Cutaneous leishmaniasis From Wikipedia, the free encyclopedia Cutaneous leishmaniasis Classification and external resources ICD-10 B55.1ICD-9 085.1-085.4 DiseasesDB3266 29171 MeSH D016773 A 1917 case of Cutaneous Leishmaniasis in the Middle East, known then locally as "Jericho Buttons" for the frequency of cases near the ancient city of Jericho.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 1/20
Cutaneous leishmaniasisFrom Wikipedia, the free encyclopedia
Cutaneous leishmaniasis
Classification and external resources
ICD-10 B55.1
ICD-9 085.1-085.4
DiseasesDB 3266 29171
MeSH D016773
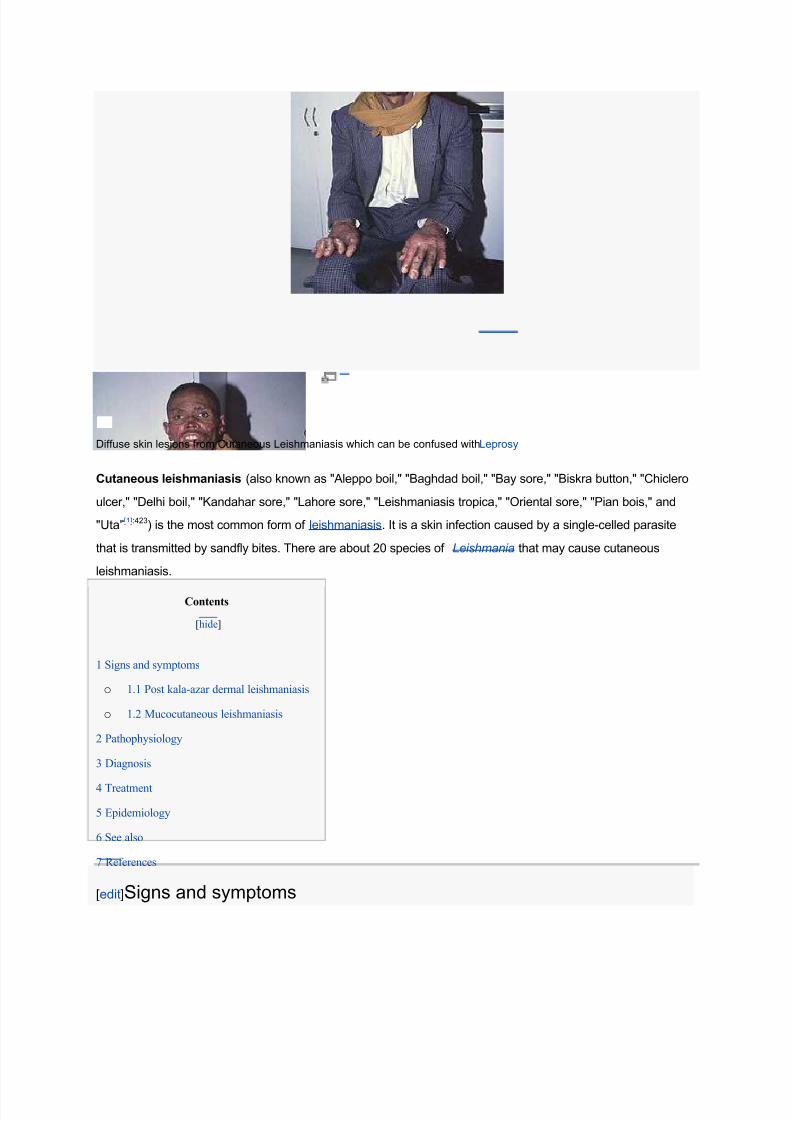
A 1917 case of Cutaneous Leishmaniasis in the Middle East, known then locally as "Jericho Buttons" for the frequency of
cases near the ancient city of Jericho.
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 2/20
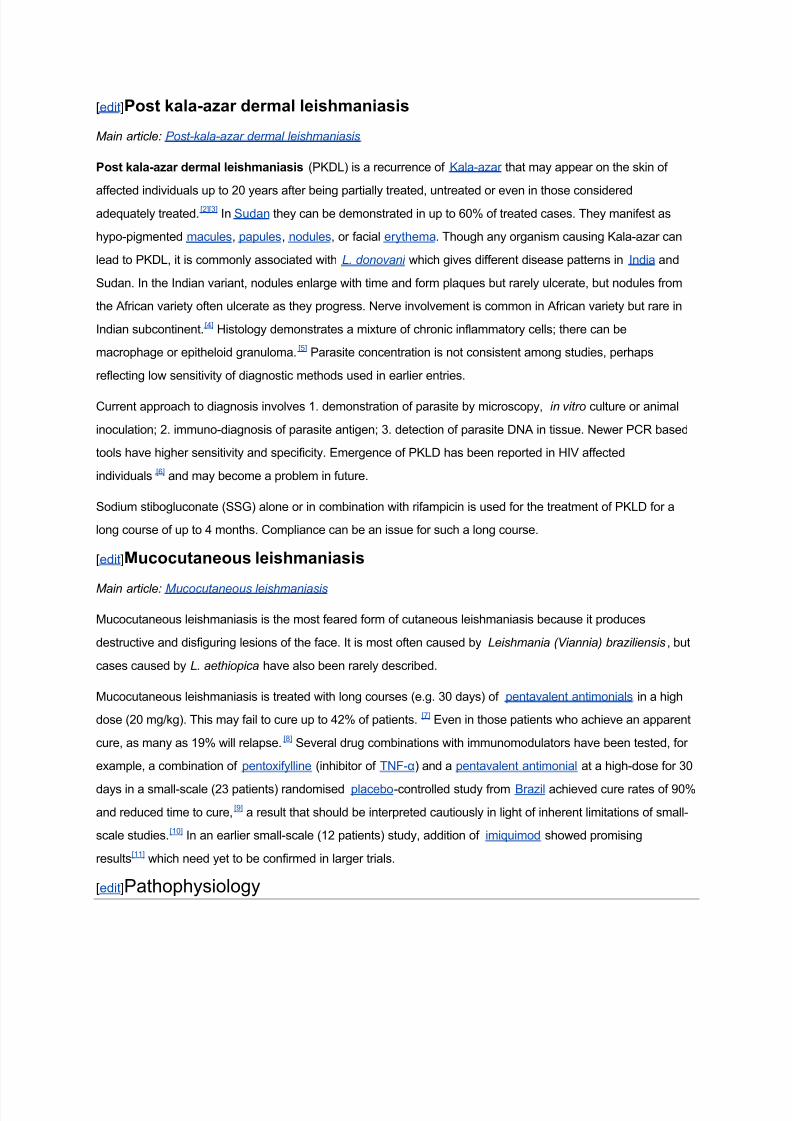
Diffuse skin lesions from Cutaneous Leishmaniasis which can be confused withLeprosy
Cutaneous leishmaniasis (also known as "Aleppo boil," "Baghdad boil," "Bay sore," "Biskra button," "Chiclero
ulcer," "Delhi boil," "Kandahar sore," "Lahore sore," "Leishmaniasis tropica," "Oriental sore," "Pian bois," and
"Uta"[1]:423) is the most common form of leishmaniasis. It is a skin infection caused by a single-celled parasite
that is transmitted by sandfly bites. There are about 20 species of Leishmania that may cause cutaneous
leishmaniasis.
Contents
[hide]
1 Signs and symptoms
o 1.1 Post kala-azar dermal leishmaniasis
o 1.2 Mucocutaneous leishmaniasis
2 Pathophysiology
3 Diagnosis
4 Treatment
5 Epidemiology
6 See also
7 References
[edit]Signs and symptoms
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 3/20
[edit]Post kala-azar dermal leishmaniasis
M ain article: Post-kala-azar dermal leishmaniasis
Post kala-azar dermal leishmaniasis (PKDL) is a recurrence of Kala-azar that may appear on the skin of
affected individuals up to 20 years after being partially treated, untreated or even in those consideredadequately treated.
