Rathachai Kaewlai, MD Division of Emergency Radiology, Department of Radiology Ramathibodi Hospital, Mahidol University, Bangkok RCRT 2015 at Centara Grand @CentralPlaza Ladprao

CT Radiation Management: Why and How
Jul 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Rathachai Kaewlai, MD Division of Emergency Radiology, Department of Radiology Ramathibodi Hospital, Mahidol University, Bangkok RCRT 2015 at Centara Grand @CentralPlaza Ladprao
! Lack of scientific consensus ! Assumption of risk from atomic bomb survivors
! How to act? Two possible errors… ! Assume risks are real and to then discover that
they do not exist ! Assume risks are nonexistent and to
subsequently discover that they are real
Huda W. Radiation risks: what is to be done? AJR 2015 January
! Lack of scientific consensus ! Assumption of risk from atomic bomb survivors
! How to act? Two possible errors… ! Assume risks are real and to then discover that
they do not exist ! Assume risks are nonexistent and to
subsequently discover that they are real
Huda W. Radiation risks: what is to be done? AJR 2015 January

! Low-level radiation (up to 100 mSv) ! 30-40X annual natural
background ! 10X a usual CT scan
! Linear no-threshold hypothesis
! 12 cancers with significant lifetime excessive risks: lung, liver, breast, prostate, stomach, colon, thyroid and leukemia
Committee on the Biological Effects of Ionizing radiation of the US National Academy of Sciences (2005) Figure from web.princeton.edu

! At low doses, the risk = one excess cancer in 100 exposed persons (100 mSv) during their lifetime. Mortality is about one-half.
! Higher risk in female and children
Committee on the Biological Effects of Ionizing radiation of the US National Academy of Sciences (2005)

! “Most recent data for the survivors of the atomic bombings are largely consistent with linear or linear-quadratic dose trends over a wide range of doses”
United Nations Scientific Committee on the Effects of Atomic Radiation (2006)
! “….the practical system of radiation protection recommended by the Commission will continue to be based on the assumption that, at doses below about 100 mSv, a given increment in dose will produce a directly proportionate increment in the probability of incurring cancer.”
International Commission on Radiological Protection (2007)
! Do we agree on the risk of radiation? ! Do we agree on our role in it?
Radiologists’ professional role
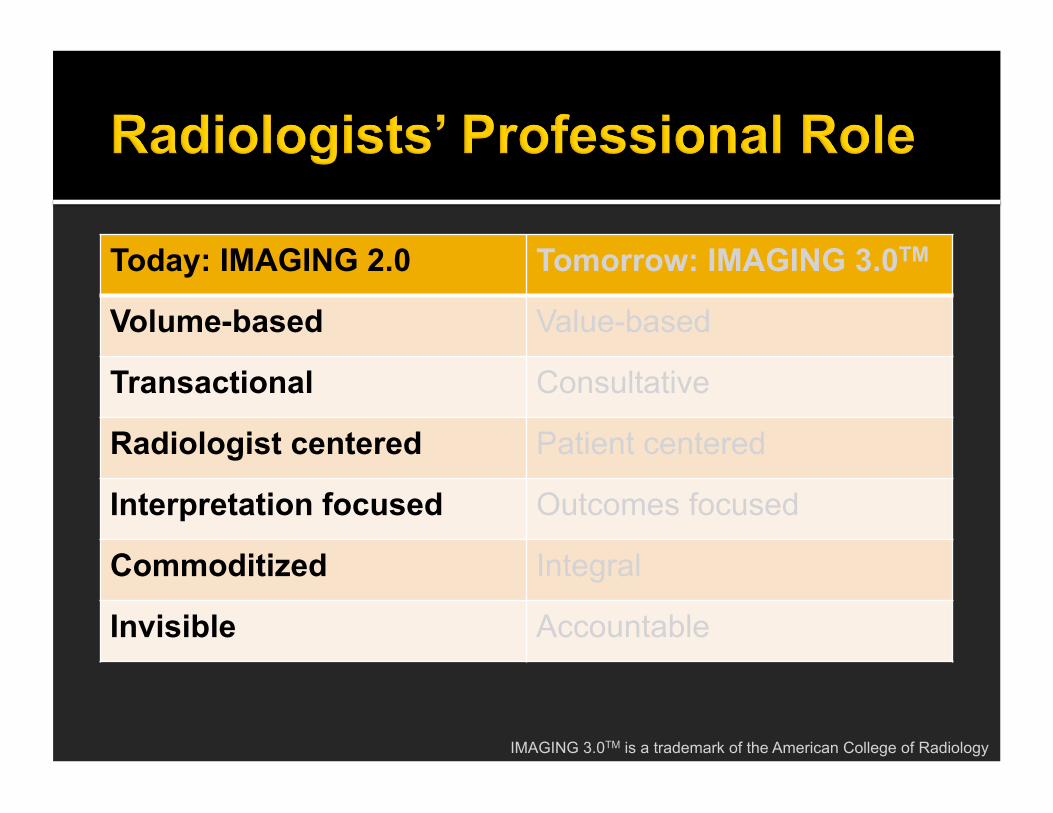
Today: IMAGING 2.0 Tomorrow: IMAGING 3.0TM
Volume-based Value-based
Transactional Consultative
Radiologist centered Patient centered
Interpretation focused Outcomes focused
Commoditized Integral
Invisible Accountable
IMAGING 3.0TM is a trademark of the American College of Radiology

