Guide to Applicants for Grandparented Registration 祖祖祖祖祖祖祖祖 Binjiang Wu Ph.D/Prof/ Chief TCM Physician 吴吴吴 吴吴 / 吴吴 / 吴吴吴吴 President, Ontario College of Traditional Chinese Medicine 吴吴吴吴吴吴吴吴吴吴吴吴 Chief, WFAMS Professionals Accreditation Agency in Canada Standing Director, World Federation of Chinese Medicine Societies (WFCMS) 吴吴吴吴吴吴吴吴吴吴吴吴吴吴 Executive Member, the World Federation of Acupuncture & Moxibustion Societies (WFAS)(Non- Governmental Organization in Relation with WHO) 吴吴吴吴吴吴吴吴吴吴 吴吴吴吴吴吴吴吴吴吴吴吴吴吴 吴吴

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Guide to Applicants for Grandparented Registration祖辈注册申请指南
Binjiang Wu Ph.D/Prof/ Chief TCM Physician
吴滨江 博士 / 教授 / 主任医师
President, Ontario College of Traditional Chinese Medicine
加拿大安大略中医学院院長
Chief, WFAMS Professionals Accreditation Agency in Canada
Standing Director, World Federation of Chinese Medicine Societies (WFCMS)
世界中医药学会联合会常务理事
Executive Member, the World Federation of Acupuncture & Moxibustion Societies (WFAS)(Non-Governmental Organization in Relation with WHO)
世界针灸学会联合会(世界卫生组织非政府组织机构) 执委

2
Registration Requirements, Grandparented Class 祖辈类别注册要求
The requirements for registration are stipulated in Ontario Regulation 27/13, Registration, made under Traditional Chinese Medicine Act, 2006.
该注册要求依据 2006 年传统中医法下安省第 27/13 注册条例而订。
According to Section 6, subsection (1) of O.Reg. 27/13:
根据该条例第 6 章第( 1 )节规定:“6. (1) The following are non‐exemptible requirements for a Grandparented certificate of registration:
以下规定为祖辈类别注册不可豁免的要求:
1. The applicant must have completed a minimum of 2,000 traditional Chinese medicine patient visits in Canada, which may include traditional Chinese acupuncture patient visits, within the five‐year period immediately before this paragraph came into force.
申请人必须在此条款生效前的五年内在加拿大以中医药诊治至少有 2000 病人人次,其中可包括中医针灸诊治病人。
2. The applicant must have submitted the completed application to the Registrar on or before the first anniversary of the day this paragraph came into force.
申请人必须将填好的表格在此条款生效的一年之内送交注册处。
3. The applicant must have successfully completed the Safety Program that was set or approved by the Council or by a body that is approved by the Council for the purpose.
申请人必须要通过管理局设定或局方委托第三方设定的安全课程。
4. The applicant must have successfully completed the jurisprudence course set or approved by the Registration Committee.
申请人必须要通过由注册委员会设定或承认的法律考试。