[2][3]In Sudan they can be demonstrated in up to 60% of treated cases. They manifest as
hypo-pigmented macules, papules, nodules, or facial erythema. Though any organism causing Kala-azar can
lead to PKDL, it is commonly associated with L. donovani which gives different disease patterns in India and
Sudan. In the Indian variant, nodules enlarge with time and form plaques but rarely ulcerate, but nodules from
the African variety often ulcerate as they progress. Nerve involvement is common in African variety but rare in
Indian subcontinent.[4] Histology demonstrates a mixture of chronic inflammatory cells; there can be
macrophage or epitheloid granuloma.[5] Parasite concentration is not consistent among studies, perhaps
reflecting low sensitivity of diagnostic methods used in earlier entries.
Current approach to diagnosis involves 1. demonstration of parasite by microscopy, in vitro culture or animal
inoculation; 2. immuno-diagnosis of parasite antigen; 3. detection of parasite DNA in tissue. Newer PCR based
tools have higher sensitivity and specificity. Emergence of PKLD has been reported in HIV affected
individuals [6] and may become a problem in future.
Sodium stibogluconate (SSG) alone or in combination with rifampicin is used for the treatment of PKLD for a
long course of up to 4 months. Compliance can be an issue for such a long course.
[edit]Mucocutaneous leishmaniasis
M ain article: Mucoc utaneous leishmaniasis
Mucocutaneous leishmaniasis is the most feared form of cutaneous leishmaniasis because it produces
destructive and disfiguring lesions of the face. It is most often caused by Leishmania (Viannia) braziliensis, but
cases caused by L. aethiopica have also been rarely described.
Mucocutaneous leishmaniasis is treated with long courses (e.g. 30 days) of pentavalent antimonials in a high
dose (20 mg/kg). This may fail to cure up to 42% of patients. [7] Even in those patients who achieve an apparent
cure, as many as 19% will relapse.[8] Several drug combinations with immunomodulators have been tested, for
example, a combination of pentoxifylline (inhibitor of TNF-) and a pentavalent antimonial at a high-dose for 30
days in a small-scale (23 patients) randomised placebo-controlled study from Brazil achieved cure rates of 90%
and reduced time to cure,[9]
a result that should be interpreted cautiously in light of inherent limitations of small-
scale studies.[10] In an earlier small-scale (12 patients) study, addition of imiquimod showed promising
results[11] which need yet to be confirmed in larger trials.
[edit]Pathophysiology
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 4/20
Promastigotes of leishmania are transmitted to human skin by the bite of a sandfly. Leishmania then invades
human macrophages and replicates intracellularly.
A raised, red lesion develops at the site of the bite (often weeks or sometimes years afterwards). The lesion
then ulcerates and may become secondarily infected with bacteria. In many species (for example, L. major ) the
lesion often spontaneously heals with atrophic scarring. In some species (for example, L. viannia braziliensis)
the lesion may spontaneously heal with scarring, but then re-appear elsewhere (especially as destructive
mucocutaneous lesions). Lesions of other leishmania species may spontaneously heal and then re-appear as
satellite lesions around the site of the original lesion, or along the route of lymphatic drainage.
Some species tend to cause cutaneous leishmaniasis (e.g., L. major and L.tropica), whereas some species
tend to cause visceral leishmaniasis (e.g., L. infant um and L donovani ), though emerging research (due to high
deployment rates of western countries to indigenous areas) is showing these species specific presentation
lines are blurring[citation needed ].
[edit]Diagnosis
Diagnosis is based on the characteristic appearance of non-healing raised, scaling lesions that may ulcerate
and become secondarily infected with organisms such as Staphylococc us aureus, in someone who has
returned from an endemic area. The gold standard for diagnosis is PCR.[12]
[edit]Treatment
The evidence for optimal treatment of cutaneous leishmaniasis is patchy. Treatments that work for one species
of leishmania may not work for another; it is recommended that advice of a tropical medicine or geographical
medicine specialist be sought. Ideally, every effort should be made to establish the species of leishmania by
molecular techniques (PCR) prior to starting treatment. In the setting of a developing country, there is often
only one species present in a particular locality, so it is usually unnecessary to speciate every infection.
Unfortunately, leishmaniasis is an orphan disease, and almost all the current treatment options are toxic with
significant side-effects.
Leishmania major
L. major infections are usually considered to heal spontanously and do not require treatment, but there
have been several reports of severe cases caused by L. major in Afghanistan. In Saudi Arabia, a six
week course of oral fluconazole 200mg daily has been reported to speed up healing.[13]
Leishmania (Viannia) braziliensis
Treatment with pentavalent antimonials or amphotericin is mandatory, because of the risk of
developing disfiguring mucocutaneous lesions.
Leishmania infantum

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 5/20
L. infant um causes cutaneous leishmaniasis in southern France.[14]
New treatment options are arising from the new oral drug Miltefosine (Impavido) which has
shown in several clinical trials to be very efficient and safe in visceral and cutaneous
leishmaniasis. Recent studies from Bolivia show a high cure rate for mucocutaneous
leishmaniasis. Comparative studies against pentavalent antimonials in Iran and Pakistan are
also beginning to show a high cure rate for L.major and L.tropica. It is registered in many
countries of Latin America (e.g., Colombia), as well in Germany, the home country of its
developer Zentaris GmbH. In October 2006 it received orphan drug status from the US Food
and Drug administration. The drug is generally better tolerated than other drugs. Main side
effects are gastrointestinal disturbances in the 1±2 days of treatment which does not affect the
efficacy.
Secondary bacterial infection (especially with Staphylococc us aureus) is common and may
require antibiotics. Unfortunately, clinicians who are unfamiliar with cutaneous leishmaniasis
may mistake the lesion for a pure bacterial infection (especially after isolation of S.
aureus from bacterial skin swabs) and fail to consider the possibility of leishmaniasis.
[edit]Epidemiology
Cutaneous leishmaniasis is endemic to many parts of the world. Around twenty different
species of Leishmania parasite are capable of infecting humans. The distribution of cutaneous
leishmaniasis is very tightly linked to geography and villages even 15 miles apart can have
very different rates of cutaneous leishmaniasis.
Some Leishmania species are closely linked to humans and are therefore found in cities
(e.g., L. tropica), whereas some are more traditionally associated with animal species and are
therefore considered zoonoses (e.g., L. major ). Some species that are traditionally considered
zoonotic (e.g., L. panamensis) may be becoming primarily human diseases.[15]
Cutaneous leishmaniasis has been occurring in troops coming back from Afghanistan.[16]
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 6/20
Cutaneous Leishmaniasis: Recognition and Treatment
William H. Markle, M.D., and Khaldoun Makhoul, M.D., University of Pittsburgh Medical Center,
McKeesport Hospital, McKeesport, Pennsylvania
Am Fam Physician. 2004 Mar 15;69(6):1455-1460.
Cutaneous leishmaniasis is a parasitic disease occurring throughout the Americas from Texas to
Argentina, and in the Old World, particularly theMiddle East and North Africa. It is spread by the
female sandfly. The condition is diagnosed every year in travelers, immigrants, and military
personnel.Physicians in the United States must be alert to the diagnosis of leishmaniasis in
travelers returning from endemic areas.Physicians working for short periods in endemic areas
often must make the diagnosis and should be aware of local disease patterns. When faced with a
possible leishmanial skin lesion, a skin scraping with microscopic analysis is the best test.Punch
biopsies with tissue-impression smears also can be diagnostic. Needle aspiration of tissue fluid
from the margin of a lesion can yield fluid for culture to isolate the organism and identify the
species. Immunologic tests are being developed, including a highly sensitive polymerase chain
reaction test. The treatment mainstay is pentavalent antimony (e.g., sodium stibogluconate). Notall patients require treatment; many lesions heal spontaneously. Antimonials have a high
incidence of reversible adverse effects. Other medications used for treatment include
amphotericin B, pentamidine isethionate, paromomycin, and antifungals. This disease must be
considered in at-risk patients, and family physicians should know the basics of diagnosis andwhere to go for more help.
