CU-1 Iron Overload: Iron Overload: Complications and Need for Complications and Need for Therapy Therapy John B. Porter, MD Professor of Hematology University College, London, UK

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CU-1
Iron Overload: Complications and Iron Overload: Complications and Need for TherapyNeed for Therapy
John B. Porter, MDProfessor of HematologyUniversity College, London, UK

CU-2
Iron Distribution & Turnover In HumansIron Distribution & Turnover In Humans
Erythron 2g
Macrophages 0.6g
Transferrin 3mg 20-30 mg/day2-3mg/day
1-2 mg day
Gut
20-30mg/day
20-30 mg/day
Adapted with permission from Porter JB; Hematol/Oncol Clinics 2005; 19, 1-6. Andrews NC. N Engl J Med. 1999; 341:1986-1995.
Parenchyma0.3g
Liver1g

CU-3
Iron Loading From Blood TransfusionsIron Loading From Blood Transfusions
1 unit of blood contains approximately 200 mg of irona
– Normally, total body iron is approximately3 to 4 g
– Chronic transfusion-dependent patients have an iron excess of 0.3 to 0.7 mg/kg/day, equivalent to 4 to 10 g of iron per yearb
Iron accumulates with repeated blood transfusion
a Porter JB. Br J Haematol. 2001;115:239-252.b Andrews NC. N Engl J Med. 1999;341:1986-1995.

CU-4
Parenchyma
Hepatocytes
Hepatocytes
Parenchyma
Transfusional Iron OverloadTransfusional Iron Overload
Red
Erythron
Macrophages
Gut
Transfusion
20-40mg/day(0.3- 0.7 mg/kg/d)
NTBI
Transferrin
Adapted with permission from Porter JB; Hematol/Oncol Clinics 2005 19,1-6
CU-5
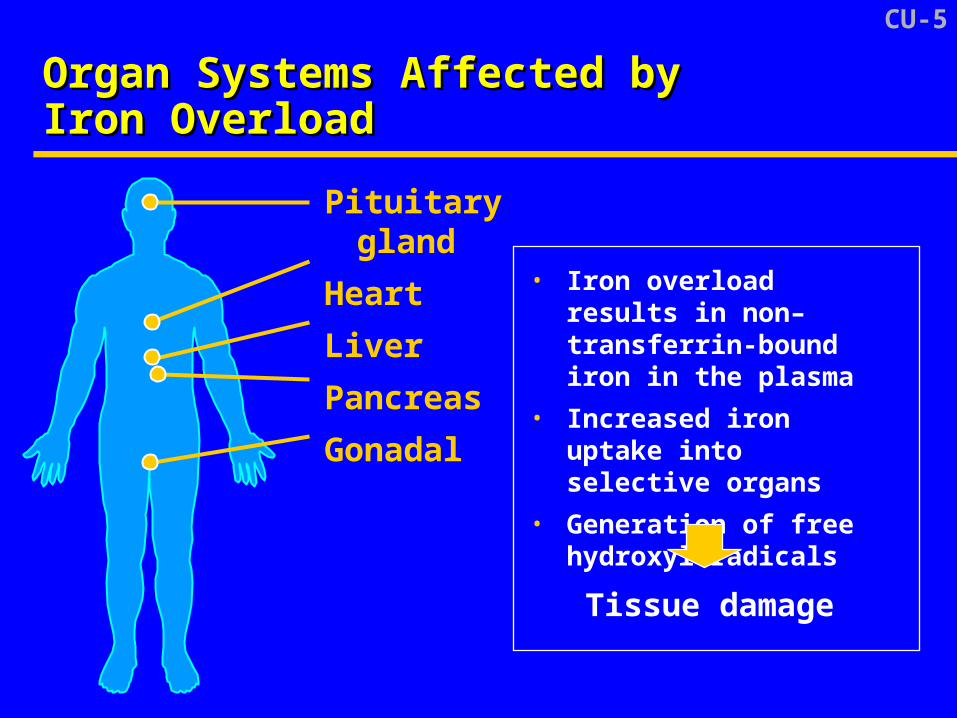
Organ Systems Affected byOrgan Systems Affected byIron OverloadIron Overload
Pituitary gland
Heart
Liver
Pancreas
Gonadal
• Iron overload results in non–transferrin-boundiron in the plasma
• Increased iron uptake into selective organs
• Generation of free hydroxyl radicals
Tissue damage

CU-6
Complications of Iron OverloadComplications of Iron Overload
Cardiomyopathy and cardiac failure
Hepatic cirrhosis
Diabetes mellitus
Impaired growth
Hypogonadism and infertility
Andrews NC. N Engl J Med. 1999;341:1986–1995

CU-7
Diseases Associated WithDiseases Associated WithTransfusional Iron OverloadTransfusional Iron Overload
β-thalassemiaOther chronic anemias
– Fanconi anemia (hypoplastic anemia)
– Diamond-Blackfan anemia (red cell aplasia)
– Congenital dyserythropoietic anemiasSickle cell anemiaAplastic anemiaMyelodysplastic syndromes (MDS)
Andrews NC. N Engl J Med. 1999;341:1986-1995.

CU-8
Initiation of Therapy for Iron OverloadInitiation of Therapy for Iron OverloadCurrent PracticeCurrent Practice
With repeated blood transfusions, iron rapidly accumulates in the body
– Chelation treatment is generally initiated after 10 to 20 transfusions or when serum ferritin > 1000 µg/L
– Alternatively, if iron loading is unclear, LIC may be measured
LIC = Liver iron concentration.Porter JB. Br J Haematol. 2001;115:239-252.

