REVIEW Current orthopaedic treatment of ballistic injuries David A. Volgas * , James P. Stannard, Jorge E. Alonso Division of Orthopaedic Surgery, University of Alabama at Birmingham, 950 Faculty Office Tower, 510 South 20th Street, Birmingham, AL 35294-3409, USA Accepted 18 August 2004 Contents Introduction ................................................................ 381 Initial assessment ............................................................ 381 Initial treatment ............................................................. 383 Principles of debridement ....................................................... 383 Retained fragments ........................................................... 383 Joint involvement ............................................................ 383 Vascular injury .............................................................. 383 Neurological injury ........................................................... 384 Fractures ................................................................. 384 Infection .................................................................. 384 Injury, Int. J. Care Injured (2005) 36, 380—386 www.elsevier.com/locate/injury KEYWORDS Gunshot wound; Ballistic injury; Penetrating trauma Summary The purpose of this review is to examine current orthopaedic treatment of gunshot wounds. Surgeons are increasingly confronted by gunshot wounds that occur in both military and civilian settings. Much of the published work has been from military settings. In the United States, low-energy gunshot wounds are very common, and their incidence is increasing elsewhere in the world. Current treatment and its rationale is reviewed and a systematic approach to the assessment and treatment of these injuries is offered, taking into account the entirety of the injury, rather than simply the velocity of the missile. # 2004 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +1 205 934 6413; fax: +1 205 975 9532. E-mail address: [email protected] (D.A. Volgas). 0020–1383/$ — see front matter # 2004 Elsevier Ltd. All rights reserved. doi:10.1016/j.injury.2004.08.038

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Injury, Int. J. Care Injured (2005) 36, 380—386
www.elsevier.com/locate/injury
REVIEW
Current orthopaedic treatment of ballistic injuries
David A. Volgas*, James P. Stannard, Jorge E. Alonso
Division of Orthopaedic Surgery, University of Alabama at Birmingham, 950 Faculty Office Tower,510 South 20th Street, Birmingham, AL 35294-3409, USA
Accepted 18 August 2004
KEYWORDSGunshot wound;Ballistic injury;Penetrating trauma
Summary The purpose of this review is to examine current orthopaedic treatmentof gunshot wounds. Surgeons are increasingly confronted by gunshot wounds thatoccur in both military and civilian settings. Much of the published work has been frommilitary settings. In the United States, low-energy gunshot wounds are very common,and their incidence is increasing elsewhere in the world. Current treatment and itsrationale is reviewed and a systematic approach to the assessment and treatment ofthese injuries is offered, taking into account the entirety of the injury, rather thansimply the velocity of the missile.# 2004 Elsevier Ltd. All rights reserved.
Contents
Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381
Initial assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381
Initial treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
Principles of debridement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
Retained fragments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
Joint involvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
Vascular injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
Neurological injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
Fractures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
Infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
* Corresponding author. Tel.: +1 205 934 6413; fax: +1 205 975 9532.E-mail address: [email protected] (D.A. Volgas).
0020–1383/$ — see front matter # 2004 Elsevier Ltd. All rights reserved.doi:10.1016/j.injury.2004.08.038

Current orthopaedic treatment of ballistic injuries 381
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385
Introduction
After several years of steady increase, firearms-related deaths have declined in the UnitedStates.17—19,24,33 However, in Europe and Canada,firearms-related deaths appear to be on the rise.24
In the United States, there were 30,708 fatal gun-shot wounds and 64,484 nonfatal wounds in 1998,compared to 39,595 fatal and 104,241 nonfatalinjuries in 1993.16 By contrast, 58,156 soldiers diedin the 10-year involvement in Vietnam. The civiliandecline in gunshot deaths follows the downwardtrend in violent crimes during that period. Notwith-standing the favourable trend, deaths related tofirearms remain the fourth leading cause of deathin children under 14 years and the second leadingcause of death for people aged 15—24 in the UnitesStates.16 In 1998, 57% of firearms-related deathswere self-inflicted and overwhelmingly involvedmen, 85%. Of the non-fatal injuries, approximatelyhalf were hospitalized for their injuries.16
In the United States, handguns are often boughtfor home security. However, Kellerman and Reay22
reported that guns kept in the home are 43 timesmore likely to kill a family member, or friend, thanto kill an intruder. While these numbers are likely tobe true, approximately half of these deaths are self-inflicted. Nevertheless, accidental shootings arecommon in the United States.