Leishmaniasis is endemic in 88 countries throughout Africa, Asia, Europe, and North and South
America.1 There are an estimated 12 million casesworldwide, with 1.5 to 2 million new cases each year.
Although the incidence of leishmaniasis is greater in the Old World than in the New World, the U.S.
traveler is most likely to contract this disease in Latin America. Fifty to 100 cases of New World
cutaneous leishmaniasis are diagnosed each year in the United States. They are contracted mainly in Peru
and Brazil, although the disease is endemic and can be contracted in any country from Mexico toArgentina, except Uruguay and Chile.2 There also is an endemic focus in Texas. Leishmaniasis is a
disease associated with rural areas and poverty, but it has adapted to the urban environment as well.
In World War II, there was a high incidence of leishmaniasis and sandfly fever in troops deployed to the
Persian Gulf region. In the Gulf War (1990 to 1991), approximately 697,000 U.S. troops were deployed
in this region. Only 19 cases of cutaneous leishmaniasis and 12 cases of visceral disease were diagnosed
in this group. The improvement came about because of the use of insecticides and repellents, lower
transmission rates in the summer, and more time spent in urban areas. 3,4 About 150 cases of leishmaniasis
have reportedly been diagnosed in U.S. soldiers serving in Iraq in 2003, and more are
expected.
5
Preliminary data on 22 cases of cutaneous leishmaniasis contracted by American troops inAfghanistan, Kuwait, and Iraq and treated at Walter Reed Army Medical Center between August 2002
and September 2003 were recently released.6 The majority of these persons were infected with Leishmania
major in urban areas of Iraq after a median period of deployment of 60 days.
The Leishmania protozoan was first described in 1903 by Leishman and Donovan, working
separately.2Since then, this organism has been found to be a complex grouping of species, at least 20 of
which cause infections in humans. Some species cause visceral leishmaniasis, some cause cutaneous

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 7/20
disease, and some cause both. Visceral leishmaniasis is a systemic infection characterized by fever,
weight loss, and hepatosplenomegaly, and it is usually fatal without treatment. This article focuses on
cutaneous leishmaniasis, the more common form of the disease.
Life Cycle and Vector
The promastigote form of the parasite is a motile form with an anterior flagellum that develops in the
sandfly, the insect vector. The promastigote form develops into a metacyclic infectious form over
approximately 10 days. The parasite enters the human host with the bite of the sandfly and is pulled into
macrophages by ingestion. Leishmania are able to survive the acidic environment of the lysosome and
become amastigote forms. These forms are obligate, intracellular, non-motile, and about 2.5 to 7 microns
in diameter. It is this amastigote form that causes disease in humans and affects cellular immunity.
Eventually, a sandfly will pick up this form while feeding, and it will develop into the promastigote form
again in the insect.
The sandfly vector is a 2-mm long, hairy fly of the genus Phlebotomus in the Old World and Lutzomyia
in the New World. These flies are able to pass through the usual netting used for mosquitoes. Sandflies
are found around human habitations and breed in specific organic wastes such as feces, manure, rodent
burrows, and leaf litter.7
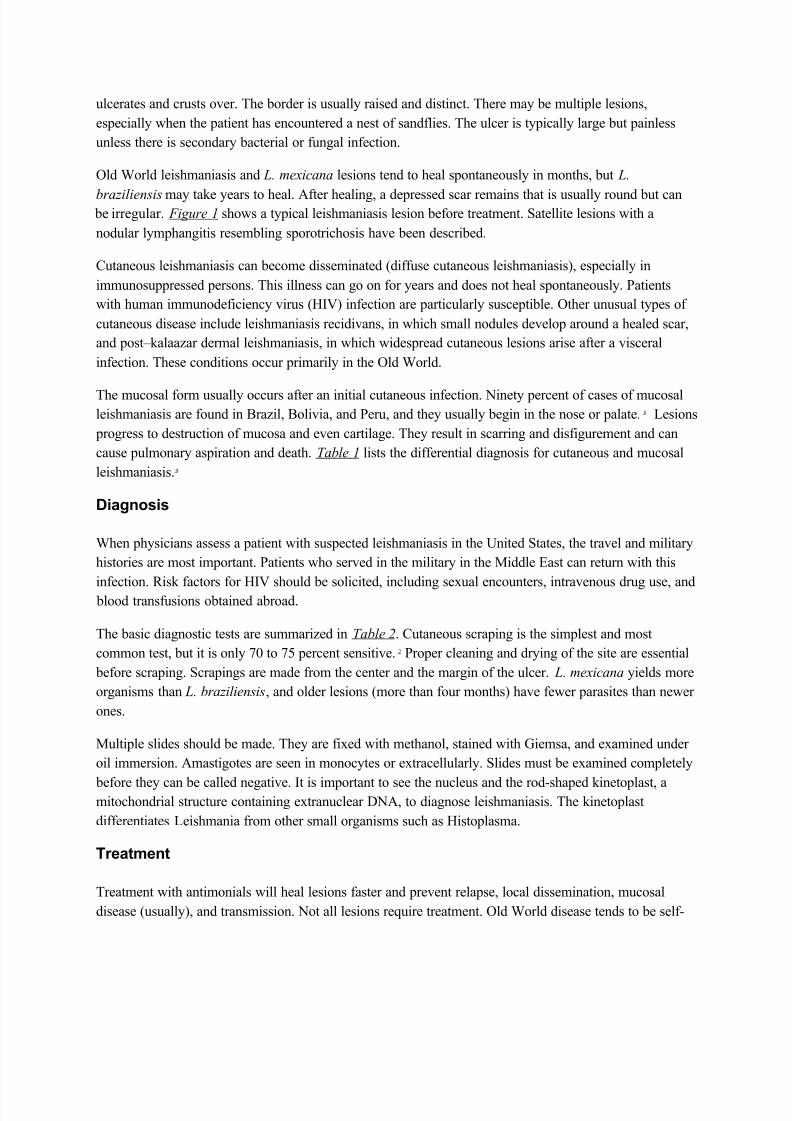
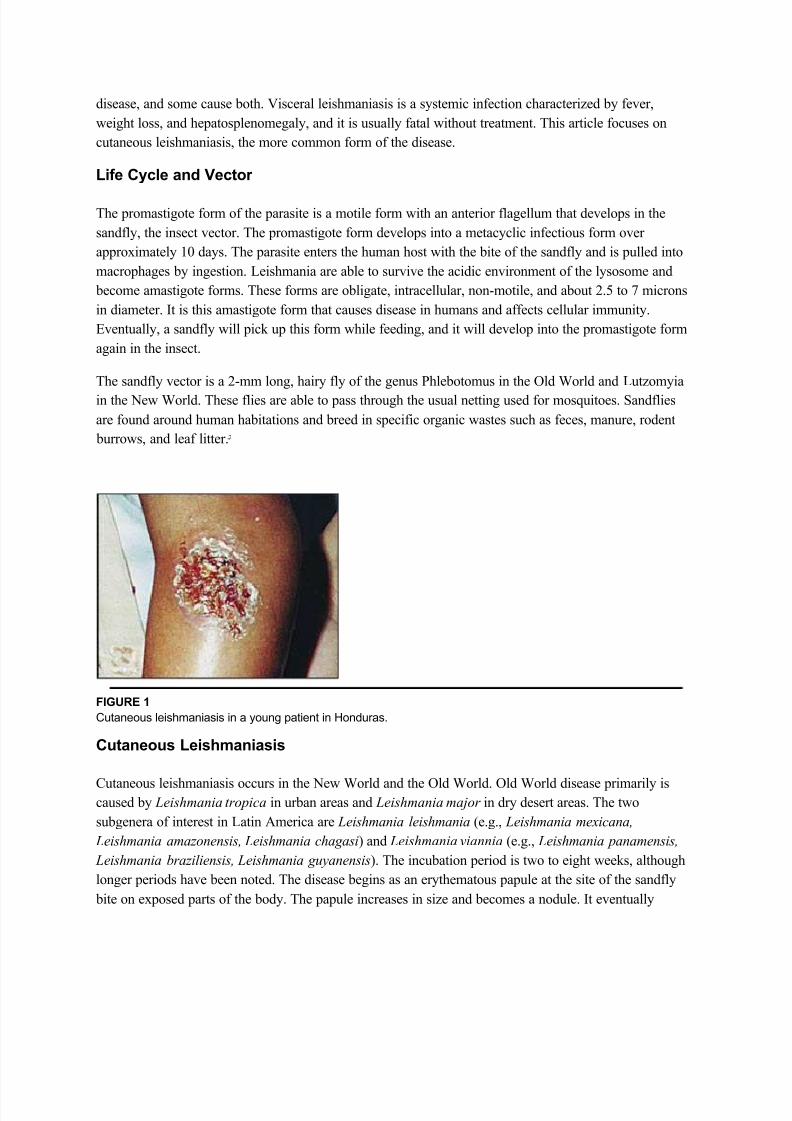
FIGURE 1
Cutaneous leishmaniasis in a young patient in Honduras.
