Curriculum Planning

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The International Conference on Residency Education | La Conférence internationale sur la formation des résidents
Curriculum Planning
ASPIRE: EssentialsSeptember 26, 2019 - Ottawa
08:00 – 08:15Welcome08:15 – 09:15Enacting a safety culture in residencyEric Monteiro
9:15 – 10:45 *break 9:30-10:15Preparing residents for the initial management of a patient safety incidentBrian Wong
11:30 – 12:15 Lunch
13:15 – 15:00 *break 14:00-14:30Teaching QI on the flyBrian Wong
15:00 – 15:45Planning a QIPS curriculumChris Hillis
10:45 – 11:30Engaging residents to analyze and design safer systemsEd Kwok
12:15 – 13:15Engaging residents to analyze and design safer systems - continuedEd Kwok
Patient Safety & Medical Education
Teaching PS to Trainees
• Formal curriculum• Informal curriculum• Hidden curriculum
Acad Med. 2009 84:1510-1515
Patient Safety & Medical Education
Teaching discrete patient safety skills
• Patient handover (Pediatrics: IPASS)• Teamwork training (TEAMSTEPPS)• Disclosing patient safety incidents*• Incident reporting• Patient centered communication• Simulation
Patient Safety & Medical Education
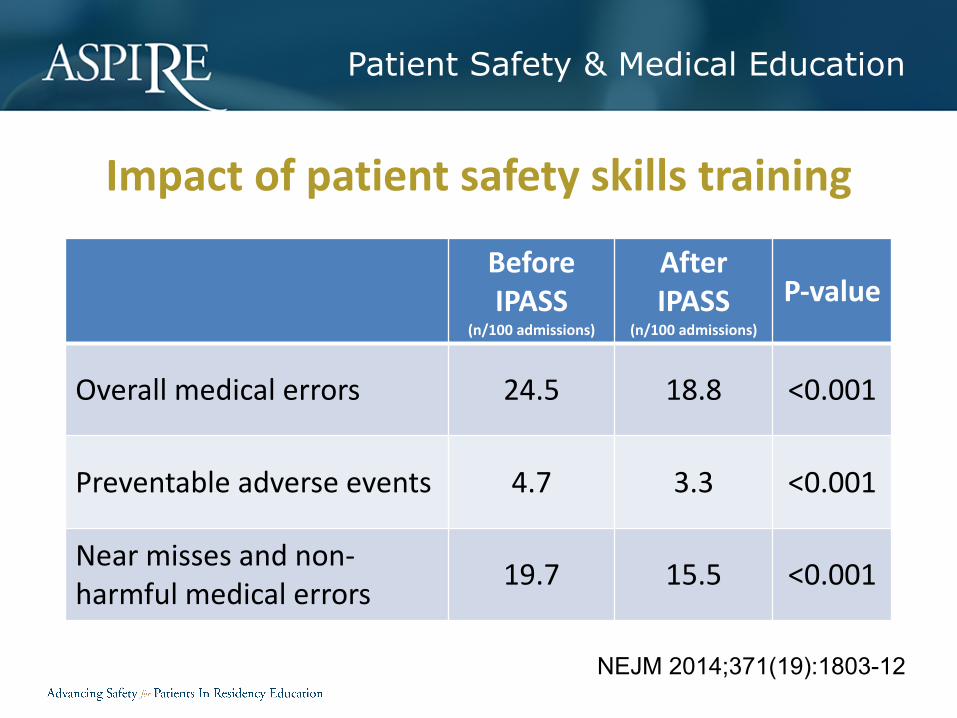
Impact of patient safety skills training
Before IPASS
(n/100 admissions)
After IPASS
(n/100 admissions)
P-value
Overall medical errors 24.5 18.8 <0.001
Preventable adverse events 4.7 3.3 <0.001
Near misses and non-harmful medical errors 19.7 15.5 <0.001
NEJM 2014;371(19):1803-12
Educational Design
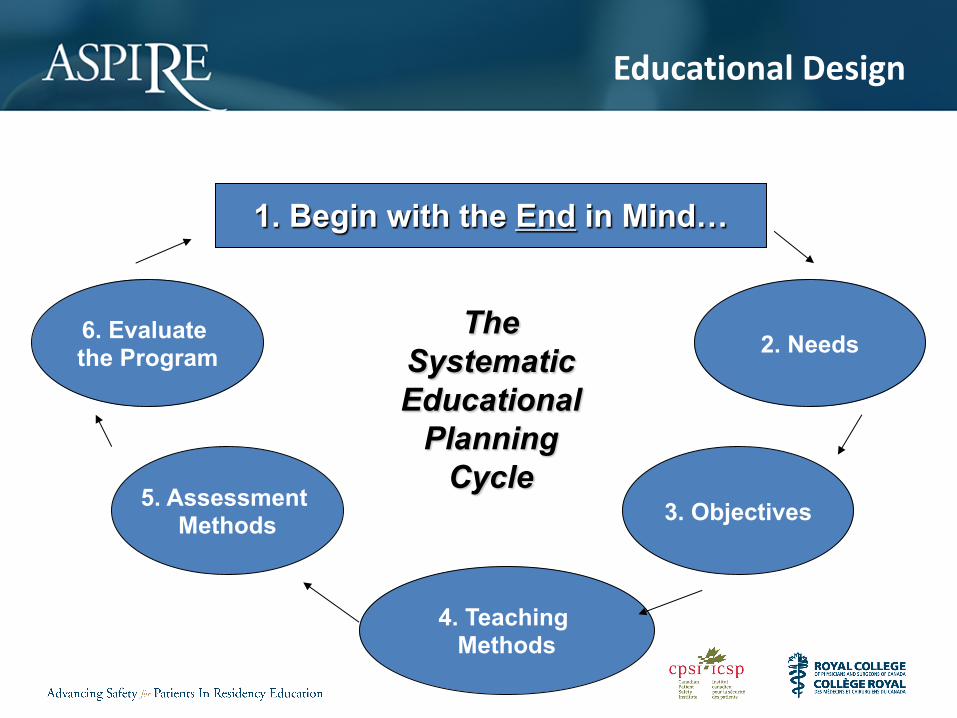
Educational design
The systematic plan for an educational event.
So How To Begin…?