Today: IMAGING 2.0 Tomorrow: IMAGING 3.0TM
Volume-based Value-based
Transactional Consultative
Radiologist centered Patient centered
Interpretation focused Outcomes focused
Commoditized Integral
Invisible Accountable
IMAGING 3.0TM is a trademark of the American College of Radiology
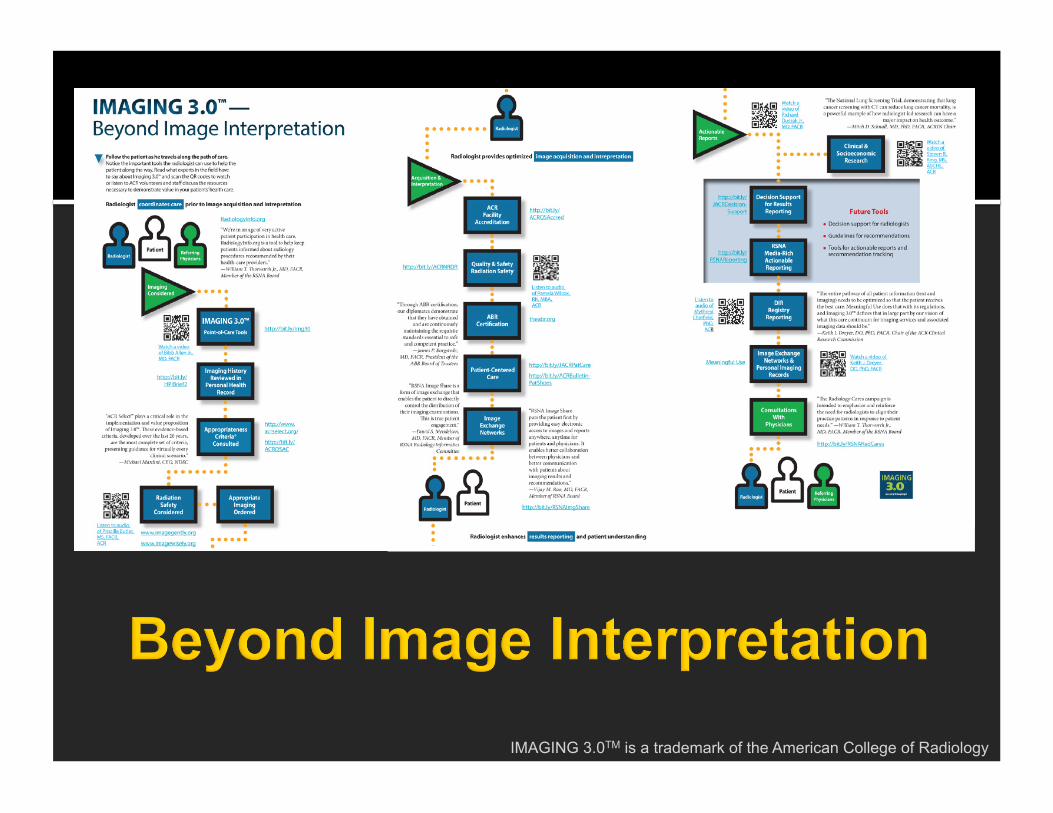
IMAGING 3.0TM is a trademark of the American College of Radiology
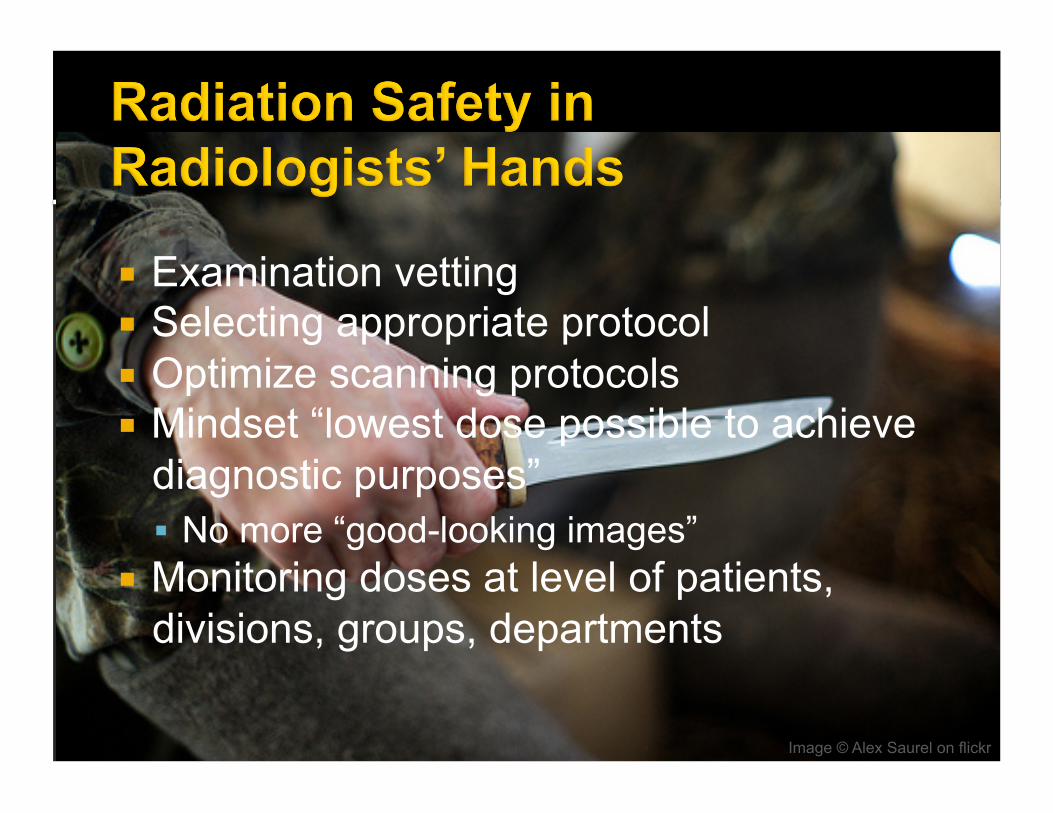
Image © Alex Saurel on flickr
! Examination vetting ! Selecting appropriate protocol ! Optimize scanning protocols ! Mindset “lowest dose possible to achieve
diagnostic purposes” ! No more “good-looking images”
! Monitoring doses at level of patients, divisions, groups, departments

! Low-level radiation is a health hazard – LNT hypothesis
! Radiologists have a critical role in optimizing CT radiation exposure (should be a leader of the team)
! Why CT? ! CT parameters and radiation units ! Ramathibodi Emergency Radiology
experience ! Case examples (acute abdomen) ! Step-by-step guide to manage CT
radiation

! Medical radiation is now the majority of radiation exposure in human ! CT accounts for most of this
! CT volume on the rise ! No dose penalty in CT ! CT radiation dose is intrinsically high ! No binding regulations on CT doses ! CT radiation errors made into headlines

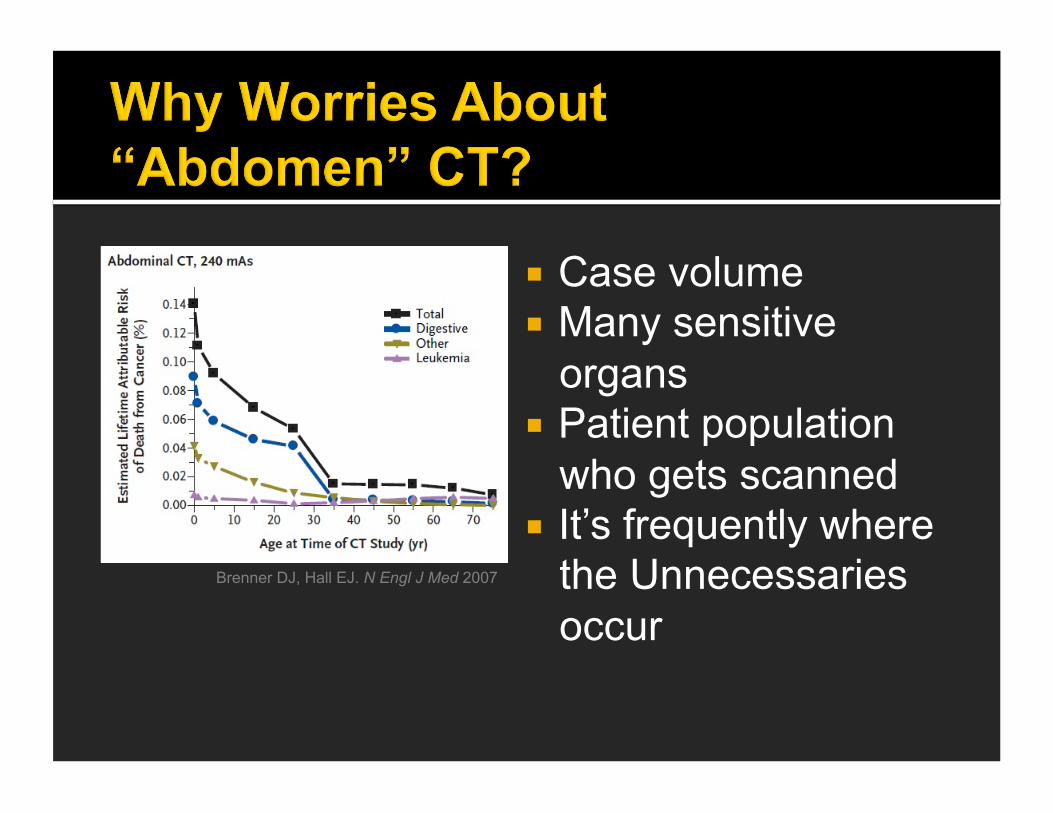
! Case volume ! Many sensitive
organs ! Patient population
who gets scanned ! It’s frequently where
the Unnecessaries occur
Brenner DJ, Hall EJ. N Engl J Med 2007

! Assuming radiation risks are real ! Doing CT is weighing this risk with benefit
! If benefit > risk means a justified examination ! Providing other diagnostic options
! Using as low radiation as possible to obtain needed diagnostic information (ALARA)