Cutaneous Leishmaniasis
Cutaneous leishmaniasis occurs in the New World and the Old World. Old World disease primarily iscaused by Leishmania tropica in urban areas and Leishmania major in dry desert areas. The two
subgenera of interest in Latin America are Leishmania leishmania (e.g., Leishmania mexicana,
Leishmania amazonensis, Leishmania chagasi) and Leishmania viannia (e.g., Leishmania panamensis,
Leishmania braziliensis, Leishmania guyanensis). The incubation period is two to eight weeks, although
longer periods have been noted. The disease begins as an erythematous papule at the site of the sandfly
bite on exposed parts of the body. The papule increases in size and becomes a nodule. It eventually
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 8/20
ulcerates and crusts over. The border is usually raised and distinct. There may be multiple lesions,
especially when the patient has encountered a nest of sandflies. The ulcer is typically large but painless
unless there is secondary bacterial or fungal infection.
Old World leishmaniasis and L. mexicana lesions tend to heal spontaneously in months, but L.
braziliensis may take years to heal. After healing, a depressed scar remains that is usually round but can be irregular. Figure 1 shows a typical leishmaniasis lesion before treatment. Satellite lesions with a
nodular lymphangitis resembling sporotrichosis have been described.
Cutaneous leishmaniasis can become disseminated (diffuse cutaneous leishmaniasis), especially in
immunosuppressed persons. This illness can go on for years and does not heal spontaneously. Patients
with human immunodeficiency virus (HIV) infection are particularly susceptible. Other unusual types of
cutaneous disease include leishmaniasis recidivans, in which small nodules develop around a healed scar,
and post±kalaazar dermal leishmaniasis, in which widespread cutaneous lesions arise after a visceral
infection. These conditions occur primarily in the Old World.
The mucosal form usually occurs after an initial cutaneous infection. Ninety percent of cases of mucosalleishmaniasis are found in Brazil, Bolivia, and Peru, and they usually begin in the nose or palate. 8 Lesions
progress to destruction of mucosa and even cartilage. They result in scarring and disfigurement and can
cause pulmonary aspiration and death. Table 1 lists the differential diagnosis for cutaneous and mucosal
leishmaniasis.9
Diagnosis
When physicians assess a patient with suspected leishmaniasis in the United States, the travel and military
histories are most important. Patients who served in the military in the Middle East can return with this
infection. Risk factors for HIV should be solicited, including sexual encounters, intravenous drug use, and
blood transfusions obtained abroad.
The basic diagnostic tests are summarized in Table 2. Cutaneous scraping is the simplest and most
common test, but it is only 70 to 75 percent sensitive. 2 Proper cleaning and drying of the site are essential
before scraping. Scrapings are made from the center and the margin of the ulcer. L. mexicana yields more
organisms than L. braziliensis, and older lesions (more than four months) have fewer parasites than newer
ones.
Multiple slides should be made. They are fixed with methanol, stained with Giemsa, and examined under
oil immersion. Amastigotes are seen in monocytes or extracellularly. Slides must be examined completely
before they can be called negative. It is important to see the nucleus and the rod-shaped kinetoplast, amitochondrial structure containing extranuclear DNA, to diagnose leishmaniasis. The kinetoplast
differentiates Leishmania from other small organisms such as Histoplasma.
Treatment
Treatment with antimonials will heal lesions faster and prevent relapse, local dissemination, mucosal
disease (usually), and transmission. Not all lesions require treatment. Old World disease tends to be self-
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 9/20
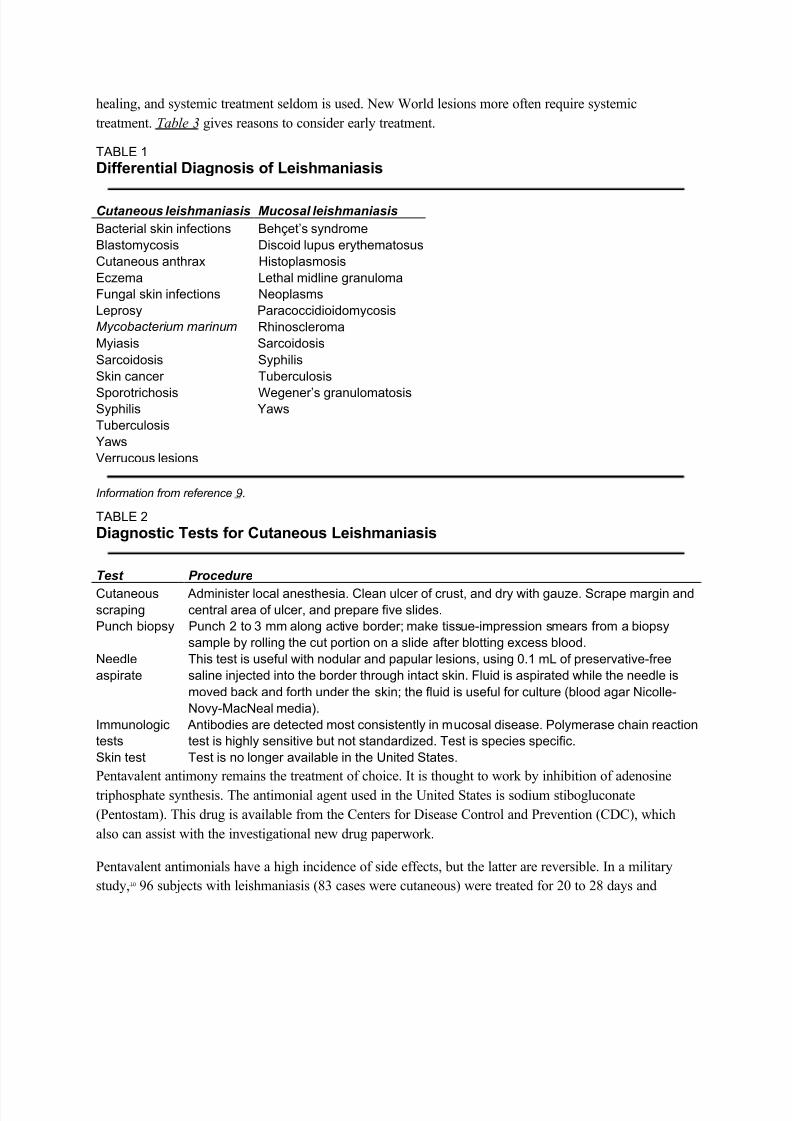
healing, and systemic treatment seldom is used. New World lesions more often require systemic
treatment. Table 3 gives reasons to consider early treatment.
