PEDIATRIC ANNALS 39:1 | JANUARY 2 010 www.PediatricSuperSite.com | 15 Croup: Common Syndromes and Therapy D iseases resulting in airway com- promise are the leading cause of cardiac arrest in children. 1 The narrowest portion of the pediatric airway (in those younger than 10 years) is at the level of the cricoid cartilage, termed the subglottis, just below the vocal cords. This anatomic feature makes children more susceptible to airway obstruction from infectious diseases than adults. 1. Delineate th e diffe rential diagnos is of croup in children. 2. Review the clinical evidence support- ing the use of nebulized epineph- rine for croup in the emergency department, as well as the criteria for discharge home after treatment. 3. Discuss the clinical evidence supporting the use of systemic or nebulized steroids in the treatment of viral laryngotracheobronchitis . Eric L. Wald, MD, is with the Division of Critical Care Medicine, Northwestern University, Chicago. Addr ess co rrespon den ce to: E ric L. Wal d, MD, 2300 Children’s Plaza, Box 73, Chicago, IL 60614; fax: 773-880-6300; e-mail EWald@ childrensmemorial.org. Dr. Wald has disclosed no relevant finan- cial relationships. doi: 10.3928/00904481-2 0091210-04 EDUCATIONAL OBJECTIVES C M E Eric L. Wald, MD © i S t o c k p h o t o . c o m C M E 3901EWald croup indd 15 3901EWald.croup.indd 15 1/6/2010 2:38:09 PM 1/6/2010 2:38:09 PM

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 1/8
PEDIATRIC ANNALS 39:1 | JANUARY 2010 www.PediatricSuperSite.com | 15
Croup: Common Syndromes and Therapy
Diseases resulting in airway com-
promise are the leading cause of
cardiac arrest in children.1 The
narrowest portion of the pediatric airway
(in those younger than 10 years) is at the
level of the cricoid cartilage, termed the
subglottis, just below the vocal cords.
This anatomic feature makes children
more susceptible to airway obstruction
from infectious diseases than adults.
1. Delineate the differential diagnosisof croup in children.
2. Review the clinical evidence support-ing the use of nebulized epineph-rine for croup in the emergencydepartment, as well as the criteria fordischarge home after treatment.
3. Discuss the clinical evidencesupporting the use of systemic ornebulized steroids in the treatmentof viral laryngotracheobronchitis.
Eric L. Wald, MD, is with the Division
of Critical Care Medicine, Northwestern
University, Chicago.
Address correspondence to: Eric L. Wald,
MD, 2300 Children’s Plaza, Box 73, Chicago,
IL 60614; fax: 773-880-6300; e-mail EWald@
childrensmemorial.org.
Dr. Wald has disclosed no relevant finan-
cial relationships.
doi: 10.3928/00904481-20091210-04
EDUCATIONAL OBJECTIVESCM E
Eric L. Wald, MD
© i S
t o c k p h
o t o . c
o m
CM E
3901EWald croup indd 153901EWald.croup.indd 15 1/6/2010 2:38:09 PM1/6/2010 2:38:09 PM

8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 2/8
16 | www.PediatricSuperSite.com PEDIATRIC ANNALS 39:1 | JANUARY 2010
Because airway resistance is inversely
proportional to the fourth power of the
radius, minimal reductions in cross-sec-
tional area of the airway secondary to in-
flammation or edema can exponentially
increase airway resistance, as well as
work of breathing.
The term “croup” describes a constel-
lation of mainly acute and infectious ill-
nesses characterized by varying degrees
of barking cough, hoarseness, inspira-
tory stridor, and respiratory distress.
Most clinicians use the term “laryngo-
tracheitis” or “laryngotracheobronchi-
tis” for the most common form of croup
in which involvement of the larynx is
enough to produce typical symptoms,
and they reserve the term “laryngotra-
cheobronchopneumonitis” for more se-
vere disease that extends into the lower
airways. A distinction is made between
spasmodic croup, an entity thought to
have an allergic component that rarely
requires treatment, and laryngotrache-
itis, which is thought always to have an
infectious etiology. All these terms de-
scribe inflammation of the vocal cords
and structures inferior to the cords. In-
flammation of structures superior to the
cords, such as the epiglottis, arytenoids,
and aryepiglottic folds, is termed “su-
praglottitis.” All of these processes are
similar enough to consider them withinthe spectrum of a single disease. The
discussion here focuses on the history,
epidemiology, pathogenesis, clinical
presentation, and management of croup
illnesses: epiglottitis, laryngotracheitis
[including laryngotracheobronchitis
(LTB) and laryngotracheobronchopneu-
monitis], and bacterial tracheitis. Clas-
sification and clinical characteristics are
shown in Table 1 (see page 17).