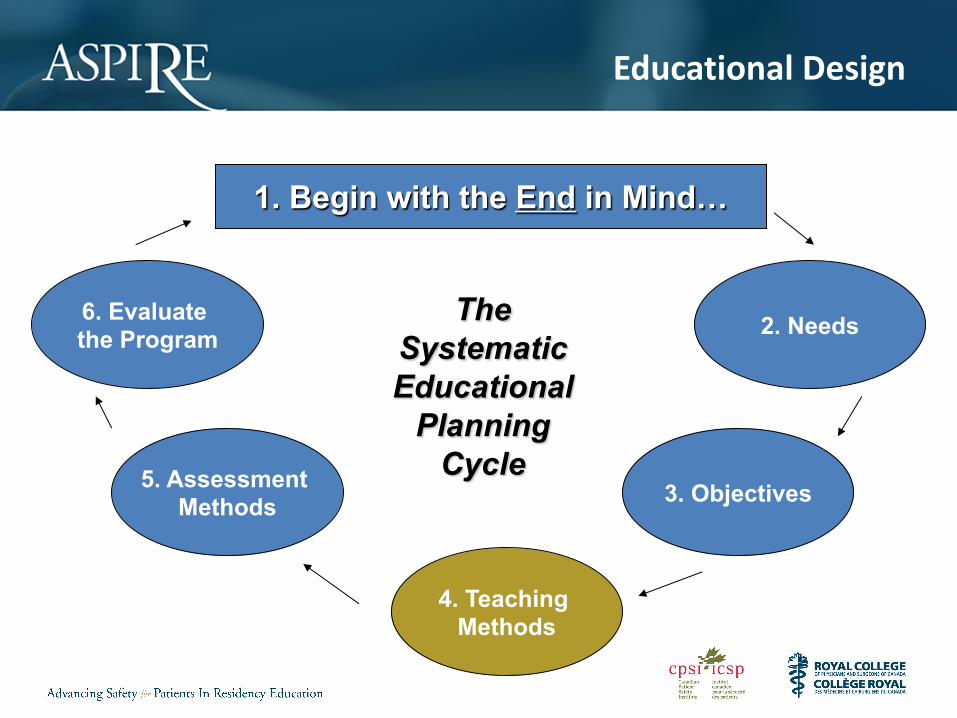
Educational Design
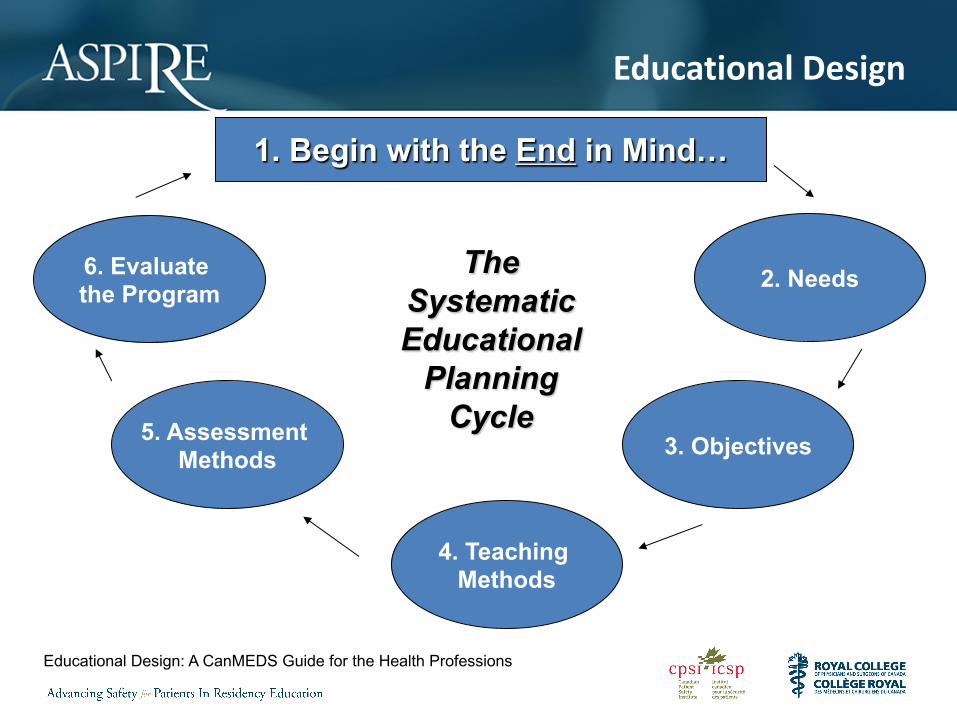
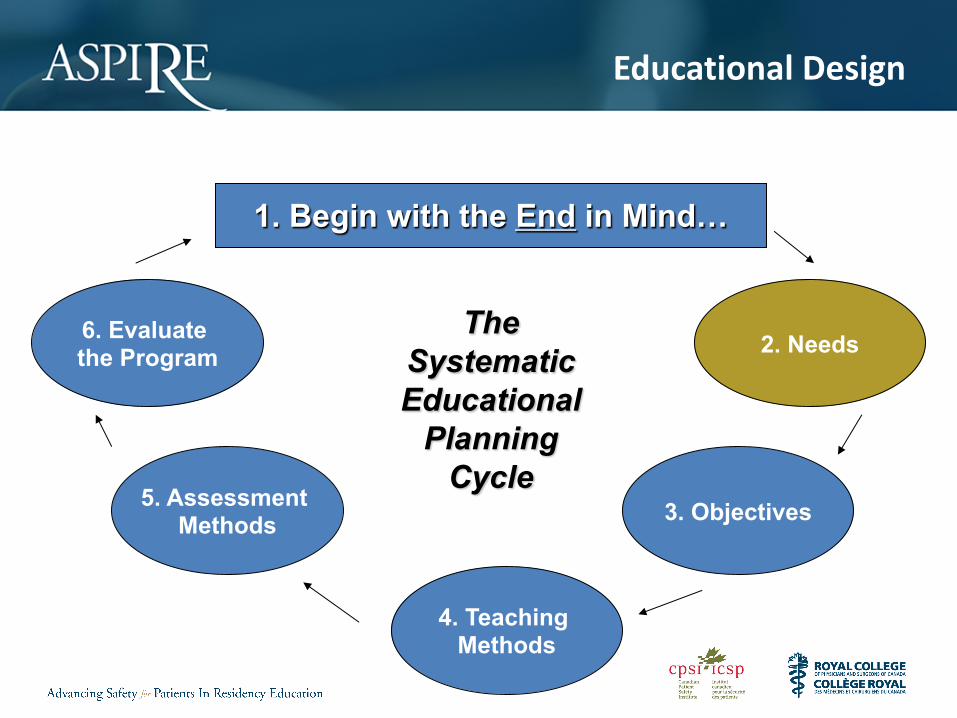
1. Begin with the End in Mind…
2. Needs
3. Objectives
4. Teaching Methods
5. Assessment Methods
6. Evaluate the Program
The Systematic Educational
Planning Cycle
Educational Design: A CanMEDS Guide for the Health Professions
Patient Safety & Medical Education
Ultimate Goal of ASPIRE• To advance patient safety education through
faculty development
Educational Design
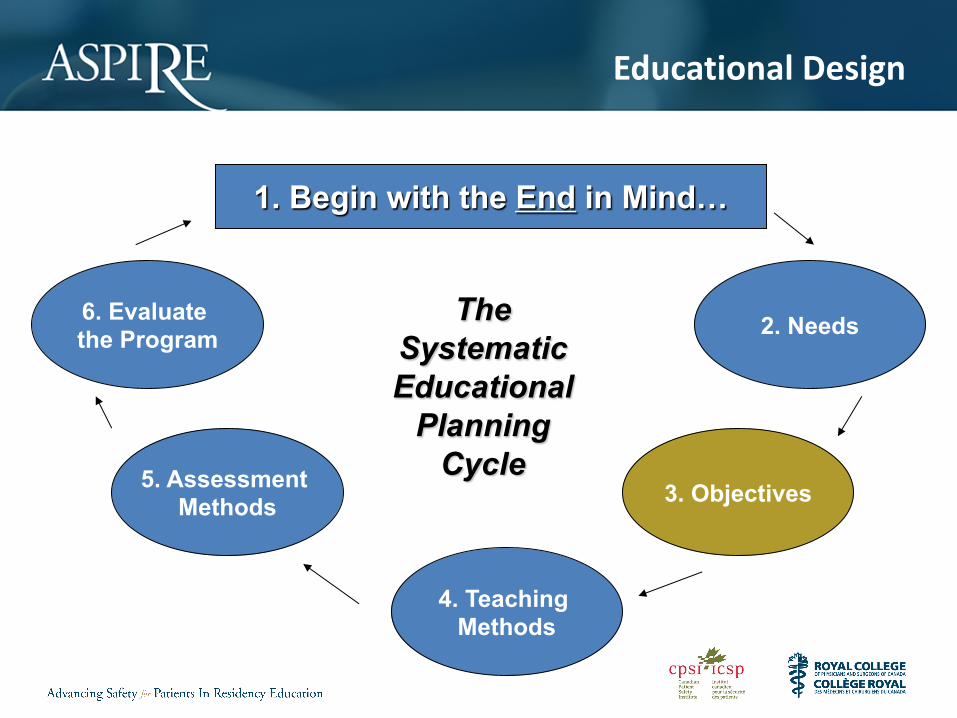
1. Begin with the End in Mind…
2. Needs
3. Objectives
4. Teaching Methods
5. Assessment Methods
6. Evaluate the Program
The Systematic Educational
Planning Cycle
Educational Design
Step 2: Needs Assessment• Perceived needs: I know what I don’t know• Unperceived needs: I don’t know what I
don’t know– These might be institutional needs (i.e.,
organizational priorities) or societal needs (i.e., priorities identified by patients and populations)
Educational Design
1. Begin with the End in Mind…
2. Needs
3. Objectives
4. Teaching Methods
5. Assessment Methods
6. Evaluate the Program
The Systematic Educational
Planning Cycle
Educational Design
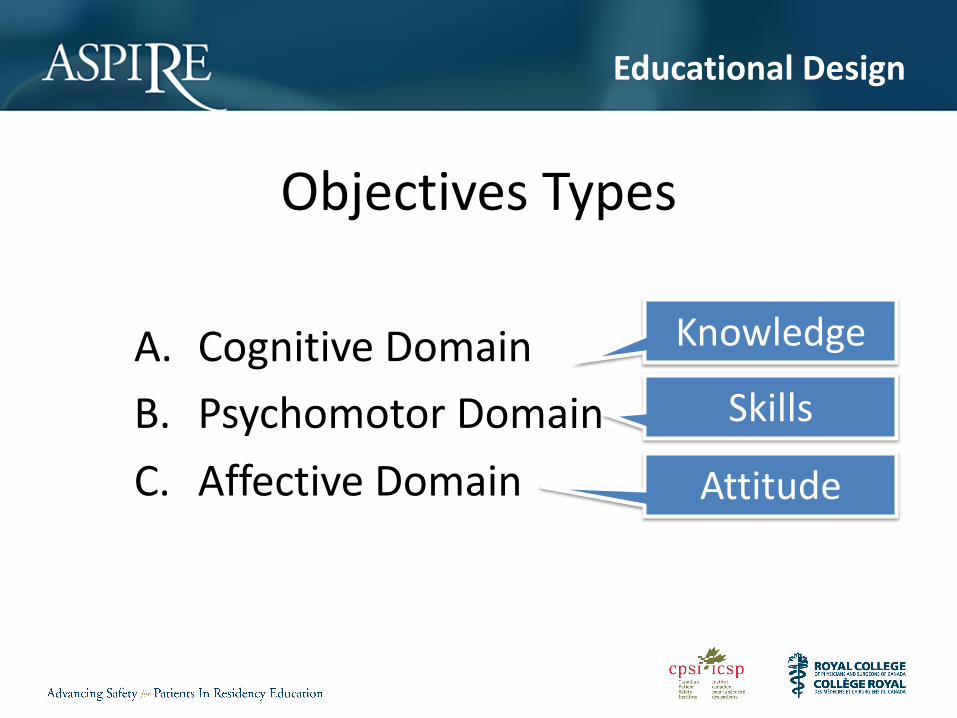