In Europe, data are more difficult to obtain. Astudy, commissioned by the government of TheNetherlands, found that violent crimes committedby juveniles rose nearly 60% from 1986 to 1994 inEngland and Wales. A similar trend was noted inGermany.37
Initial assessment
Great emphasis has been placed on the distinctionbetween high- and low-velocity weapons. Unfortu-nately, a simplistic approach to gunshot wounds isnot relevant to the spectrum of injuries seen eitherin a combat environment, or in the emergencydepartment of an urban hospital. While it is truethat high-energy weapons have greater woundingcapacity than lower-energy weapons, this knowl-edge does not help the surgeon to treat an individualpatient. Furthermore, the type of weapon usedis commonly not known in the civilian setting.
Likewise, there is a school of thought that focuseson energy transfer as being a major mechanism ofwounding. In truth, energy transfer by itself, exceptwhen caused by very large projectiles such as can-nonballs, is generally not sufficient to cause majordamage. Consider that a 0.45 caliber pistol roundhas 900 J5 of energy, equivalent to a 5 kg weightbeing dropped from a height of 20 m. Even if thesurgeon had a good idea of the amount of energytransferred to tissue, energy can be absorbed dif-ferently, depending on the characteristics of thetissues through which the missile passed.
Because the amount of energy transferred fromthe projectile to the tissues is so variable, and theeffect of a given amount of energy on specific tissuesis equally variable, the surgeon focusing on anyone aspect of energy, or velocity, may be deceived.The surgeon must assess the characteristics of thespecific injury and look for clues that may lead to asuspicion of occult injury.8
What tools, then, does the surgeon have availableto assess the patient? Perhaps the most useful con-cept to employ is that of high- versus low-riskwounds. Using this concept, all available data, suchas bullet fragmentation, path of the projectile,cleanliness of the environment, etc. are used todetermine whether or not the unique combinationof these factors creates an injury which is likely toharm the individual. This concept gives equal weightto all of the mechanisms that can cause injury, notmerely concentrating on a single factor. Table 1 willhelp the surgeon decide if the gunshot wound ishigh- or low-risk.
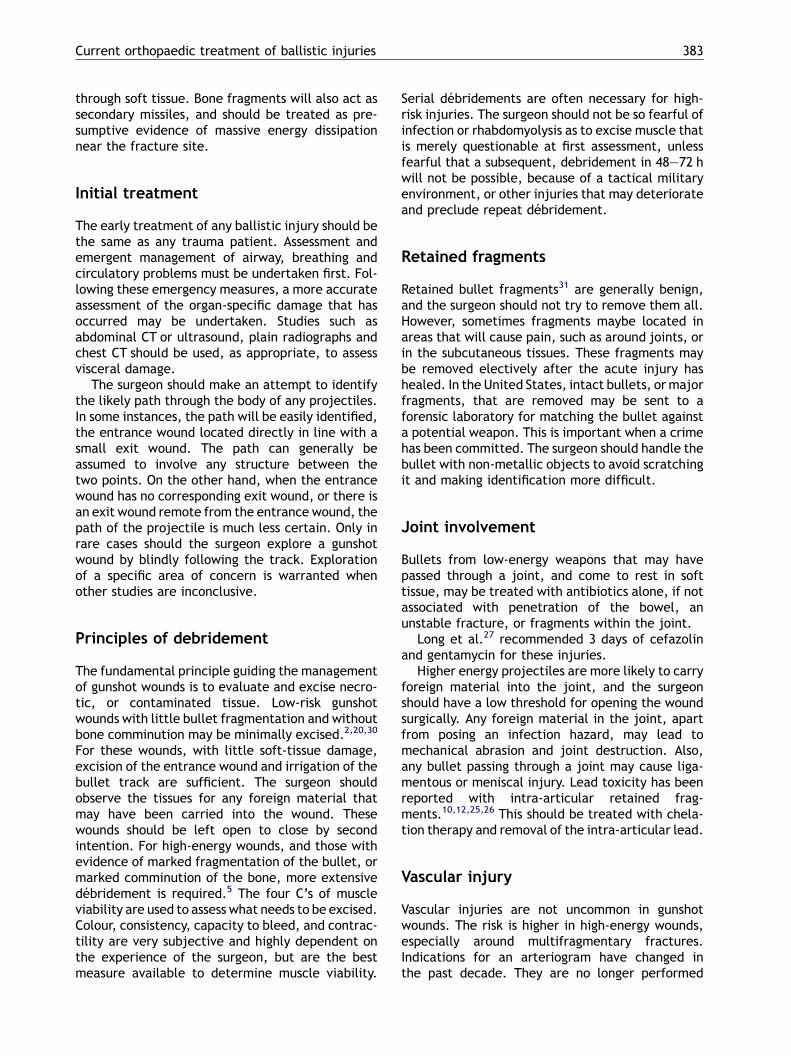