Imaging exam ordered by referring physician
Vetting/protocoling by radiologist
Scanning
Post-processing
Monitoring of quality
Assetprotectionlawjournal.com
Massgeneralimaging.org
Medicineworld.org Jenkinsclinic.org
Blog.vpi-corp.com
" Educate physicians about radiation risks
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
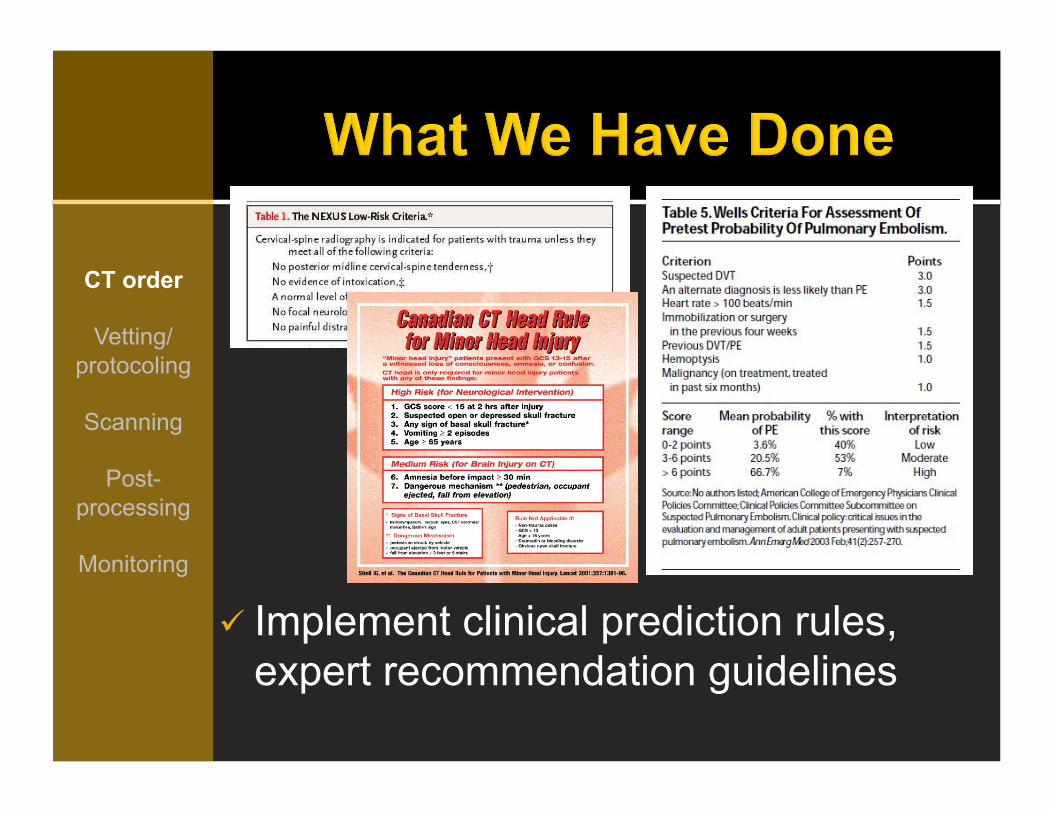
" Implement clinical prediction rules, expert recommendation guidelines
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
" Import exams from outside hospitals to PACS
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
! Patients transferred to trauma center 38/137 (28%) received duplicated scans in 24 hours
! Most common reason for duplication = lack thin-section data on CD (37%)
! Additional radiation 10.2 mSv ! Additional charge $409
Can we use radiation-free imaging (US, MRI) instead of CT for this
clinical scenario?
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
Make ultrasound (by radiologist) available and easily accessible 24/7

Can we use radiation-free imaging (US, MRI) instead of CT for this
clinical scenario?
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
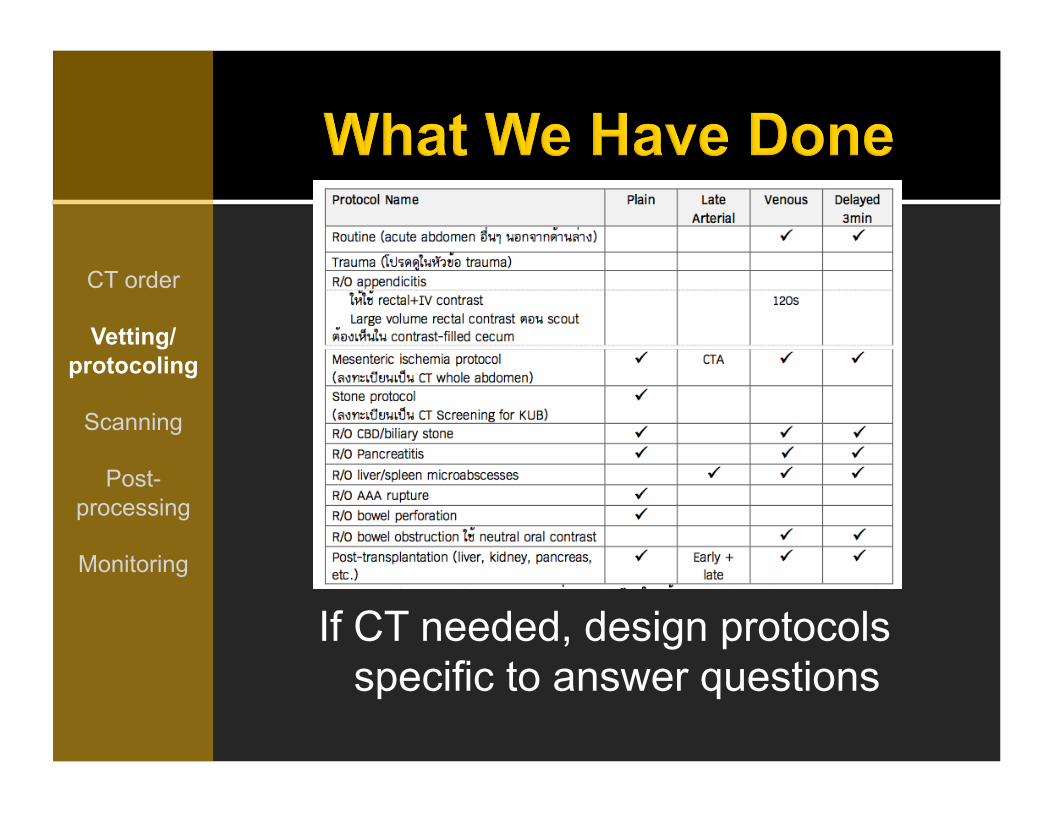
If CT needed, design protocols specific to answer questions
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring

“Routine” protocol with minimum scanning phases. Nonroutine done by add-ons
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
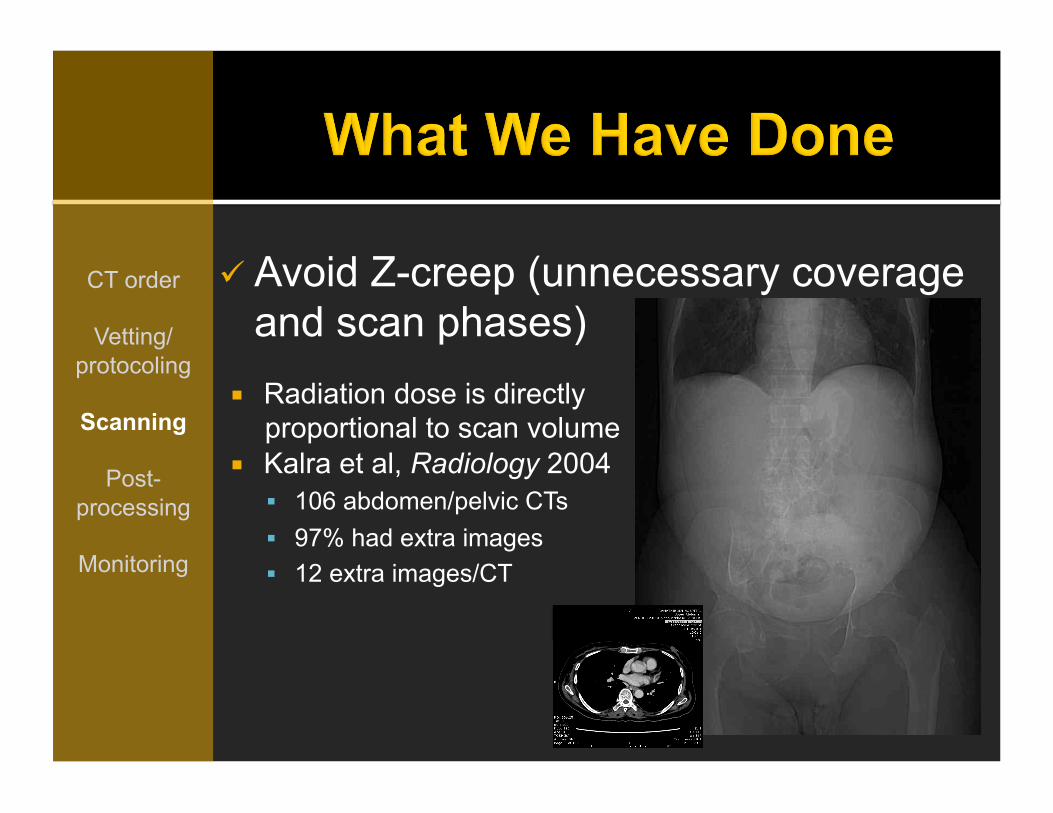
" Avoid Z-creep (unnecessary coverage and scan phases)
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
! Radiation dose is directly proportional to scan volume
! Kalra et al, Radiology 2004 ! 106 abdomen/pelvic CTs ! 97% had extra images ! 12 extra images/CT
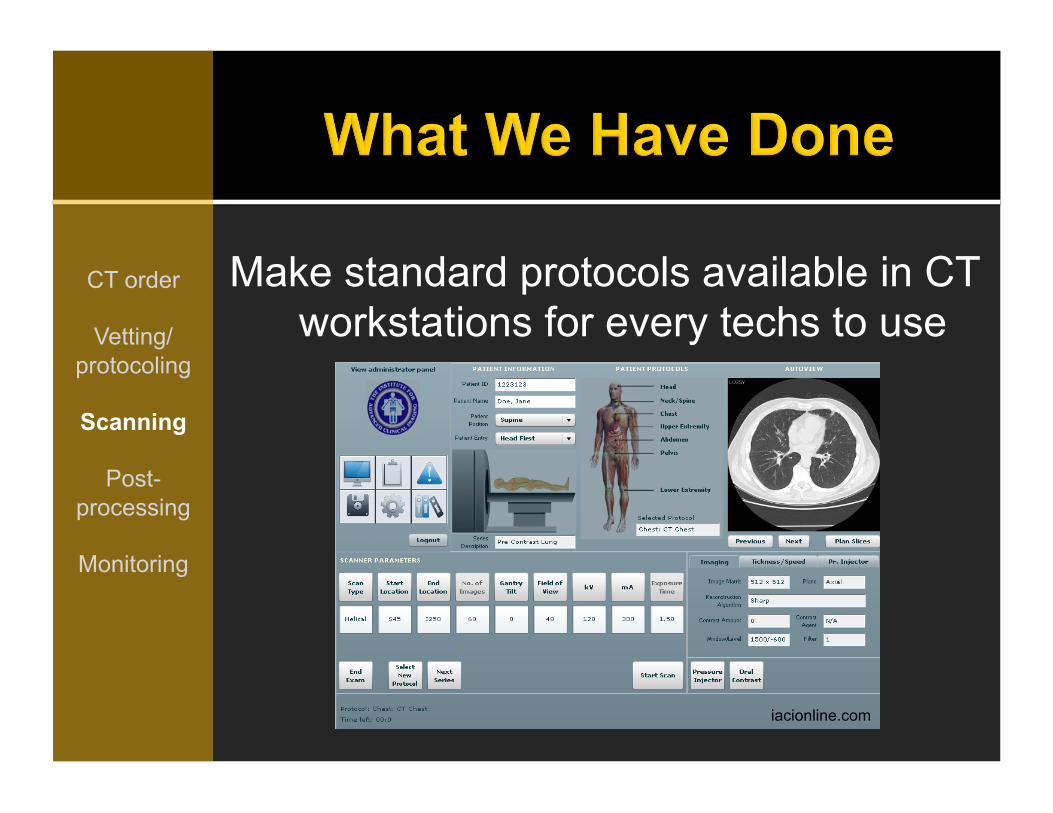
Make standard protocols available in CT workstations for every techs to use
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
iacionline.com
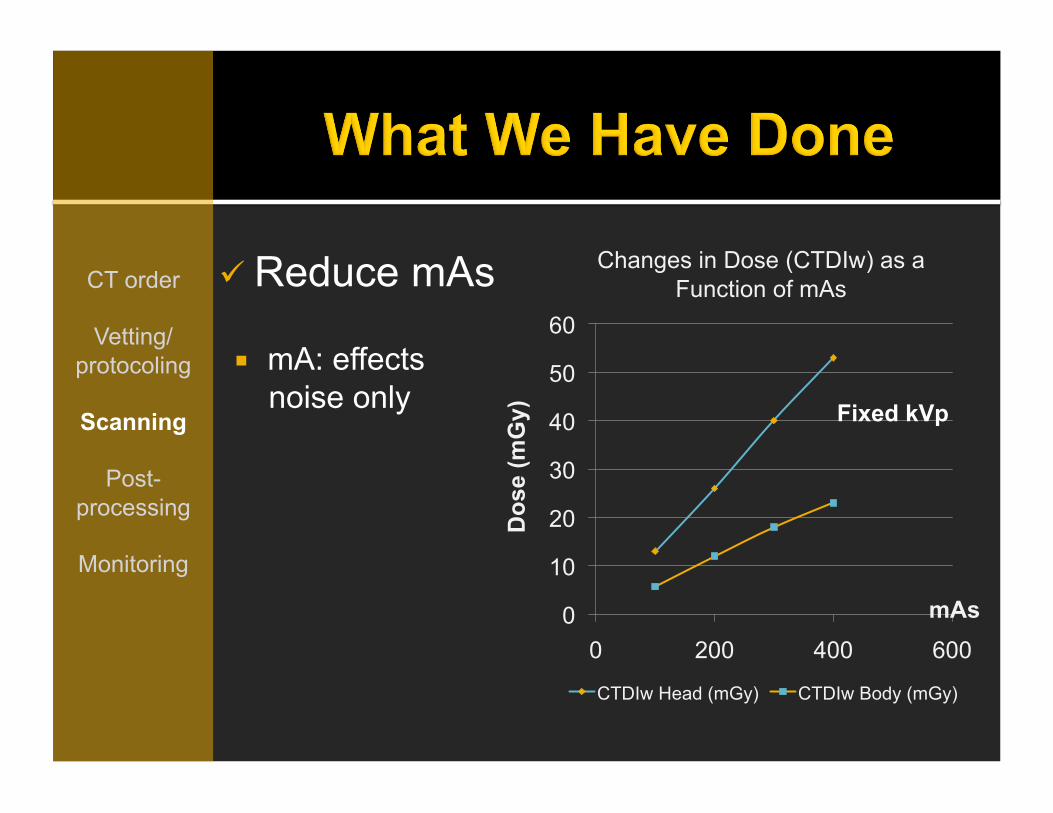
" Reduce mAs CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
! mA: effects noise only
0
10
20
30
40
50
60
0 200 400 600
Changes in Dose (CTDIw) as a Function of mAs
CTDIw Head (mGy) CTDIw Body (mGy)
Fixed kVp
Dos
e (m
Gy)
mAs

Use automatic tube current modulation CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring

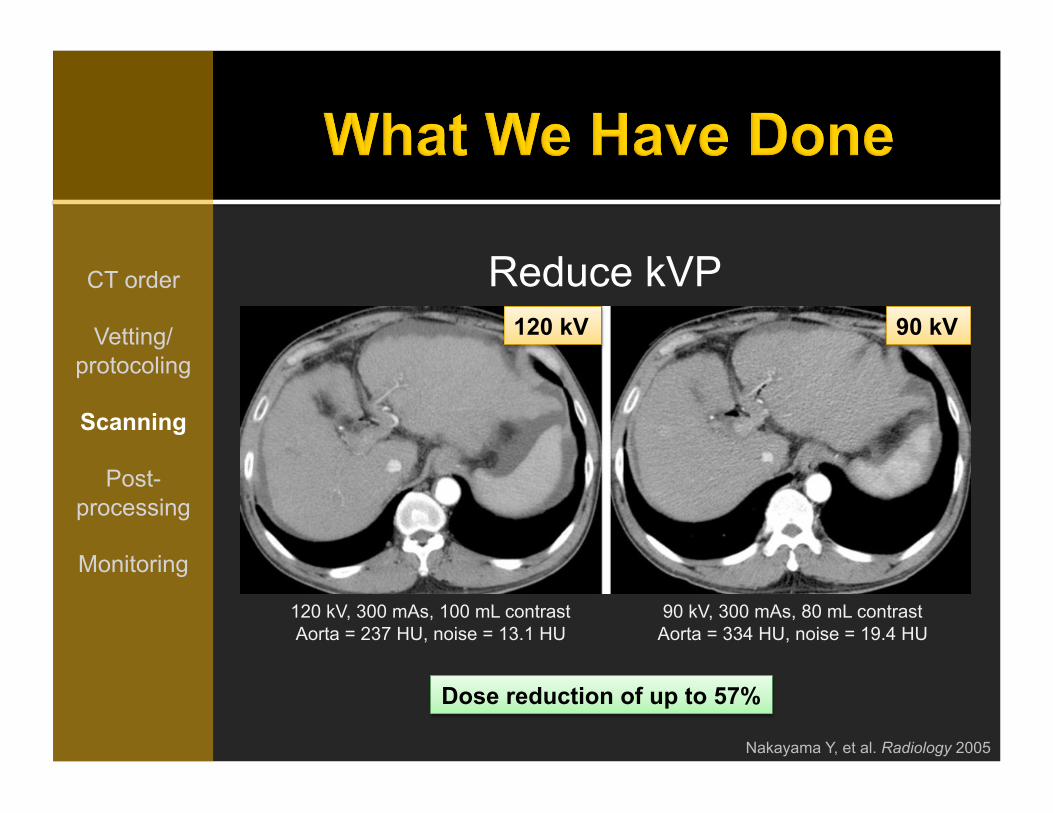
" Reduce kVP (esp for CTA, stone protocol)
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
! Effect on both noise and attenuation
0
10
20
30
40
50
60
0 50 100 150
Changes in CTDIw as a Function of kVp
CTDIw Head (mGy) CTDIw Body (mGy)
Fixed mAs