Objectives Types
A. Cognitive DomainB. Psychomotor DomainC. Affective Domain
Knowledge
Skills
Attitude
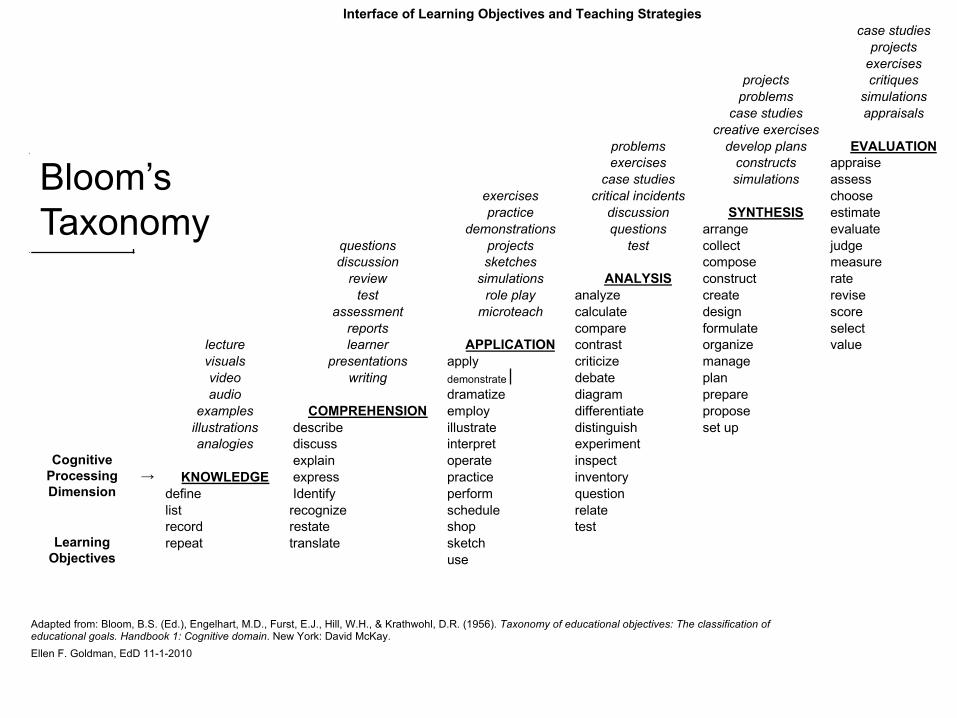
Interface of Learning Objectives and Teaching Strategiescase studies
projectsexercises
projects critiquesproblems simulations
case studies appraisalscreative exercises
problems develop plans EVALUATIONexercises constructs appraise
case studies simulations assessexercises critical incidents choosepractice discussion SYNTHESIS estimate
demonstrations questions arrange evaluatequestions projects test collect judgediscussion sketches compose measure
review simulations ANALYSIS construct ratetest role play analyze create revise
assessment microteach calculate design scorereports compare formulate select
lecture learner APPLICATION contrast organize valuevisuals presentations apply criticize managevideo writing demonstrate debate planaudio dramatize diagram prepare
examples COMPREHENSION employ differentiate proposeillustrations describe illustrate distinguish set upanalogies discuss interpret experiment
Cognitive Processing Dimension
explain operate inspect→ KNOWLEDGE express practice inventory
define Identify perform question list recognize schedule relaterecord restate shop test