(2) The requirements in paragraphs 3 and 4 of subsection (1) are not considered to have been met unless the applicant satisfies those requirements either within the three‐year period immediately before the date of that applicant’s application or at some point following the submission of his or her application but before the certificate of registration is issued.”
第( 1 )部分中的第 3 和第 4 段不应视为(在注册申请前)符合要求,除非申请人能在注册申请提交后的三年之内或在提交申请后但在会员注册证书颁发前通过(这两个考试)。
Other requirements common to all classes of registration, including Grandparented certificate of registration are stipulated in Section 4 of O. Reg. 27/13.
其他关于所有种类会员,包括祖辈法注册会员的要求,依据安省第 27/13 注册条例中第 4 节内容。
To access the Ontario Regulation 27/13, Registration, made under Traditional Chinese Medicine Act, 2006, please visit the following link on e‐laws: http://www.elaws.gov.on.ca/html/regs/english/elaws_regs_130027_e.htm
欲了解根据 2006 传统中医法内安省第 27/13 注册条例所规定的内容,请点击以下链接获得电子法律条款:http://www.elaws.gov.on.ca/html/regs/english/elaws_regs_130027_e.htm
APPLICATION PROCESS 申请步骤
Step 1第一步骤
Download the Grandparented Registration Application Form from the College website:www.ctcmpao.on.ca. OR Pick up a hard copy at our office.在管理局网站 www.ctcmpao.on.ca 下载祖辈法注册申请表。或到我们的办公地点领取。
Step 2第二步骤
Complete, Sign and Notarize your application (Incomplete information and/or missing signatures will cause delay.)填写完成、签名并公证申请(未完成信息及 / 或遗漏签名可能会耽误注册。)Read all instructions carefully before completing the form.在填写表格前仔细阅读所有说明。All sections must be completed. Print legibly. Illegible applications will be returned.须填写表格上的所有内容。清晰填写。疗程不清的申请将被退回。Check the title/designation you wish to apply. (See page 3 for details.)确定欲申请的头衔 / 名称。(参考第三页的详细说明。)Both you and your witness must sign the Validation Certificate to validate completion of 2,000 Patient visits within the past 5 years (on page 10 of the application form.)您和您的证人都需在验证证书上签字,以确认在过去的五年内完成了 2000 人次就诊。(见申请表格第 10页)Sign the completed form before a Commissioner of Oaths, Notary Public or lawyer.在监誓官,公证人或律师面前在完成的表格上签字。
Step 3第三步骤
Prepare and attach all documents listed below to your application (Missing documents will cause delays.)
准备并在申请表后附上以下列出的所有文件(遗失文件可能会耽误注册。) Evidence of your identity – Note: The name used in your practice and the name on
your College Register must be the same. The College requires evidence of your identity. If the name on your documents is different from your current name, you must provide proof of your name change. Evidence of name change documents include: birth certificate, marriage certificate, divorce decree, passport, or validation of identity signed by legal counsel.
身份证明 --- 注:用作执业的姓名必须要与在管理局注册的姓名一致。管理局需要申请者身份的证明。如果文件上的姓名与现使用姓名不同,您需要提供更改姓名的证明。更改姓名证据包括:出生证明,结婚证明,离婚判决书,护照,或由律师签署的身份有效证明。
A passport‐size photo taken within the last 12 months;1 张护照尺寸的照片,照片需为过去 12 个月之内的; The letter issued by the Registrar confirming your completion of the Jurisprudence
Course (test);由注册主任颁发的通过法律课程(考试)的确认函; The letter issued by the Registrar confirming your completion of the Safety Program
(test);由注册主任颁发的通过安全课程(考试)的确认函; Your written language plan (if you took the Jurisprudence test with interpretation; or
if you declared in the application that you are unable to speak, read, and write with reasonable fluency in English or French);
语言计划(如果参加法律考试时申请了翻译;或如果在申请中声明了您无法足够流利地使用英语或法语交流、阅读和书写);
Professional liability insurance certificate (if not available, submit within 30 days after registration has been approved.);
专业责任保险证明(如果当时没有,则需要在注册通过后的 30天内提交。); Criminal background check. For registration purposes, the College only requires a
name‐based criminal check.犯罪调查记录。根据注册目的,管理局仅需以姓名为基础的犯罪调查记录。
8
Step 4第 4 步骤
Submit TWO SEPARATE Certified Cheques or Money Orders payable to “CTCMPAO” for
提交两张银行保付支票或现金支票收款人为“ CTCMPAO” 分别给:1. Application fee (non‐refundable) for $169.50 ($150 application fee + $19.50 HST);
AND申请费(不可退) $169.50 ( 申请费 $150 +税 $19.50 ); 和1. 2013‐14 Registration fee for $960.50 ($850.00 registration fee + $110.50 HST).2013-14 年注册费 $960.50 ( 注册费 $850.00 +税 $110.50).1. The Registration fee will be returned if the application is not successful.如果申请未通过,该注册费将被退回。
Step 5第 5 步骤
Photocopy your application form and all attachments for your own record. Use the check list of information/documents to ensure that you have provided all information and required documents.复印您的申请表和所有提交附件自己留作备案。使用信息 / 文件清单以确保提供了所有的信息和要求的文件。
Step 6第 6 步骤
Mail or deliver your application package to:邮寄或递送申请包至以下地址:RegistrarCollege of Traditional Chinese Medicine Practitioners andAcupuncturists of Ontario163 Queen Street East, 4/FToronto, Ontario M5A 1S1Your application will be processed according to the time your application package arrives at the office. It will be processed within 3‐6 weeks. Incomplete information, missing supporting documents, fees, or signatures will cause delay.申请处理将依据申请包到达注册办公室的时间顺序。申请将会在 3-6周内处理。不完整的信息、遗漏的说明文件、费用或签名将会耽误注册完成时间。
9
TITLE/DESIGNATION TO APPLY 申请头衔 /名称
An applicant may wish to apply for one or both of the titles/designations described below. The College shall make the final decision on the title and designation to be awarded to an applicant depending on the experience and the documents he or she provides to support the application.
申请者可能想申请以下描述的一个或两个头衔 / 名称。管理局将根据申请人的经验和提供的文件来最终决定为申请者授予的头衔。
An applicant for the title “Traditional Chinese Medicine Practitioner” and designation “R.TCMP” is expected to:
申请”传统中医师”职称和”注册中医师”名称的申请者需:
have experience in TCM diagnosing and have provided treatments using TCM herbal and acupuncture therapies as evidenced in his or her 2,000 patient visits within the 5 years in Canada prior to application for registration; and
具备中医诊断的经验并具备使用中药和针灸技术治疗病人的经验,这些经验在申请人过去 5 年内在加拿大的2000 人次就诊中(体现);及
Have successfully completed the Safety Program test for TCM Practitioner.
通过了中医师的安全课程考试。
An applicant for the title “Acupuncturist” and designation “R.Ac” is expected to:
申请“针灸师”头衔和“注册针灸师”名称的申请者需:
have experience in TCM diagnosing and have provided treatments using acupuncture therapies only as evidenced in his or her 2,000 patient visits within the 5 years in Canada prior to application for registration; and
具备中医诊断的经验并具备仅使用针灸技术治疗病人的经验,这些经验在申请人过去 5 年内在加拿大的 2000 人次就诊中(体现);及
have successfully completed the Safety Program test for Acupuncturist.
通过了针灸师的安全课程考试。
Instructions 填写指南
1. ALL applicants must complete this form and submit TWO SEPARATE certified cheques or money orders made payable to “CTCMPAO”
所有申请者需填写完整该表格并提交两张银行保付支票或现金支票,收款人为“ CTCMPAO” 分别给:
One for the non‐refundable application fee for $169.50 ($150.00 application fee + $19.50 HST) and
其一为不可退款申请费 $169.50 ($150.00 申请费 + $19.50 税 ) ,以及Another for the 2013‐14 registration fee for $960.50 ($850.00 registration fee + $110.50 HST).
另一为 2013-14 年注册费 $960.50 ($850.00 注册费 + $110.50 税 ).
The registration fee will be returned if the application is not successful.
如果申请未通过,该注册费将被退回。
2. To avoid delay in processing of your application, ensure that you:
为了防止耽误申请过程,请您确保:
complete all sections of the form that apply to you
请完整填写申请表中所有适用于您的部分 attach the required documents
附上所有需要的文件 sign the application form
在申请表格上签名 attach your certified cheque /money order for payment to the College
附上您付给管理局的银行本票或现金支票
3. If the College does not receive a completed application form with all required documents and certified cheques/money orders, the application form will not be processed.
如果管理局未收到完整的表格及所有所需文件和银行本票或现金支票,该申请表格将不会被处理。
4. Print your information on the application form legibly. Illegible forms will be returned.
清晰填写表格。填写不清晰的表格将会被退回。
5. Send or deliver your completed application form to:
邮寄或提交完整的申请至以下地址:
Registrar
CTCMPAO
163 Queen Street East, 4th Floor
Toronto, Ontario M5A 1S1
1. TITLE/DESGINATION 头衔 / 名称
An applicant may apply for one or both of the titles/designations described below. The Traditional Chinese Medicine Practitioner (R.TCMP) title denotes that an applicant can use both Traditional Chinese Medicine Practitioner and Acupuncturist titles and designations. The Acupuncturist (R. Ac) title denotes that an applicant can only use the Acupuncturist title and designation.申请者可以申请以下描述的一个或两个头衔 / 名称。注册中医师头衔表示申请者可以用中医师和针灸师的头衔和名称。注册针灸师表示申请者仅能使用针灸师的头衔和名称。 Check the box(es) applicable to you 在使用您的选项方框内打√I am applying for Grandparented Registration to use the title/designation(s):我申请注册祖辈法会员的头衔 / 名称为: Traditional Chinese Medicine Practitioner (R. TCMP) Acupuncturist (R. Ac) 中医师(注册中医师) 针灸师(注册针灸师)
The College shall decide on the title and designation to be awarded to an applicant depending on the experience and the documents he or she provides to support the application. (Refer to the Guide to Applicants for more information).管理局将根据申请人的经验和提供的文件来最终决定为申请者授予的头衔。(请参考申请人指南中有关的详细说明)