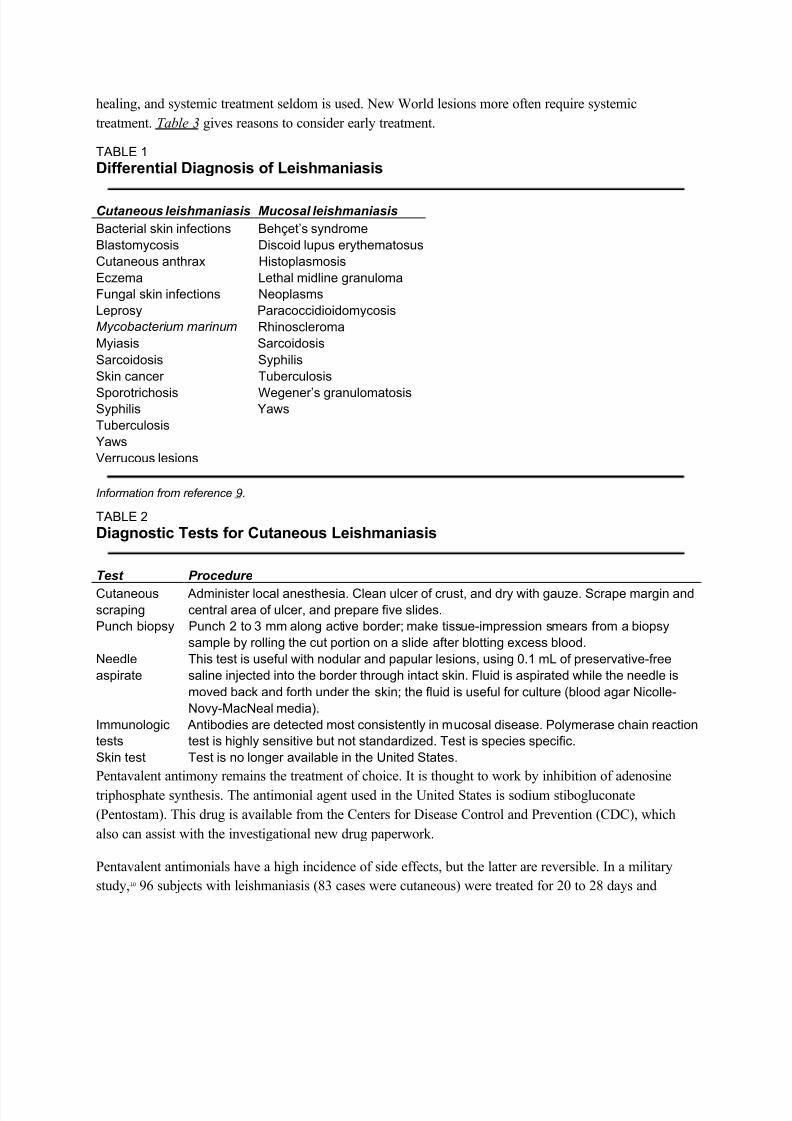
TABLE 1
DifferentialDiagnosis of Leishmaniasis
C utaneous leishmaniasis Mucosal leishmaniasis
Bacterial skin infections Behçet¶s syndrome
Blastomycosis Discoid lupus erythematosus
Cutaneous anthrax Histoplasmosis
Eczema Lethal midline granuloma
Fungal skin infections Neoplasms
Leprosy Paracoccidioidomycosis
M ycobacteri um marinum Rhinoscleroma
Myiasis Sarcoidosis
Sarcoidosis Syphilis
Skin cancer Tuberculosis
Sporotrichosis Wegener¶s granulomatosisSyphilis Yaws
Tuberculosis
Yaws
Verrucous lesions
I nformation from reference 9.
TABLE 2
Diagnostic Tests for Cutaneous Leishmaniasis
T est Procedure
Cutaneous
scraping
Administer local anesthesia. Clean ulcer of crust, and dry with gauze. Scrape margin and
central area of ulcer, and prepare five slides.
Punch biopsy Punch 2 to 3 mm along active border; make tissue-impression smears from a biopsy
sample by rolling the cut portion on a slide after blotting excess blood.
Needle
aspirate
This test is useful with nodular and papular lesions, using 0.1 mL of preservative-free
saline injected into the border through intact skin. Fluid is aspirated while the needle is
moved back and forth under the skin; the fluid is useful for culture (blood agar Nicolle-
Novy-MacNeal media).
Immunologic
tests
Antibodies are detected most consistently in mucosal disease. Polymerase chain reaction
test is highly sensitive but not standardized. Test is species specific.
Skin test Test is no longer available in the United States.
Pentavalent antimony remains the treatment of choice. It is thought to work by inhibition of adenosine
triphosphate synthesis. The antimonial agent used in the United States is sodium stibogluconate
(Pentostam). This drug is available from the Centers for Disease Control and Prevention (CDC), which
also can assist with the investigational new drug paperwork.
Pentavalent antimonials have a high incidence of side effects, but the latter are reversible. In a military
study,10 96 subjects with leishmaniasis (83 cases were cutaneous) were treated for 20 to 28 days and
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 10/20
followed for one year. Side effects included aching, arthralgia, fatigue, gastrointestinal upset, elevation of
amylase, lipase, and liver enzyme levels, leukopenia, anemia, and electrocardiographic abnormalities.
In general, more adverse reactions are expected in patients with liver and renal impairment, cardiac
arrhythmias, and prolonged QT intervals; in small children; in pregnant and breastfeeding women; and in
obese, elderly, and immunocompromised patients. There are no known drug interactions, but hepatotoxicdrugs, including alcohol, and drugs that prolong the QT interval should be avoided. 10 Because pentavalent
antimony is difficult to use, consultation with an infectious disease specialist and the CDC is
recommended before using it.
After 20 days of treatment with pentavalent antimonials, there is usually evidence of healing, but lesions
may not be re-epithelialized completely. They generally go on to heal. Healing is determined by a healed
appearance at two months, no relapse at 12 months, and no subsequent mucosal disease. Mucosal disease
requires a longer treatment course and is more difficult to cure.
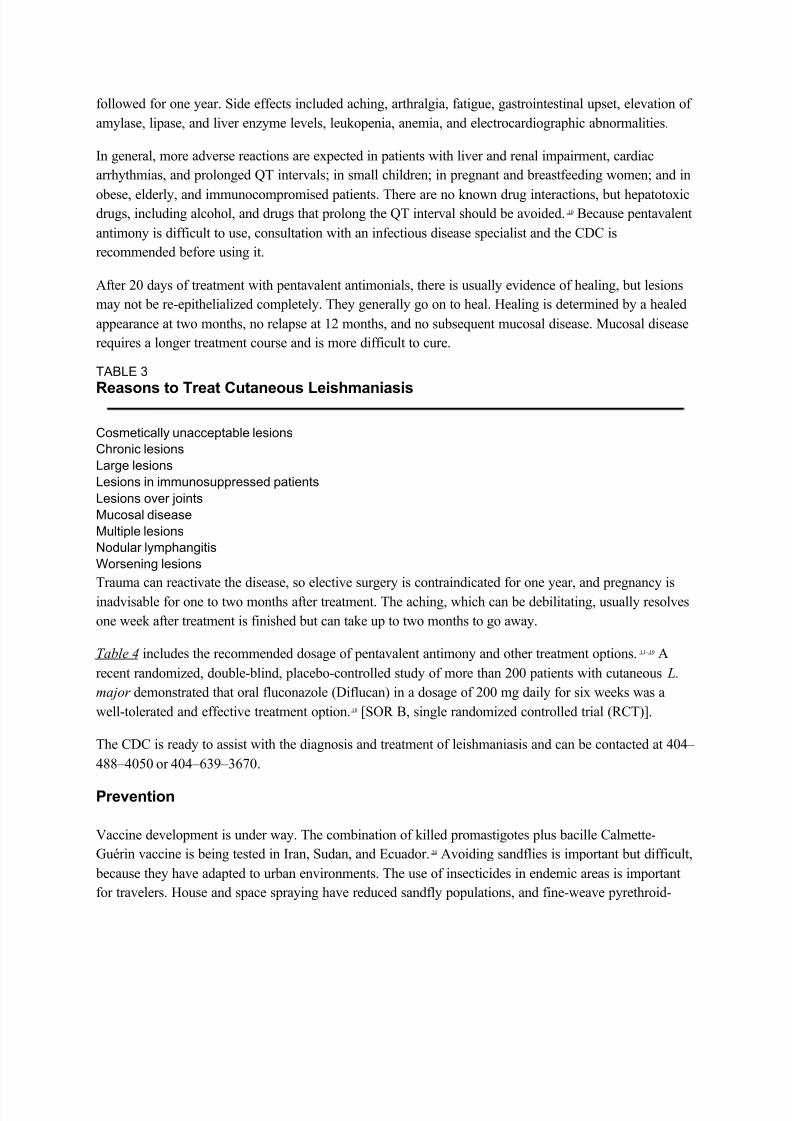
TABLE 3
Reasons to Treat Cutaneous Leishmaniasis
Cosmetically unacceptable lesions
Chronic lesions
Large lesions
Lesions in immunosuppressed patients
Lesions over joints
Mucosal disease
Multiple lesions
Nodular lymphangitis
Worsening lesions
Trauma can reactivate the disease, so elective surgery is contraindicated for one year, and pregnancy isinadvisable for one to two months after treatment. The aching, which can be debilitating, usually resolves
one week after treatment is finished but can take up to two months to go away.