Certainly, the entrance and exit wounds areimportant clues to the nature of the weapon usedand the likely injuries that may be encountered.Fig. 1A shows typical handgun entrance and exitwounds, Fig. 1B shows typical shotgun entrance andexit wounds, and Fig. 1C shows typical military rifleentrance and exit wounds; the latter passed througha door before striking the victim. Note the similaritybetween the shotgun entrance wound and the mili-tary rifle entrance wound. Both demonstratemarked tearing of the skin at the entrance wound.This kind of entrance wound is not typical of militaryrounds. The entrance wound of a military roundoften resembles that of a handgun.
A stellate entrance wound with powder inthe wound is characteristic of contact gunshotwounds.14 Intermediate range gunshot wounds
382 D.A. Volgas et al.
Table 1 Determination of high- vs. low-risk wounds
Low risk High risk
Location of wounding City street Battlefield/farmyardTime to treatment Less than 1 h Greater than 6 hWeapon used Handgun Military rifle, hunting rifle, shotgunPath of projectile Straight through, entrance and
exit wounds at same levelEntrance and exit wounds at differentlevels, �no exit wound
Size of exit wound Small LargeOrgan involvement Skin, muscle only Solid organs, spine, CNS, vascular injuryBone involvement Intact, little comminution Much comminutionBullet fragmentation Little MuchNumber of projectiles One Several
may have a stippled appearance around the wound,which is caused by unburned powder embedded inthe skin.15 Long-range wounds, especially fromhigh-energy weapons, typically have a smallentrance wound, but if the bullet strikes anotherobject, such as a belt buckle, or is fired from lessthan 25 m (themissile still precessing), the entrancewound may be oblique and slightly larger.
Exit wounds reflect what happened to the bulletbetween the entrance and the exit. For example, ahigh-velocity round, which passes through the thighwithout striking bone, will generally have an exitwound only slightly larger than the entrance wound.Little intervening damage will have been done. Onthe other hand, a round which yaws within the soft
Figure 1 (A) Typical handgun entrance and exit wounds; (military rifle entrance and exit wounds (which passed throug
tissue, or strikes bone, may either not exit the body,or may leave a large exit wound.
The path through the soft tissues will also giveimportant clues to damage to be expected. Anentrance wound in the thigh and a bullet thatremains intact in the abdomen, must be assumedto have penetrated all of the intervening structures.It is rarely indicated thoroughly to explore theentire wound track, but it is necessary to look care-fully for signs of injury to the bladder, colon, etc.
