Current Trends in FCE Standards and RAW Services An update on how to interpret evaluations and the effectiveness of on-site services

Current Trends in FCE Standards and RAW Services An update on how to interpret evaluations and the effectiveness of on-site services.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Current Trends in FCE Standards and RAW ServicesAn update on how to interpret evaluations and the effectiveness of on-site services

Intro to your presenter
Kevin Jones, PT,DPT,CSCS,TWD
• 8.5 years of practice• Doctorate degree from University of
Indianapolis• Transitional work developer and creator of
Active at Work Consulting• “Reform Advocate”• Co-owner at Active Physical Therapy in Hilliard
www.activePTcolumbus.com
What stinks?
Objectives
• Attendee will gain knowledge of all components of a typical functional capacity evaluation
• Attendee will improve understanding of how to identify quality reporting measures (not all FCEs are created equal!!)
• Attendee will gain a more comprehensive understanding of when and how FCEs are used for injured worker guidance
• Attendee will gain knowledge of current evidence supporting transitional work and onsite physical therapy services

Intro to FCEs
• Brief History• Used by Occupational therapists and psychologists in 1947 for veterans of
WWII• Became used in Workers’ Comp in mid 1970s (Matheson)• 1990s saw a rapid increase in number of models
• FCEs are a bridge between subjective self-reports and objective analysis• What can the client do safely?• What can the person do repetitiously?• Did the person give full effort?
• Lack of standardization and consistency has created frustration and confusion
Intro to FCEs
• Components of FCE Testing• History and review of medical records• Physical Examination• Movement tests • Material handling tests• Aerobic tests• Positional tolerance

Intro to FCEs
Job-Specific General FCE
Job-specific task assessment Generic work items
Short, less expensive Longer, more expensive
Must be created from job description
Standardized models created already
Includes unique job tasks Can be used for many jobs
Early and chronic claims Chronic claims
Types of return-to-work FCEs
Intro to FCEs
• What constitutes quality?• MEET THE NEEDS OF ALL STAKEHOLDERS!• Scientific reliability and validation• Indications of safety of work performance• Indications of MAXIMUM work performance• Clarity of language• Work task language• Information that links physical ability with work, that must include
PSYCHOPHYSICAL considerations• Objective information that is written in clear and concise terms by a
professional with a BACKGROUND that supports ability to do functional capacity testing

FCE components: Interview
• Intake interview and subjective history• Must include review of imaging, surgical reports, and
treatment to date• Review injury specifics• Ask about employment history and education level• Assess potential contraindications of testing• Determine injury history and/or prior claims
FCE Components: Psychometric Questionnaires
• Assesses individual response to illness and disability• Low Back: Oswestry Disability Index• Shoulder: DASH and Quick DASH• Lower extremity: LEFS, FADI• Neck: NDI• Psychosocial: FABQ, TSK
FCE Components- Musculoskeletal evaluation
• Should be focused on claim injury, but can address other limitations
• Strength, range-of-motion, neurological evaluation• Can be a clue to psychophysical processes• Cog wheeling• Flexion relaxation phenomenon (lack of)• Fear of movement and correlates with questionnaires
FCE Components: Dynamic Material Handling
• Use of partial task assessment- should use real-work objects for job-specific evaluation • Low lift• Knee lift• Waist lift• Chest lift• Shoulder lift• Overhead lift
• Recommended end points• Maximal acceptable weight (55% of body weight)• Physiological: O2 consumption; heart rate (USE of RPE**)• Biomechanical• Psychophysical