2. PERSONAL INFORMATION 个人信息 Mr. Ms.Legal First Name 法律名
Legal Last Name 法律姓 Legal Middle Name (if any)法律中间名(如果有)
Previous First Name 曾用名(if different from legal name)(如果与法律名不同 )
Previous Last Name 曾用姓(if different from legal name)(如果与法律名不同 )
Previous Middle Name 曾 用 中间名(if different from legal name)(如果与法律名不同 )
Commonly Used First Name 常用名(if different from legal name)(如果与法律名不同 )
Commonly Used Last Name 常用姓(if different from legal name)(如果与法律名不同 )
Commonly Used Middle Name常用中间名(if different from legal name)(如果与法律名不同 )
If more than one name is provided above, or if the name on any of your documents is different from your current name you must provide proof of name change. (See Guide to Applicants – Step 3).如果在以上提供了多于一个姓名,或您任何文件上的姓名与现使用姓名不同,您需提供姓名更改证明(请参考申请指南 -第 3 步骤)。The College requires evidence of your identity. If the name on any of your documents is different from your current name, you must provide proof of your name change. Examples of name change documents: birth certificate, marriage certificate, divorce decree, passport or validation of identity signed by legal counsel.管理局需要您身份的证明。如果您的任何文件上的姓名与现有姓名不同,您必须要提供姓名更改的证明。姓名更改证明文件如:出生证明,结婚证明,离婚判决书,护照或由律师签署的身份有效证明。 Document attached OR Signature (签名) ______________________________________________ 附文件或 A Commissioner of Oaths, Notary Public, Lawyer 监誓官,公证人,律师 (Official seal/stamp or business card must be provided)( 需附官方
印章或名片 )Preferred name to be used on Certificate of Registration and on College Register选择在管理局及注册证书上的名字 Legal Name (法律)名 Commonly Used Name 常用名 Both 两个都用The name that you choose to be put on the Certificate of Registration and on the College Register must be the name that you use in your practice. 选择在管理局及注册证书上的名字必须要与治疗中用的姓名一致。 Date of Birth (mm/dd/yyyy) 生日(月月 / 日日 / 年年年年) / / / Gender 性别 Male男 Female女
This information is necessary to verify identity for registration purposes with the College. 必须填写该表格以在管理注册中确认身份。
3 . CONTACT INFORMATION 联系方式Home Address – Street No. & Name 家庭住址 – 街号及街名
Apt/Suite No. 公寓号
City/Town城市
Province 省份 Postal Code邮政编码 Country国家
Email邮件
Tel 电话 Fax 传真
Primary Business Address ‐ Street No. & Name 办公地址 1 – 街号及街名
Apt/Suite No. 公寓号
City/Town 城市
Province 省份 Postal Code 邮政编码 Country 国家
Email 邮件
Tel. 电话 Fax 传真
Secondary Business Address ‐ Street No. & Name 办公地址 2 – 街号及街名
Apt/Suite No. 公寓号
City/Town城市
Province 省份 Postal Code邮政编码 Country国家
Email邮件
Tel 电话 Fax 传真
Choose one address for your mailing address Home Primary Business Secondary Business选择您的邮递地址 家庭住址 办公地址 1 办公地址 2 Note that your business address information is available to the public. If you provide your home address as yourbusiness address, it will be available to the public.请注意: 您的公司地址将向公众提供,如果您的家庭地址作为您的办公场所,那么此家庭地址也将向公众提供。
17
4 . PHOTO 照片
One photograph must be full faced, of passport size and quality, taken within 12months of submitting the application.一张免冠照片,护照照片的大小和质量,近 12 个月内拍摄。 My photograph attached here was taken on 所附的照片是以下日期拍摄的 : ______/_____/___________/ _________________________ (mm月 / dd日 / yyyy年 ) Signature 签字
Paste a passport-sizePhoto here
护照大小的照片
请贴于此处Photo ID is required for registration verification and wallet‐sized Photo ID purposes. Be advised that when you resign as a member of the College your photo will be destroyed unless the photo is required for regulatory purposes. For more information, refer to the Registration Policies on “Photo Destruction” available on our website at www.ctcmpao.on.ca.带有照片的身份证是注册时用于证明身份及方便放入钱包随身携带的目的。请注意,当你从管理局注销后,您的照片将被销毁,除非照片时处于监管目的。有关的详细内容,请登陆官方网站 www.ctcmpao.on.ca. ,参阅注册政策“照片的销毁”一栏。
5 . COMPLETION OF JURISPRUDENCE COURSE (TEST) 完成法律课程
Check the box(es) applicable to you. 请在适用于您的 里√ 打勾。 Yes, I have successfully completed the College Jurisprudence Course (test). 是的,我已经成功完成了管理局的法律课程(测试)。 Date completed 完成日期 ______/_____/___________/ Language of Test 考试语言 __________________ (mm月 / dd日 / yyyy年 ) (please specify 请具体 ) If yes, attach a copy of the letter confirming the completion of the College Jurisprudence Course (test). 如果是,请附上的完成管理局法律课程(测试)证明信的复印件。 No, I will be taking the College Jurisprudence Course (test) on ______/_____/___________/ 没有,我将会在以下日期去考参加法律课程(测试) (mm月 / dd日 / yyyy年 ) Note that the College Jurisprudence Course is to be completed either within the 3‐year period immediately before the date of this application or at some point following the submission of this application, but before the certificate of registration is issued. Jurisprudence Course (test) results are valid for only 3 years after the date on your confirmation letter issued by the College.需要注意:管理局的法律课程必须在 3 年内递交注册申请表,或者在提交申请表格后及颁发注册证书前完成。法律课程(测试)的结果自管理局的证明信日期开始计算,有效期为 3 年。
6 . COMPLETE OF SAFETY PROGRAM (TEST) 完全安全课程
Check the box(es) applicable to you. 请在适用于您的 里√ 打勾。 Yes, I have successfully completed the College Safety Program to pursue R.TCMP designation on ___/_____/_____/ (mm月 / dd日 / yyyy年 ) 是的,我已经成功完成了管理局的中医师的安全课程 Yes, I have successfully completed the College Safety Program to pursue R.Ac designation on ___/_____/_____/ 是的,我已经成功完成了管理局的针灸师的安全课程 (mm月 / dd日 / yyyy年 ) If yes, attach a copy of the letter confirming the completion of the College Safety Program (test). 如果是,请附上完成管理局安全课程证明信的复印件。 No, I will be taking the College Safety Program (test) on ______/_____/___________/ 没有,我将会在以下日期去参加安全课程(测试) (mm月 / dd日 / yyyy年 ) Note that the College Safety Program is to be completed either within the 3‐year period immediately before the date of this application or at some point following the submission of this application, but before the certificate of registration is issued. Safety Program (test) results are valid for only 3 years after the date on your confirmation letter issued by the College.需要注意:管理局的安全课程必须在 3 年内递交注册申请表,或者在提交申请表格后及颁发注册证书前完成。安全课程(测试)的结果自管理局的证明信日期开始计算,有效期为 3 年。

7 . LANGUAGE FLUENCY 语言能力Check the box(es) applicable to you. 在适用的选项内打√a) Are you able to speak, read, and write with reasonable fluency in English
so that you can offer professional services to patients in that language? 您是否可以流利地用英文交流、阅读及书写,足以为病人用英文提供专业服务?
Yes是
No否
b) Are you able to speak, read and write with reasonable fluency in French so that you can offer professional services to patients in that language? 您是否可以流利地用法文交流、阅读及书写,足以为病人用法文提供专业服务?
Yes是 No否
c) Additional languages in which you can personally and competently provide professional services. (Provide up to 5 as applicable.)其他您可以使用的语言进行个人和全面的专业服务。(至多提供 5 种) 1. _____________________ 2. ____________________ 3.________________________ 4. _____________________ 5. ____________________
If you have indicated that you are unable to speak, read, and write with reasonable fluency in either English or Frenchto offer professional services to patients, submit a written plan demonstrating how you will effectively communicatewith patients and the health care system either in English or French. For more information, refer to the RegistrationPolicies on “Written Language Plan” available on our website at www.ctcmpao.on.ca. 如果您填写的是不能流利地用英文或法文进行交流、阅读及书写,无法为病人用英文或法文提供专业服务,请提交一份语言计划,说明如何与病人和卫生系统其他人员使用英语或法语进行有效的沟通。有关此方面的更多信息,请参考官方网站了解“书写语言计划”内容: www.ctcmpao.on.ca.
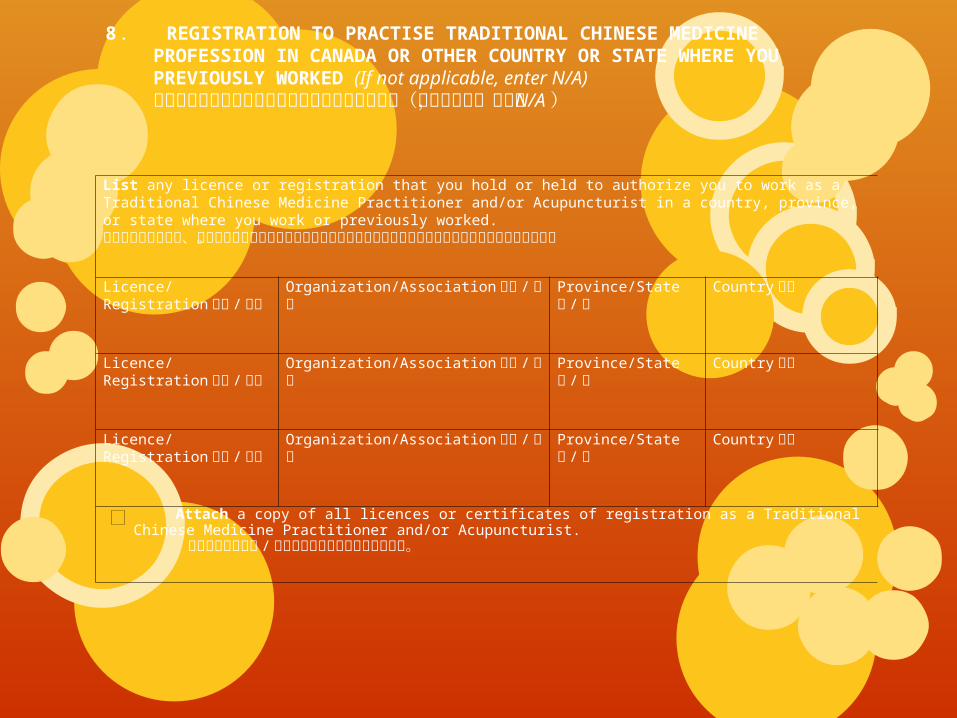
8 . REGISTRATION TO PRACTISE TRADITIONAL CHINESE MEDICINE PROFESSION IN CANADA OR OTHER COUNTRY OR STATE WHERE YOU PREVIOUSLY WORKED (If not applicable, enter N/A)过去在加拿大或其他国家或州进行中医治疗的经验(如果不适用,请填写 N/A)
List any licence or registration that you hold or held to authorize you to work as a Traditional Chinese Medicine Practitioner and/or Acupuncturist in a country, province, or state where you work or previously worked.请列出您在任何国家、省或州工作或曾经工作过的地方持有或过去持有的全部经授权的中医师或针灸师执照或注册。
Licence/Registration执照 / 注册
Organization/Association 组织 /协会
Province/State省 /州
Country国家
Licence/Registration执照 / 注册
Organization/Association 组织 /协会
Province/State省 /州
Country国家
Licence/Registration执照 / 注册
Organization/Association 组织 /协会
Province/State省 /州
Country国家
Attach a copy of all licences or certificates of registration as a Traditional Chinese Medicine Practitioner and/or Acupuncturist.
附上所有中医师和 / 或针灸师执照或注册证书的复印件。

