1 Viewing Gliptins – Cardiologist Prospective Dr. Neeraj Bhalla Senior Consultant and Director Deptt of Cardiology BLK Super Speciality Hospital

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Viewing Gliptins – Cardiologist Prospective Dr. Neeraj Bhalla
Senior Consultant and Director Deptt of Cardiology BLK Super Speciality Hospital


• Diabetes is a constellation of metabolic abnormalities
• As there is no unifying causative mechanism ; there is no unique treatment for it. Treatment includes managing its components
3

Gelfand EV et al, 2006; Vasudevan AR et al, 2005
Global cardiometabolic risk (CMR)
4

5
Impact of Hypoglycemia & weight gain in T2DM – Cardiovascular perspective

Hypoglycaemia & Weight gain
HbA1c
The challenge of tight glucose control
6

Hypoglycemia as a cause for cardiovascular events - Mechanisms
8
Desouza CV, et al. Diabetes Care. 2010;
33:1389–394

Metabolic Syndrome facts…
• The relative risk of developing diabetes , hypertension and CVD increases with an increase in body weight
1 kg weight gain CVD risk by 3.1 %
Diabetes risk by 4.5-9 %
Ref : Curr. Med. Chem. – Imm., Endoc. & Metab. Agents, 2001, Vol. 1, No. 1 ; IDF Defination
• 78% of patients with metabolic syndrome have insulin resistance, & 48% of people with insulin resistance have metabolic syndrome.
• People with metabolic syndrome are twice as likely to die from & thrice as likely to have stroke or heart attack then people without it
9

10
The Unmet need with current therapy for T2DM

Most Insulin secretagogues , including glimepiride, associated with increased mortality & cardiovascular risk compared with metformin
11
Monotherapy with the most used Insulin secretagogues (ISs), including glimepiride, glibenclamide,
glipizide, and tolbutamide, seems to be associated with increased mortality and cardiovascular risk
compared with metformin. Gliclazide and repaglinide appear to be associated with a lower risk
than other ISs
N = 107 806 subjectsfollowed for up to 9 years (median 3.3 years)
TK Schramm etal, European Heart Journal Advance Access published April 6, 2011
Haz
ard
Ratio
(%)

Hypoglycemia is Common with SUs
*Hypoglycemia: fingerstick blood glucose measurement 50 mg/dL (2.75 mmol/L)
1. Glucovance [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2004. 2. UKPDS Group. Lancet1998; 352: 837–853. 3. Draeger KE, et al. Horm Metab Res. 1996; 28: 419–425. 4. McGavin JK, et al. Drugs 2002;62; 1357–1364. 5. Metaglip [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2002
Sulfonylureas
Glipizide5Gliclazide4Chlorpropamide2Glyburide1
0
5
10
15
20
25
Inci
den
ce o
f H
ypo
gly
cem
ia (
%)
21.3%
15.3%
5%2.9%*
14%
11%
Glibenclamide3 Glimepiride3

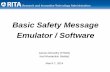
Weight Gain is a Common Side Effect of Diabetes Treatments
TZDs4–6
Metformin + TZD5,6,9
Metformin + SU1–3
Meglitinides4,7,8
SUs1–4
Metformin1–3
Weight Change (kg)OAD Agents
OAD=oral antidiabetic agent; SU=sulfonylurea; TZD=thiazolidinedione.1Glucophage [package insert]. Princeton, NJ: Bristol-Meyers Squibb Company, 2004. 2Glucovance [package insert]. Princeton, NJ: Bristol-Meyers Squibb Company, 2004. 3Metaglip [package insert]. Princeton, NJ: Bristol-Meyers Squibb Company, 2002. 4Malone M. Ann Pharmacother. 2005; 39: 2046–2055. 5Actos [package insert]. Indianapolis, Ind: Eli Lilly and Company, 2004. 6Avandia [package insert]. Research Triangle Park, NC: GlaxoSmithKline, 2005. 7Starlix [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2004. 8Prandin [package insert]. Princeton, NJ: Novo Nordisk, Inc, 2004. 9Avandamet [package insert]. Research Triangle Park, NC: GlaxoSmithKline, 2005.
−5 −4 −3 −2 −1 0 1 2 3 4 5
-3.8–0.5
-0.4–1.7
0.9–4.6
0.3–3.0
-0.3–1.9
0.8–2.1

Edema is Common with TZDs (Pioglitazone)
TZDs=thiazolidinediones.1Actos [prescribing information]. Indianapolis, IN: Eli Lilly and Company, 2004.
4.8
7.26.0
15.3
1.22.1 2.5
7.0
0
2
4
6
8
10
12
14
16
18
Monotherapy Combinationwith SU
Combinationwith
metformin
Combinationwith insulin
Prop
ortio
n of
Pati
ents
(%)
Pioglitazone1
Placebo or combination

Use of TZDs is Associated with Increased Incidence of Congestive Heart FailureN
umbe
r of C
HF
Even
ts
P=0.01
CHF=congestive heart failure; TZDs=thiazolidinediones.Adapted from DREAM Trial Investigators, et al. Lancet. 2006; 368: 1096–1105.
HF=heart failureAdapted from Dormandy JA, et al. Lancet. 2005; 366: 1279–1289.
P <0.000114
2
0
5
10
15
20
11
8
0
5
10
15
RosiglitazonePlacebo
Patie
nts
with
HF
(%)
Placebo Pioglitazone ≤45 mg daily
DREAM StudyPROactive Study