Bullet fragmentation is a major contributor towounding.5 Evidence of fragmentation is usuallyapparent on plain radiographs. The surgeon shouldconsider fragmentation to be the equivalent ofmultiple small missiles, each with its own track
B) typical shotgun entrance and exit wounds; (C) typicalh a door before striking the victim).
Current orthopaedic treatment of ballistic injuries 383
through soft tissue. Bone fragments will also act assecondary missiles, and should be treated as pre-sumptive evidence of massive energy dissipationnear the fracture site.
Initial treatment
The early treatment of any ballistic injury should bethe same as any trauma patient. Assessment andemergent management of airway, breathing andcirculatory problems must be undertaken first. Fol-lowing these emergency measures, a more accurateassessment of the organ-specific damage that hasoccurred may be undertaken. Studies such asabdominal CT or ultrasound, plain radiographs andchest CT should be used, as appropriate, to assessvisceral damage.
The surgeon should make an attempt to identifythe likely path through the body of any projectiles.In some instances, the path will be easily identified,the entrance wound located directly in line with asmall exit wound. The path can generally beassumed to involve any structure between thetwo points. On the other hand, when the entrancewound has no corresponding exit wound, or there isan exit wound remote from the entrance wound, thepath of the projectile is much less certain. Only inrare cases should the surgeon explore a gunshotwound by blindly following the track. Explorationof a specific area of concern is warranted whenother studies are inconclusive.
Principles of debridement
The fundamental principle guiding the managementof gunshot wounds is to evaluate and excise necro-tic, or contaminated tissue. Low-risk gunshotwounds with little bullet fragmentation and withoutbone comminution may be minimally excised.2,20,30
For these wounds, with little soft-tissue damage,excision of the entrance wound and irrigation of thebullet track are sufficient. The surgeon shouldobserve the tissues for any foreign material thatmay have been carried into the wound. Thesewounds should be left open to close by secondintention. For high-energy wounds, and those withevidence of marked fragmentation of the bullet, ormarked comminution of the bone, more extensivedebridement is required.5 The four C’s of muscleviability are used to assess what needs to be excised.Colour, consistency, capacity to bleed, and contrac-tility are very subjective and highly dependent onthe experience of the surgeon, but are the bestmeasure available to determine muscle viability.
Serial debridements are often necessary for high-risk injuries. The surgeon should not be so fearful ofinfection or rhabdomyolysis as to excise muscle thatis merely questionable at first assessment, unlessfearful that a subsequent, debridement in 48—72 hwill not be possible, because of a tactical militaryenvironment, or other injuries that may deteriorateand preclude repeat debridement.
Retained fragments
Retained bullet fragments31 are generally benign,and the surgeon should not try to remove them all.However, sometimes fragments maybe located inareas that will cause pain, such as around joints, orin the subcutaneous tissues. These fragments maybe removed electively after the acute injury hashealed. In the United States, intact bullets, or majorfragments, that are removed may be sent to aforensic laboratory for matching the bullet againsta potential weapon. This is important when a crimehas been committed. The surgeon should handle thebullet with non-metallic objects to avoid scratchingit and making identification more difficult.
Joint involvement
Bullets from low-energy weapons that may havepassed through a joint, and come to rest in softtissue, may be treated with antibiotics alone, if notassociated with penetration of the bowel, anunstable fracture, or fragments within the joint.
Long et al.27 recommended 3 days of cefazolinand gentamycin for these injuries.
Higher energy projectiles are more likely to carryforeign material into the joint, and the surgeonshould have a low threshold for opening the woundsurgically. Any foreign material in the joint, apartfrom posing an infection hazard, may lead tomechanical abrasion and joint destruction. Also,any bullet passing through a joint may cause liga-mentous or meniscal injury. Lead toxicity has beenreported with intra-articular retained frag-ments.10,12,25,26 This should be treated with chela-tion therapy and removal of the intra-articular lead.