22
9 .MEMBERSHIP WITH PROFESSIONAL ASSOCIATION OF TRADITIONAL CHINESE MEDICINE AND ACUPUNCTURE (If not applicable, enter N/A)中医和针灸专业协会会员(如果不适用,请填写 N/A )
Organization Name ‐ 1 协会名称 -1 Certification /identifier # ______________________ from ______/_____/_______/ to ______/_____/_______/ 证书 / 会员号 (mm月 / dd日 /yyyy年 ) (mm月 / dd日 /yyyy年 ) Organization Address ‐ Street No. & Name 协会地址 1 – 街号及街名
Apt/Suite No. 公寓号
City/Town 城市
Province 省份 Postal Code 邮政编码 Country 国家
Email 邮件
Tel. 电话 Fax 传真
Official position(s) held (specify title and duration, if applicable) ______/_______/_______/官方职位(如果适用,请明确头衔和期限) (mm月 / dd日 /yyyy年 ) Organization Name ‐ 2协会名称 -2 Certification /identifier # ______________________ from ______/_____/_______/ to ______/_____/_______/ 证书 / 会员号 (mm月 / dd日 /yyyy年 ) (mm月 / dd日 /yyyy年 ) Organization Address ‐ Street No. & Name 协会地址 1 – 街号及街名
Apt/Suite No. 公寓号
City/Town 城市
Province 省份 Postal Code 邮政编码 Country 国家
Email 邮件
Tel. 电话 Fax 传真
Official position(s) held (specify title and duration, if applicable) ______/_______/_______/官方职位(如果适用,请明确头衔和期限) (mm月 / dd日 /yyyy年 )

23
10. WORK HISTORY/PRACTICE EXPERIENCE AS A TRADITIONAL CHINESE MEDICINE PRACTITIONER AND/OR ACUPUNCTURIST IN CANADA过去在加拿大作为中医师和 / 或针灸师工作经验 / 治疗经验
You must provide evidence that within the last 5 years you have practiced the profession as a Traditional ChineseMedicine Practitioner and/or Acupuncturist.您必须提供在过去 5 年内作为中医师和 / 或针灸师的证据。You are required to provide your work history as a Traditional Chinese Medicine Practitioner and/or Acupuncturist within the last 5 years in Canada, from ______ /_____ /______ / to _____/______ /_____ /您需提供过去 5 年在加拿大作为中医师和 / 或针灸师的工作记录, 从 __/___/___到 __/___/___ (日期)。Practice Experience in Canada 在加拿大的从医经验 Employer or Facility
Address雇主或单位地址
Employer/Facility PhoneNumber 雇主或单位电话
Start Date ofEmployment(mm/dd/yyyy) 工作开始日期(月 /日 / 年)
End Date ofEmployment(mm/dd/yyyy) 工作截止日期(月 /日 / 年)
Employer or Facility Name 工作单位
_____/______ /____ / _____/______ /____ / (xxx)xxx—xxx
_____/______ /____ / _____/______ /____ / (xxx)xxx—xxx
_____/______ /____ / _____/______ /____ / (xxx)xxx—xxx
_____/______ /____ / _____/______ /____ / (xxx)xxx—xxx
_____/______ /____ / _____/______ /____ / (xxx)xxx—xxx
If necessary, attach additional pages to describe your work history/practice experience.如果需要,可再附上额外页说明工作历史 / 治疗经验。 You will be required to provide evidence of having completed a minimum of 2,000 traditional Chinese medicine patient visits in Canada within the last 5 years. You must complete the Validation Certificate on the following pages with respect to the 2,000 traditional Chinese medicine patient visits, listing all of the traditional Chinese medicine diagnoses and treatments that you have performed as a Traditional Chinese Medicine Practitioner and/or Acupuncturist in Canada within the past 5 years.您需要提供过去 5 年内在加拿大完成了至少 2, 000 次中医病人就诊记录。您必须要完成后面几页有关 2,000 次中医就诊记录的确认记录,罗列过去五年在加拿大作为中医师和 / 或针灸师进行过的所有中医诊断和治疗。 You must sign the Validation Certificate of traditional Chinese medicine patient visits to state that the information is true.您必须要在中医病人就诊记录的确认上签字,以证明所列信息为真实的。
24
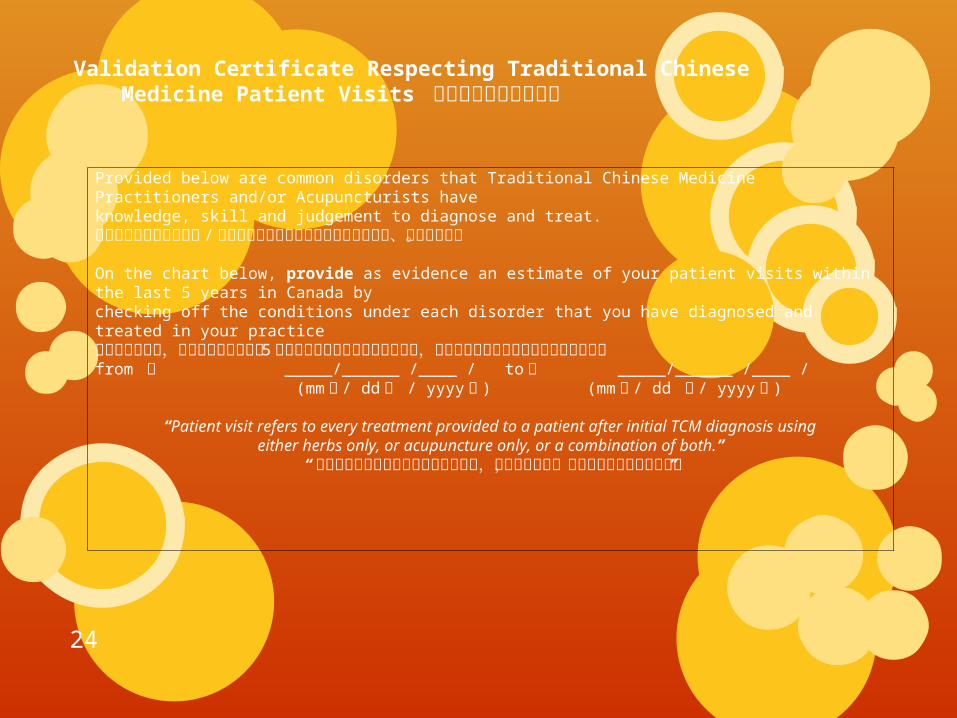
Validation Certificate Respecting Traditional Chinese Medicine Patient Visits 中医病人就诊记录确认
Provided below are common disorders that Traditional Chinese Medicine Practitioners and/or Acupuncturists haveknowledge, skill and judgement to diagnose and treat.以下常见疾病为中医师和 / 或针灸师在诊断和治疗中所需具备的知识、技巧和判断。 On the chart below, provide as evidence an estimate of your patient visits within the last 5 years in Canada bychecking off the conditions under each disorder that you have diagnosed and treated in your practice在以下的表格里,请大致评估您过去的 5 年内在加拿大治疗的病人就诊次数,请在每项疾病后填写您诊断和治疗的情况from 自 _____/______ /____ / to 至 _____/______ /____ / (mm月 / dd日 / yyyy年 ) (mm月 / dd 日 / yyyy年 )
“Patient visit refers to every treatment provided to a patient after initial TCM diagnosis usingeither herbs only, or acupuncture only, or a combination of both.”
“病人就诊指的是在出诊后或仅适用草药,或仅使用针灸,或两者并用为病人提供治疗”