FCE Components: Positional Tolerances
• Assess injured worker’s ability to sustained postures• Sitting/standing• Walking• Climbing• Balancing/dexterity• Stooping• Kneeling• Crouching• Reaching• Fingering/dexterity• Pushing/Pulling
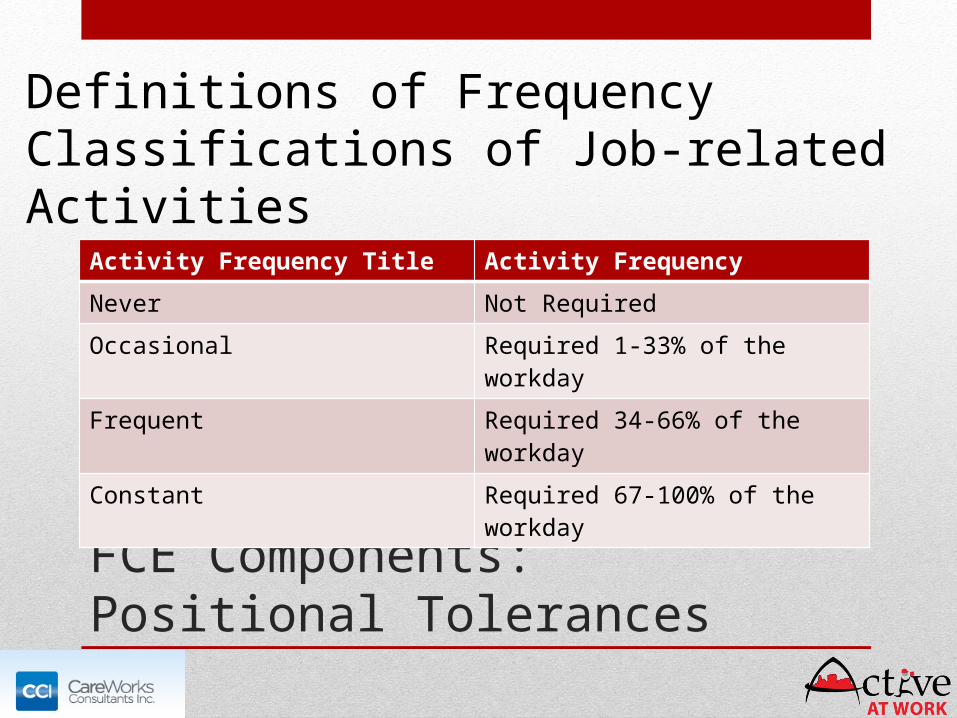
FCE Components: Positional Tolerances
Activity Frequency Title Activity Frequency
Never Not Required
Occasional Required 1-33% of the workday
Frequent Required 34-66% of the workday
Constant Required 67-100% of the workday
Definitions of Frequency Classifications of Job-related Activities
FCE Components: Aerobic Capacity Testing
• Anecdotally, the most overlooked part of FCEs• For job-specific, need to match task demand• Treadmill ergometry• Step Tests (can be utilized for onsite FCEs)• Bicycle ergometry for IWs with balance deficits• Use 40% of VO2max for an 8 hour day

