Current Therapy for Type II Diabetes

Current Therapy for Type II Diabetes. New ADA Guidelines- 4/20/12 Inzucchi, Diabetologia 4/20/12 SU most prominent- First, reading L to R Added back.
Jan 02, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Current Therapy for Type II Diabetes

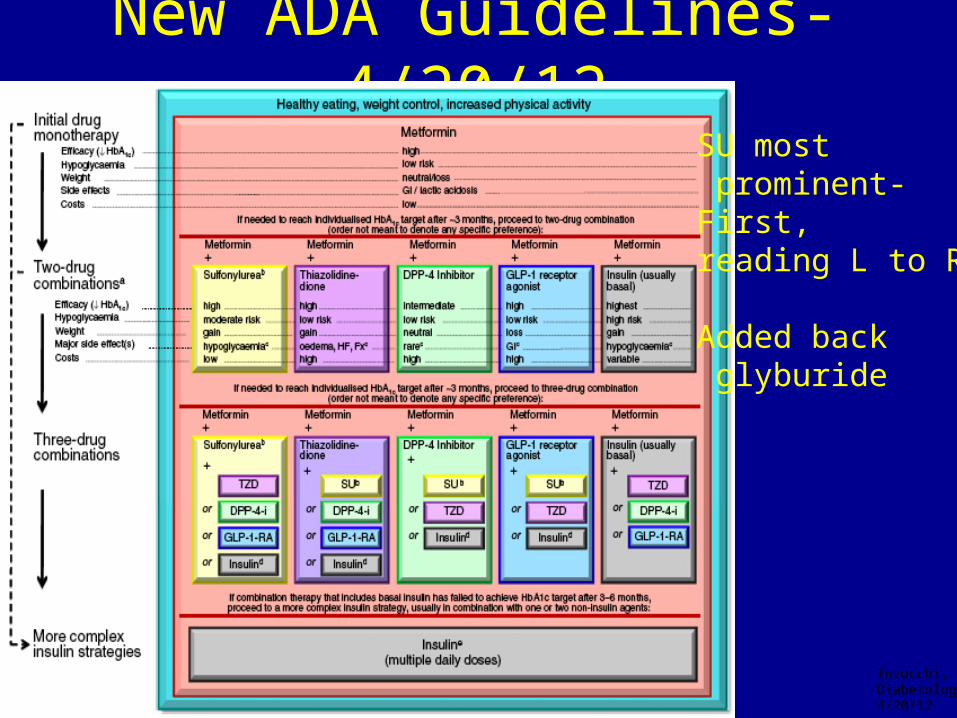
New ADA Guidelines- 4/20/12
Inzucchi,Diabetologia4/20/12
SU most prominent-First, reading L to R
Added back glyburide

Non-Insulin Therapy for Hyperglycemia in Type 2 Diabetes,Treating Defronzo’s Octet:
Match Patient Characteristics to Drug Characteristics
5.Gut CHOAbsorption:
Incretin,Pramlintide,Glucosidase inh.
Peripheralglucose uptake
--
-
1.Pancreatic insulin
Secretion:Incretin, ranolazine
2.Pancreatic glucagon
Secretion- Incretin
HYPERGLYCEMIA
6.Fat- TZD, metformin
7.Brain-TZD,INCRETIN,bromocryptine
8.Kidney-
SGLT2
3.Muscle- TZD, Incretin
4.Liver
Hepatic glucose production:
Metformin, incretin
De

AACE/ACE: Recommendations Based on A1C at Diagnosis/ or When you see in Office
EMPHASIS on Using Combination Therapy to ADDRESS multiple etiologies of hyperglycemia in Octet
Rodbard HW, et al. Endocr Pract. 2009;15:540-559.
A1C 6.5%-7.5% A1C 7.6%-9.0% A1C > 9.0%If undertreatment
If drugnaive
Insulin plusother
agent(s)*Insulin plus
other agent(s)*
Symptoms
No sy
mpt
oms
Lifestyle Modifications
Use Sulfonylureas/Glinides LAST, IF AT ALL
Monotherapy
Dual therapy
Triple therapy
Dual therapy
Triple therapy
Triple therapy
Therapeutic Choice, based on Safety/ Efficacy, Should Match The Drug Characteristics With Patient Characteristics

Issues1. Tells you CONSIDER stopping SU- MUST2. Doesn’t tell you what to do with other non-insulin therapies-CONTINUE3. Doesn’t tell you use other non insulin agents before use prandial insulin since >80 % (conservative) of type 2 pts won’t require bolus insulin if on GLP-1 RA with
SGLT-2 inhibitor +/- other

There is No perfect Exogenous Insulin:All result in HyperInsulinemia and Potential Hypoglycemia
Exogenous Insulin
Perfect glucose sensor-Insulin secretion modulator
Hypoglycemia
NORMAL:Insulin into portal system
and B-cell=
CONCLUSION:DELAY INSULIN THERAPY;AVOID BOLUS RX if possible

Philosophy for Reduced Insulin Need in T2DM
1. No Perfect InsulinExogenous insulin not put in portal system; no fine-tuning a la Beta Cell
2. Leads to Hyperinsulinism- leads to Insulin Resistance (suppresses dopamine in ‘biologic clock’ of hypothalamus)– leads to Increased Weight, Hypoglycemia Risk
3. So Goal of all Insulin Therapy- Least Hypoglycemia, Least Weight Gain
4. Old Logic- use Early Insulin to reduce Glucotoxicity, Lipotoxicity but GLP-1 RAs and SGLT-2 Inh. do that first day!!, with no weight gain, no hypoglycemia
5. Therefore no need for Early Insulin- use 3-4 Non-Insulin therapy before go to Basal Insulin;
keep Non-Insulin Therapies and 95% of T2DM won’t need Bolus Insulin (by avoiding bolus insulin reduce hypoglycemic risk 85%)

Uses Across Continuum of Care
1. Pre-Diabetes
2. Rest of Continuum of Care
3. AACE Guidelines, Triple RX before Insulin Pick Right Drug for Right Patient
4. Delay Need for Insulin No need for Early Insulin
5. If need Insulin, Continue Non-Insulin RX Avoids need for Meal-Time Insulin Decrease Risk Hypoglycemia 85%
6. Get Patients off insulin Had been given Early Insulin
Colsevalam, ranolazine, AGI
Related Documents