Vascular injury
Vascular injuries are not uncommon in gunshotwounds. The risk is higher in high-energy wounds,especially around multifragmentary fractures.Indications for an arteriogram have changed inthe past decade. They are no longer performed
384 D.A. Volgas et al.
‘‘for proximity’’ wounds, that is wounds whose pathpasses close to a major artery. Rather, a more care-ful clinical assessment is made to determine if thepulse is identical to the contralateral one.9 If thereare diminished pulses in the injured extremity, anarteriogram is indicated. Pseudoaneurysm andaneurysm have been reported in association withgunshot wounds.1,6,23,40 A bruit may be present overan aneurysm and should also lead to an arteriogram,or exploration.
Neurological injury
Nerve palsy is a common finding in gunshot woundsand is usually temporary. Omer28 reported thatspontaneous recovery occurred in nearly 70%,usually within 6—9 months. Because of this, mostsurgeons opt to treat these injuries expectantly. Ifthere is no recovery within 6—12 weeks, an EMGmaybe useful to determine whether there is nerverecovery. Certainly, if a wound requires debride-ment and the surgeon takes the opportunity toobserve whether or not the nerve is in continuity,this will aid in decision-making. A nerve that isknown to be transected should be repaired afterthe acute inflammation has subsided. Recoveryafter nerve repair is reported to be 25%.28
Fractures
For the most part, any fractures may be treatedas an identical fracture caused by a differentmechanism. However, marked comminution atthe fracture site implies that there may be manydevitalized bone fragments. This, coupled with theknowledge that there is often extensive soft tissuedamage associated with this type of ballistic frac-ture and that the bullets are not sterile,35,36,38 willgenerally lead to treatment as an open fracture.Clearly, fractures that are caused by high-energyweapons, or shotguns, should be treated as openfractures.3,5,20,21,41 Thorough debridement andirrigation of the fracture site, with removal ofdevitalized bone fragments, is required. Whenthe bone cannot be covered by soft tissue, anantibiotic bead pouch, or negative-pressure ther-apy, may be used.
Fractures caused by gunshots are often multi-fragmentary. These fractures will frequently requirebone grafting, but this should be delayed until anyacute inflammatory response has resolved and thewound is healed.
Fractures caused by bullets that have first passedthrough large bowel, oesophagus or pharynx, should
be considered contaminated and generally requireoperative debridement of the fracture.7,32 Stabili-zation of these fractures should be based on thefracture stability. Therefore, a bullet that passesthrough the colon and causes an iliac wing fracturemay require no treatment of the fracture other thanirrigating the fracture site. This concept also appliesto gunshot wounds of the spine.4,32
There is debate over whether fractures can becaused indirectly by the temporary cavity createdby high-energy projectiles.5 It appears that whilethis mechanism is possible, it is unusual. Thesefractures likewise tend to be simpler patterns anddo not require extensive debridement.
Infection
Infection has historically been a major cause ofmortality on the battlefield. In the American CivilWar, soldiers had a three-fold greater likelihood ofdying from infection after a gunshot wound, thanbeing killed outright by the bullet.
In World War I, the battlefields were often heavilycontaminated with clostridium and evacuation fromthe field of battle was often delayed for days.Because of the advent of sulphonamides and themuch more rapid evacuation of wounded, World WarII saw a dramatic decrease in such infections.5 Thisdownward trend has continued through the KoreanWar, Vietnam and into current conflicts.
In general, high-risk gunshot wounds are treatedwith debridement, with tetanus antitoxin, andtriple antibiotic therapy (first generation cephalos-porin, aminoglycoside and penicillin). Alternatively,some centres are using piperacilin/tazobactam as asingle drug therapy. There is no literature to supportthis, though the spectrum of activity of this combi-nation seems to fit the microbiology of civiliangunshot wounds. Prophylactic therapy should becontinued in high-risk injuries for 72 h after woundclosure. Shotgun injuries should be treated the sameas high-energy wounds.
