P level of 0.05 or less.All animal studies were conducted in accordance with the
criteria of the Investigation and Ethics Committee of theHospital ClõÂ nic and the European Community laws govern-
ing the use of experimental animals.
Results
Animals treated with CCl4 showed the characteristic features
of micronodular cirrhosis (i.e. a stage of well-establishedcirrhosis with a combination of nodular regeneration of livercell plates surrounded by thick connective tissue septa and
proliferating bile ducts). The volume of ascites of cirrhoticrats ranged between 12 and 40 ml.Constitutive COX-1 and COX-2 protein expression was
detected by Western blot and immunohistochemistry analysis
in renal tissue collected from rats with cirrhosis and ascites(Figures 1 ± 3). However, whereas COX-1 protein expressionwas found to be unchanged as compared to controls, COX-2
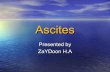
expression was consistently up-regulated in kidneys fromcirrhotic rats (Figure 1). In these animals, COX-1 immunor-eactivity was observed in the collecting ducts, renal
vasculature, and papillary interstitial cells, being its expres-sion intense in the papillary collecting ducts and low-to-moderate in the cortical collecting ducts (Figure 2). On the
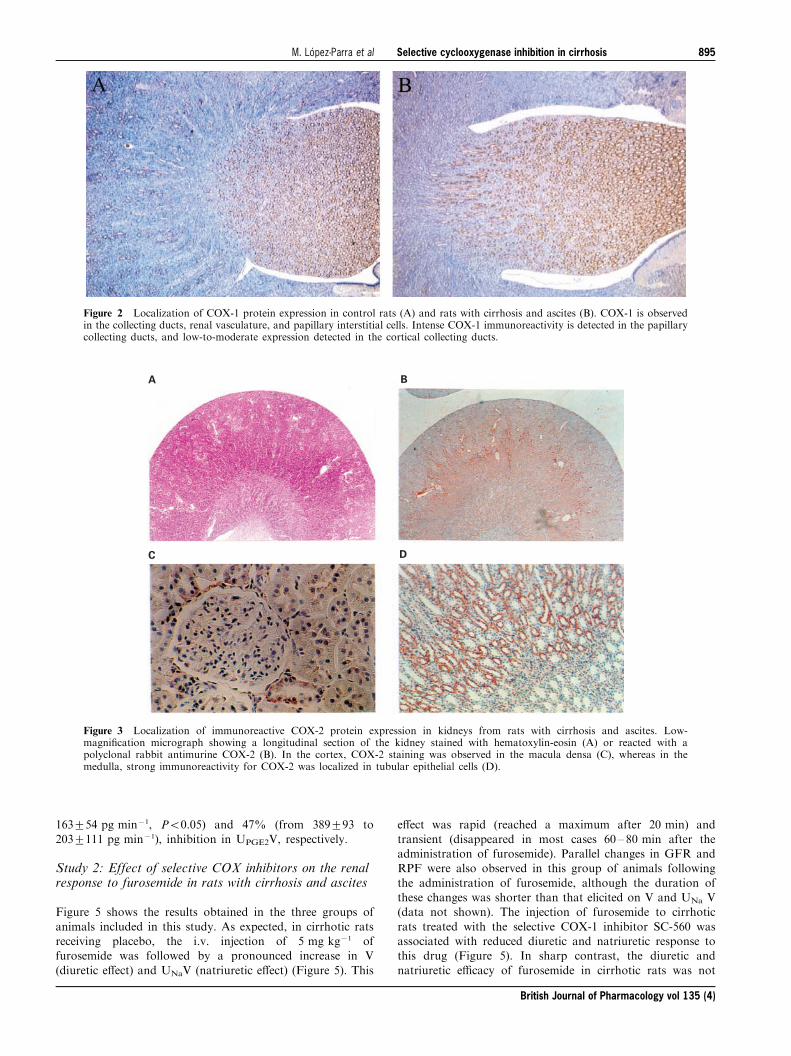
other hand, positive COX-2 immunoreactive protein waslocalized in the macula densa and outer medulla collectingducts (Figure 3).
Study 1: Effect of selective COX inhibitors on renalhemodynamics and renal excretory function in rats withcirrhosis and ascites
No statistically signi®cant di�erences were detected in thethree groups of rats receiving placebo, SC-560 or celecoxib
with respect to baseline body weight, MAP, HR, serumsodium and potassium concentrations, serum osmolality, V,UNaV, UPGE2V, GFR and RPF (Table 1).