Learning Objectives
repeat translate sketchuse
Adapted from: Bloom, B.S. (Ed.), Engelhart, M.D., Furst, E.J., Hill, W.H., & Krathwohl, D.R. (1956). Taxonomy of educational objectives: The classification of educational goals. Handbook 1: Cognitive domain. New York: David McKay.Ellen F. Goldman, EdD 11-1-2010
Bloom’s Taxonomy
Educational Design
1. Begin with the End in Mind…
2. Needs
3. Objectives
4. Teaching Methods
5. Assessment Methods
6. Evaluate the Program
The Systematic Educational
Planning Cycle
Educational Design
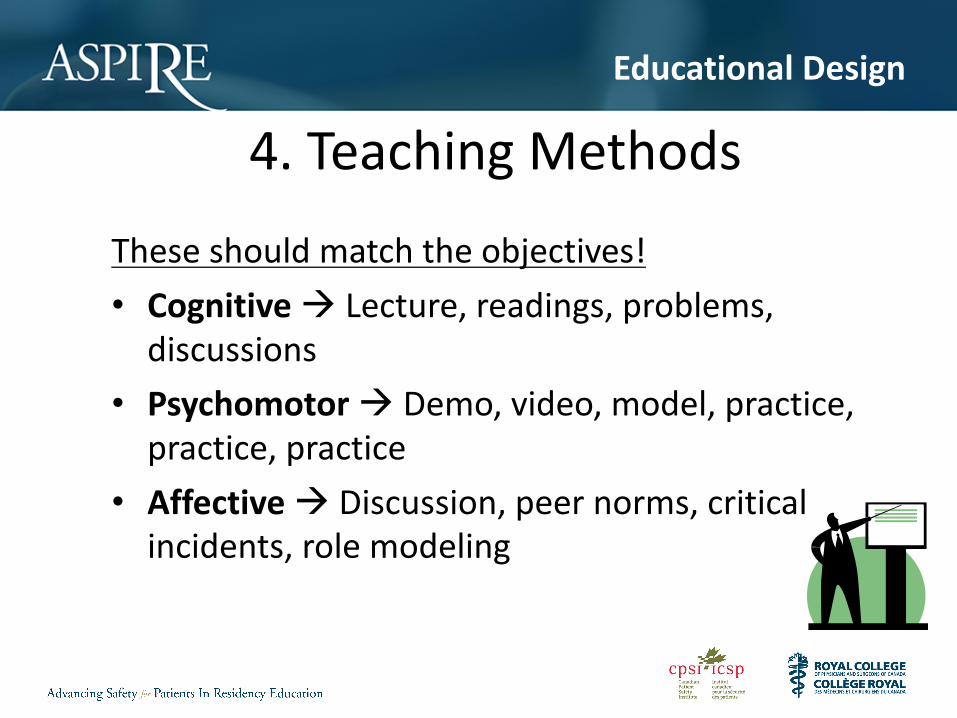
4. Teaching MethodsThese should match the objectives!• Cognitive à Lecture, readings, problems,
discussions• Psychomotor à Demo, video, model, practice,
practice, practice• Affective à Discussion, peer norms, critical
incidents, role modeling
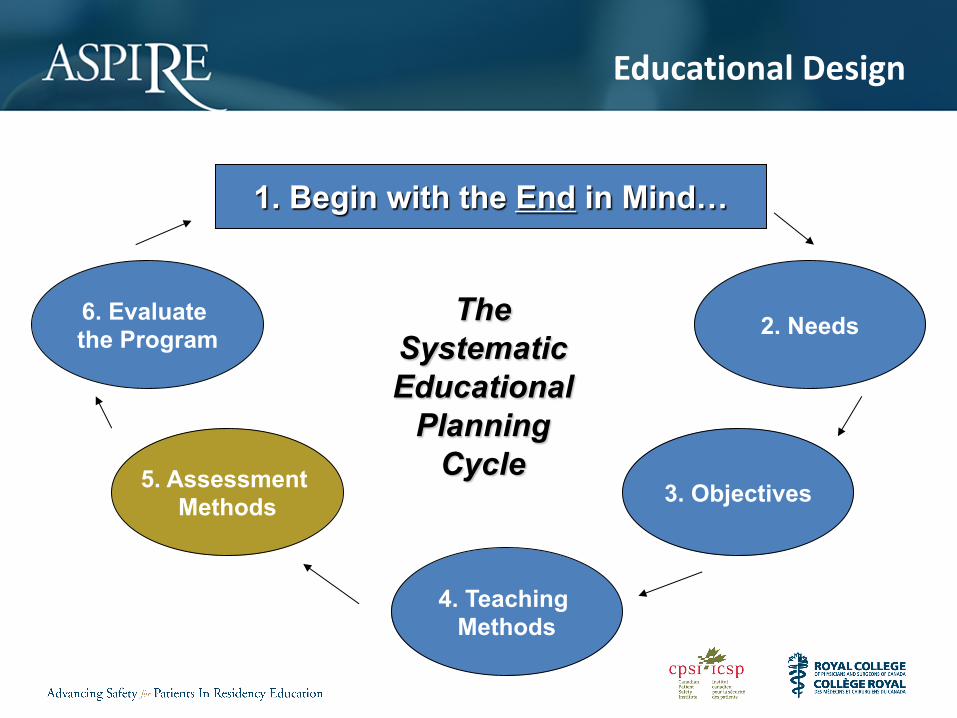
Educational Design
1. Begin with the End in Mind…
2. Needs
3. Objectives
4. Teaching Methods
5. Assessment Methods
6. Evaluate the Program
The Systematic Educational
Planning Cycle
Educational Design
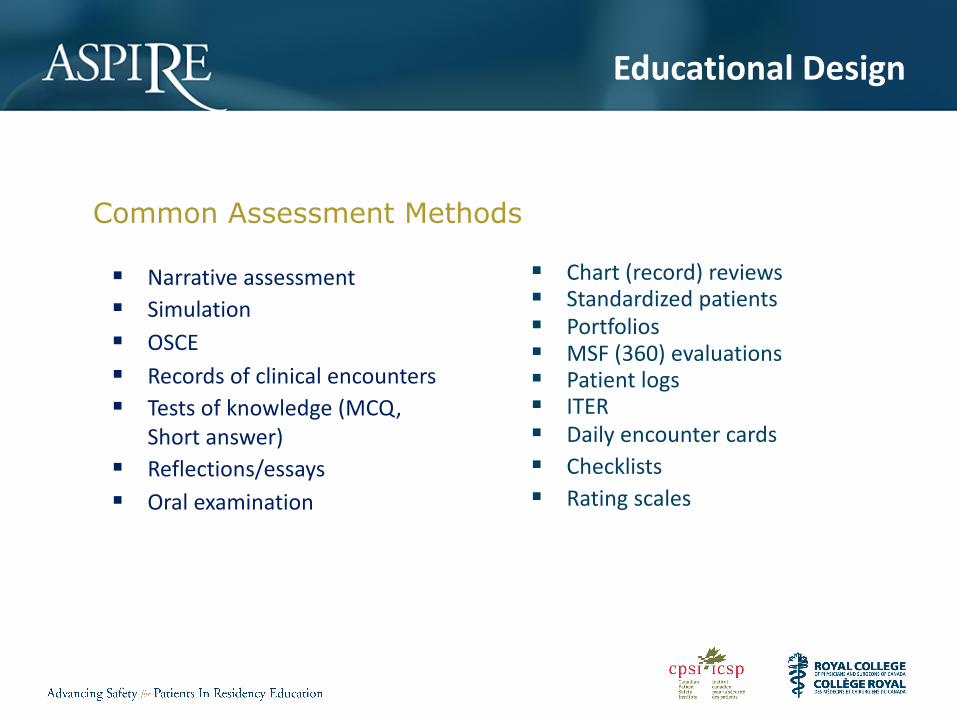
Common Assessment Methods
§ Chart (record) reviews§ Standardized patients§ Portfolios§ MSF (360) evaluations§ Patient logs§ ITER§ Daily encounter cards§ Checklists§ Rating scales