25
Disorders疾病
TCMDiagnosis 中医诊断 Estimated Number
of Patient Visits forTCM HERBALMEDICINE ONLY仅用草药治疗中医病人就诊次数的大致数字
Estimated No. of patient Visits for ACUPUNCTURE ONLY (Including Tuina, Cupping & Moxibusti on, etc.)仅用针灸(包括推拿,拔罐和艾灸等)治疗中医病人就诊次数的大致数字
Estimated No. ofPatient Visits forpatients whoreceived BOTH TCMHerbal Medicineand Acupuncture使用草药和针灸治疗中医病人就诊次数的大致数字
Yes是
No否
Respiratory Disorders 呼吸道疾病
1Gan Mao 感冒: Common Cold & Flu
2 Ke Sou 咳嗽: Cough
3Xiao Chuan 哮喘: Wheezing & Asthma/Breathless Digestive Disorders
Digestive Disorders 消化道疾病
4Wei Wan Tong 胃脘痛:EpigastricPain/Gastralgia
5 Tu Suan 吐酸 : Acid Reflux 6 Cao Za嘈杂 : Gastric Upset
7Fu Tong 腹痛 : Abdominal Pain/Colitis
8 Xie Xie 泄泻 : Diarrhea 9 Bian Mi 便秘 : Constipation 10 Xiao Ke 消渴 : Diabetes 11 Ou Tu 呕吐 : Vomiting

26
Pain/ Neurological Disorders疼痛 / 神经疾病
12Bi Zheng痹证: Painful Obstruction Syndrome/Arthritis
13Mian Tong 面痛 : Facial Pain/TrigeminalNeuralgia
14Yao Tong 腰痛: Lumbago/Sciatica
15Lao Zhen 落枕: Neck Sprain/Stiff Neck
16 Niu Shang 扭伤 : Sprains
17Mian Tan 面瘫 :Facial Paralysis/Bell’s Palsy
18 Tou Tong 头痛: Headaches
19Xie Tong 胁痛:Hypochondria Pain
20Xuan Yun 眩晕: Dizziness/Vertigo
21 Zhong Feng 中风: Stroke
22 Jue Zheng 厥证: Syncope
23Wei Zheng 痿证: Atrophy Syndrome
27
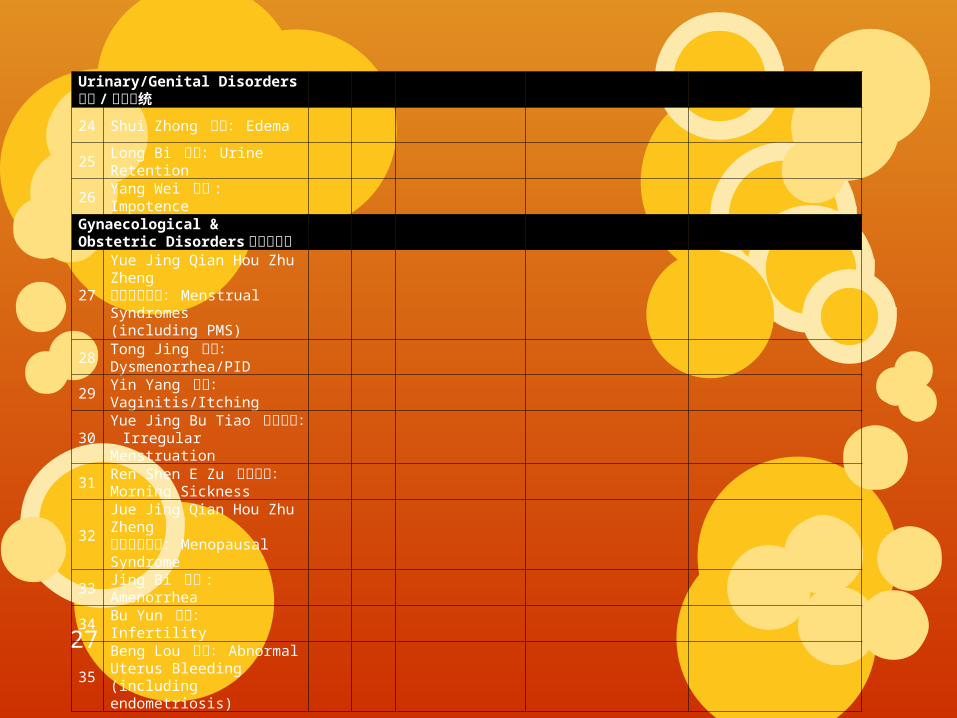
Urinary/Genital Disorders泌尿 / 生殖系统
24 Shui Zhong 水肿: Edema
25Long Bi 癃闭: Urine Retention
26 Yang Wei 阳痿 : Impotence
Gynaecological & Obstetric Disorders 妇产科疾病
27
Yue Jing Qian Hou Zhu Zheng月经前后诸证: Menstrual Syndromes(including PMS)
28Tong Jing 痛经: Dysmenorrhea/PID
29Yin Yang 阴痒: Vaginitis/Itching
30Yue Jing Bu Tiao 月经不调: IrregularMenstruation
31Ren Shen E Zu 妊娠恶阻:Morning Sickness
32Jue Jing Qian Hou Zhu Zheng绝经前后诸证: Menopausal Syndrome
33 Jing Bi 经闭 : Amenorrhea
34 Bu Yun 不孕: Infertility
35Beng Lou 崩漏: Abnormal Uterus Bleeding(including endometriosis)
28
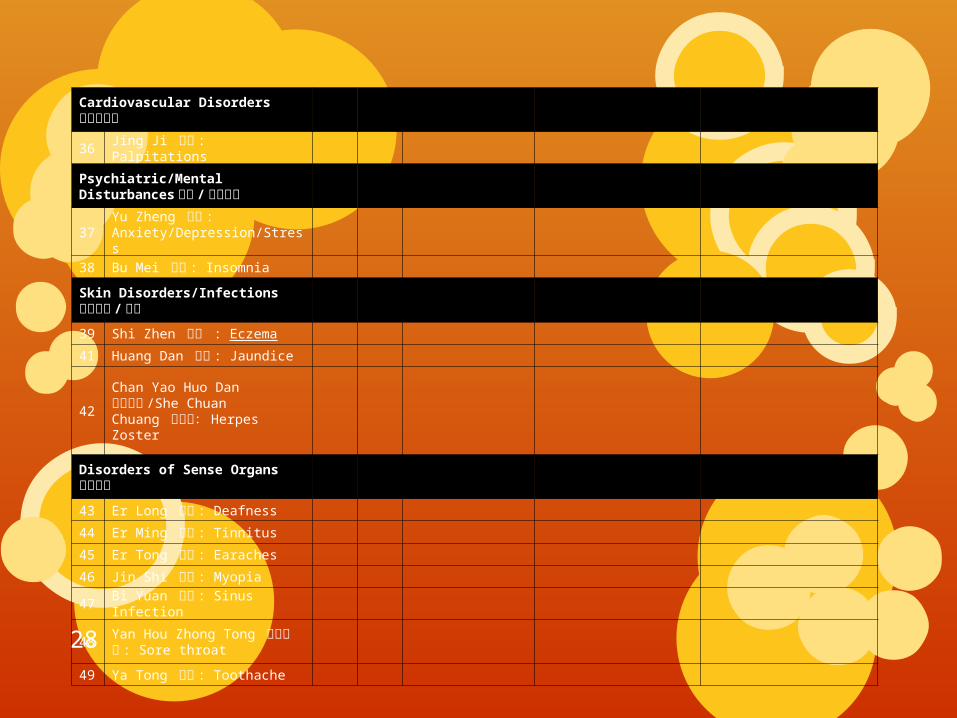
Cardiovascular Disorders心血管疾病
36 Jing Ji 惊悸 : Palpitations
Psychiatric/Mental Disturbances 神经 /心理疾病
37Yu Zheng 郁证 : Anxiety/Depression/Stress
38 Bu Mei 不寐 : Insomnia
Skin Disorders/Infections皮肤疾病 / 感染
39 Shi Zhen 湿疹 : Eczema
41 Huang Dan 黄疸 : Jaundice
42Chan Yao Huo Dan 缠腰火丹 /She ChuanChuang 蛇串疮: Herpes Zoster
Disorders of Sense Organs感官疾病
43 Er Long 耳聋 : Deafness
44 Er Ming 耳鸣 : Tinnitus
45 Er Tong 耳痛 : Earaches
46 Jin Shi 近视 : Myopia
47 Bi Yuan 鼻渊 : Sinus Infection
48Yan Hou Zhong Tong 咽喉肿痛 : Sore throat
49 Ya Tong 牙痛 : Toothache