Figure 4 shows the e�ects of placebo, SC-560 or celecoxibon V, UNaV, GFR and RPF in cirrhotic rats with ascites.The i.v. administration of the selective COX-1 inhibitor SC-
560 signi®cantly decreased V, UNaV, GFR and RPF incirrhotic rats. In these animals, renal function was impairedas early as 20 min following SC-560 administration andexperienced a progressive decline throughout the entire study
period, except for UNaV which reached a maximum plateauat 40 min after the administration of the drug (Figure 4). Incontrast, the renal e�ects associated with selective COX-2
inhibition with celecoxib were similar to those of placeboexcept that celecoxib induced a reduction in V which reachedstatistical signi®cance at 60 min after administration of the
drug (Figure 4). This e�ect, however, was transient andrapidly reversed and after 80 min of receiving celecoxib, theV values in this group of animals did not di�er from those ofthe placebo group. No changes in MAP and HR were
observed throughout the entire course of the study in anygroup of cirrhotic animals (data not shown).
The administration of SC-560 and celecoxib to cirrhotic
rats was associated with a 48% (from 312+82 to
Figure 1 Renal COX-1 and COX-2 protein levels. Upper panels:representative Western blot analysis of COX-1 (Mr, 70 kDa) andCOX-2 (Mr, 72 kDa) in renal tissue samples from two control rats(CT1 and CT2) and two cirrhotic rats with ascites (CH1 and CH2).Renal protein extracts were electrophoresed and probed with speci®canti-COX-1 and anti-COX-2 antibodies. Lower panels: COX-1 andCOX-2 band intensities were determined by scanning densitometry.Results show the mean+s.e.m. of six cirrhotic and seven control rats.
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al894
163+54 pg min71, P50.05) and 47% (from 389+93 to203+111 pg min71), inhibition in UPGE2V, respectively.
Study 2: Effect of selective COX inhibitors on the renalresponse to furosemide in rats with cirrhosis and ascites
Figure 5 shows the results obtained in the three groups of
animals included in this study. As expected, in cirrhotic ratsreceiving placebo, the i.v. injection of 5 mg kg71 offurosemide was followed by a pronounced increase in V
(diuretic e�ect) and UNaV (natriuretic e�ect) (Figure 5). This
e�ect was rapid (reached a maximum after 20 min) andtransient (disappeared in most cases 60 ± 80 min after theadministration of furosemide). Parallel changes in GFR andRPF were also observed in this group of animals following
the administration of furosemide, although the duration ofthese changes was shorter than that elicited on V and UNa V(data not shown). The injection of furosemide to cirrhotic
rats treated with the selective COX-1 inhibitor SC-560 wasassociated with reduced diuretic and natriuretic response tothis drug (Figure 5). In sharp contrast, the diuretic and
natriuretic e�cacy of furosemide in cirrhotic rats was not
Figure 2 Localization of COX-1 protein expression in control rats (A) and rats with cirrhosis and ascites (B). COX-1 is observedin the collecting ducts, renal vasculature, and papillary interstitial cells. Intense COX-1 immunoreactivity is detected in the papillarycollecting ducts, and low-to-moderate expression detected in the cortical collecting ducts.
C
BA
D
Figure 3 Localization of immunoreactive COX-2 protein expression in kidneys from rats with cirrhosis and ascites. Low-magni®cation micrograph showing a longitudinal section of the kidney stained with hematoxylin-eosin (A) or reacted with apolyclonal rabbit antimurine COX-2 (B). In the cortex, COX-2 staining was observed in the macula densa (C), whereas in themedulla, strong immunoreactivity for COX-2 was localized in tubular epithelial cells (D).
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al 895

a�ected by celecoxib (Figure 5). Consequently, rats treatedwith SC-560 showed a pronounced reduction in overall urine
output and cumulative sodium excretion over the 80 minperiod after furosemide injection, whereas these parametersremained unaltered in those rats treated with celecoxib
(Figure 6). The decrease in the response to furosemide inrats receiving SC-560 was dose-dependent and reachedstatistical signi®cance at doses of 20 and 30 mg kg71 (Figure6).
Study 3: Effects of COX inhibitors on renal watermetabolism in rats with cirrhosis and ascites.
Under baseline conditions, all three treatment groups exhibitedsimilar renal ability to excrete free water, as estimated by the
percentage of water load excreted (placebo: 82+11%; SC-560:92+6% and celecoxib: 86+7%) and mUOsm (Placebo:103+15 mOsm kg71; SC-560: 69+5 mOsm kg71 and celecox-ib: 88+17 mOsm kg71). Figure 7 shows the percentage
of water load excreted and mUOsm under baseline conditions
and following the oral administration of the drugs to ratswith cirrhosis and ascites. In these animals, neither placebo,SC-560 or celecoxib produced any signi®cant change in
either the percentage of water load excreted or mUOsm(Figure 7).