FCE Components: Evaluating IW effort
• Widely Used Methods• Coefficients of Variation (via grip
strength)• Repeated grip measures• Questionable test-retest reliability
and low sensitivity
• Five Rung Grip Test• Should encompass bell-shaped curve
• Non-organic signs (Waddell’s)• Not to be used for sincerity
• Vitals signs vs. RPE; Self-report measures
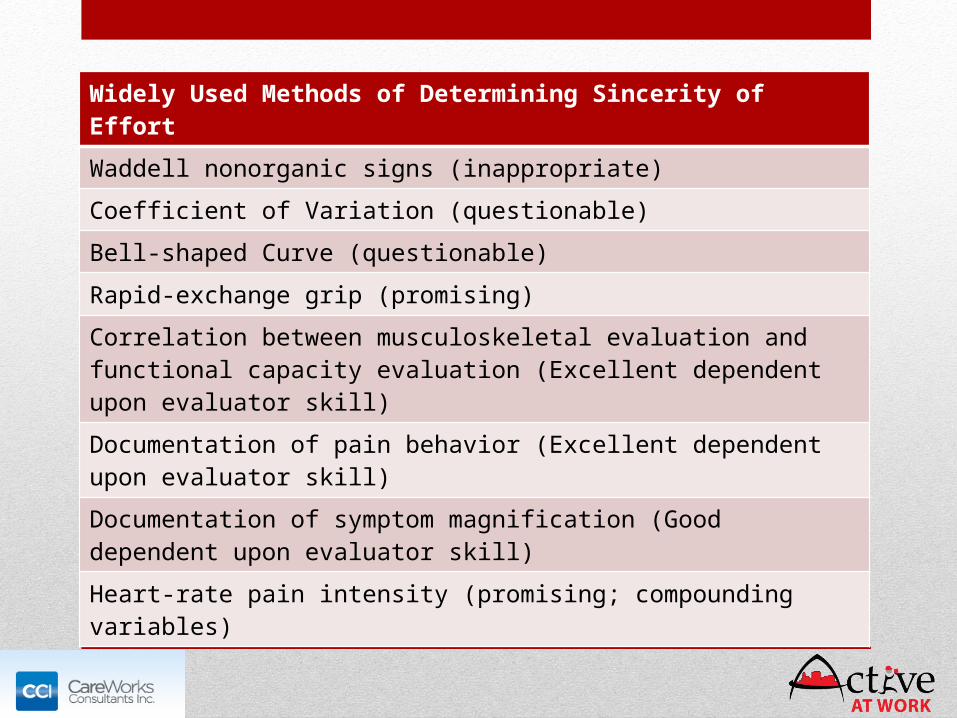
FCE Components: Evaluating IW effort
Widely Used Methods of Determining Sincerity of Effort
Waddell nonorganic signs (inappropriate)
Coefficient of Variation (questionable)
Bell-shaped Curve (questionable)
Rapid-exchange grip (promising)
Correlation between musculoskeletal evaluation and functional capacity evaluation (Excellent dependent upon evaluator skill)
Documentation of pain behavior (Excellent dependent upon evaluator skill)
Documentation of symptom magnification (Good dependent upon evaluator skill)
Heart-rate pain intensity (promising; compounding variables)
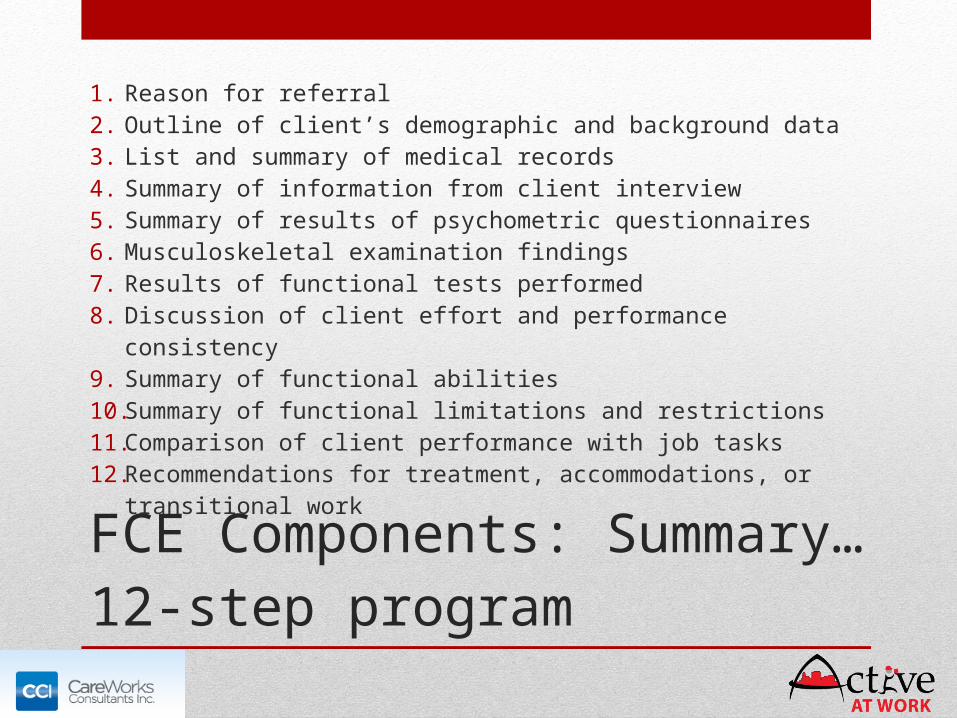
FCE Components: Summary… 12-step program
1. Reason for referral2. Outline of client’s demographic and background data3. List and summary of medical records4. Summary of information from client interview5. Summary of results of psychometric questionnaires6. Musculoskeletal examination findings7. Results of functional tests performed8. Discussion of client effort and performance consistency9. Summary of functional abilities10. Summary of functional limitations and restrictions11. Comparison of client performance with job tasks12. Recommendations for treatment, accommodations, or
transitional work