Reduce kVP CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
Reduce kVP CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
120 kV, 300 mAs, 100 mL contrast Aorta = 237 HU, noise = 13.1 HU
90 kV, 300 mAs, 80 mL contrast Aorta = 334 HU, noise = 19.4 HU
Dose reduction of up to 57%
120 kV 90 kV
Nakayama Y, et al. Radiology 2005

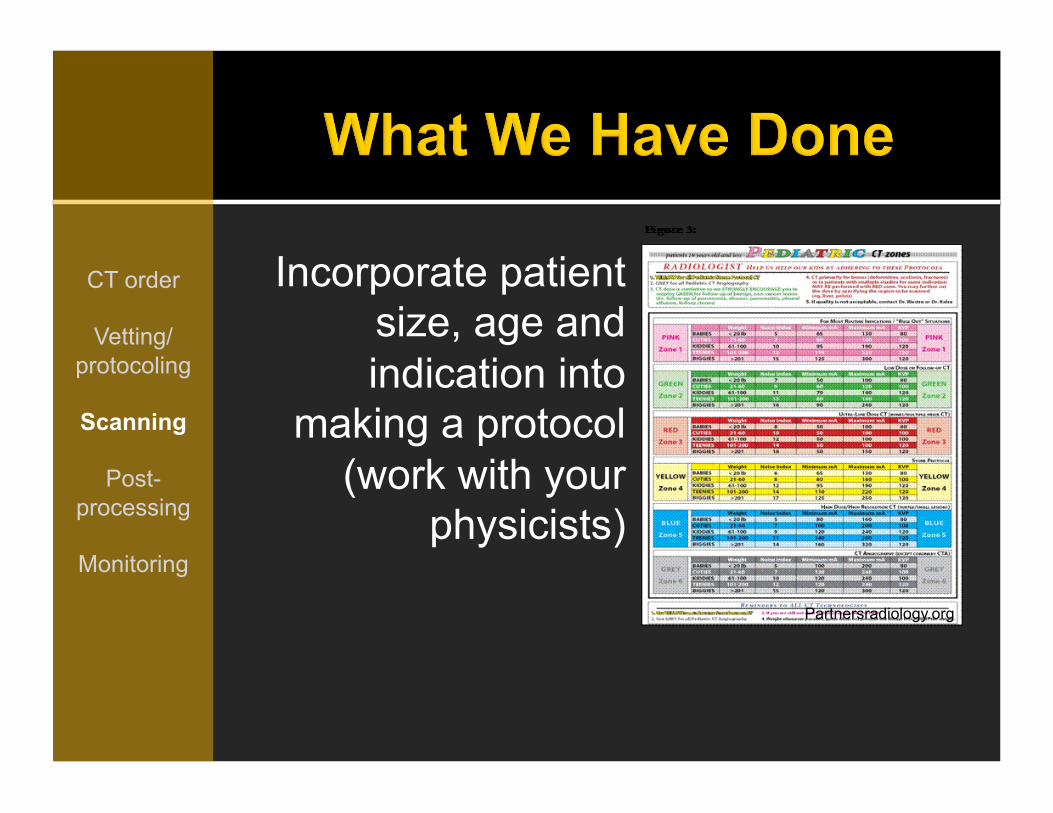
Incorporate patient size, age and indication into making a protocol (work
with your physicists)
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
! Image noise increases with less kVp but noise is less in smaller phantoms
Seigel MJ, et al. Radiology 2004
Incorporate patient size, age and indication into
making a protocol (work with your
physicists)
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
Partnersradiology.org
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
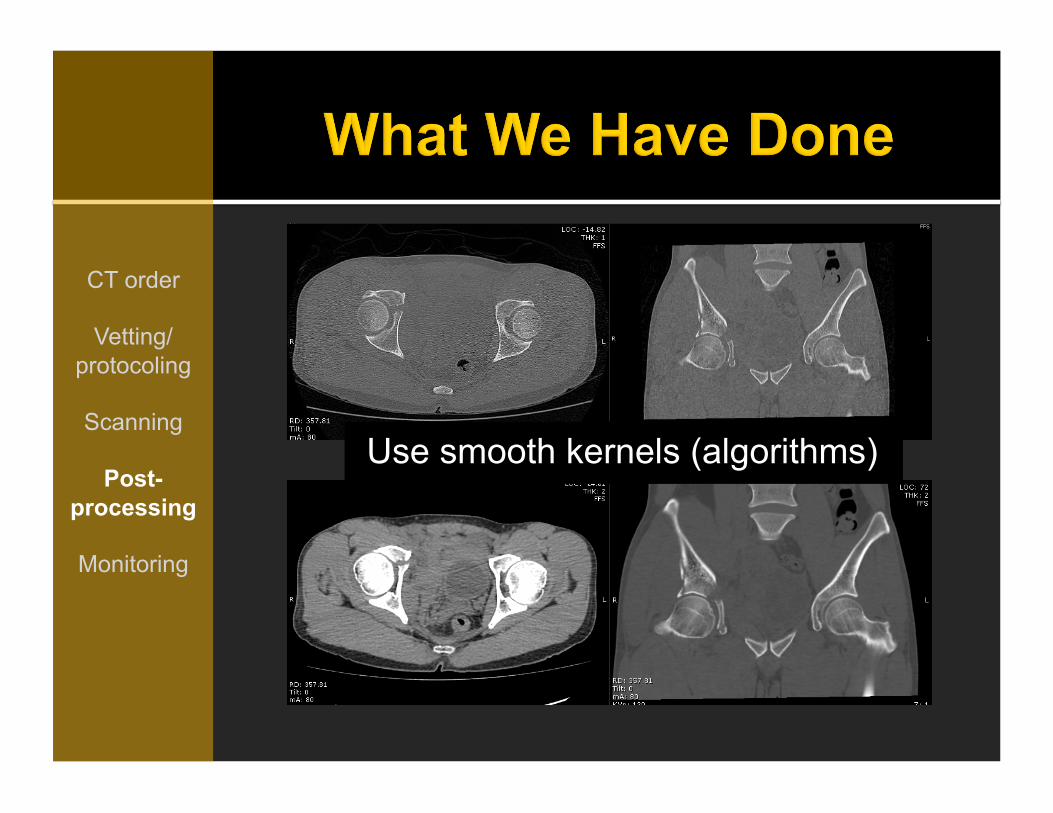
Use smooth kernels (algorithms)
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
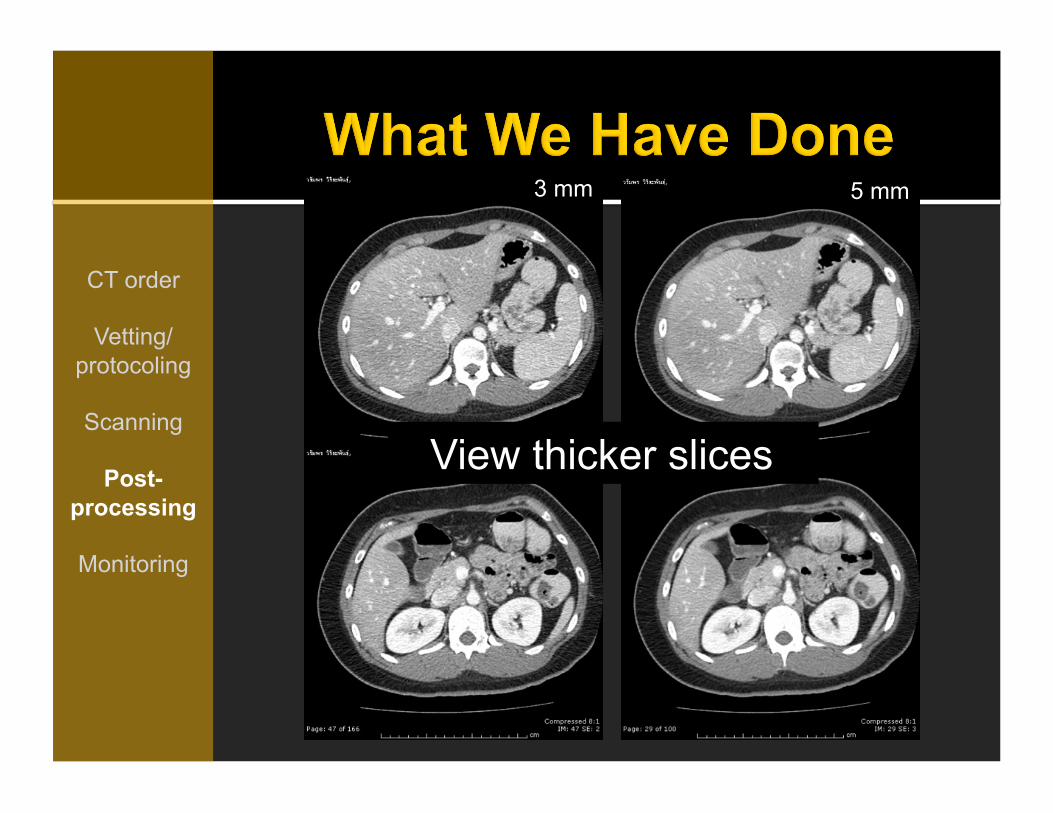
5 mm 3 mm
View thicker slices
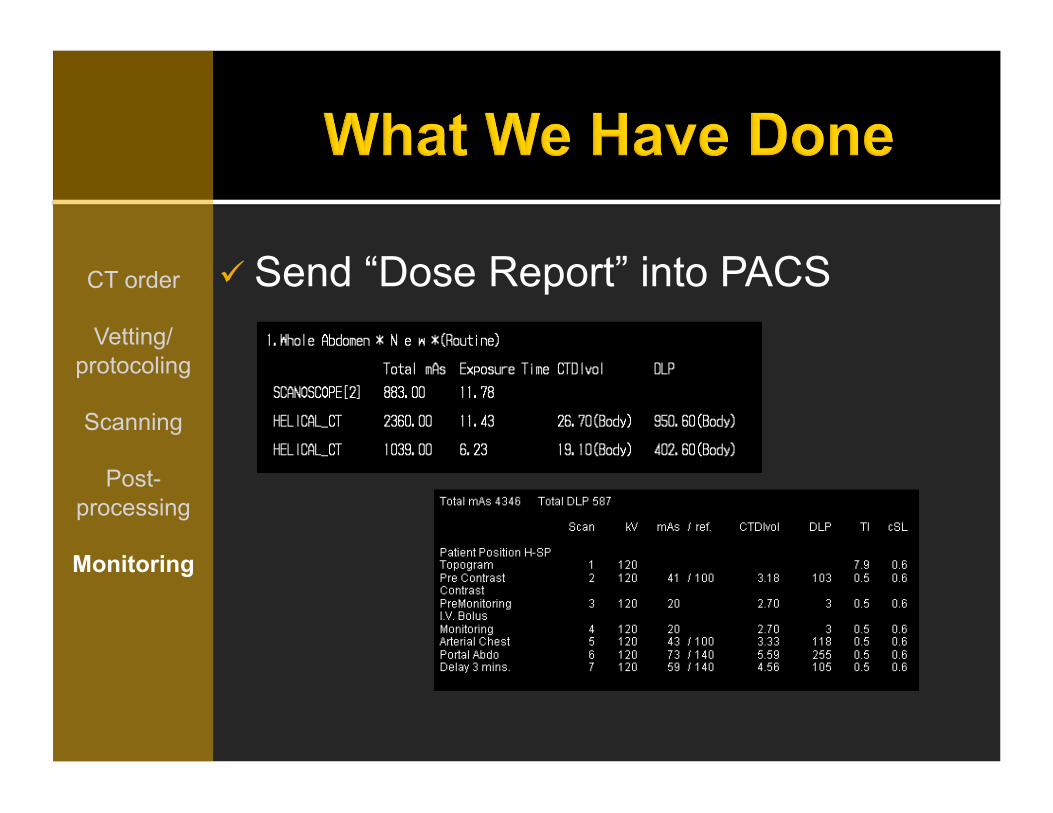
" Send “Dose Report” into PACS CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring

" Educate radiologists and trainees about dose parameters and standards
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring

" Regular updates of CT protocols CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
libraries.psu.edu

o Use decision support tools
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
Sanjay Saini, MD. MGH Sistrom CL et al. Radiology 2009

Systemwide tackle of defensive medicine and self referral
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
Texler.deviantart.com

Streamlined vetting and protocoling processes
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
Claimruler.com
Managingamericans.com

CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring
Color zones: - Pink = routine, R/O situation - Green = F/U CT with one prior - Red = bone evaluation or multiple priors - Yellow = kidney stone - Blue = subtle or small lesions suspected or identified with other imaging - Gray = vascular assessment with CTA
kVp mA Noise Index
Singh S, et al. Radiology 2009

Use iterative reconstruction
(IR)
CT order
Vetting/protocoling
Scanning
Post-processing
Monitoring

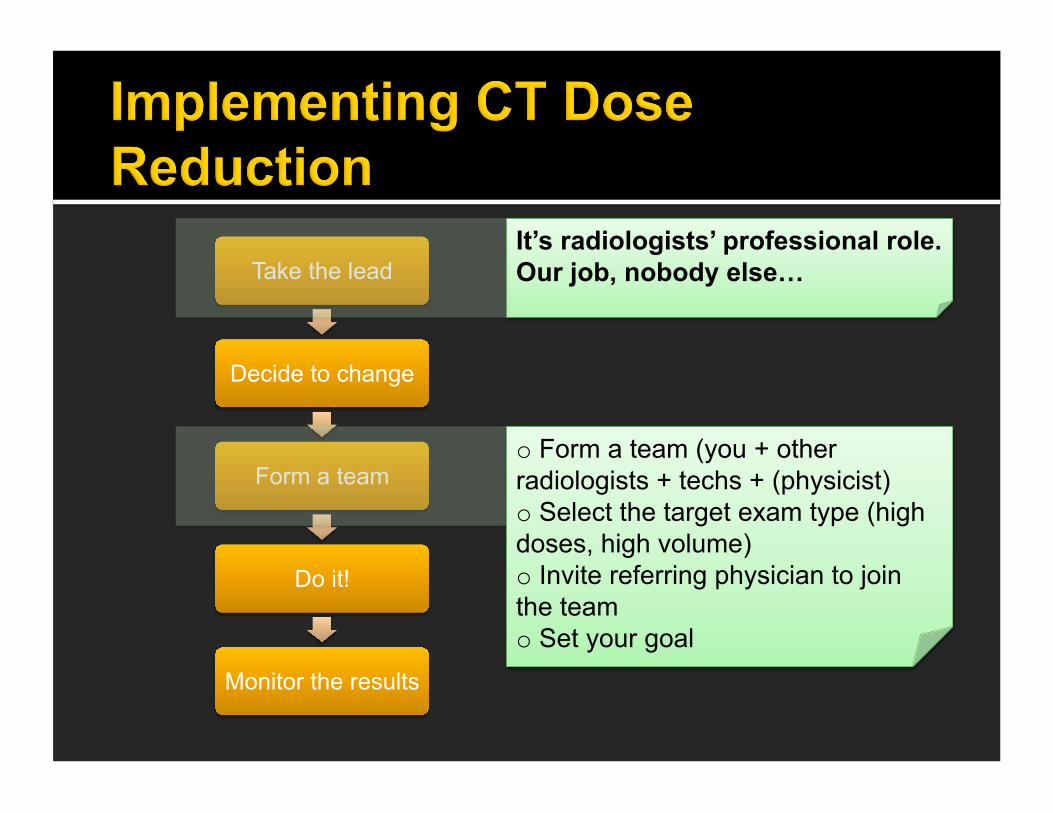
Take the lead
Decide to change
Form a team
Do it!
Monitor the results
It’s radiologists’ professional role. Our job, nobody else…