29
Pediatric Disorders 小儿疾病
50
Gan Ji 疳积: Indigestion for Children
Blood Disorders 血液疾病
Cancer 癌症
Other 其他
51
Xu Lao 虚劳 : Tiredness/Fatigue
52
Zhi Chuang 痔疮 : Hemorrhoid
30
GRAND TOTAL总计 :_______________Total: 2,000 TCM patient visits 总计: 2,000 中医就诊次数 Yes是 No否 Validation of Traditional Chinese Medicine Patient Visits中医病人就诊确认 "I hereby certify that I have been trained to perform, am competent to perform and have performed in myemployment the specific treatments and diagnoses set out above, within the time frame indicated. I hereby certifythat I have completed a minimum of 2,000 traditional Chinese medicine patient visits within the past 5 years. Iunderstand that providing false or misleading information about my patient visits is grounds for denying or revokingmy registration".“我在此证明我经过治疗训练,能够胜任治疗且已经在我的工作单位进行过了上述特定的治疗和诊断,满足时间要求。我在此证明我在过去的五年内已经完成了 2,000 次中医病人就诊次数。 我明白在我的病人就诊上提供虚假和误导性资料会导致注册被拒或撤销。” _____________________________ ________________________ _______________________Applicant’s Signature 申请人签字 Print Name 打印姓名 Date Signed 签字日期 _____________________________ ________________________ _______________________\Witness Signature 目击者签字 Print Name 打印姓名 Date Signed 签字日期 Be advised that the College reserves the right to contact you and your employer for clarification regarding your employment history and patient visits listed on this Validation Certificate respecting traditional Chinese medicine patient visits that you have completed and signed.请了解,管理局保留联系您和您雇主的权利,以调查确认您的工作经历和在上述确认记录中罗列的您签字确认的进行过的中医病人就诊记录。

31
11. PROFESSIONAL LIABILITY INSURANCE 职业保险
I confirm that I shall comply with the College’s required professional liability insurance coverage as specified in the By‐laws of College.
我确认我会遵守根据管理局法规规定管理局要求的个人职业保险。 Check ONE of the following two boxes请在以下一个选项方框中划√ I agree to submit the insurance certificate to the College within 30 days after my registration has been approved. 我同意在我的注册申请被批准后 30天之内将保险证明提交到管理局。 I have attached the certficate of professional liability insurance. 我已附上我的个人职业保险证明。 For more information, refer to the Registration Policies on “Professional Liability Insurance” available on our websiteat www.ctcmpao.on.ca.更多有关”职业保险”注册要求的信息,请参加管理局网站: www.ctcmpao.on.ca.
32
12. DECLARATION OF CONDUCT 行为声明
a) Have you ever been found guilty of any non‐criminal offence that resulted in a fine ofover $1,000 or any form of custody or detention or had a finding of guilt for a criminaloffence in Ontario or in any other jurisdiction in or outside Canada? Yes 是 No否您有没有被判超过 $1,000元以上的罚款或被判以任何形式的拘留或扣押的非刑事犯罪,或在安省或以任何形式在加拿大或海外被判决的刑事犯罪? b) Has there ever been a finding of professional negligence or malpractice against you? Yes 是 No否您是否被判决过专业疏忽或错误操作? c) Has there ever been any finding of professional misconduct, incompetence orincapacity, or similar finding against you by any regulatory body in Ontario or in anyother jurisdiction? Yes 是 No否您是否被安省规管机构或其他管辖机构判决过有专业失误、缺乏专业能力或不胜任,或类似判决? d) Is there currently a proceeding against you involving an allegation of professionalmisconduct, incompetence or incapacity, or any similar proceeding by any regulatorybody in Ontario or in any other jurisdiction? Yes 是 No否您现在是否涉及被被安省规管机构或其他管辖机构指控专业失误、缺乏专业能力或不胜任,或其他类似指控的程序中? e) Have you ever made an application for registration as a Traditional Chinese MedicinePractitioner and/or Acupuncturist in any other jurisdiction that was refused? Yes 是 No否您是否曾经在任何其他的管辖机构提交中医师和 / 或针灸师申请而被拒? f) Have you ever had an application for registration rejected by a regulatory College inOntario or in another province? Yes 是 No否您是否曾经在安省或其他省向任何一个管理局提交注册申请被拒? g) Have you ever been unsuccessful in an attempt to pass a registration examination fora regulated health profession in Ontario or in another jurisdiction? Yes 是 No否您是否曾经在安省的卫生规管或其他任何管辖机构参加注册考试而未通过?
33
h) Has there ever been a court proceeding brought against you alleging that you heldyourself out as, or practising as a regulated health professional without being soregistered? Yes 是 No否您是否经历过被指控您本身或作为规管的卫生职业中在治疗时没有注册?
i) Do you currently suffer from any physical or mental condition or disorder which mayimpair your ability to practise traditional Chinese medicine safely and competentlyand which, if left untreated, would impair your ability to practise traditional Chinesemedicine safely and competently? Yes 是 No否您目前是否在经历身体或心理的疾病阶段,导致丧失部分安全和胜任使用中医治疗的能力,在这种情况下,如果未被治疗,将会影响您安全和胜任使用中医治疗的能力?
NOTE: If you answer “yes” to question i), provide a detailed explanation and arrange for your treating regulated health professional(s) to send directly to the College a report on your condition or disorder setting out your diagnosis, course of treatment and current health prognosis. Where appropriate, this report should indicate any accommodation(s) that your regulated health professional deems necessary in order for you to practise in a safe manner.说明:如果您在 i)问题后面选了“是”,您需要提供详细的说明并安排注册卫生体系治疗师直接向管理局提交报告说明您的情况和病况诊断,治疗进程和当前的健康预估。在适当情况下,该报告需指出您作为规管的卫生体系专业人员要安全治疗病人必须具备的条件。
The College might require further information from your past and/or present treating regulated health professional and will contact him or her, if necessary.管理局在需要时可能会在今后向您过去和 / 或现有的注册治疗师索要信息和与其进行联系。In submitting this form, you are providing your authorization to your past and/or present treating regulated health professional to disclose further information to the College.提交该表格,表示您向您过去和 / 或现有的注册治疗师授权将更多的信息提交给管理局。
34
j) If you were registered with a body responsible for the regulation of aprofession, and you ceased being registered, were you in good standing, (i.e., allfees paid, all information provided, no outstanding investigations, proceedingsor sanctions) at the time you ceased being registered? If no, provide details. Yes 是 No否 N/A 不适用如果您曾经在某职业注册机构注册,而您停止了注册,是否在您停止注册时遵守了所有要求,(如付清所有费用,提供了所有信息,未被进行重大调查、指控或制裁?如果不是,请提供细节。
k) If you are a member of a regulated profession, did you ever fail to comply withany obligation to pay fees or provide information to the regulator? Yes 是 No否 N/A 不适用如果您是规管职业的注册会员,您是否曾有未完成付费或为管理局提供信息的义务?
l) If you are a member of a regulated profession, has an investigation by theregulator ever been initiated in respect of you? Yes 是 No否 N/A 不适用如果您是规管职业的注册会员,您是否曾接受过管理局的调查?
m) If you are a member of a regulated profession, has the regulator ever imposed asanction on you? Yes 是 No否 N/A 不适用如果您是规管职业的注册会员,您是否曾接受过管理局的制裁?
n) Is there any other event that would provide reasonable grounds that you willnot practise traditional Chinese medicine in a safe and professional manner? Yes 是 No否有没有发生过任何事件足以证明您不安全和不专业地使用中医治疗病人?
35
If you answer “yes” to any of the above questions (with the exception of j), provide full details and attach copies of all relevant documents.如果以上任何问题的回答是“是”(除了 j),请提供细节并附上所有相关材料复印件。 If your answer to any of the above questions changes following your submission of the application, but before any issuance of a certificate, you must immediately advise the College and provide written details with respect to any change.如果您对以上问题的回答在您提交申请后发生任何变化,而该变化发生在注册证书颁发前,您必须要即刻通知管理局并提交有关变化的详细书面说明。 I have attached a criminal background check using the Canadian Police Information Centre (CPIC) database 我已附上了通过加拿大警察信息中心数据库出示的犯罪背景调查, issued on ______ /______ /_______ / and by _________________________调查颁发 (mm月 / dd日 / yyyy年 ) (Specify OPP or municipal police service in Canada) (请具体安大略省警察局或在加拿大的市级警局) For more information, refer to the Registration Policies on “Criminal Background Check” available on our website atwww.ctcmpao.on.ca.更多有关”犯罪背景调查”注册要求的信息,请参加管理局网站: www.ctcmpao.on.ca