The striking benefits of remain at work (RAW) services
• Why onsite physical therapy/transitional work?
• Out-of-control claim cost drivers
• Variability of providers
• Lost-time claim frustrations
• Lack of “claim control”
Claim cost drivers
• Early SPECIALIST intervention for basic musculoskeletal injuries (sprain/strain, low back pain)• MRI, X-Ray, injections• Labeling effect that feeds fear-avoidance and claim defense
• “Failed” outpatient physical therapy• Early allowance for higher-cost ICD-9/10 coding
• Failure to utilize predictive models for early recognition of claims “at risk”
• Early attorney involvement
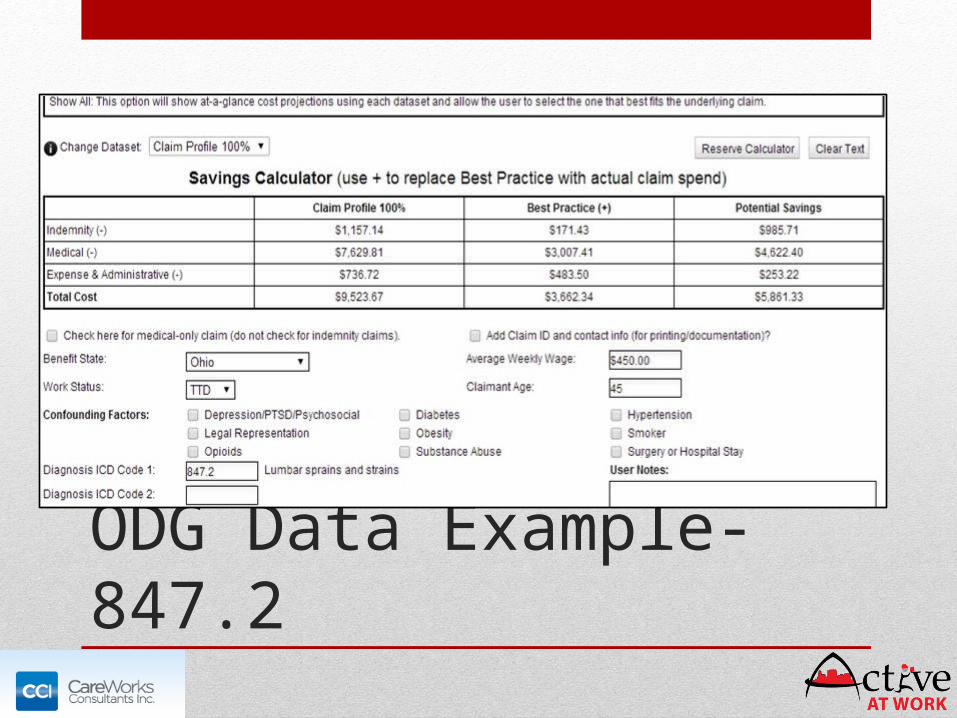
ODG Data Example- 847.2
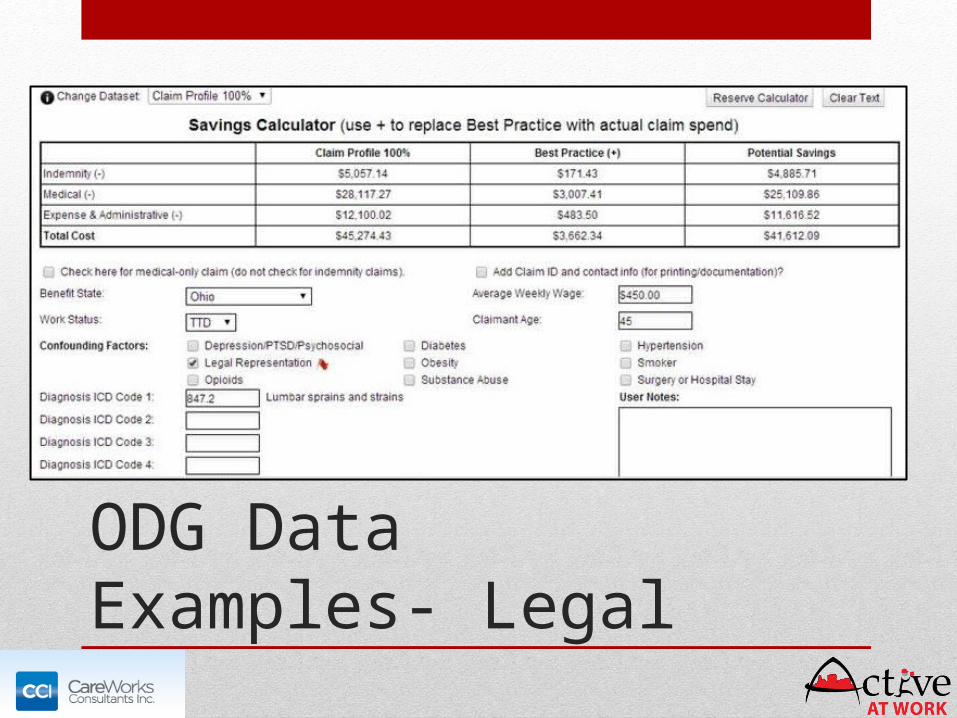
ODG Data Examples- Legal