§ Narrative assessment§ Simulation§ OSCE§ Records of clinical encounters§ Tests of knowledge (MCQ,
Short answer)§ Reflections/essays§ Oral examination
Educational Design
Step 5: Learner AssessmentThese should match the objectives!• Cognitive (Knowledge) à Written tests, orals• Psychomotor (Skills) à OSCEs, labs, sims• Affective (Attitudes) à ITERs, peer, 360
Educational Design
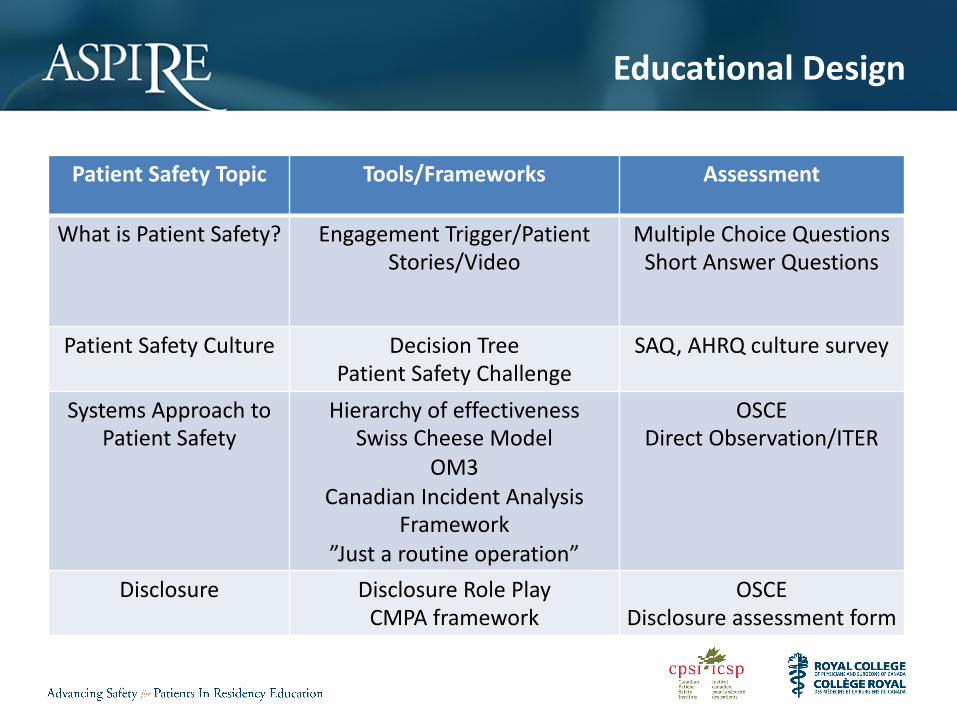
Patient Safety Topic Tools/Frameworks Assessment
What is Patient Safety? Engagement Trigger/Patient Stories/Video
Multiple Choice QuestionsShort Answer Questions
Patient Safety Culture Decision TreePatient Safety Challenge
SAQ, AHRQ culture survey
Systems Approach to Patient Safety
Hierarchy of effectivenessSwiss Cheese Model
OM3Canadian Incident Analysis
Framework”Just a routine operation”
OSCEDirect Observation/ITER
Disclosure Disclosure Role PlayCMPA framework
OSCEDisclosure assessment form
Educational Design
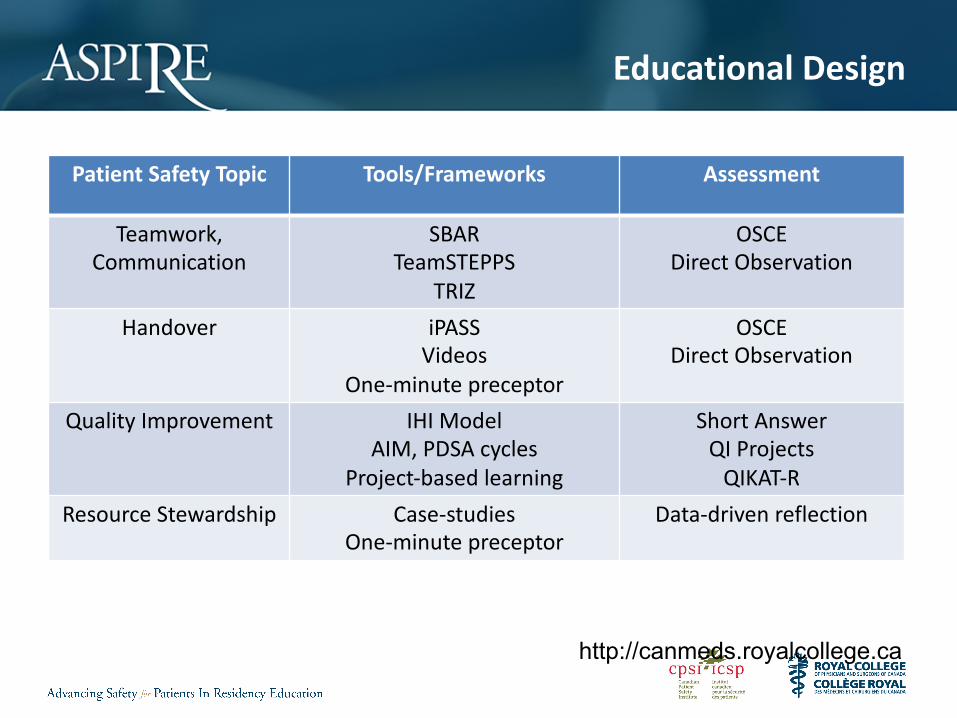
Patient Safety Topic Tools/Frameworks Assessment
Teamwork,Communication
SBARTeamSTEPPS
TRIZ
OSCEDirect Observation
Handover iPASSVideos
One-minute preceptor
OSCEDirect Observation
Quality Improvement IHI ModelAIM, PDSA cycles
Project-based learning
