Dec-2014-CSBRP

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dec-2014-CSBRP

Dec-2014-CSBRP
Aneurysms and DissectionAneurysms and Dissection
CSBR.Prasad, MD.,

Dec-2014-CSBRP
Aneurysm - Definition:
Localized abnormal dilation of a blood vessel or the heart
It may be congenital or acquired

Common sites
Dec-2014-CSBRP

Aneurysm of left ventricle
Dec-2014-CSBRP

Aneurysm of the left ventricle
Dec-2014-CSBRP

The gross morphology of aneurysms reveals several different pathological features:
Dec-2014-CSBRP

Dec-2014-CSBRP

Dec-2014-CSBRP
Types: True aneurysms:
Dilation of intact arterial wall or thinned ventricular wall of the heart Atherosclerotic, syphilitic, and congenital
vascular aneurysms, ventricular aneurysms following MI
False aneurysms / Pseudoaneurysms: A defect in the vascular wall leading to an
extravascular hematoma that freely communicates with the intravascular space (“pulsating hematoma”) ventricular rupture after MI that is contained by
a pericardial adhesion

True & False aneurysms
Dec-2014-CSBRP

Cardiac aneurysm
Dec-2014-CSBRP

Dec-2014-CSBRP
Complication: Both true and false aneurysms can
rupture, often with catastrophic consequences

Dec-2014-CSBRP
Morphological types: Saccular aneurysms:
Spherical outpouchings involving only a portion of the vessel wall vary from 5 to 20 cm in diameter and often contain thrombus
Fusiform aneurysms: Circumferential dilations of a long
vascular segment vary in diameter (up to 20 cm) and can involve extensive portions
These types are not specific for any disease or clinical manifestations

Dec-2014-CSBRP
Aneurysms:

Dec-2014-CSBRP
Pathogenesis of Aneurysms: Aneurysms can occur when the
structure or function of the connective tissue within the vascular wall is compromised Inherited defects in connective tissues Acquired connective tissue defects

Dec-2014-CSBRP
Pathogenesis of Aneurysms: The intrinsic quality of the vascular wall
connective tissue is poor The balance of collagen degradation and
synthesis is altered by inflammation and associated proteases
The vascular wall is weakened through loss of smooth muscle cells or the synthesis of noncollagenous or nonelastic extracellular matrix

Dec-2014-CSBRP
Pathogenesis of Aneurysms: The intrinsic quality of the vascular wall
connective tissue is poor Marfan syndrome:
Defective protein fibrillin leads to aberrant TGF-ß activity and weakening of elastic tissue
Loeys-Dietz syndrome: Mutations in TGF-ß receptors lead to defective
synthesis of elastin and collagens I and III Ehlers-Danlos syndrome:
Defective type III collagen synthesis Vitamin C deficiency:
Altered collagen cross-linking

Dec-2014-CSBRP
Pathogenesis of Aneurysms: The intrinsic quality of the vascular wall
connective tissue is poor The balance of collagen degradation and
synthesis is altered by inflammation and associated proteases
The vascular wall is weakened through loss of smooth muscle cells or the synthesis of noncollagenous or nonelastic extracellular matrix

Dec-2014-CSBRP
Pathogenesis of Aneurysms: The balance of collagen degradation and
synthesis is altered by inflammation and associated proteases Increased matrix metalloprotease (MMP)
expression AS, Vasculitis
Decreased expression of tissue inhibitors of metalloproteases (TIMPs) Inflammatory lesions – AS Local Inflammation – production of IL-4, IL-10

Dec-2014-CSBRP
Pathogenesis of Aneurysms: The intrinsic quality of the vascular wall
connective tissue is poor The balance of collagen degradation and
synthesis is altered by inflammation and associated proteases
The vascular wall is weakened through loss of smooth muscle cells or the synthesis of noncollagenous or nonelastic extracellular matrix

Dec-2014-CSBRP
Pathogenesis of Aneurysms: The vascular wall is weakened
through loss of smooth muscle cells or the synthesis of noncollagenous or nonelastic extracellular matrix Ischemia of the inner media
[Histo: Cystic medial degeneration] AS, Systemic hypertension Tertiary syphilis

Dec-2014-CSBRP
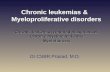
Cystic medial degeneration
Alcian Blue-PAS
Marfan’s syndromeMarfan’s syndrome
NormalNormal

Dec-2014-CSBRP
Important causes of aortic aneurysmsThe two most important causes of aortic
aneurysms: Atherosclerosis [AAA] Hypertension [Thoracic aortic aneurysm] Others:
Trauma Vasculitis Congenital defects & Infections

Dec-2014-CSBRP
Mycotic aneurysms: Mycotic aneurysms can originate: Septic embolus [infective endocarditis] Extension of an adjacent suppurative
process Circulating organisms directly infecting
the arterial wall

Dec-2014-CSBRP
Abdominal Aortic Aneurysm: AAA Atherosclerosis Men >50yrs Smokers

Dec-2014-CSBRP
Abdominal Aortic Aneurysm: MORPHOLOGY Usual position: below the renal
arteries and above the bifurcation of the aorta
Saccular or fusiform 15 cm in diameter, and up to 25
cm in length Usually contains a bland, laminated,
mural thrombus

