Day of Learning: Current Best Practices for Contraceptive Provision

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Day of Learning: Current Best Practices for Contraceptive Provision

Thank you to our Sponsors
• Carnegie Science Center• Jewish Healthcare Foundation• Allegheny Health Network’s Center for Inclusion Health• CWRHI• Adagio Health• Bayer• Merck• Cooper Surgical


Mission
To expand access to high quality reproductive health services and optimize
reproductive health outcomes for all individuals in Western Pennsylvania

Barriers to contraceptive access• Contraception coverage:
ACA/Obamacare Grandfathered plans Religious exemptions AHCA/Trumpcare
• Access: Medically accurate education/information Trained providers in accessible locations Faith-based organizations (1 in 6 hospitals in US) Federal sterilization consent Postpartum tubal ligation
• Reimbursement model: Postpartum LARC: global fee vs separate fee Placement at time of any visit Value-based care (provider incentives)

How RBC can help:• Educational workshops• Sharing resources• Creating networks for professional development• Mentorships• Industry Relationships (education, pharmaceutical)• Research• Legal Assistance

Disclosure of significant relationships with relevant commercial companies:
The speakers listed below have indicated that neither they, nor any member of their immediate family, have an actual or potential conflict of interest in relation to the content of this program: • Sonya Borrero, MD, MS• Eric Lantzman, MD
The speakers listed below have reported an actual or potential conflict of interest in relation to the content of this program:
Contraception 101
Eric Lantzman, MDCo-Director of Division of Family Planning
Allegheny Health Network

Outline
• How does contraception work?
• What are all the FDA approved options?
• What is LARC?
• Who is a candidate for contraception?

How does contraception work?
Progestin prevents ovulation
Progestin, condoms & diaphragm prevent spermfrom entering the cervix
Progestin and copper prevents
sperm from reaching egg
Sterilization closes the
fallopian tubes
Estrogen stops pituitary from
producing FSH/LH
• Placeholder for Eric’s slides
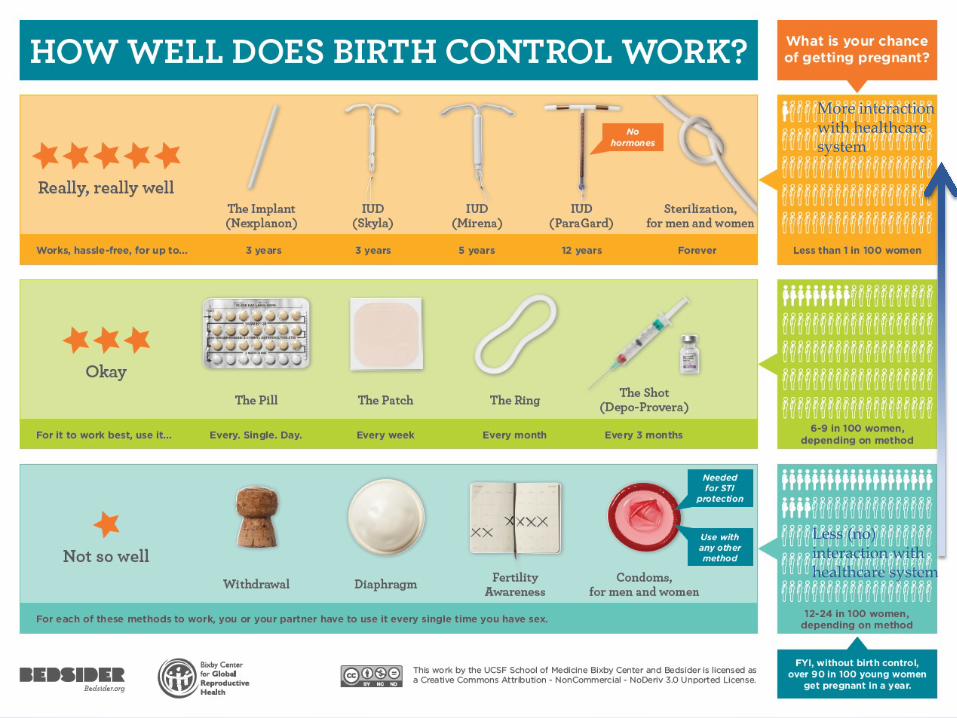
More interaction with healthcare system
Less (no) interaction with healthcare system