Short AnswerQI Projects
QIKAT-RResource Stewardship Case-studies
One-minute preceptorData-driven reflection
http://canmeds.royalcollege.ca
Educational Design
1. Begin with the End in Mind…
2. Needs
3. Objectives
4. Teaching Methods
5. Assessment Methods
6. Evaluate the Program
The Systematic Educational
Planning Cycle

The International Conference on Residency Education | La Conférence internationale sur la formation des résidents
RESOURCES
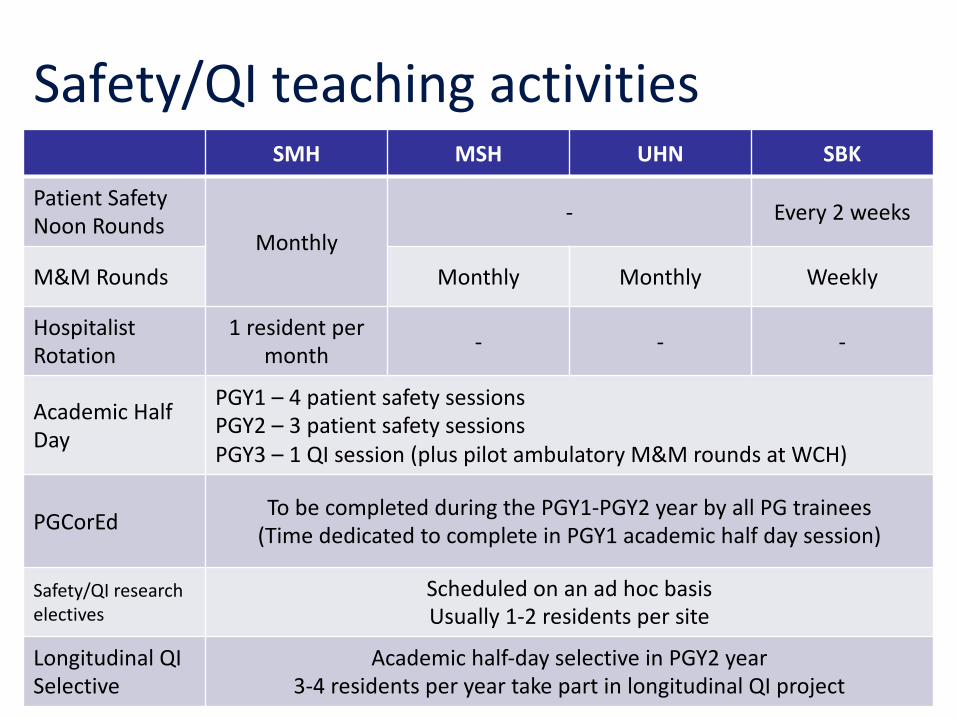
Safety/QI teaching activitiesSMH MSH UHN SBK
Patient Safety Noon Rounds
Monthly- Every 2 weeks
M&M Rounds Monthly Monthly Weekly
Hospitalist Rotation
1 resident per month - - -
Academic Half Day
PGY1 – 4 patient safety sessionsPGY2 – 3 patient safety sessionsPGY3 – 1 QI session (plus pilot ambulatory M&M rounds at WCH)
PGCorEd To be completed during the PGY1-PGY2 year by all PG trainees(Time dedicated to complete in PGY1 academic half day session)
Safety/QI research electives
Scheduled on an ad hoc basisUsually 1-2 residents per site
Longitudinal QI Selective
Academic half-day selective in PGY2 year3-4 residents per year take part in longitudinal QI project
Educational Design
Patient Safety Curriculum Guide
Topic 1 What is patient safety?