Table 4 includes the recommended dosage of pentavalent antimony and other treatment options. 11 ± 19 A
recent randomized, double-blind, placebo-controlled study of more than 200 patients with cutaneous L.
major demonstrated that oral fluconazole (Diflucan) in a dosage of 200 mg daily for six weeks was a
well-tolerated and effective treatment option.18 [SOR B, single randomized controlled trial (RCT)].
The CDC is ready to assist with the diagnosis and treatment of leishmaniasis and can be contacted at 404±
488±4050 or 404±639±3670.
Prevention
Vaccine development is under way. The combination of killed promastigotes plus bacille Calmette-
Guérin vaccine is being tested in Iran, Sudan, and Ecuador.20 Avoiding sandflies is important but difficult,
because they have adapted to urban environments. The use of insecticides in endemic areas is important
for travelers. House and space spraying have reduced sandfly populations, and fine-weave pyrethroid-

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 11/20
impregnated bed-nets have been used in Burkina Faso, Sudan, and Columbia. Destruction of rodent
reservoirs by pumping insecticides into rodent burrows has had limited success.7
A recent randomized study in Venezuela evaluated the effectiveness of pyrethroid-impregnated curtains
in an urban area with an incidence of cutaneous leishmaniasis of 4 percent. In 569 homes, 2,913
inhabitants were included in this study. Use of the curtains reduced the sandfly population and, 12 monthsafter the installation of these curtains, the incidence of cutaneous leishmaniasis dropped to zero. 21 [SOR B,
single RCT]
TABLE 4
Treatment of Cutaneous Leishmaniasis
Pentavalent antimony
Meglumine antimoniate (Glucantime) and sodium stibogluconate (Pentostam); cure rate 94 percent;
eliminated by kidneys
Dosage: 20 mg per kg per day for 20 days
Stibogluconate supplied as 100 mg Sb per mL light-sensitive solutionCalculated dose (12 to 20 mL for adults) is diluted in 50 mL of 5 percent dextrose in distilled water,
infused intravenously over 10 to 15 minutes
Amphotericin B (Fungizone)
Reserved for antimony failures
Dosage: 0.5 to 1.0 mg per kg every other day for up to eight weeks; total dosage is 1.5 to 2 g for the
treatment period
Pentamidine isethionate (Pentam 300)
Dosage: 2 mg per kg intramuscularly every other day for seven days
Toxic effects: damage to pancreas, kidney, or bone marrow may be irreversible
May induce diabetes mellitus
Others
Topical paromomycin is effective with L. major and L. mexicana. It can be combined with antimonials toreduce the number of injections.
Oral antifungals have demonstrated conflicting results, although some good results have been achieved
with L. mexicana19 and L. major .18
Allopurinol (Zyloprim) incorporates into parasite RNA with lethal effect. Studies are conflicting, and it is not
recommended, although there is synergistic activity with antimonials.11 ±14
Heat15 ±16 and cryotherapy17 show good results in uncontrolled trials.
Excision is not recommended because of the high risk of local relapse and disfiguration.
I nformation from references 11 throug h 19.

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 12/20
Cutaneous Leishmaniasis: Recognition and Treatment
William H. Markle, M.D., and Khaldoun Makhoul, M.D., University of Pittsburgh Medical Center,
McKeesport Hospital, McKeesport, Pennsylvania
Am Fam Physician. 2004 Mar 15;69(6):1455-1460.
Cutaneous leishmaniasis is a parasitic disease occurring throughout the Americas from Texas to
Argentina, and in the Old World, particularly theMiddle East and North Africa. It is spread by the
female sandfly. The condition is diagnosed every year in travelers, immigrants, and military
personnel.Physicians in the United States must be alert to the diagnosis of leishmaniasis in
travelers returning from endemic areas.Physicians working for short periods in endemic areas
often must make the diagnosis and should be aware of local disease patterns. When faced with a
possible leishmanial skin lesion, a skin scraping with microscopic analysis is the best test.Punch
biopsies with tissue-impression smears also can be diagnostic. Needle aspiration of tissue fluid
from the margin of a lesion can yield fluid for culture to isolate the organism and identify the
species. Immunologic tests are being developed, including a highly sensitive polymerase chain
reaction test. The treatment mainstay is pentavalent antimony (e.g., sodium stibogluconate). Notall patients require treatment; many lesions heal spontaneously. Antimonials have a high
incidence of reversible adverse effects. Other medications used for treatment include
amphotericin B, pentamidine isethionate, paromomycin, and antifungals. This disease must be
considered in at-risk patients, and family physicians should know the basics of diagnosis andwhere to go for more help.
Leishmaniasis is endemic in 88 countries throughout Africa, Asia, Europe, and North and South
America.1 There are an estimated 12 million casesworldwide, with 1.5 to 2 million new cases each year.
Although the incidence of leishmaniasis is greater in the Old World than in the New World, the U.S.
traveler is most likely to contract this disease in Latin America. Fifty to 100 cases of New World
cutaneous leishmaniasis are diagnosed each year in the United States. They are contracted mainly in Peru
and Brazil, although the disease is endemic and can be contracted in any country from Mexico toArgentina, except Uruguay and Chile.2 There also is an endemic focus in Texas. Leishmaniasis is a
disease associated with rural areas and poverty, but it has adapted to the urban environment as well.
In World War II, there was a high incidence of leishmaniasis and sandfly fever in troops deployed to the
Persian Gulf region. In the Gulf War (1990 to 1991), approximately 697,000 U.S. troops were deployed
in this region. Only 19 cases of cutaneous leishmaniasis and 12 cases of visceral disease were diagnosed
in this group. The improvement came about because of the use of insecticides and repellents, lower
transmission rates in the summer, and more time spent in urban areas. 3,4 About 150 cases of leishmaniasis
have reportedly been diagnosed in U.S. soldiers serving in Iraq in 2003, and more are
expected.
5
Preliminary data on 22 cases of cutaneous leishmaniasis contracted by American troops inAfghanistan, Kuwait, and Iraq and treated at Walter Reed Army Medical Center between August 2002
and September 2003 were recently released.6 The majority of these persons were infected with Leishmania
major in urban areas of Iraq after a median period of deployment of 60 days.