For low-risk gunshot wounds, such as thosecaused by civilian handguns, numerous studies sup-port the use of any of several regimens. Geissler13
reported that a single dose of cefonicid given in theEmergency Department was as effective as a 48 hcourse of intravenous antibiotics. Dickey10 reporteda prospective study of 96 patients, who were trea-ted with either no antibiotics or with 24 h of a first-generation cephalosporin. In this study, there wasno difference in infection rates. Ordog,29 in a mas-sive retrospective review of nearly 3400 patients,found that the use of antibiotics did not influenceinfection rates. Most other studies demonstrate

Current orthopaedic treatment of ballistic injuries 385
similar findings.11,30,34,39 Despite the lack ofcompelling evidence that antibiotics make a differ-ence in low-energy gunshot wounds, many surgeonsfeel uncomfortable not using them. The authors’approach is to use them sparingly, and only forwounds that are at risk.
Discussion
Gunshot wounds are becoming increasingly commonin Europe and in Asia. As political changes occuracross Europe, Africa and Asia, increasing numbersof high-energy gunshot wounds are anticipated.Orthopaedic surgeons are now more likely to seegunshot wounds as a part of their practice. A funda-mental knowledge of ballistics and woundingmechanisms is essential in treating these wounds.
Contrary to traditional teaching, a simplistic viewof gunshot wounds, based on either bullet velocity,or on energy transfer, may lead to mistakes inmanagement. The surgeon must learn to assessthe pattern of injury as a whole, and only thencome to a decision about how aggressively to treata particular wound. Infection, vascular injury andnerve injury are common and may ultimately be thedeterminants of the outcome, rather than the frac-ture alone.
Conflict of interest statementThere are no conflicts of interest to be disclosed
by any of the authors of this work.
References
1. Albrecht RJ, Parra JR. Traumatic peroneal artery pseudoa-neurysm: use of preoperative coil embolization. J Vasc Surg2004;39(4):912.
2. Bartlett CS. Clinical update: gunshot wound ballistics. ClinOrthop 2003;408:28—57.
3. Bartlett CS, Helfet DL, Hausman MR, Strauss E. Ballistics andgunshot wounds: effects on musculoskeletal tissues. J AmAcad Orthop Surg 2000;8(1):21—36.
4. Bono CM, Heary RF. Gunshot wounds to the spine. Spine J2004;4(2):230—40.
5. Buescher TM, CioffiWG Jr., Johnson AJ, et al. In: Zajtchuk R,editor. Textbook of Military Medicine: Series on CombatCasualty Care, Vol. 5. Washington: Office of the SurgeonGeneral at TMM Publications; 1998.
6. Chan KT, Korivi N. Lumbar artery pseudoaneurysm in trau-matic spinal cord injury: a case report. Arch Phys Med Rehabil2003;84(3):455—7.
7. Christy JP. Complications of combat casualties with combinedinjuries of bone and bowel: personal experience with nine-teen patients. Surgery 1972;71(2):270—4.
8. Clasper J. The interaction of projectiles with tissues and themanagement of ballistic fractures. JR Army Med Corps2001;147(1):52—61.
9. Cornwell III EE. Current concepts of gunshot wound treat-ment: a trauma surgeon’s prospective. Clin Orthop 2003;408:58—64.
10. Dickey RL, Barnes BC, Kearns RJ, Tullos HS. Efficacy ofantibiotics in low-velocity gunshot fractures. J OrthopTrauma 1989;3(1):6—10.
11. Dickson K, Watson TS, Haddad C, et al. Outpatient manage-ment of low-velocity gunshot-induced fractures. Orthopedics2001;10:951—4.
12. Dillman RO, Crumb CK, Lidsky MJ. Lead poisoning from agunshot wound. Report of a case and review of the literature.Am J Med 1979;66(3):509—14.
13. Geissler WB, Teasedall RD, Tomasin JD, Hughes JL. Manage-ment of low velocity gunshot-induced fractures. J OrthopTrauma 1990;4(1):39—41.
14. http://medlib.med.utah.edu/WebPath/FORHTML/FOR018.html.