o Tell technologists to send dose report to PACS o Check 10-20 reports of all organ systems o Compare your doses with standard DRLs o Convince your Superior/Head
Take the lead
Decide to change
Form a team
Do it!
Monitor the results
It’s radiologists’ professional role. Our job, nobody else…
o Form a team (you + other radiologists + techs + (physicist) o Select the target exam type (high doses, high volume) o Invite referring physician to join the team o Set your goal
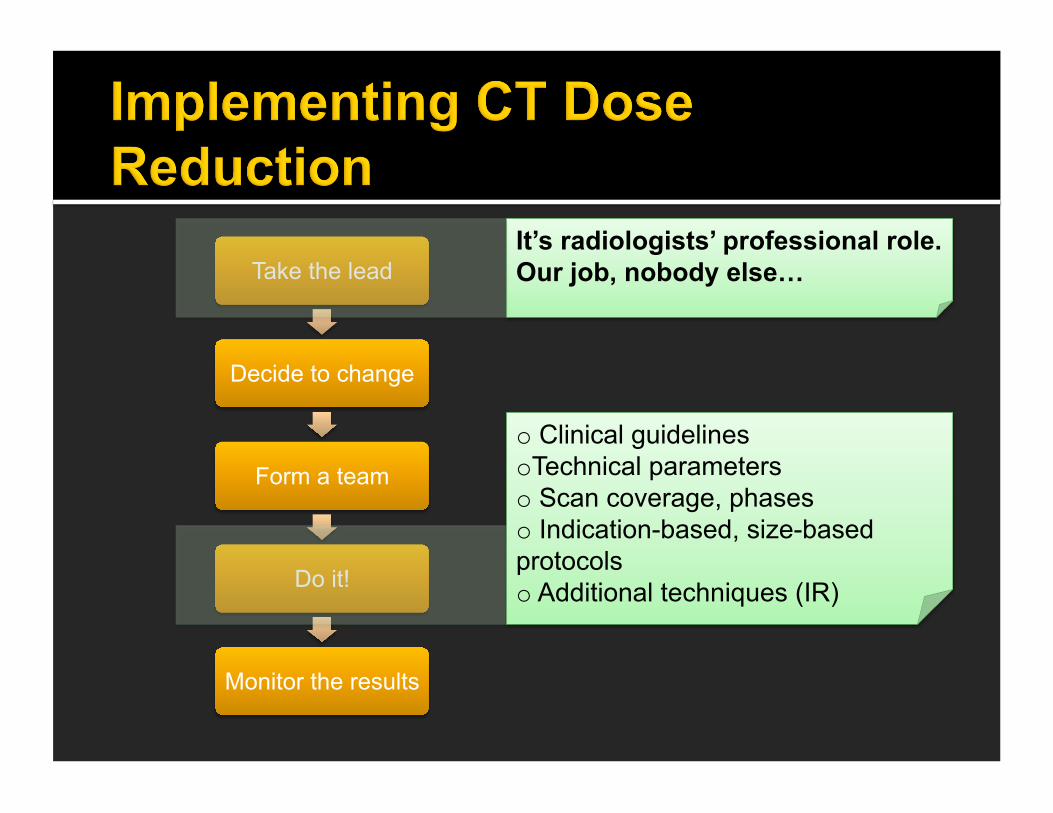
Take the lead
Decide to change
Form a team
Do it!
Monitor the results
It’s radiologists’ professional role. Our job, nobody else…
o Clinical guidelines o Technical parameters o Scan coverage, phases o Indication-based, size-based protocols o Additional techniques (IR)
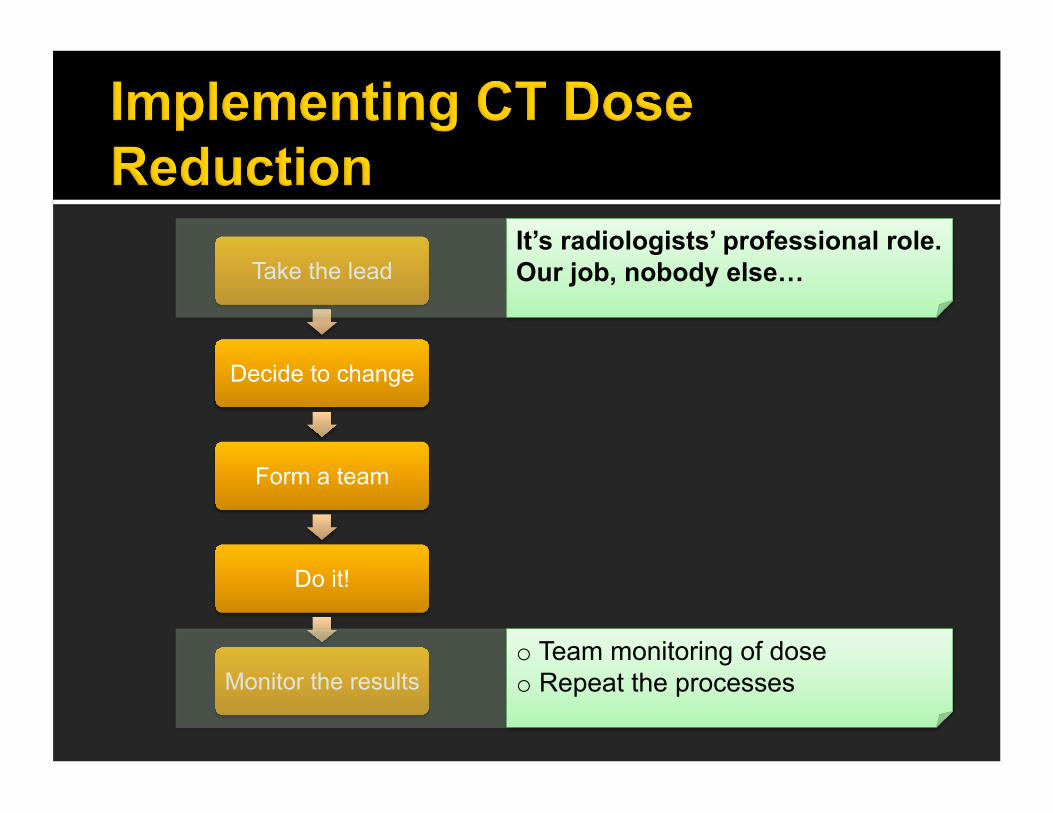
Take the lead
Decide to change
Form a team
Do it!
Monitor the results
It’s radiologists’ professional role. Our job, nobody else…
o Team monitoring of dose o Repeat the processes
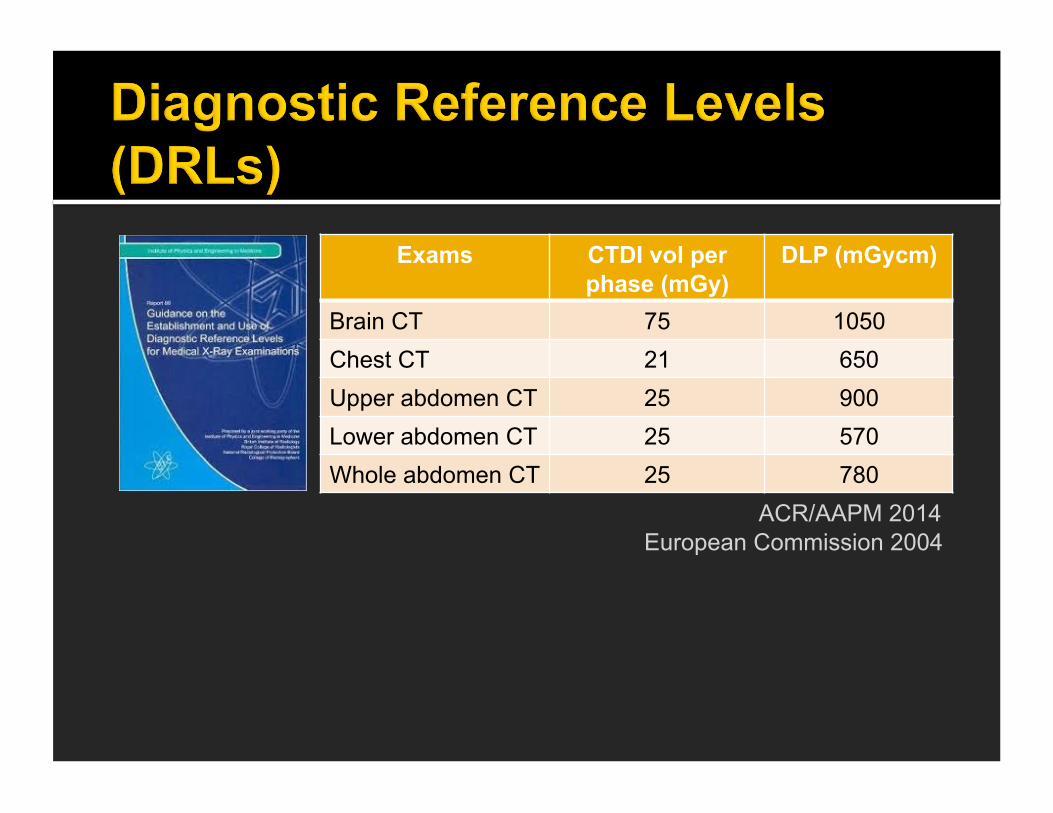
Exams CTDI vol per phase (mGy)
DLP (mGycm)
Brain CT 75 1050 Chest CT 21 650 Upper abdomen CT 25 900 Lower abdomen CT 25 570 Whole abdomen CT 25 780
ACR/AAPM 2014 European Commission 2004