The Leishmania protozoan was first described in 1903 by Leishman and Donovan, working
separately.2Since then, this organism has been found to be a complex grouping of species, at least 20 of
which cause infections in humans. Some species cause visceral leishmaniasis, some cause cutaneous
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 13/20
disease, and some cause both. Visceral leishmaniasis is a systemic infection characterized by fever,
weight loss, and hepatosplenomegaly, and it is usually fatal without treatment. This article focuses on
cutaneous leishmaniasis, the more common form of the disease.
Life Cycle and Vector
The promastigote form of the parasite is a motile form with an anterior flagellum that develops in the
sandfly, the insect vector. The promastigote form develops into a metacyclic infectious form over
approximately 10 days. The parasite enters the human host with the bite of the sandfly and is pulled into
macrophages by ingestion. Leishmania are able to survive the acidic environment of the lysosome and
become amastigote forms. These forms are obligate, intracellular, non-motile, and about 2.5 to 7 microns
in diameter. It is this amastigote form that causes disease in humans and affects cellular immunity.
Eventually, a sandfly will pick up this form while feeding, and it will develop into the promastigote form
again in the insect.
The sandfly vector is a 2-mm long, hairy fly of the genus Phlebotomus in the Old World and Lutzomyia
in the New World. These flies are able to pass through the usual netting used for mosquitoes. Sandflies
are found around human habitations and breed in specific organic wastes such as feces, manure, rodent
burrows, and leaf litter.7
FIGURE 1
Cutaneous leishmaniasis in a young patient in Honduras.
Cutaneous Leishmaniasis
Cutaneous leishmaniasis occurs in the New World and the Old World. Old World disease primarily iscaused by Leishmania tropica in urban areas and Leishmania major in dry desert areas. The two
subgenera of interest in Latin America are Leishmania leishmania (e.g., Leishmania mexicana,
Leishmania amazonensis, Leishmania chagasi) and Leishmania viannia (e.g., Leishmania panamensis,
Leishmania braziliensis, Leishmania guyanensis). The incubation period is two to eight weeks, although
longer periods have been noted. The disease begins as an erythematous papule at the site of the sandfly
bite on exposed parts of the body. The papule increases in size and becomes a nodule. It eventually

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 14/20
ulcerates and crusts over. The border is usually raised and distinct. There may be multiple lesions,
especially when the patient has encountered a nest of sandflies. The ulcer is typically large but painless
unless there is secondary bacterial or fungal infection.
Old World leishmaniasis and L. mexicana lesions tend to heal spontaneously in months, but L.
braziliensis may take years to heal. After healing, a depressed scar remains that is usually round but can be irregular. Figure 1 shows a typical leishmaniasis lesion before treatment. Satellite lesions with a
nodular lymphangitis resembling sporotrichosis have been described.
Cutaneous leishmaniasis can become disseminated (diffuse cutaneous leishmaniasis), especially in
immunosuppressed persons. This illness can go on for years and does not heal spontaneously. Patients
with human immunodeficiency virus (HIV) infection are particularly susceptible. Other unusual types of
cutaneous disease include leishmaniasis recidivans, in which small nodules develop around a healed scar,
and post±kalaazar dermal leishmaniasis, in which widespread cutaneous lesions arise after a visceral
infection. These conditions occur primarily in the Old World.
The mucosal form usually occurs after an initial cutaneous infection. Ninety percent of cases of mucosalleishmaniasis are found in Brazil, Bolivia, and Peru, and they usually begin in the nose or palate. 8 Lesions
progress to destruction of mucosa and even cartilage. They result in scarring and disfigurement and can
cause pulmonary aspiration and death. Table 1 lists the differential diagnosis for cutaneous and mucosal
leishmaniasis.9
Diagnosis
When physicians assess a patient with suspected leishmaniasis in the United States, the travel and military
histories are most important. Patients who served in the military in the Middle East can return with this
infection. Risk factors for HIV should be solicited, including sexual encounters, intravenous drug use, and
blood transfusions obtained abroad.
The basic diagnostic tests are summarized in Table 2. Cutaneous scraping is the simplest and most
common test, but it is only 70 to 75 percent sensitive. 2 Proper cleaning and drying of the site are essential
before scraping. Scrapings are made from the center and the margin of the ulcer. L. mexicana yields more
organisms than L. braziliensis, and older lesions (more than four months) have fewer parasites than newer
ones.
Multiple slides should be made. They are fixed with methanol, stained with Giemsa, and examined under
oil immersion. Amastigotes are seen in monocytes or extracellularly. Slides must be examined completely
before they can be called negative. It is important to see the nucleus and the rod-shaped kinetoplast, amitochondrial structure containing extranuclear DNA, to diagnose leishmaniasis. The kinetoplast
differentiates Leishmania from other small organisms such as Histoplasma.
Treatment
Treatment with antimonials will heal lesions faster and prevent relapse, local dissemination, mucosal
disease (usually), and transmission. Not all lesions require treatment. Old World disease tends to be self-
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 15/20
healing, and systemic treatment seldom is used. New World lesions more often require systemic
treatment. Table 3 gives reasons to consider early treatment.
TABLE 1
DifferentialDiagnosis of Leishmaniasis
C utaneous leishmaniasis Mucosal leishmaniasis
Bacterial skin infections Behçet¶s syndrome
Blastomycosis Discoid lupus erythematosus
Cutaneous anthrax Histoplasmosis
Eczema Lethal midline granuloma
Fungal skin infections Neoplasms
Leprosy Paracoccidioidomycosis
M ycobacteri um marinum Rhinoscleroma
Myiasis Sarcoidosis
Sarcoidosis Syphilis
Skin cancer Tuberculosis
Sporotrichosis Wegener¶s granulomatosisSyphilis Yaws
Tuberculosis
Yaws
Verrucous lesions
I nformation from reference 9.
TABLE 2
Diagnostic Tests for Cutaneous Leishmaniasis
T est Procedure
Cutaneous
scraping
Administer local anesthesia. Clean ulcer of crust, and dry with gauze. Scrape margin and
central area of ulcer, and prepare five slides.
Punch biopsy Punch 2 to 3 mm along active border; make tissue-impression smears from a biopsy
sample by rolling the cut portion on a slide after blotting excess blood.
Needle
aspirate
This test is useful with nodular and papular lesions, using 0.1 mL of preservative-free
saline injected into the border through intact skin. Fluid is aspirated while the needle is
moved back and forth under the skin; the fluid is useful for culture (blood agar Nicolle-
Novy-MacNeal media).
Immunologic
tests
Antibodies are detected most consistently in mucosal disease. Polymerase chain reaction
test is highly sensitive but not standardized. Test is species specific.
Skin test Test is no longer available in the United States.
Pentavalent antimony remains the treatment of choice. It is thought to work by inhibition of adenosine
triphosphate synthesis. The antimonial agent used in the United States is sodium stibogluconate
(Pentostam). This drug is available from the Centers for Disease Control and Prevention (CDC), which
also can assist with the investigational new drug paperwork.
Pentavalent antimonials have a high incidence of side effects, but the latter are reversible. In a military
study,10 96 subjects with leishmaniasis (83 cases were cutaneous) were treated for 20 to 28 days and

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 16/20
followed for one year. Side effects included aching, arthralgia, fatigue, gastrointestinal upset, elevation of
amylase, lipase, and liver enzyme levels, leukopenia, anemia, and electrocardiographic abnormalities.
In general, more adverse reactions are expected in patients with liver and renal impairment, cardiac
arrhythmias, and prolonged QT intervals; in small children; in pregnant and breastfeeding women; and in
obese, elderly, and immunocompromised patients. There are no known drug interactions, but hepatotoxicdrugs, including alcohol, and drugs that prolong the QT interval should be avoided. 10 Because pentavalent
antimony is difficult to use, consultation with an infectious disease specialist and the CDC is
recommended before using it.