1
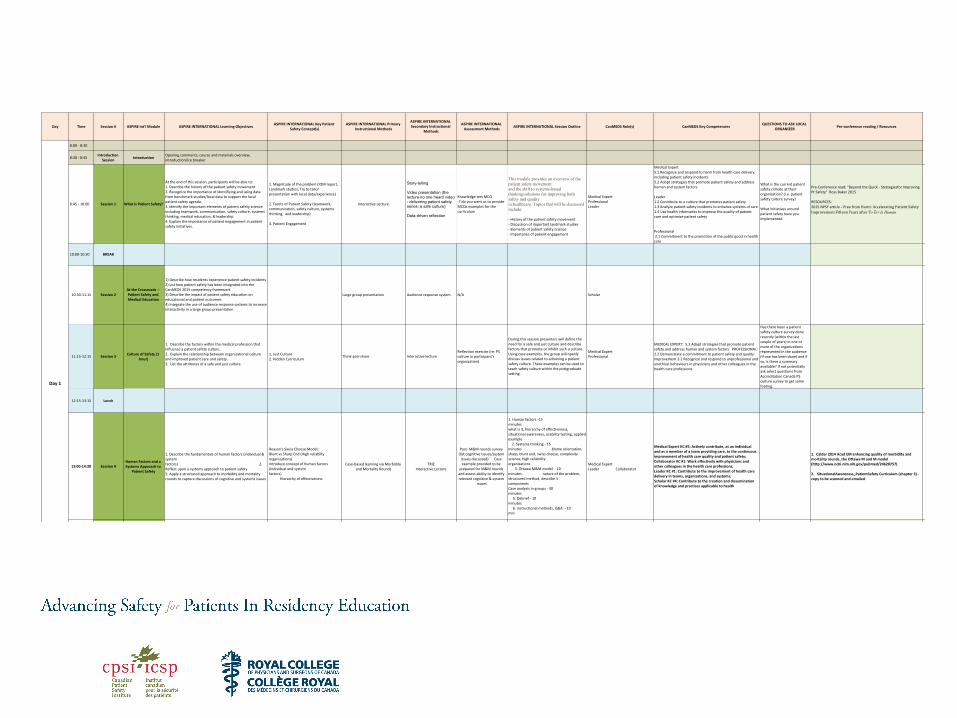
Day Time Session # ASPIRE Int'l Module ASPIRE INTERNATIONAL Learning Objectives ASPIRE INTERNATIONAL Key Patient Safety Concept(s)
ASPIRE INTERNATIONAL Primary Instructional Methods
ASPIRE INTERNATIONAL Secondary Instructional
Methods
ASPIRE INTERNATIONAL Assessment Methods ASPIRE INTERNATIONAL Session Outline CanMEDS Role(s) CanMEDS Key Competencies QUESTIONS TO ASK LOCAL
ORGANIZER Pre-conference reading / Resources Other resources
Day 1
8:00 - 8:30
8:30 - 8:45 Introduction Session Introduction Opening comments, course and materials overview,
introduction/ice breaker
8:45 - 10:00 Session 1 What is Patient Safety?
At the end of this session, participants will be able to: 1. Describe the history of the patient safety movement 2. Recognize the importance of identifiying and using data from benchmark studies/local data to support the local patient safety agenda.3. Identify the important elements of patient safety science including teamwork, communication, safety culture, systems thinking, medical education, & leadership4. Explain the importance of patient engagement in patient safety initiatives.