CU-9
Liver Iron Concentration Accurately Liver Iron Concentration Accurately Reflects Total Body Iron StoresReflects Total Body Iron Stores
Reprinted with permission from Angelucci E, et al. N Engl J Med. 2000;343:327-331.
Liver iron concentration (LIC), mg/g dry weight
To
tal
bo
dy
iro
n s
tore
s, m
g/k
g
0 5 10 15 20 25
300
250
200
150
100
50
0
r = 0.98
• Stores calculated by
quantitative phlebotomy
• LIC measured from
biopsy samples ≥ 1 mg
dry weight in 25 patients
Body iron (mg/kg) = 10.6 x LIC (mg/g dry wt)

CU-10
HH heterozygotes
50403020100
50
100
150
200
250
Age, years
Hep
atic
iro
n, µ
mo
l/g w
et w
eig
ht
50
40
30
20
10
0
Hep
atic
iro
n, m
g/g
dry
wei
gh
t
Threshold for cardiac disease and early death
Increased risk of complications
Normal
Olivieri & Brittenham, 1997 Blood. 89; 739-761.
Thalassemia major
Liver Iron and Risk of Complications From Liver Iron and Risk of Complications From Iron OverloadIron Overload
0

CU-11
Plasma Ferritin as a Plasma Ferritin as a Monitor of Iron LoadingMonitor of Iron Loading
Relatively non-invasive Inexpensive Obtained as
routine laboratory assay
Values confounded by
– Inflammation
– Liver function
0 4000 8000 12000
24,000
12,000
8000
4000
0
Hepatic iron, µg Fe/g liver *
Pla
sma
ferr
itin
, µ
g/L
Brittenham et al. Am J Hematol. 1993;42:81.
Sickle cell anemia (n = 37)
Thalassemia major (n = 74)

CU-12
Liver Iron Concentration and Serum Liver Iron Concentration and Serum FerritinFerritin
Change in serum ferritin over time reflects change in LIC
– Sequential evaluation of ferritin levels provides a good index of chelation historya
Maintenance of serum ferritin < 2500 µg/L significantly correlates with cardiacdisease-free survivalb,c,d,e
a Gabutti V and Piga A. Acta Haematol. 1996;95:26-36.b Olivieri NF, et al. N Engl J Med. 1994;331:574-578. c Telfer PT, et al. Br J Haematol. 2000;110:971-977.d Davis BA, et al. Blood. 2004;104:263-269.e Borgna-Pignatti C, et al. Haematologica. 2004;89:1187-1193.

CU-13
Cardiac Disease and % of Time WithCardiac Disease and % of Time WithSerum Ferritin > 2500 µg/LSerum Ferritin > 2500 µg/L
Olivieri, et al. N Engl J Med. 1994;331:574.
Assessments > 2500 µg/L
1.00
0.75
0.50
0.25
00 2 4 6 8 10 12 14 16
Years of chelation therapy
Pro
po
rtio
n w
ith
ou
tc
ard
iac
dis
ea
se
< 33%33% - 67%> 67%

CU-14
Ideal Properties of an Iron ChelatorIdeal Properties of an Iron Chelator
Control of body iron Prevention of iron mediated organ toxicity Simplicity and ease of administration Once daily oral administration Suitable for monotherapy Acceptable toxicity profile
– Iron free drug - dose relationship
– Iron complex - stable no redistribution of iron Simplicity and ease of monitoring

CU-15
Current Therapy for Iron OverloadCurrent Therapy for Iron Overload
Deferoxamine (Desferal®) is the only drug available in US to treat iron overload
Because of short half-life (20 minutes), must be given by continuous infusion
– 8 to 12 hours/day, 5 to 7 days/week
Compliance is poor because ofside effects and quality-of-life issues
Oral therapy is highly desirable
Porter JB and Huehns CR. Baillieres Clin Haematol. 1989;2:459-474.

CU-16
Compliance With Deferoxamine Infusions Compliance With Deferoxamine Infusions Is Related to Survival in ThalassemiaIs Related to Survival in Thalassemia
Kaplan-Meier analysis of survival in 257 consecutive thalassemic patientsaccording to the mean compliance with subcutaneous DFO therapy
Age, years
Su
rviv
al,
%
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
0 - 75
75 - 150
150 - 225
225 - 300
300 - 365
Gabutti V and Piga A. Acta Haematol. 1995;95:26-36.
Deferoxamineinfusions/year

CU-17
Summary of Medical NeedSummary of Medical Need
Transfusional therapy results in iron overload
Currently, the only approved therapy for iron overload in US is deferoxamine, which requires subcutaneous infusion for 8 to 12 hours, 5 to 7 times per week
– Compliance is an issue
– Many patients are not adequately treated
Treadwell MJ, et al. Pediatr Blood Cancer. 2005;44:500-507.Porter JB and Huehns CR. Baillieres Clin Haematol. 1989;2:459-474.
CU-18
Summary of Medical NeedSummary of Medical Need
Inadequately treated iron overload leads toorgan toxicity
– Related to lack of control of reactive iron, and deposition of iron in key tissues
– Developmental and endocrine dysfunction
– Cardiac dysfunction results in early death
Beutler E, et al. Hematology (Am Soc Hematol Educ Program). 2004:40-61.
Related Documents