Abdominal Aortic AneurysmUsual position:
Dec-2014-CSBRP

Dec-2014-CSBRP

Dec-2014-CSBRP
Variants of AAA:Three AAA variants merit special
mention because of their unusual features
Inflammatory AAA IgG4-related disease Mycotic AAA

Inflammatory AAA 5% to 10% of all AAA Typically seen in younger patients Back pain and Elevated inflammatory markers – CRP Histology:
Characterized by abundant lymphoplasmacytic inflammation with many macrophages, giant cells
Dense periaortic scarring that can extend into the anterior retroperitoneum
Localized immune response to the abdominal aortic wall
Dec-2014-CSBRP

IgG4-related disease AAA
High plasma levels of IgG4 Fibrosis Infiltrated by IgG4-expressing plasma cells Other organ systems may also be involved
Salivary, pancreas, biliary system
Dec-2014-CSBRP

Mycotic AAA Infected by the lodging of circulating
microorganisms in the wall
Dec-2014-CSBRP

Clinical Features of AAA Incidental finding – ‘pulsatile abdominal tumor’ Rupture into the peritoneal cavity or
retroperitoneal tissues with massive, potentially fatal hemorrhage
Obstruction of a vessel branching off from the aorta, resulting in ischemic injury to the supplied tissue
Embolism from atheroma or mural thrombus Impingement on an adjacent structure eg:
Compression of a ureter or erosion of vertebrae
Dec-2014-CSBRP

The risk of rupture - AAA Is directly related to the size
NIL - <4 cm 1% per year between 4 and 5 cm 11% per year between 5 and 6 cm 25% per year larger than 6 cm
Most aneurysms expand at a rate of 0.2 to 0.3 cm/year, but 20% expand more rapidly
Dec-2014-CSBRP
Aneurysms 5 cm or larger are managed aggressively

Thoracic Aortic Aneurysm - TAA Most commonly associated with
hypertension Other causes:
Marfan syndrome Loeys-Dietz syndrome
Dec-2014-CSBRP

Thoracic Aortic Aneurysm – TAAPresentation: Respiratory difficulties due to encroachment on
the lungs and airways Difficulty in swallowing due to compression of
the esophagus Persistent cough due to compression of the
recurrent laryngeal nerves Pain caused by erosion of bone Cardiac disease – IHD - as the aortic aneurysm
leads to AR Rupture
Dec-2014-CSBRP

Abdominal Aortic Aneurysm
Dec-2014-CSBRP

Thoracic Aortic Aneurysm – TAAPresentation:
Most patients with syphilitic aneurysms die of heart failure secondary to aortic valvular
incompetence
Dec-2014-CSBRP

Thoracic Aortic Aneurysm – TAA
Dec-2014-CSBRP

Thoracic Aortic Aneurysm – TAA
Dec-2014-CSBRP

Thoracic Aortic Aneurysm – TAA
Dec-2014-CSBRP

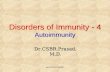
Thoracic Aortic Aneurysm – TAATree bark appearance - Syphilis
Dec-2014-CSBRP

Aortic Dissection Occurs when blood separates the
laminar planes of the media to form a blood-filled channel within the aortic wall
Occurs principally in two groups of patients: Men, 40 to 60 years with antecedent
hypertension (>90%) and Younger adults with abnormalities of
connective tissue affecting the aorta
Dec-2014-CSBRP

Aortic Dissection
Other causes: Arterial cannulization Pregnancy
Dec-2014-CSBRP

Aortic DissectionPathogenesis: Hypertension – Cystic medial degeneration Marfan syndrome Ehlers-Danlos syndrome Defects in copper metabolism
Dec-2014-CSBRP

Aortic Dissection - MORPHOLOGY
Dec-2014-CSBRP
Most frequent finding is cystic medial degeneration usually initiates with an intimal tear Spontaneous dissection:
Within 10 cm of the aortic valve Tears are typically transverse with sharp, jagged edges up to 1
to 5 cm in length Dissection can extend retrograde toward the heart as well as
distally Tear: Between the middle and outer thirds Rupture through the adventitia causing massive
hemorrhage Cardic tamponade “double-barreled aorta”

Aortic Dissection - MORPHOLOGY
Dec-2014-CSBRP

Dec-2014-CSBRP

Aortic dissection
Dec-2014-CSBRP

Dec-2014-CSBRP

Classification:
Dec-2014-CSBRP

Clinical Features: Proximal dissections are more serious and
dangerous (types I and II of the DeBakey)
PAIN: sudden onset of excruciating pain, usually beginning in the anterior chest, radiating to the back between the scapulae, and moving downward as the dissection progresses
Cardiac tamponade Aortic insufficiency Ischemic consequences
Dec-2014-CSBRP

Out come: In type A dissections: Mortality is 70% Most type B dissections can be
managed conservatively -75% survival rate
Dec-2014-CSBRP

E N D
Dec-2014-CSBRP
Related Documents