Table 1 Baseline values for the three groups of cirrhotic rats receiving placebo, SC-560 or celecoxib included in Study 1.
Placebo (n=8) SC-560 (n=10) Celecoxib (n=10)
Body weight (g) 595+28 569+21 569+30MAP (mmHg) 90+7 91+6 91+6HR (beats min71) 439+2 436+17 401+13Serum sodium (mEq l71) 138+1 130+7 133+3Serum potassium (mEq l71) 3.9+0.2 3.7+0.2 3.8+0.2Serum osmolality (mOsm kg71) 294+2 292+3 290+2V (ml min71) 31+5 28+4 28+4UNaV (mEq min71) 1.9+0.2 1.8+0.3 1.8+0.3UPGE2V (pg min71) 212+92 312+82 389+93GFR (ml min71) 3.6+0.5 3.3+0.3 3.2+0.2RPF (ml min71) 13.7+1.6 12.9+2.1 14.2+1.7
Figure 4 E�ect of selective COX inhibitors on renal function in ratswith cirrhosis and ascites. Urine ¯ow (V), urinary sodium excretion(UNaV), glomerular ®ltration rate (GFR) and renal plasma ¯ow(RPF) were measured before (720 and 0 min) and up to 80 min afterthe i.v. administration of placebo (n=8), the selective COX-1inhibitor (SC-560, 20 mg kg71, n=10) or the selective COX-2inhibitor (celecoxib, 20 mg kg71, n=10) to rats with cirrhosis andascites. Results are given as mean+s.e.m. Data are compared withthe Student's t-test for paired data. *P50.05; **P50.025 and***P50.001 vs values at 0 min.
Figure 5 E�ect of selective COX inhibitors on the renal response tofurosemide in rats with cirrhosis and ascites. Animals received i.v.placebo (n=6), the selective COX-1 inhibitor (SC-560, 20 mg kg71,n=10) or the selective COX-2 inhibitor (celecoxib, 20 mg kg71,n=10) and 1 h later they were challenged with an i.v. injection offurosemide (5 mg kg71) (time 0 min). Changes in urine ¯ow (V) andurinary sodium excretion (UNaV) were recorded for four 20-minurine collection periods after the injection of furosemide. Results aregiven as mean+s.e.m. Data are compared by the Student's t-test forunpaired data. *P50.05; **P50.025 and ***P50.005 vs placebo-treated group.
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al896

Discussion
Renal PG synthesis is markedly increased in patients with
cirrhosis and ascites as compared to patients with compen-sated cirrhosis (no ascites) and normal subjects (Arroyo et al.,1986; Dunn, 1984; Arroyo et al., 1983; Planas et al., 1983). Incompensated cirrhosis, this increase is a homeostatic response
to antagonize the exacerbated activity of the endogenousvasoconstrictor systems (i.e. the renin-angiotensin system, thesympathetic nervous system and the antidiuretic hormone
(ADH)). Two lines of evidence support this contention.Firstly, acute PG inhibition with NSAIDs (indomethacin,ibuprofen, naproxen, sulindac or aspirin) in patients with
cirrhosis and ascites is associated with a signi®cant decreasein V, UNaV, GFR and RPF (Dunn, 1984; Arroyo et al.,1983; Boyer et al., 1979; Mirouze et al., 1983; Zipser et al.,
1979). Patients with high plasma renin activity and plasmanorepinephrine concentrations are particularly sensitive tothese adverse e�ects. NSAIDs do not impair renal function inpatients with compensated cirrhosis who do not show
increased activity of the renin-angiotensin and sympatheticnervous systems. Secondly, acute PG inhibition with aspirinin patients with cirrhosis, ascites and increased plasma ADH
levels is associated with a signi®cant reduction in the renalability to excrete free water (Pe rez-Ayuso et al., 1984). Inaddition, PGs are also important in the renal response to
diuretics since the administration of aspirin, naproxen,indomethacin and sulindac suppresses the renal hemody-namic e�ect and reduces the natriuretic e�cacy of furosemide
in cirrhotic patients with ascites (Planas et al., 1983).Although the role of PGs in the maintenance of renal
function in cirrhosis is well established, at present it isunknown which COX isoform (COX-1 or COX-2) is
responsible for the synthesis of PGs involved in renalhomeostasis in this disease. Under normal conditions, both
Figure 6 Diuretic and natriuretic responses to furosemide in rats with cirrhosis and ascites treated with increasing doses ofselective COX inhibitors. Graph bars show the overall urine output and the cumulative sodium excretion over the 80 min after theadministration of furosemide (5 mg kg71) to di�erent groups of rats treated with placebo (0 mg kg71), SC-560 (10, 20 or30 mg kg71) or celecoxib (10, 20 or 30 mg kg71). Results are given as mean+s.e.m. Data are compared by the Student's t-test forunpaired data and P values denote statistically signi®cant di�erences with respect to the placebo-treated group.