36
13. HEALTH PROFESSION DATABASE 健康体系职业数据库
The Ministry of Health and Long‐Term Care and the College are working together to learn more about your profession by collecting demographic, geographic, educational, and employment information. This data collection is part of HealthForceOntario, the province's health human resources strategy. Your answers to these questions will help the Ministry develop policies and programs that address supply and distribution, education, recruitment and retention for your profession.通过收集人口调查数据、地理信息、教育信息和雇佣信息,卫生厅和管理局共同合作致力于对您的职业进行更多的了解。数据的收集部分工作属于安省健康资源 - 省卫生体系人力资源战略。您对以下问题的回答可以帮助卫生厅完善政策和开发项目以为您的职业提供补给和布局、提供教育、人才招募和维系。 All of Ontario's 80,000 regulated allied health professionals are providing this information as part of their annual registration and renewal process. To protect your privacy, the data we submit to the Ministry will be anonymous. You are required to provide this information under the Regulated Health Professions Act, 1991. The reliability of the information we receive and the quality of the decision making that follows depends on you. By completing this form accurately and thoroughly, you will help ensure that Ontarians have access to the services of your profession, when and where they need them.安省所有的 80,000 个联合规管职业人员都要在每年的注册和更新程序中提供这些信息。为了保护您的隐私,此数据将以匿名形式发给卫生厅。根据 1991 规管健康职业法案,您需要提供这个信息。我们收集到信息的可靠性和决策的有效性取决于您的行为。您准确和完整填写该信息表格,将能够帮助我们确保安省居民在需要的时候能够随时随地地获得您这类职业的服务。
37
Concurrent registration 当前注册Check the box(es) applicable to you. 请在适用您的方框里打√。 I am currently registered to practice traditional Chinese medicine in countries other than Canada我当前在加拿大以外的国际注册从事中医。 If yes, provide up to three countries where you are currently registered to practice the traditional Chinese medicine profession.如果是,请提供最多三个你所在注册从事中医的国家。 1. __________________________ 2. ___________________ 3. _________________________ Provinces/territories or states other than Ontario where you are currently registered to practise (Select up to 3)请填写您当前在安省以外从事中医的省 / 地区或州(至多选择 3 个) Alberta阿尔伯塔 British Columbia 不列颠哥伦比亚 Manitoba 曼尼托巴 Other 其他 Newfoundland纽芬兰 Nova Scotia新斯科舍 Northwest Territories 西北领地 State(s) in USA美国州 Nunavut 努勒维特 Prince Edward island 爱德华王子 New Brunswick新不伦瑞克省 1. _________________ Quebec 魁北克 Saskatchewan萨斯卡通 Yukon Territory 育空领域 2. _________________ 3. _________________

38
Practice history 从业经历
If you previously practised outside of Canada, indicate the country where you practised most recently如果您之前在加拿大以外从事中医治疗,请填写您最近从事中医的国家 ________________________________________(Country) 国家
OR If you previously practised outside of Ontario but within Canada, indicate the province/ territory whereyou practised most recently或如果您之前在加拿大内但在安省外的地方从事中医,请填写您最近从事中医的省 / 地区 ___________________________________________(Province/Territory) (省 / 地区)
If USA, specify the state 如果在美国,请明确在哪个州 _____________________________________________Last year in which you practised in the most recent location other than Ontario ___________________________去年最近您在安省以外的哪个地方从事中医 (year)(年)

39
Education related to traditional Chinese medicine 中医相关教育 Indicate all education related to the traditional Chinese medicine profession (e.g. diploma, doctorate, baccalaureate, master, professional doctorate, other.)请列出所有有关中医职业教育(如:毕业证书、博士学位、本科学士、硕士学位、专业博士、其他)
Degree学位 Institution of Graduation毕业学校
Province/State省/州
Country国家 Year of Graduation哪年毕业
1.
2.
3.
4.
5.
Education NOT related to traditional Chinese medicine qualifications与中医无关的教育资质 Highest level of education completed that was unrelated to traditional Chinese medicine qualifications与中医无关教育的最高学历 Diploma毕业证书 Baccalaureate本科学士 Masters硕士 Doctorate博士 Professional Doctorate专业博士 Other其他
Field of study for highest level of education completed that is NOT related to traditional Chinese medicine qualifications 与中医无关教育的最高学历学习领域 General Rehabilitation Science康复医学 Mathematics, Computer Information Sciences数学,计算机信息科学 Medical Laboratory Science实验医学 Health Administration/Management健康管理 Public Administration公共管理 Kinesiology and Exercise Science运动科学 Public Health公共健康 Health Professions and Related Clinical Sciences健康职业和相关临床科学 Gerontology老年医学 Biological and Biomedical Sciences生物与生物医学 Psychology心理学 Social Sciences, Arts and Humanities社会学,艺术和人文 Physical Sciences 物理学 Business, Management, Marketing and Related商业,管理,营销及相关 Education教育 Law法律 Engineering工程 Other Field of Study其他学习领域 Country of Graduation毕业国家 Canada加拿大 USA美国 Other (Specify)其他(请明确)_______________________ Year of Graduation毕业年份___________ Province/Territory, if education completed in Canada__________________ 如果在加拿大完成教育,在哪个省/地区 State(s) if education completed in USA _______________________ 如果在美国完成教育,在哪个州
40
Employment工作 Is this the first time you will practise the traditional Chinese medicine profession? Yes是 No否 这是您第一次从事中医职业吗? If no, in which country and year did you first begin to practise in the traditional Chinese medicine profession? 如果不是,您于哪年在哪个国家第一次开始从事中医职业 _________________________ ________________________________ (Country) (国家) (year) (年) If the country where you first practised the traditional Chinese medicine profession was Canada or the USA indicate province/territory or state. 如果您第一次开始从事中医职业是在加拿大或美国,请填写在哪个省/领域或州。 Alberta阿尔伯塔 British Columbia 不列颠哥伦比亚 Manitoba 曼尼托巴 Other其他 Newfoundland纽芬兰 Nova Scotia新斯科舍 Northwest Territories 西北领地 State(s) in USA美国州 Nunavut 努勒维特 Prince Edward island 爱德华王子 New Brunswick新不伦瑞克省 1. _________________ Quebec 魁北克 Saskatchewan萨斯卡通 Yukon Territory 育空领域 2. _________________ 3. _________________ If the country where you first practised the traditional Chinese medicine profession was not Canada provide the first Canadian location of practice in the profession. 如果您第一次从事中医职业的地方不是加拿大,请提供您第一次在加拿大从事该职业的地点。 Alberta阿尔伯塔 British Columbia 不列颠哥伦比亚 Manitoba 曼尼托巴 Newfoundland纽芬兰 Nova Scotia新斯科舍 Northwest Territories 西北领地 Nunavut 努勒维特 Prince Edward island 爱德华王子 New Brunswick新不伦瑞克省 Quebec 魁北克 Saskatchewan萨斯卡通 Yukon Territory 育空领域 Ontario 安省 In which year did you first begin to practise the traditional Chinese medicine profession in Canada? ____________________ 您首次在加拿大从事中医职业是在哪一年? (year)(年)