Why Options Matter…
Hyeon-Ju, 31
Anna, 27
Carlene, 31
Bridget, 25
• Has migraine w/aura, can’t use COC
• Important to have a regular period, doesn’t want LARC
• Uses withdrawal with long-term partner; accepts risk of pregnancy and would seek abortion if it occurs
• Lives in rural Texas
• Graduate student at Notre Dame University
• Uses condoms but is worried about failure rate, wants an IUD
• Student insurance won’t cover IUD – can’t afford $900 out of pocket
• Desires post-partum tubal ligation
• Told by 2 doctors that she should get an IUD instead
• Informed at final prenatal visit that she can’t schedule procedure due to Medicaid-specific, time-dependent consent requirements
• Long term OCP user• No pharmacy near home,
misses refills frequently due to work and childcare obligations
• Physician requires annual pelvic exam before refilling for next year

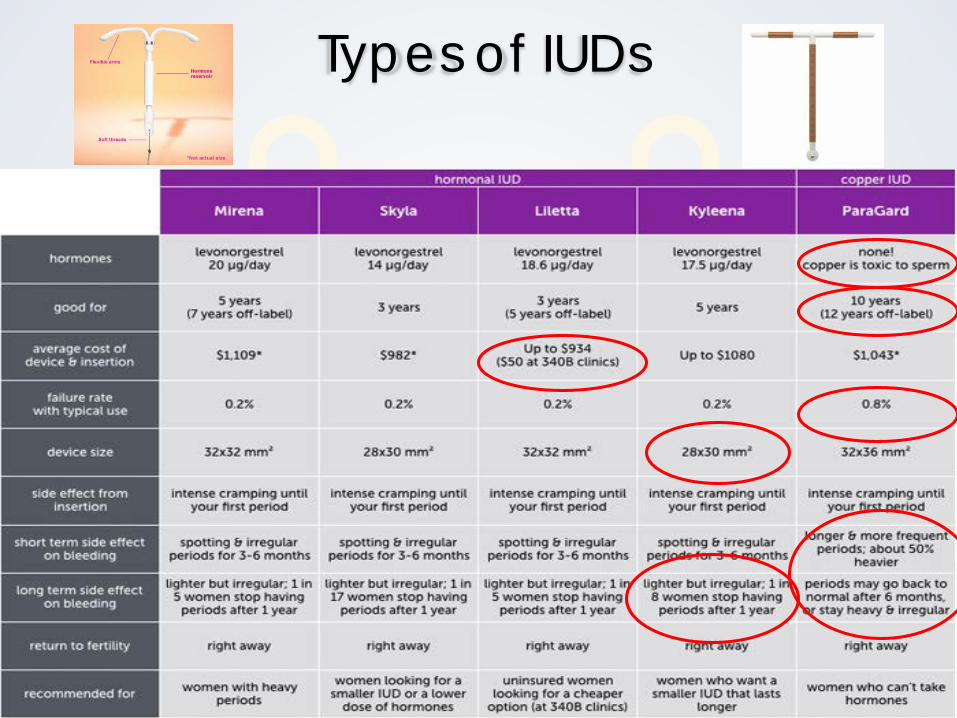
Types of IUDs

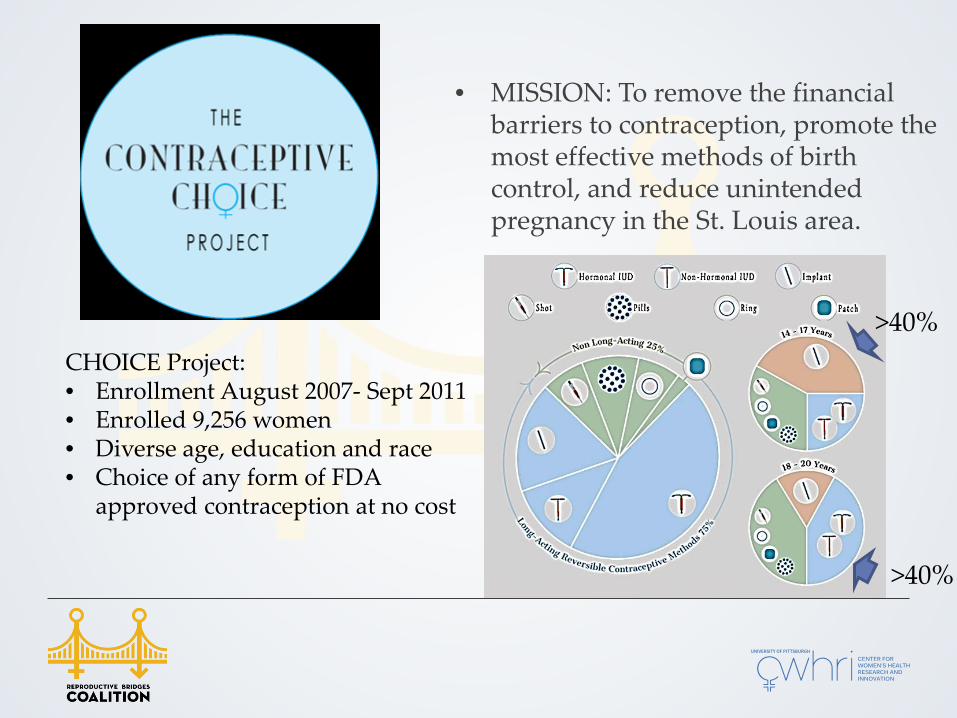
• MISSION: To remove the financial barriers to contraception, promote the most effective methods of birth control, and reduce unintended pregnancy in the St. Louis area.
CHOICE Project:• Enrollment August 2007- Sept 2011• Enrolled 9,256 women• Diverse age, education and race• Choice of any form of FDA
approved contraception at no cost
>40%
>40%