ODG Data Examples- Surgery

Variability of Providers
• Many PORs (especially specialist MDs/DOs) do not use clinical guidelines to base decision making• Over-reliance on imaging to “rule out”• Arbitrary time-off work and restrictions• Guideline.gov provides updated evidenced-based guidelines• http://www.thecochranelibrary.com/view/0/index.html
• Inherent referral relationships• Most orthopedists own imaging, opening door to treatment• Hospitals, other specialists own PT
Lost-time claim frustrations
• Employer faces indirect and direct claim costs • Direct: Medical, indemnity• Indirect: Loss of production, legal costs, hiring/retraining
new employees
• Employee gets de-conditioned while waiting for treatment and/or office visits with various specialists
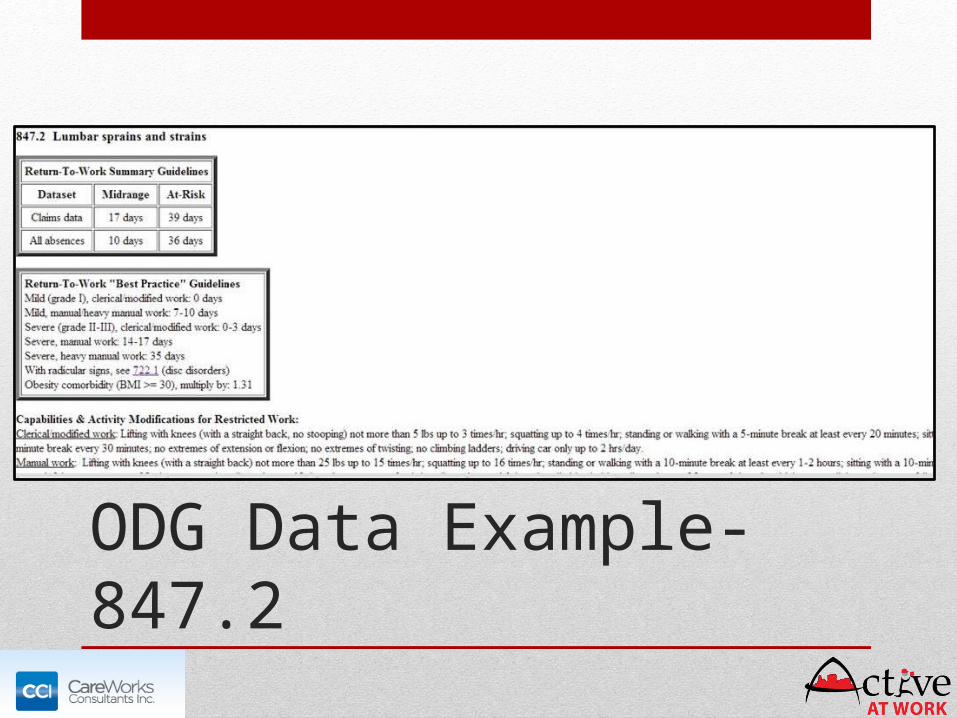
ODG Data Example- 847.2