1. Magnitude of the problem (IOM report, Landmark studies, Try to tailor presentation with local data/experience) 2. Facets of Patient Safety (teamwork, communication, safety culture, systems thinking, and leadership)
3. Patient Engagement
Interactive Lecture
Story-telling
Video presentation (the lecture no one heard video - delivering patient safety series: a safe culture)
Data-driven reflection
Knowledge test MCQ-? do you want us to provide MCQs examples for the curriculum
This module provides an overview of the patient safety movementand the shift to systems-based thinking/solutions for improving both safety and qualityin healthcare. Topics that will be discussed include:
- History of the patient safety movement- Discussion of important landmark studies- Elements of patient safety science- Importance of patient engagement
Medical ExpertProfessionalLeader
Medical Expert5.1 Recognize and respond to harm from health care delivery, including patient safety incidents5.2 Adopt strategies that promote patient safety and address human and system factors
Leader 1.2 Contribute to a culture that promotes patient safety1.3 Analyze patient safety incidents to enhance systems of care 1.4 Use health informatics to improve the quality of patient care and optimize patient safety
Professional 2.1 Commitment to the promotion of the public good in health care
What is the current patient safety climate at their organization? (i.e. patient safety culture survey)
What initiatives around patient safety have you implemented
Pre-Conference read: "Beyond the Quick - Strategiesfor Improving Pt Safety" Ross Baker 2015
RESOURCES:2015 NPSF article - Free from Harm: Accelerating Patient Safety Improvement Fifteen Years after To Err Is Human
10:00-10:30 BREAK
10:30-11:15 Session 2At the Crossroads -- Patient Safety and Medical Education
1) Describe how residents experience patient safety incidents2) List how patient safety has been integrated into the CanMEDS 2015 competency framework3) Describe the impact of patient safety education on educational and patient outcomes4) Integrate the use of audience response systems to increase interactivity in a large group presentation
Large group presentation Audience response system N/A Scholar
11:15-12:15 Session 3 Culture of Safety (1 hour)
1. Describe the factors within the medical profession that influence a patient safety culture. 2. Explain the relationship between organizational culture and improved patient care and safety. 3. List the attributes of a safe and just culture.
1. Just Culture 2. Hidden Curriculum
Think-pair-share Interactive lecture Reflection exercise (re: PS culture in participant's organization)
During this session presenters will define the need for a safe and just culture and describe factors that promote or inhibit such a culture. Using case examples, the group will openly discuss issues related to achieving a patient safety culture. These examples can be used to teach safety culture within the postgraduate setting.
Medical ExpertProfessional
MEDICAL EXPERT: 5.2 Adopt strategies that promote patient safety and address human and system factors PROFESSIONAL: 2.2 Demonstrate a commitment to patient safety and quality improvement 3.2 Recognize and respond to unprofessional and unethical behaviours in physicians and other colleagues in the health care professions.
Has there been a patient safety culture survey done recently (within the last couple of years) in one or more of the organizations represented in the audience (if one has been done) and if so, is there a summary available? If not potentially ask select questions from Accreditation Canada PS culture survey to get some footing.
12:15-13:15 Lunch
13:00-14:30 Session 4Human Factors and a Systems Approach to
Patient Safety
1. Describe the fundamentals of human factors (individual & system factors) 2. Reflect upon a systems approach to patient safety3. Apply a structured approach to morbidity and mortality rounds to capture discussions of cognitive and systems issues
Reason's Swiss Cheese Model; Blunt vs Sharp End (High reliabilty organizations)Introduce concept of human factors (Individual and system factors) Hierarchy of effectiveness
Case-based learning via Morbidity and Mortality Rounds
TRIZInteractive Lecture
Post- M&M rounds survey (list cognitive issues/system
issues discussed) Case example provided to be
prepared for M&M rounds and assess ability to identify relevant cognitive & system
issues
1. Human factors -15 minutes what is it, hierarchy of effectiveness, situational awareness, usability testing, applied example 2. Systems thinking - 15 minutes blame orientation, sharp, blunt end, swiss cheese, complexity science, high reliability organizations 3. Ottawa M&M model -10 minutes nature of the problem, structured method, describe 5 components 4. Case analysis in groups - 30 minutes 5. Debrief - 10 minutes 6. instructional methods, Q&A - 10 min
Medical ExpertLeader Collaborator
Medical Expert KC #5: Actively contribute, as an individual and as a member of a team providing care, to the continuous improvement of health care quality and patient safety; Collaborator KC #1: Work effectively with physicians and other colleagues in the health care professions; Leader KC #1: Contribute to the improvement of health care delivery in teams, organizations, and systems; Scholar KC #4: Contribute to the creation and dissemination of knowledge and practices applicable to health
1. Calder 2014 Acad EM enhancing quality of morbidity and mortality rounds_the Ottawa M and M model(http://www.ncbi.nlm.nih.gov/pubmed/24628757)
2. SituationalAwareness_PatientSafety Curriculum (chapter 3) - copy to be scanned and emailed
14:30 - end Session 5 Recap / Office Hours
Day 2
8:00 - 8:30 Breakfast / "office hours" "Office Hours"
8:30-10:00 Session 6 Patient Safety Incidents
1. Describe a framework for managing patient safety incidents, including the need to learn from events2. Recognize and respond to a patient safety incident, including identifying the threshold for disclosure 3. Apply a structured communication framework to disclose a patient safety incident to a patient/family member
1) Patient safety incident management framework (high level overview)2) Recognize / categorize patient safety incidents 3) Initial response (clinical management of the patient)4) Threshold for disclosure5) Communication framework for disclosure -- demonstrate how to do well6) Second victim
Role play (in small groups vs fishbowl)Interactive lecture Case description/patient story
Q
1. Definitions (PSI, near miss) - 5minutes 2. Recognizing and responding (recall of personal experience) - 15 minutes 3. caring for the second victim - 5 minutes 4. CMPA disclosure framework - 15 minutes 5. CPSI patient safety incident framework - 15 minutes 6. Role play of disclosure - 30 minutes 7 Debrief - 10 minutes 8. Instructional methods , & Q&A - 10 minutes
Medical expertCommunicatorProfessional
Medical Expert: 5.1 Recognize and respond to harm from health care delivery, including patient safety incidentsCommunicator: 3.2 Disclose harmful patient safety incidents to patients and their families accurately and appropriatelyProfessional: 4.3 Promote a culture that recognizes, supports, and responds effectively to colleagues in need
How are patient safety incidents measured and managed in their setting? Any cultural issues / legal requirements for disclosure that we should be aware of?
Disclosing harm from healthcare delivery: Open and honest communication with patients(https://www.cmpa-acpm.ca/-/disclosing-harm-from-healthcare-delivery-open-and-honest-communication-with-patients)
Medical ExpertLeaderCommunicator
Leader: 1.3 Analyze safety incidents to enhance systems of care
CPSI Canadian Incident Analysis Framework
http://www.patientsafetyinstitute.ca/English/toolsResources/IncidentAnalysis/Documents/Canadian
%20Incident%20Analysis%20Framework.PDF
10:00-10:30 Break
Educational Design
Objectives
Pt. Safety Competencies
Instr. Methods
Assessment
Outline
CanMEDS
Resources


Please complete your session evaluation.
Related Documents