41
14. APPLICANT’S DECLARATION (申请人声明)
I_____________solemnly declare that the contents of this application including all attachments are true and complete to the best of my knowledge and belief.我 ___________郑重声明以上申请内容以及附属文件基于我的知识和想法并且是真实的完整的。 I understand and agree that if I make any false or misleading statement or representation on or in connection with my application, I shall be deemed not to have satisfied the registration requirements for a Certificate of Registration.我了解并同意如果在申请中作出任何虚假或具误导性的陈述或申述,将被视为不符合注册要求。 I further understand and agree that if the Certificate of Registration should be issued to me based upon any false or misleading statement or representation, the Certificate of Registration can be immediately revoked and I may face disciplinary proceedings.我了解并同意,如果发给我的注册证书是基于任何我提供的虚假或误导性陈述或申述,注册证书将被立即撤销,并且可能会面临纪律处分。 I acknowledge that the information provided on this form is used by the College to administer the Regulated Health Professions Act, 1991, the Traditional Chinese Medicine Act, 2006, the Regulations under these Acts, the By‐laws, policies, Standards of Practice and programs related to the governance of the profession; and that the information is collected, used and disclosed in accordance with the Health Professions Procedural Code and the College By‐laws.我了解这份表格所提供的信息是用于管理局协助实施对专业标准和与政府相关的专业方案《规范管理健康卫生法案1991》,《中国传统医药法案 2006》的法律细则。这些信息的收集,使用和公开将与《卫生专业守则》和管理局一致 I understand that I must notify the Registrar in writing within thirty days of any change of location of practice or employment, business name of practice, home and mailing addresses, phone number, and email address.我了解,如果有任何更改包括地点,企业名称,雇员,家庭和邮寄地址, 电话号码和电邮地址,必须在三十天内以书面形式通知注册处。
42
I authorize the College to obtain information from other regulatory bodies, educational institutions, present and former employers, referees, any of my past and/or present treating regulated health practitioners, and any other sources for the purposes related to my application for registration, including any experience and qualifications.我授权管理局通过其他监管机构,教育机构,现任雇主或 / 和前雇主,仲裁人员,或是任何过去和 / 或现在的卫生监管人员,及其他任何资源,以调查注册资格为目的获取我的经历和资料。
I authorize my past and/or treating regulated health practitioners to disclose personal health information to the College for the purposes related to my application for registration.我授权我过去和 / 或现在的卫生监管人员,以我的注册申请为目的向管理局公开我的个人健康信息。
Taken and declared before me in the( 签署于 ):
_____________________ _______________________ _____________________ City/Town (城市 /城镇 ) Province/State (省 /州) Country (国家 )
This 在 ________________________________day of 日期 ________________________________________20_____
Signed______________________________________ Signature of Applicant__________________Commissioner of Oaths, Notary Public, Lawyer 监誓官,公证人,律师(Official seal/stamp or business card must be provided) ( 需附官方印章或名片 )

43
For Grandparented Registration关于祖辈法注册申请
Attached a certified cheque or money order made payable to “CTCMPAO” for $169.50; AND
请附上 $169.50 保付支票或现金支票,抬头为安省中医师及针灸师管理局。
Attached a certified cheque or money order made payable to “CTCMPAO” for $960.50
请附上 $960.50 保付支票或现金支票,抬头为安省中医师及针灸师管理局。
Selected the title/designation to apply
请选择要申请的标题 / 名称
Provided evidence of identity (e.g. birth certificate, passport, marriage certificate, divorce decree or a validation of identity signed by legal counsel.)
提供身份证明(例如:出生证明,护照,结婚证明,离婚判决书或者合法机构提供的有效身份证明)
Provided preferred name to be used for Certificate of Registration and on the Register
提供首选的名字用于证书的注册和登记
(Note: the name you use in your practice and your name on the College register must be the same. Follow instructions on section 2 of the application, if your practice name is different from your legal name.)
(注意:用于实际的名字必须和在管理局注册的名字相同。如果您实际用的名字和您有效证件的名字不相 同,请遵照申请第二部分的介绍。)
Provided business address 需提供办公地址
Attached passport size photo taken within last 12 months 请附上一年内拍摄的,护照大小的照片
Attached letter confirming completion of Jurisprudence Course 请附上完成法律体系课程的证明
Attached letter confirming completion of Safety Program 请附上完成中医师针灸师安全课程的证明
Attached written language plan if indicated that you are unable to read and write with reasonable fluency in either English or French to offer professional services to patients.
请附上书面语言计划,如果您为病人提供专业服务时不能相对流利的使用英文或法文。
Attached copy of certificate of registration or licences to practise traditional Chinese medicine profession in Canada or other Country or State where you have previously worked, if applicable
如果可以请附上您以前曾在加拿大或其他国家,其他州的中国传统医学的注册证书(或执照)的复印件
Provided membership information with professional TCM association, if applicable
如果可以请提供所属的传统中医协会的会员信息
Completed information on work history/practice experience in Canada within the last 5 years
请提供完整的工作历史信息 /近五年内在加拿大的实际经验
Completed Validation Certificate on 2,000 traditional Chinese medicine patient visits within the last five years; and Signed and Witnessed the Validation Certificate
请提供完整的在近五年内有 2,000 名传统中医药病人访问的认证。(签字并公证有效认证)
Attached professional liability insurance (if available, if not, submit within 30 days after registration has been approved)
请附上职业责任保险(如果您不能提供, 需在申请注册 30天内补交)

Answered all questions on declaration of conduct
回答所有行为守则上的所有问题
Attached report on criminal background check
请附上犯罪历史的报告
Answered all questions on Health Profession database (required by the Ministry of Health and Long‐Term Care)
回答卫生数据库上的所有问题(健康及长期护理管理局)
Applicants declaration signed and validated by Commissioner of Oaths, Notary Public, Lawyer
请提供宣誓官 ,公证人 , 律师签署并验证的申请人声明

THANK YOU!
Related Documents










![HOME [] 217 Grandparenting.pdfHome > Article Archive Relationships Grandparenting For more information, visit our Grandparenting Resource Page. When Faiths Diverge, Seek the Ties That](https://static.cupdf.com/doc/110x72/5f9550f74885157cff3b55f4/home-217-grandparentingpdf-home-article-archive-relationships-grandparenting.jpg)