Risk of Myocardial Infarction and Death from Cardiovascular Causes with Rosiglitazone
CI=confidence interval; CV=cardiovascular.Adapted from Nissen SE, Wolski K. N Engl J Med. 2007; 356: 2457–2471.
Myocardial infarction
Small trials combined
DREAM
ADOPT
Overall
Death from CV causes
Small trials combined
DREAM
ADOPT
Overall
2.0 4.01.0
Log Odds Ratio (95% CI)
0.5
1.43 (1.03–1.98) P=0.03
1.45; P=0.15
1.65; P=0.22
1.33; P=0.27
2.40; P=0.02
1.20; P=0.67
0.80; P=0.78
1.64 (0.98–2.74) P=0.06

17
Cardiovascular effects of gliptins

Vildagliptin: less hypoglycaemia & Weight gain than sulfonylurea
Hypoglycaemia
0
600
500
400
300
200
100
Ferrannini E, et al. Diabetes Obes Metab 2009; 11: 157–166
Body weight
88
91
90
Weig
ht
(kg
)
89
-8 2 12 22 32 42 52Weeks
39
554
No.
hyp
og
lycaem
ic e
ven
ts
Safety population
Glimepiride + metformin (n=1383)
Vildagliptin + metformin (n=1389)

Beneficial effect on Blood pressure and Lipids
BL=baseline; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol; BL=baseline; DBP=diastolic blood pressure; met=metformin; PBO=placebo; SBP=systolic blood pressure met=metformin; PBO=placebo; TC=total cholesterol; TG=triglycerides; vilda=vildagliptin.Primary intention-to-treat population; n refers to the patient number in the TG test. *P=0.014 vs PBO; all other values did not reach statistical significance. Bosi E, et al. Diabetes Care. 2007; 30; 890–895.

Cardiovascular effects of gliptins Potentially antiatherogenic and might reduce cardiovascular complications
André J. Scheen. Nat. Rev. Cardiol, January 201320

21

22

DPP4 inhibitors & Cardiac safetyAn overall favorable effect of DPP4i on cardiac safety
23
Monami etal, Current Medical Research & Opinion Volume 27, Number S3 2011
Overall ODDS RATIO = 0.689

The FDA position on CV outcome studies
• Sponsors should compare the incidence of important cardiovascular events occurring with the investigational agent to incidence of same types of events occurring with control group to show that upper bound of the 2-sided 95 percent confidence interval for estimated risk ratio is > 1.8.
• This can be accomplished in several ways. • The integrated analysis (meta-analysis) of the phase 2 & phase 3 clinical trials can be used. • If the data from all the studies that are part of meta-analysis will not by itself be able to show that the upper bound
of the two-sided 95 percent confidence interval for the estimated risk ratio is less than 1.8, then an additional single, large safety trial should be conducted that alone, or added to other trials, would be able to satisfy this upper bound before NDA/BLA submission.
24(Source: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm071627.pdf)
If the premarketing application contains clinical data that show that the upper bound of the two-sided 95 percent confidence interval for the estimated increased risk (i.e., risk ratio) is less than 1.3 and the overall risk-benefit analysis supports approval, a postmarketing cardiovascular trial generally may not be necessary

bid=twice daily; CI=confidence interval; CV=cardiovascular; M-H RR=Mantel-Haenszel risk ratio; qd=once daily; vilda=vildagliptin. *Vs all comparators=placebo, metformin, gliclazide, acarbose, rosiglitazone, pioglitazone and glimepiride. All-study safety population.#Guidance for Industry: Diabetes Mellitus - Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes, US Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), December 2008.Schweizer A, et al. Diabetes Obes Metab. 2010; 12: 485–494.
Vildagliptin Reference M-H RR n / N (%) n / N (%) (95% CI)
Vilda 50 mg qd* 10 / 1393 (0.72) 14 / 1555 (0.90) 0.88 (0.37–2.11)
Vilda 50 mg bid* 81 / 6116 (1.32) 80 / 4872 (1.64) 0.84 (0.62–1.14)
Risk ratio
Incidences and odds ratios for adjudicated CV events by treatment
Vildagliptin betterVildagliptin worse0.1 1 10
#Meta-analysis of vildagliptin 50 mg bid data vs all comparators according to the methodology set by the US Food and Drug Administration [50 mg bid odds ratio =
0.84 (95% CI 0.62–1.14)]
Pooled Meta-analysis of 25 Phase III studies of vildagliptin shows no increased cardiovascular risk vs comparators

Cardiac Safety data of gliptins
26
1 = Schweizer A, et al. Diabetes Obes Metab. 2010; 12: 485–494. 2 = http://clinicaltrials.gov/ct2/show/NCT00894868?term=vildagliptin+%2B+heart+failure&rank=1 NCT00894868 Effect of Vildagliptin on Left Ventricular Function in Patients With Type 2 Diabetes and Congestive Heart Failure – Recruiting patients 3 = VERIFY:A Study to Compare Combination Regimen With Vildagliptin & Metformin Versus Metformin in Treatment-naïve Patients With Type 2 Diabetes Mellitus NCT01528254 4 = Scheen A, Expert Opin. Pharmacother. (2012) 13(1):81-99 * Based on routine search on www.clinicaltrial.gov

CONCLUSION
Gliptins are cardiac safe unlike other OHAs -may be cardio protective

Thank You from Cardiology Team BLK
Related Documents