Figure 7 E�ects of selective COX inhibitors on renal watermetabolism in rats with cirrhosis and ascites. The percentage (%)water load excreted (A) and the mUOsm (B) were measured beforeand after the administration of placebo (n=6), SC-560 (30 mg kg71,n=7) or celecoxib (30 mg kg71, n=8) to cirrhotic rats with ascites.Results represent the mean+s.e.m. and data are compared by theStudent's t-test for paired data.
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al 897

COX-1 and COX-2 are constitutively expressed in thekidneys (O'Neill & Ford-Hutchinson, 1993; Harris et al.,1994; Vio et al., 1997; Jensen & Kurtz, 1997; Khan et al.,
1998; Bosch-Marce et al., 1999). Speci®cally, in normal rats,COX-1 is mainly expressed in cells of the collecting duct andrenal vasculature and in a small number of papillaryinterstitial cells, while COX-2 expression is consistently focal
and limited to the macula densa of the juxtaglomerularapparatus, epithelial cells of the thick ascending limb andpapillary interstitial cells (Khan et al., 1998; Vio et al., 1997;
Harris et al., 1994; Jensen & Kurtz, 1997). Our results showthat both COX-1 and COX-2 are also present in kidneysfrom rats with cirrhosis and ascites. Moreover, whereas the
expression of COX-1 was found to be unchanged, theexpression of COX-2 was up-regulated in kidneys of cirrhoticrats. These ®ndings are consistent with the notion that COX-
2, but not COX-1, is regulated in a cell-speci®c fashion inresponse to altered volume status. Indeed, increased COX-2expression has been reported in the macula densa and peri-macula densa region of rats and dogs with chronic salt
depletion and in the renal medulla of rats with a high-saltdiet (Khan et al., 1998; Harris et al., 1994; Jensen & Kurtz,1997; Yang et al., 1998). Furthermore, increased COX-2
expression has been reported in the renal medulla of water-deprived rats (Yang et al., 1999). Collectively, these resultssuggest that renal COX-2 up-regulation in cirrhosis is likely
to be a consequence of changes in volume status, althoughthe exact mechanism for this phenomenon is, at present, notunderstood.
Despite cirrhotic rats showing increased COX-2 proteinimmunoreactivity in the renal area, renal function in theseanimals appears to be mainly dependent on PGs derived fromCOX-1. In fact, in Study 1 of this investigation, we observed a
signi®cant inhibition in renal PGE2 synthesis concomitant withmarked impairment in renal haemodynamics and renal sodiumhandling following the administration of a selective COX-1
inhibitor (SC-560) to CCl4-induced cirrhotic rats. In contrast,the selective COX-2 inhibitor celecoxib did not compromiserenal function in cirrhotic rats. Interestingly, and although
celecoxib administration was not associated with severe renale�ects in cirrhotic rats, this compound reduced UPGE2V tolevels equivalent to SC-560. McAdam et al. (1999) also found asimilar suppression in urinary PG excretion in both healthy
subjects treated with celecoxib and in those receiving ibuprofen.Taken together, these results suggest that urinary PGs arederived from both COX-1 and COX-2, yet only those from
COX-1 are involved in the maintenance of renal function incirrhosis. The physiological signi®cance of PGs derived fromCOX-2 in the kidneys, not only in disease states, but also in
healthy conditions, remains to be determined.PGs are clearly involved in the renal natriuretic response to
loop diuretics (Katayama et al., 1984). Loop diuretics, such
as furosemide, are the most powerful diuretics currentlyavailable. These drugs inhibit sodium reabsorption in theascending limb of the loop of Henle by acting on a speci®cco-transport system, the Na+-2Cl7K+ carrier (Puschett,
1981). Loop diuretics also increase GFR and renal blood¯ow and the renal production of PGE2 whereas NSAIDs canmodulate the renal vasodilatory e�ect and the natriuretic
e�ciency of these drugs (Katayama et al., 1984). The resultsobtained in Study 2 demonstrate that response to furosemidein cirrhotic rats is mainly dependent on COX-1 derived PGs
and that selective COX-2 inhibition spares furosemide-induced renal salt transport in cirrhosis. It is noteworthy topoint out that in cirrhotic rats the e�ects of selective COX-1
inhibition with SC-560 on furosemide-induced diuretic andnatriuretic response were dose-dependent. However, contraryto what was previously reported by Katayama et al. (1984),who found that indomethacin can either enhance or inhibit
the e�ect of furosemide-induced natriuresis depending on thedose of this conventional NSAID used, we found that at lowdoses (10 mg kg71), SC-560 induced no changes whereas
higher doses (20 and 30 mg kg71) signi®cantly inhibited theresponse to furosemide.