Lack of Claim Control
• Once IW leaves the worksite, control is lost
• Early denial of treatment may lead to antagonism• Lack of validation of injury• “me vs them” mentality
• A transitional work program can help guide IWs to quality providers and treatment
• Those IWs “at risk” can be managed in a more timely manner
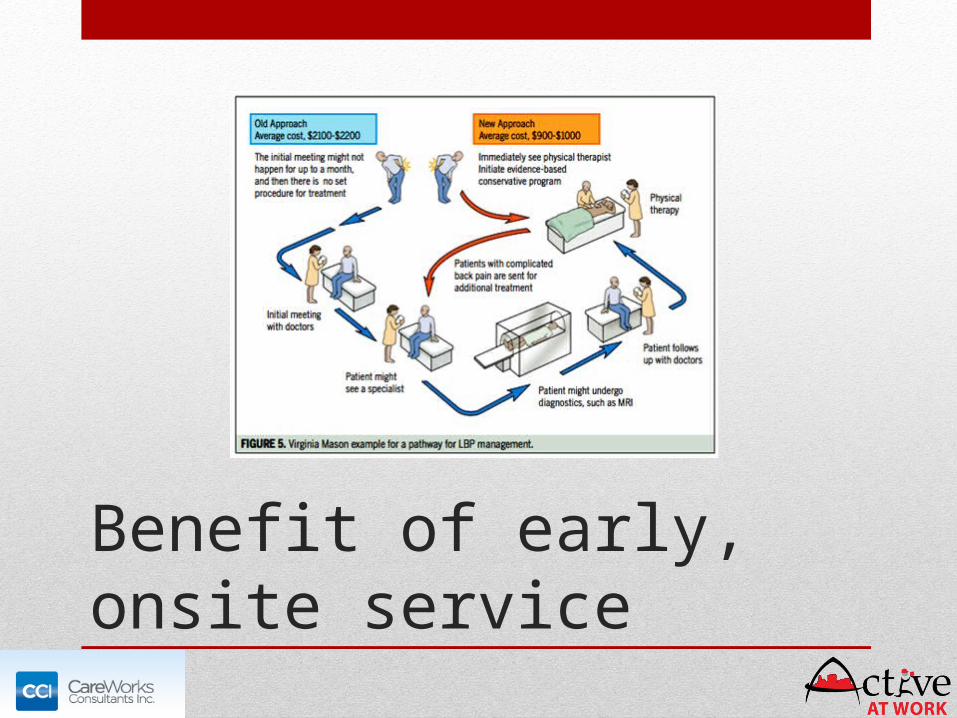
Benefit of early, onsite service
Current evidence
• 2008 study from the University of Cincinnati• Dunning, KK et al in the Journal of
Occupational and Environmental Hygiene• Companies enrolled in TWP and those
who were not were matched for industry type, claim frequency, and size
• Those enrolled saw decrease in indemnity and an improved lost-time to medical-only ratio
• Demonstrated a 2.5 million dollar savings for OBWC

Thank You!
Questions?
Related Documents