After 20 days of treatment with pentavalent antimonials, there is usually evidence of healing, but lesions
may not be re-epithelialized completely. They generally go on to heal. Healing is determined by a healed
appearance at two months, no relapse at 12 months, and no subsequent mucosal disease. Mucosal disease
requires a longer treatment course and is more difficult to cure.
TABLE 3
Reasons to Treat Cutaneous Leishmaniasis
Cosmetically unacceptable lesions
Chronic lesions
Large lesions
Lesions in immunosuppressed patients
Lesions over joints
Mucosal disease
Multiple lesions
Nodular lymphangitis
Worsening lesions
Trauma can reactivate the disease, so elective surgery is contraindicated for one year, and pregnancy isinadvisable for one to two months after treatment. The aching, which can be debilitating, usually resolves
one week after treatment is finished but can take up to two months to go away.
Table 4 includes the recommended dosage of pentavalent antimony and other treatment options. 11 ± 19 A
recent randomized, double-blind, placebo-controlled study of more than 200 patients with cutaneous L.
major demonstrated that oral fluconazole (Diflucan) in a dosage of 200 mg daily for six weeks was a
well-tolerated and effective treatment option.18 [SOR B, single randomized controlled trial (RCT)].
The CDC is ready to assist with the diagnosis and treatment of leishmaniasis and can be contacted at 404±
488±4050 or 404±639±3670.
Prevention
Vaccine development is under way. The combination of killed promastigotes plus bacille Calmette-
Guérin vaccine is being tested in Iran, Sudan, and Ecuador.20 Avoiding sandflies is important but difficult,
because they have adapted to urban environments. The use of insecticides in endemic areas is important
for travelers. House and space spraying have reduced sandfly populations, and fine-weave pyrethroid-

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 17/20
impregnated bed-nets have been used in Burkina Faso, Sudan, and Columbia. Destruction of rodent
reservoirs by pumping insecticides into rodent burrows has had limited success.7
A recent randomized study in Venezuela evaluated the effectiveness of pyrethroid-impregnated curtains
in an urban area with an incidence of cutaneous leishmaniasis of 4 percent. In 569 homes, 2,913
inhabitants were included in this study. Use of the curtains reduced the sandfly population and, 12 monthsafter the installation of these curtains, the incidence of cutaneous leishmaniasis dropped to zero. 21 [SOR B,
single RCT]
TABLE 4
Treatment of Cutaneous Leishmaniasis
Pentavalent antimony
Meglumine antimoniate (Glucantime) and sodium stibogluconate (Pentostam); cure rate 94 percent;
eliminated by kidneys
Dosage: 20 mg per kg per day for 20 days
Stibogluconate supplied as 100 mg Sb per mL light-sensitive solutionCalculated dose (12 to 20 mL for adults) is diluted in 50 mL of 5 percent dextrose in distilled water,
infused intravenously over 10 to 15 minutes
Amphotericin B (Fungizone)
Reserved for antimony failures
Dosage: 0.5 to 1.0 mg per kg every other day for up to eight weeks; total dosage is 1.5 to 2 g for the
treatment period
Pentamidine isethionate (Pentam 300)
Dosage: 2 mg per kg intramuscularly every other day for seven days
Toxic effects: damage to pancreas, kidney, or bone marrow may be irreversible
May induce diabetes mellitus
Others
Topical paromomycin is effective with L. major and L. mexicana. It can be combined with antimonials toreduce the number of injections.
Oral antifungals have demonstrated conflicting results, although some good results have been achieved
with L. mexicana19 and L. major .18
Allopurinol (Zyloprim) incorporates into parasite RNA with lethal effect. Studies are conflicting, and it is not
recommended, although there is synergistic activity with antimonials.11 ±14
Heat15 ±16 and cryotherapy17 show good results in uncontrolled trials.
Excision is not recommended because of the high risk of local relapse and disfiguration.
I nformation from references 11 throug h 19.

8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 18/20
Leishmaniasis
Leishmaniasis is a parasitic disease spread by the bite of the sandfly.
Causes
There are different forms of leishmaniasis.
y Cutaneous leishmaniasis affects the skin and mucus membranes. Skin sores usually start at the
site of the sandfly bite. They can last for months or years before healing on their own. In a few
people, sores may develop on mucus membranes.
y Systemic, or visceral leishmaniasis affects the entire body. This form occurs 2 - 8 months after a
person is bitten by the sandfly. Most people do not remember having a skin sore. This form can
lead to deadly complications. The parasites damage the immune system by decreasing the
numbers of disease-fighting cells.
Cases of leishmaniasis have been reported on all continents except Australia and Antarctica. In the
Americas, leishmaniasis can be found in Mexico and South America. Leishmaniasis has been reported in
military personnel returning from the Persian Gulf.
Symptoms
Cutaneous leishmaniasis affects the skin and sometimes the mucus membranes. Symptoms may include:
y Skin sores, which may become a skin ulcer that heals very slowly
y Ulcers and wearing away (erosion) in the mouth, tongue, gums, lips, nose, and inner nose
y Stuffy nose, runny nose, and nosebleedsy Breathing difficulty
y Swallowing difficulty
Systemic visceral infection in children usually begins suddenly with vomiting, diarrhea, fever, and cough.
Adults usually have a fever for 2 weeks to 2 months, along with symptoms such as fatigue, weakness,
and appetite loss. Weakness increases as the disease gets worse.
Other symptoms of systemic visceral leishmaniasis may include:
y Belly area (abdominal) discomfort
y Cough (children)
y Diarrhea (children)
y Fever that lasts for weeks; may come and go in cycles
y Night sweats
y Scaly, gray, dark, ashen skin
y Thinning hair
y Vomiting (children)
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 19/20
y Weight loss
Exams and Tests
A physical exam may show signs of an enlarged spleen, liver, and lymph nodes. The patient may have
been bitten by sandflies, or was in an area known for leishmaniasis.
Tests that may be done to diagnose the condition include:
y Biopsy of the spleen and culture
y Bone marrow biopsy and culture
y Direct agglutination assay
y Indirect immunofluorescent antibody test
y Lymph node biopsy and culture
y Montenegro skin test
y Skin biopsy
Other tests that may be done include:
y Complete blood count
y Serum immunoglobulin levels
y Serum protein
y Serum albumin
y Serologic testing
Treatment
Medicines called antimony-containing compounds are the main drugs used to treat leishmaniasis. Theseinclude:
y Meglumine antimonate
y Sodium stibogluconate
Other drugs that may be used include:
y Amphotericin B
y Fluconazole
y Pentamidine
Plastic surgery may be needed to correct the disfigurement caused by sores on the face (cutaneous
leishmaniasis). Patients with drug-resistant viral leishmaniasis may need to have their spleen removed
(splenectomy).
Outlook (Prognosis)
8/8/2019 Cutaneous Lei Sh Manias Is
http://slidepdf.com/reader/full/cutaneous-lei-sh-manias-is 20/20
Cure rates are high with the proper medicine. Patients should get treated before damage to the immune
system occurs. Cutaneous leishmaniasis may lead to disfigurement.
Death is usually caused by complications (such as other infections), rather than from the disease itself.
Death often occurs within 2 years.
Possible Complications
y Deadly infections due to immune system damage
y Disfigurement of the face
y Bleeding (hemorrhage)
When to Contact a Medical Professional
Contact your health care provider if you have symptoms of leishmaniasis after visiting an area where the
disease is known to occur.
Prevention
Preventing sandfly bites is the most immediate form of protection. You can prevent a bite by:
y Wearing insect repellent
y Wearing protective clothing
y Screening windows
y Putting fine mesh netting around the bed (in areas where the disease occurs)
Public health measures to reduce the sandfly population and animal reservoirs are important. There are
no preventive vaccines or drugs for leishmaniasis.
Alternative Names
Kala-azar
References
Jeronimo SMB, DeQueiroz-Sousa A, Pearson RD. Leishmaniasis. In: Goldman L, Ausiello D, eds. C ecil
M edicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier;2007:chap 369.
Related Documents