PGs are also involved in renal water transport by
modulating the tubular actions of ADH (Mattix & Badr,2000). Speci®cally, PGE2 inhibits the hydroosmotic e�ect ofADH whereas PG inhibition with NSAIDs enhances the
tubular e�ect of this hormone (Mattix & Badr, 2000; He bert etal., 1990). In our study, neither SC-560 nor celecoxib modi®edrenal water metabolism in rats with cirrhosis and ascites.These results are in sharp contrast with those previously
obtained with the NSAID ketorolac which signi®cantlyimpaired the ability to excrete free water in cirrhotic rats(Bosch-Marce et al., 1999). Given that ketorolac is a mixed
COX-1/COX-2 inhibitor, these ®ndings suggest that renalwater homeostasis in cirrhosis is dependent on PGs derivedfrom both COX isoforms. Thus, a compensatory mechanism
appears to be present in cirrhotic rat kidneys, in such a waythat when only one isoform is inhibited, water metabolism canbe maintained by PGs produced by the other isoform.
Controlled clinical studies have demonstrated that selectiveCOX-2 inhibitors have equal therapeutic e�cacy but with alower incidence of gastrointestinal ulcers and erosions thanconventional NSAIDs (Emery et al., 1999; Bombardier et al.,
2000). The marketed selective COX-2 inhibitors rofecoxiband celecoxib have also been evaluated in randomizedcontrolled trials in terms of their e�ects on renal PGs, renal
function and occurrence of adverse renal events. Whereas inelderly subjects, rofecoxib did not produce any signi®cantalteration in GFR after 2 weeks of treatment, it produced a
reduction in urinary sodium excretion similar to that withindomethacin during the ®rst 3 days of therapy (Catella-Lawson et al., 1999). In contrast, in elderly patients with mildrenal impairment and stabilized on a low-sodium diet,
rofecoxib produced decreases in GFR of similar magnitudeto those observed in indomethacin-treated subjects, withouta�ecting urinary sodium excretion (Swan et al., 2000). In
elderly patients, celecoxib, like rofecoxib, failed to decreaseGFR, but did produce transient reductions in urinary sodiumexcretion similar to those of naproxen (Whelton et al., 2000).
Finally, in a trial in salt-depleted subjects, celecoxib not onlypromoted sodium retention but also produced signi®cantdose-related decreases in GFR (Rossat et al., 1999). There-
fore, the unwanted renal-side e�ects of selective COX-2inhibitors still remain, at present, uncharacterized. Thissubject is particularly important in circumstances moresusceptible to NSAID-induced renal failure, such as advanced
liver disease, congestive heart failure and nephrotic syn-drome. For this reason, our ®ndings in the experimentalmodel of cirrhosis warrant further studies in humans
investigating the feasibility of selective COX-2 inhibitorspossibly being the anti-in¯ammatory option of choice inpatients with chronic liver disease.
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al898

These studies were supported in part by Ministerio de Ciencia yTecnologõ a (SAF 00/0043) and Fondo de Investigaciones Sanitar-ias (FIS 00/0616). M. Lo pez-Parra and E. Titos were supported byMinisterio de Ciencia y Tecnologõ a and Ministerio de Sanidad y
Consumo (BEFI 98/9314), respectively. A. PlanagumaÁ received afellowship from IDIBAPS. The authors are indebted to M. Borrajofor expert technical assistance.
References
ARROYO, V., PLANAS, R., GAYA, J., DEULOFEU, R., RIMOLA, A.,
PEÂ REZ-AYUSO, R.M., RIVERA, F. & RODEÂ S, J. (1983). Sympa-thetic nervous activity, renin-angiotensin system and renalexcretion of prostaglandin E2 in cirrhosis. Relationship tofunctional renal failure and sodium and water excretion. Eur. J.Clin. Invest., 13, 271 ± 278.
ARROYO, V., GINEÂ S, P., RIMOLA, A. & GAYA, J. (1986). Renalfunction abnormalities, prostaglandins, and e�ects of nonster-oidal anti-in¯ammatory drugs in cirrhosis with ascites. Anoverview with emphasis on pathogenesis. Am. J. Med., 81,104 ± 122.