15. http://medlib.med.utah.edu/WebPath/FORHTML/FOR038.html.
16. http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5002a1.htm.
17. http://www.ojp.usdoj.gov/bjs/abstract/fifc.htm.18. http://www.ojp.usdoj.gov/bjs/guns.htm.19. http://www-medlib.med.utah.edu/WebPath/TUTORIAL/
GUNS/GUNSTAT.html.20. Hull JB. Management of gunshot fractures of the extremities.
J Trauma 1996;40(Suppl 3):193—7.21. Islinger RB, Kuklo TR, McHale KA. A review of orthopedic
injuries in three recent U.S. military conflicts. Mil Med2000;165(6):463—5.
22. Kellermann AL, Reay DT. Protection or peril? An analysis offirearm-related deaths in the home N Engl J Med 1986;314(24):1557—60.
23. Krishnan DG, Marashi A, Malik A. Pseudoaneurysm of internalmaxillary artery secondary to gunshot wound managed byendovascular technique. J Oral Maxillofac Surg 2004;62(4):500—2.
24. Krug EG, Powell KE, Dahlberg LL. Firearm-related deaths inthe United States and 35 other high- and upper-middle-income countries. Int J Epidemiol 1998;27:214—21.
25. Lees RE, Scott GD, Mils CG. Subacute lead poisoning fromretained lead shot. CMAJ 1988;138(2):130—1.
26. Leonard MH. The solution of lead by synovial fluid. ClinOrthop 1969;64:255—61.
27. Long WT, Brien EW, Boucree Jr JB, et al. Management ofcivilian gunshot injuries to the hip. Orthop Clin North Am1995;26(1):123—31.
28. Omer Jr GE. Injuries to nerves of the upper extremity. J BoneJoint Surg Am 1974;56(8):1615—24.
29. Ordog GJ, Sheppard GF, Wasserberger JS, et al. Infection inminor gunshot wounds. J Trauma 1993;34(3):358—65.
30. Ordog GJ, Wasserberger J, Balasubramanium S, ShoemakerW. Civilian gunshot wounds–—outpatient management. JTrauma 1994;36(1):106—11.
31. Rhee JM, Martin R. The management of retained bullets inthe limbs. Injury 1997;28(Suppl 3):S-C23—8.
32. Romanick PC, Smith TK, Kopaniky DR, Oldfield D. Infectionabout the spine associated with low-velocity-missile injury tothe abdomen. J Bone Joint Surg Am 1985;67(8):1195—201.
33. Simpson BM, Grant RE. A synopsis of urban firearm ballistics:Washington, DC model. Clin Orthop 2003;408:12—6.
34. Simpson BM, Wilson RH, Grant RE. Antibiotic therapy ingunshot wound injuries. Clin Orthop 2003;408:82—5.
35. Thoresby FP, Darlow HM. The mechanisms of primary infec-tion of bullet wounds. Br J Surg 1967;54(5):359—61.
36. Thoresby FP, Watts JC. Gas gangrene of the high-velocitymissile wound. Br J Surg 1967;54(1):25—9.
386 D.A. Volgas et al.
37. Travis J, Director. National Institute of Justice ResearchPreview: Trends in Juvenile Violence in European Countries.May 1998.
38. Wolf AW, Benson DR, Shoji H, et al. Autosterilization in low-velocity bullets. J Trauma 1978;18(1):63.
39. Yang EC, Eisler J. Treatment of isolated type I open fractures:is emergent operative debridement necessary? Clin Orthop2003;410:289—94.
40. Yetkin U, Gurbuz A. Posttraumatic pseudoaneurysm of thebrachial artery and its surgical treatment. Tex Heart Inst J2003;30(4):293—7.
41. Yildiz C, Atesalp AS, Demiralp B, Gur E. High-velocity gunshopwounds of the tibial plafond managed with Ilizarov externalfixation: a report of 13 cases. J Orthop Trauma 2003;17(6):421—429.
Related Documents