LARC is 10-20x more effective!!!
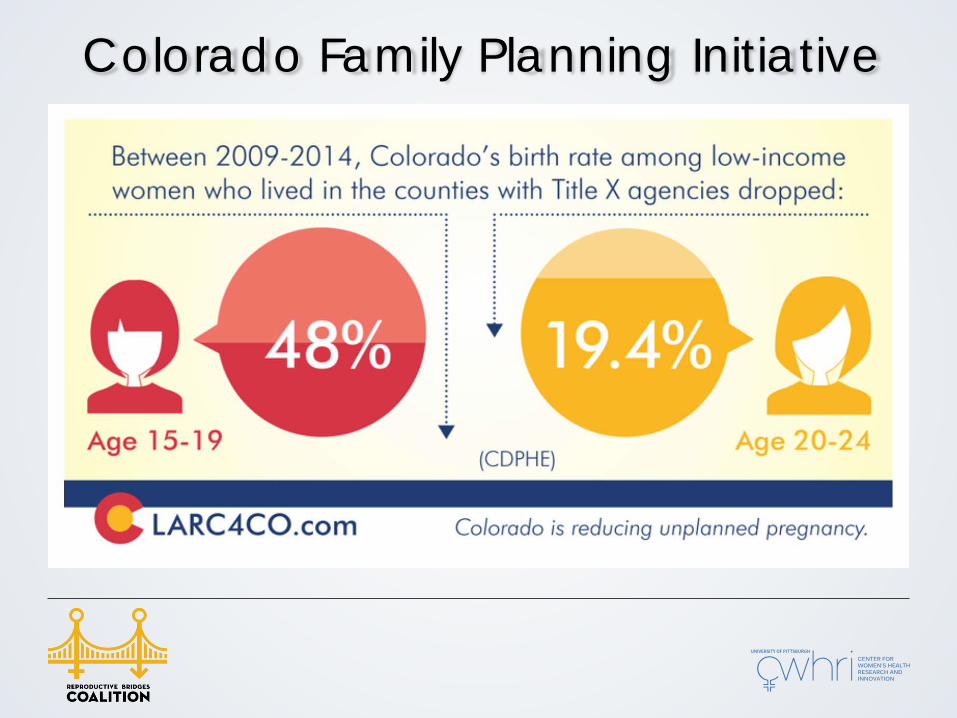
Colorado Family Planning Initiative
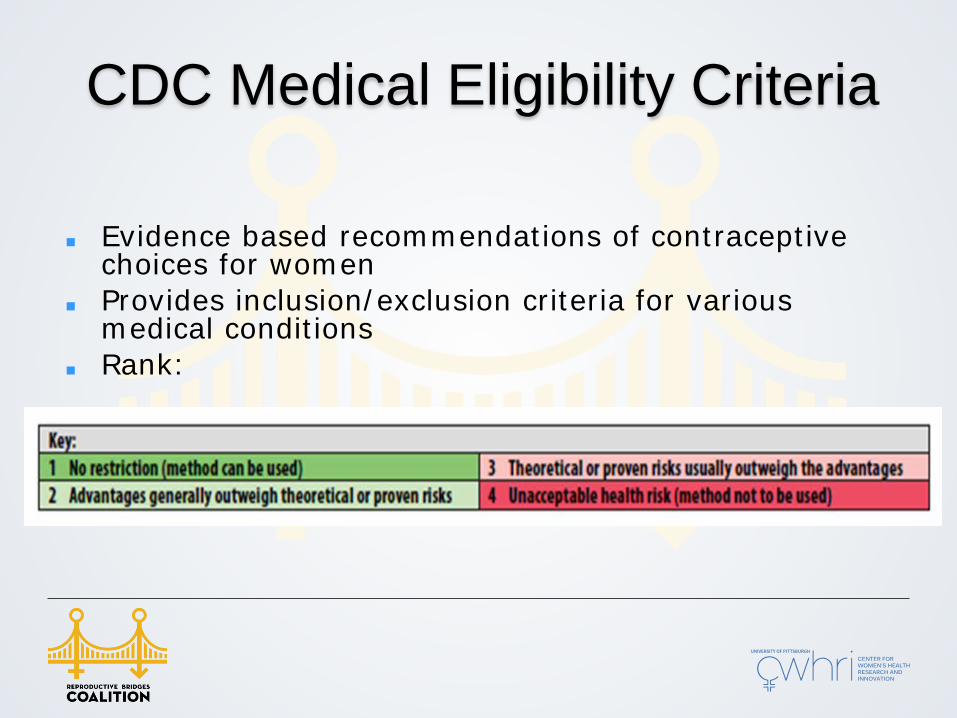
CDC Medical Eligibility Criteria
■ Evidence based recommendations of contraceptive choices for women
■ Provides inclusion/exclusion criteria for various medical conditions
■ Rank:
Medical Eligibility Criteria■ Includes:
• Combined hormonal contraception (CHC): pills,injectables, patch, ring
• Progestin only: pills (POP), injectables, implants• IUC: Cu-IUD, LNG-IUD• Barrier methods• Fertility awareness-based methods• Lactational amenorrhea method• Sterilization
■ Timing: • initiation (I)• continuation (C)