BOMBARDIER, C., LAINE, L., REICIN, A., SHAPIRO, D., BURGOS-
VARGAS, R., DAVIS, B., DAY, R., FERRAZ, M.B., HAWKEY, C.J.,
HOCHBERG, M.C., KVIEN, T.K. & SCHNITZER, T.J. (2000).Comparison of upper gastrointestinal toxicity of rofecoxib andnaproxen in patients with rheumatoid arthritis. N. Engl. J. Med.,343, 1520 ± 1528.
BOSCH-MARCEÂ , M., CLAÁ RIA, J., TITOS, E., MASFERRER, J.L.,
ALTUNA, R., POO, J.L., JIMEÂ NEZ, W., ARROYO, V., RIVERA, F.
& RODEÂ S, J. (1999). Selective inhibition of cyclooxygenase-2spares renal function and prostaglandin synthesis in cirrhotic ratswith ascites. Gastroenterology, 116, 1167 ± 1175.
BOYER, T.D., ZIA, P. & REYNOLDS, T.B. (1979). E�ect ofindomethacin and prostaglandin A1 on renal function andplasma renin activity in alcoholic liver disease. Gastroenterology,77, 215 ± 222.
CATELLA-LAWSON, F., MCADAM, B., MORRISON, B.W., KAPOOR,
S., KUJUBU, D., ANTES, L., LASSETER, K.C., QUAN, H., GERTZ,
B.J. & FILTZGERALD, G.A. (1999). E�ects of speci®c inhibitionon cyclooxygenase-2 on sodium balance, hemodynamics andvasoactive eicosanoids. J. Pharm. Exp. Ther., 289, 735 ± 741.
CLAÁ RIA, J. & JIME NEZ, W. (1999). Renal dysfunction and ascites incarbon tetrachloride-induced cirrhosis in rats, In The Liver andthe Kidney. ed. Arroyo, V., Schrier, R.W., Rode s, J., GineÁ s, P. pp.379 ± 396, Boston: Blackwell Science.
DECOSTERD, L.A., KARAGIANNIS, A., ROULET, J.M., BEÂ LAZ, N.,
APPENZELLER, M., BUCLIN, T., VOGEL, P. & BIOLLAZ, J. (1997).High-performance liquid chromatography of the renal blood¯ow marker p-aminohippuric acid (PAH) and its metabolite N-acetyl PAH improves PAH clearance measurements. J. Chroma-tog., 703, 25 ± 36.
DUNN, M.J. (1984). Role of eicosanoids in the control of renalfunction in severe hepatic disease. Gastroenterology, 87, 1392 ±1395.
EMERY, P., ZEIDLER, H., KVIEN, T.K., GUSLANDI, M., NAUDIN, R.,
STEAD, H., VERBURG, K.M., ISAKSON, P.C., HUBBARD, R.C. &
GEIS, G.S. (1999). Celecoxib versus diclofenac in long-termmanagement of rheumatoid arthritis: randomised double-blindcomparison. Lancet, 354, 2106 ± 2111.
GRETZER, B., MARICIC, N., RESPONDEK, M., SCHULIGOI, R. &
PESKAR, B.M. (2001). E�ects of speci®c inhibition of cyclo-oxygenase-1 and cyclo-oxygenase-2 in the rat stomach withnormal mucosa and after acid challenge. Br. J. Pharmacol., 132,1565 ± 1573.
HARRIS, R.C., MCKANNA, J.A., AKAI, Y., JACOBSON, H.R., DUBOIS,
R.N. & BREYER, M.D. (1994). Cyclooxygenase-2 is associatedwith the macula densa of rat kidney and increases with saltrestriction. J. Clin. Invest, 94, 2504 ± 2510.
HEÂ BERT, R.L., JACOBSON, H.R. & BREYER, M.D. (1990). PGE2
inhibits AVP-induced water ¯ow in cortical collecting ducts byprotein kinase C activation. Am. J. Physiol., 259, F318 ± F325.
HERSCHMAN, H.R. (1996). Prostaglandin synthase 2. Biochim.Biophys. Acta., 1299, 125 ± 140.
HLA, T. & NEILSON, K. (1992). Human cyclooxygenase-2 cDNA.Proc. Natl. Acad. Sci. U.S.A., 89, 7384 ± 7388.
JENSEN, B.L. & KURTZ, A. (1997). Di�erential regulation of renalcyclooxygenase mRNA by dietary salt intake. Kidney Int., 52,1242 ± 1249.