! Estimated dose x conversion factor = SSDE
! Closer to “real” dose ! Thinner patients get more dose
compared with obese patients of the same DLP
! Based on our own unpublished data, SSDE is 30%+ that of estimated dose
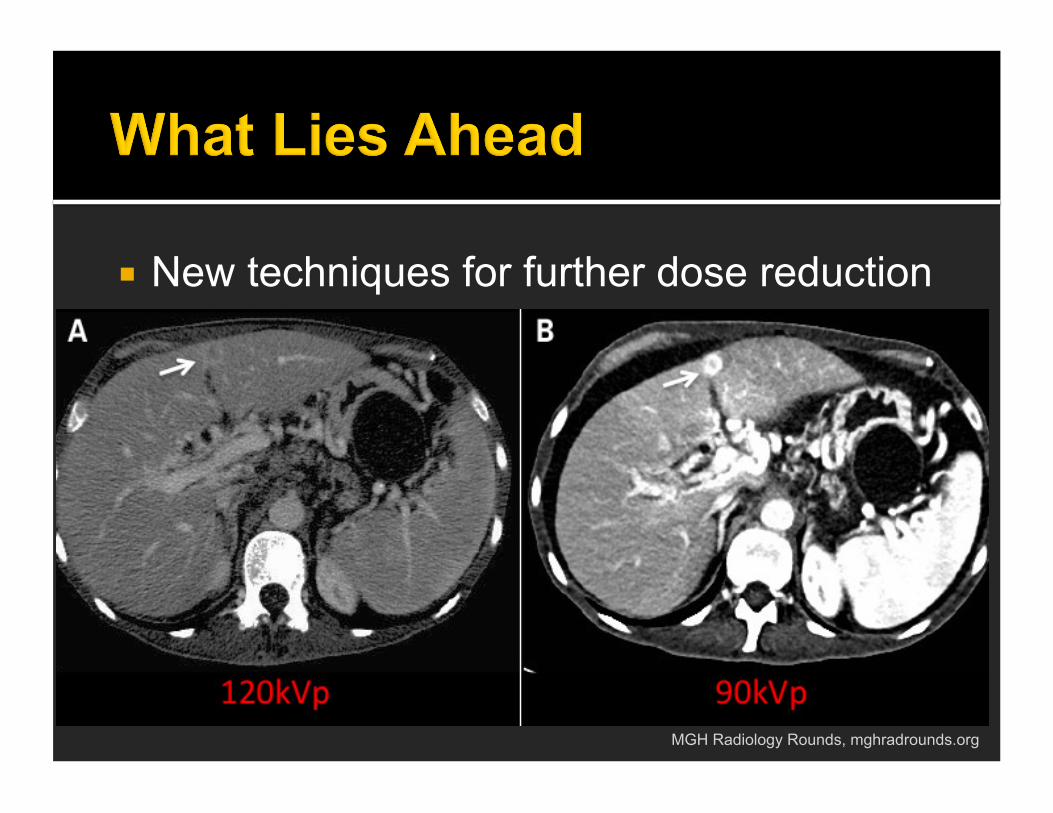
! New techniques for further dose reduction
MGH Radiology Rounds, mghradrounds.org
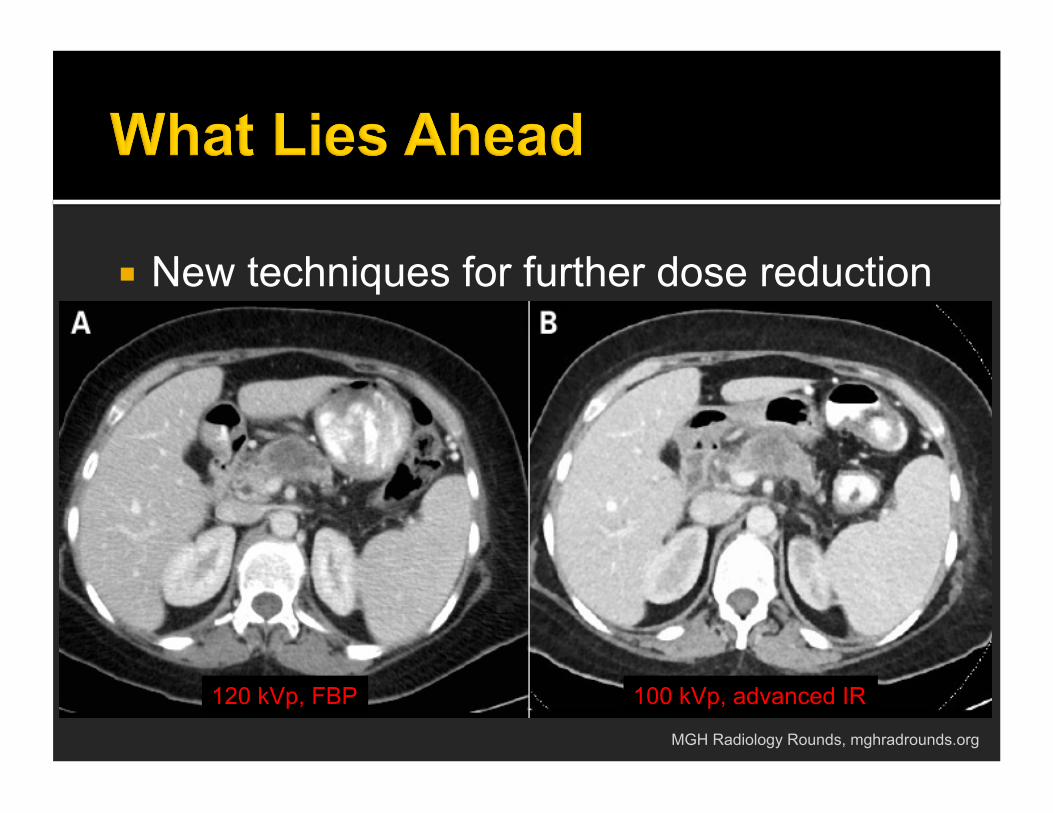
! New techniques for further dose reduction
MGH Radiology Rounds, mghradrounds.org
120 kVp, FBP 100 kVp, advanced IR

! 1- and sub-mSv scan
MGH Radiology Rounds, mghradrounds.org
! It is not a “choice” to reduce CT radiation. As a radiologist, it is a responsibility to our patients
! No more best-looking images. Images should be “enough for diagnostic purpose”
! Multiphase CT should not be “routine”. ! CT dose is manageable: take a lead, make
a decision, form a team and “just do it”.
Related Documents