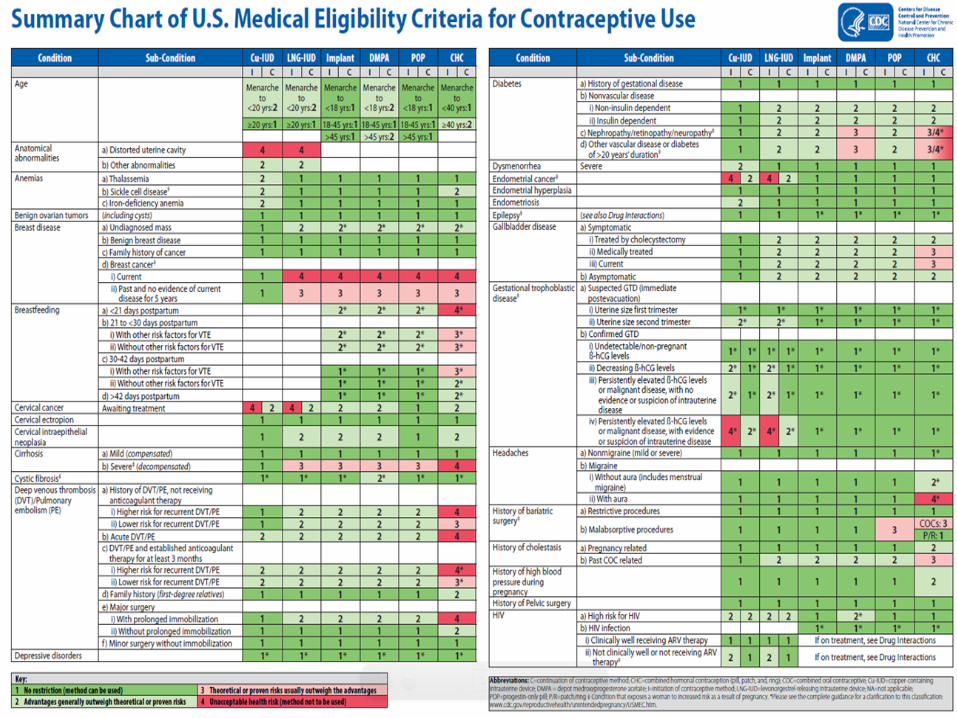
MEC Summary Chart
http://www.cdc.gov/reproductivehealth/UnintendedPregnancy/PDF/Legal_Summary%20Chart_English_Final_TAG508.pdf
MEC:


Thank You
• Any Questions???
• Take home items: Who: MEC What: Bedsider Chart When: Quickstart Algorithm
Related Documents