KATAYAMA, S., ATTALLAH, A.A., STAHL, R.A., BLOCH, D.L. & LEE,
J.B. (1984). Mechanism of furosemide-induced natriuresis bydirect stimulation of renal prostaglandin E2. Am. J. Physiol., 247,F555 ± F561.
KHAN, K., VENTURINI, C.M., BUNH, R.T., BRASSARD, J.A., KOKI,
A.T., MORRIS, D.L., TRUMP, B.F., MAZIASZ, T.J. & ALDEN, C.L.
(1998). Interspecies di�erences in renal localization of cycloox-ygenase isoforms: implications in nonsteroidal antiin¯ammatorydrug-related nephrotoxicity. Toxic. Pathol., 26, 612 ± 620.
KUJUBU, D.A., FLETCHER, B.S., VARNUM, B.C., LIM, R.W. &
HERSCHMAN, H.R. (1991). TIS10, a phorbol ester tumorpromoter-inducible mRNA from Swiss 3T3 cells, encodes anovel prostaglandin synthase/cyclooxygenase homologue. J.Biol. Chem., 266, 12866 ± 12872.
MARNETT, L.J. & KALGUTKAR, A.S. (1999). Cyclooxygenase 2inhibitors: discovery, selectivity and the future. TIPS, 20, 465 ±469.
MASFERRER, J.L., SEIBERT, K., ZWEIFEL, B.S. & NEEDLEMAN, P.
(1992). Endogenous glucocorticoids regulate an induciblecyclooxygenase enzyme. Proc. Natl. Acad. Sci. U.S.A., 89,3917 ± 3921.
MATTIX, H.J. & BADR, K.F. (2000). Arachidonic acid metabolitesand the kidney, In The Kidney. ed. Brenner, B.M., Rector, F.C.pp. 756 ± 792, Philadelphia: Saunders.
MCADAM, B.F., CATELLA-LAWSON, F., MARDINI, I.A., KAPOOR, S.,
LAWSON, J.A. & FITZGERALD, G.A. (1999). Systemic biosynth-esis of prostacyclin by cyclooxygenase (COX)-2: the humanpharmacology of a selective inhibitor of COX-2. Proc. Natl.Acad. Sci. U.S.A., 96, 272 ± 277.
MIROUZE, D., ZIPSER, R.D. & REYNOLDS, T.D. (1983). E�ects ofinhibitors of prostaglandin synthesis on induced diuresis incirrhosis. Hepatology, 3, 50 ± 55.
NIEDERBERGER, E., TEGEDER, I., VETTER, G., SCHMIDTKO, A.,
SCHMIDT, H., EUCHENHOFER, C., BRAÈ UTIGAM, L., GROÈ SCH, S.
& GEISSLINGER, G. (2001). Celecoxib loses its anti-in¯ammatorye�cacy at high doses through activation of NF-kB. FASEB J.,15, 1622 ± 1624.
O'NEILL, G.P. & FORD-HUTCHINSON, A.W. (1993). Expression ofmRNA for cyclooxygenase-1 and cyclooxygenase-2 in humantissues. FEBS Lett., 330, 156 ± 160.
PAYAN, D.G. & KATZUNG, B.G. (1995). Nonsteroidal anti-in¯am-matory drugs; nonopioid analgesics; drugs used in gout, In Basic& Clinical Pharmacology. ed. Katzung, B.G. pp. 536 ± 559Norwalk: Appleton & Lange.
PEÂ REZ-AYUSO, R.M., ARROYO, V., CAMPS, J., RIMOLA, A., GAYA,
J., COSTA, J., RIVERA, F. & RODEÂ S, J. (1984). Evidence that renalprostaglandins are involved in renal water metabolism incirrhosis. Kidney Int., 26, 72 ± 80.
PLANAS, R., ARROYO, V., RIMOLA, A., PEÂ REZ-AYUSO, R.M. &
RODEÂ S, J. (1983). Acetylsalicylic acid suppresses the renalhemodynamic e�ect and reduces the diuretic action of furosemidein cirrhosis with ascites. Gastroenterology, 84, 247 ± 252.
PUSCHETT, J.B. (1981). Sites and mechanisms of diuretics in thekidney. J. Clin. Pharmacol., 21, 564 ± 574.
ROS, J., CLAÁ RIA, J., JIMEÂ NEZ, W., BOSCH-MARCEÂ , M., ANGELI, P.,
ARROYO, V., RIVERA, F. & RODEÂ S, J. (1995). Role of nitric oxideand prostacyclin in the control of renal perfusion in experimentalcirrhosis. Hepatology, 22, 915 ± 920.
ROSSAT, J., MAILLARD, M., NUSSBERGER, J., BRUNNER, H.R. &
BURNIER, M. (1999). Renal e�ects of selective cyclooxygenase-2inhibition in normotensive salt-depleted subjects. Clin. Pharma-col. Ther., 66, 76 ± 84.
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al 899

SWAN, S., RUDY, D.W., LASSETER, K.C., RYAN, C.F., BUECHEL,
K.L., LAMBRECHT, L.J., PINTO, M.B., DILZER, S.C., OBRDA, O.,
SUNDBLAD, K.J., GUMBS, C.P., EBEL, D.L., QUAN, H., LARSON,
P.J., SCHWARTZ, J.I., MUSLINER, T.A., GERTZ, B.J., BRATER, C.
& YAO, S.-L. (2000). E�ect of cyclooxygenase-2 inhibition onrenal function in elderly persons receiving a low-salt diet. Ann.Intern. Med., 133, 1 ± 9.
SEIBERT, K., ZHANG, Y., LEAHY, K., HAUSER, S., MASFERRER, J.,
PERKINS, W., LEE, L. & ISAKSON, P. (1994). Pharmacological andbiochemical demonstration of the role of cyclooxygenase 2 inin¯ammation and pain. Proc. Natl. Acad. Sci. U.S.A., 91, 12013 ±12017.
SMITH, C.J., ZHANG, Y., KOBOLDT, C.M., MUHAMMAD, J.,
ZWEIFEL, B.S., SHAFFER, A., TALLEY, J.J., MASFERRER, J.L.,
SEIBERT, K. & ISAKSON, P.C. (1998). Pharmacological analysis ofcyclooxygenase-1 in in¯ammation. Proc. Natl. Acad. Sci. U.S.A.,95, 13313 ± 13318.
VANE, J.R. (1971). Inhibition of prostaglandin synthesis as amechanism of action for the aspirin-like drugs. Nature, 231,232 ± 235.
VIO, C.P., CESPEDES, C., GALLARDO, P. & MASFERRER, J.L. (1997).Renal identi®cation of cyclooxygenase-2 in a subset of thickascending limb cells. Hypertension, 30, 687 ± 692.
WALLACE, J.L., McKNIGHT, W., REUTER, B.K. & VERGNOLLE, N.
(2000). NSAID-induced gastric damage in rats: requirement forinhibition of both cyclooxygenase 1 and 2. Gastroenterology, 199,706 ± 714.
WARNER, T.D., GIULIANO, F., VOJNOVIC, I., BUKASA, A., MITCH-
ELL, J.A. & VANE, J.R. (1999). Nonsteroid drug selectivities forcyclooxygenase-1 rather than cyclooxygenase-2 are associatedwith human gastrointestinal toxicity: a full in vitro analysis. Proc.Natl. Acad. Sci. U.S.A., 96, 7563 ± 7568.
WHELTON, A., SCHULMAN, G., WALLEMARK, C., DROWER, E.J.,
ISAKSON, P.C., VERBURG, K.M. & GEIS, G.S. (2000). E�ects ofcelecoxib and naproxen on renal function in the elderly. Arch.Intern. Med., 160, 1465 ± 1470.
YANG, T., SCHNERMANN, J.B. & BRIGGS, J.P. (1999). Regulation ofcyclooxygenase-2 expression in renal medulla by tonicity in vivoand in vitro. Am. J. Physiol., 277, F1 ± F9.
YANG, T., SINGH, I., PHAM, H., SUN, D., SMART, A., SCHNER-
MANN, J.B. & BRIGGS, J.P. (1998). Regulation of cyclooxygenaseexpression by dietary salt intake. Am. J. Physiol., 274, F481 ±F489.
ZIPSER, R., HOEFS, J.C., SPECKART, P.F., ZIA, P.K. & HORTON, R.
(1979). Prostaglandins: modulators of renal function and pressorresistance in chronic liver disease. J. Clin. Endocrinol. Metab., 48,895 ± 900.
(Received November 1, 2001Accepted November 23, 2001)
British Journal of Pharmacology vol 135 (4)
Selective cyclooxygenase inhibition in cirrhosisM. LoÂpez-Parra et al900
Related Documents
![INDEX [link.springer.com]978-1-4615-4737-2/1.pdf · Index Bladder (cant.) prostaglandins, 171-179 cyclooxygenase isofonns, 173--179 fetal development, 175 regulation of, 173-177 therapeutic](https://static.cupdf.com/doc/110x72/5e53ff3d431ff900b93c1802/index-link-978-1-4615-4737-21pdf-index-bladder-cant-prostaglandins-171-179.jpg)