EPIDEMIOLOGY
Croup occurs in children younger
than 6 years, with a peak incidence from7 to 36 months.2 Approximately 5% of
children have croup during the second
year of life. The incidence in boys is 1.4
to 2 times higher than in girls.2 Longi-
tudinal croup studies have described
a biennial mid-autumn peak in North
America, occurring in odd years, which
correlates with the prevalence of para-
influenza virus infection, as well as an
annual summer trough.3,4 The most fre-
quent etiologic agents include parain-
fluenza viruses (types 1-3), respiratory
syncytial virus, influenza viruses A and
B, and adenovirus, while Mycoplasma
pneumoniae, herpes simplex type I,
measles, and varicella have also been
reported. Human metapneumovirus and
human coronavirus HL-63 are two new-
ly described pathogens that are strongly
associated with croup in children.5
CLINICAL PRESENTATION
Patients with laryngotracheitis com-
monly present with 1 to 3 days of nonspe-
cific upper respiratory tract symptoms,
with progression to the characteristic
barking cough, stridor, and respiratory
distress. Symptom onset is abrupt and
typically occurs during nighttime hours.
Several hypotheses exist to explain the
nighttime onset, including nocturnal
airway cooling, gastroesophageal re-
flux and concomitant inflammation, and
the effect of nadir levels of cycling en-
dogenous substances, such as cortisol
and epinephrine.6,7
Inspiratory stridoris most common, with biphasic stridor
suggesting a more severe or fixed ob-
struction. Low-grade fever is often pres-
ent. Tachypnea, retractions, hypoxia, or
desaturation are often ominous signs of
worsening obstruction and impending
respiratory failure.
DIFFERENTIAL DIAGNOSIS
Children with classic croup symp-
toms are readily diagnosed, but clini-
cians must be cognizant that there may
be progression of infection into the tra-
chea and lower airways. Furthermore,there are several other acute obstructive
disease processes that occur in the lar-
ynx and are also present with stridor and
respiratory distress (see Sidebar). First
described in 1878 by Michel as angina
epiglottidea anterior, epiglottitis in chil-
dren has become a rarity since the intro-
duction of Hemophilus influenzae type
b (Hib) conjugate vaccines in 1991.8 It
represents a bacterial infection of the su-
praglottic structures in which worsening
edema forces the epiglottis posteriorly,
causing airway obstruction. Epiglottitis
usually occurs in patients 2 to 8 years,
although the average age is increas-
ing as is the ratio of adult to pediatric
cases since the introduction of the Hib
vaccine.9 Despite a sharp drop in inci-
dence, H. influenzae is still seen second-
ary to vaccine failure and in unimmu-
nized children. Group A beta hemolytic
Streptococcus is now the leading cause
of epiglottitis, although its absolute
frequency has not increased. Staphy-
lococci, pneumococci, moraxella, and
candida species, as well as many other
bacteria and viruses, have been isolated
from surface cultures of the epiglottis.
Children usually have rapid onset of
symptoms and present with throat pain,
a muffled, “hot potato” voice, fever, irri-
SIDEBAR.
Differential Diagnosisof Acute Laryngeal
Obstruction
• Acute laryngotracheitis
• Spasmodic croup
• Epiglottitis
• Bacterial tracheitis
• Foreign body aspiration(tracheal and esophageal)
• Laryngeal inflammation caused
by thermal injury
• Angioneurotic edema
• Allergic reaction
• Retropharyngeal abscess
• Peritonsillar abscess
• Neoplasm/hemangioma
• Vocal cord paresis/paralysis
• Laryngeal diphtheria
CM E
3901EWald croup indd 163901EWald.croup.indd 16 1/6/2010 2:38:11 PM1/6/2010 2:38:11 PM
8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 3/8
PEDIATRIC ANNALS 39:1 | JANUARY 2010 www.PediatricSuperSite.com | 17
TABLE 1.
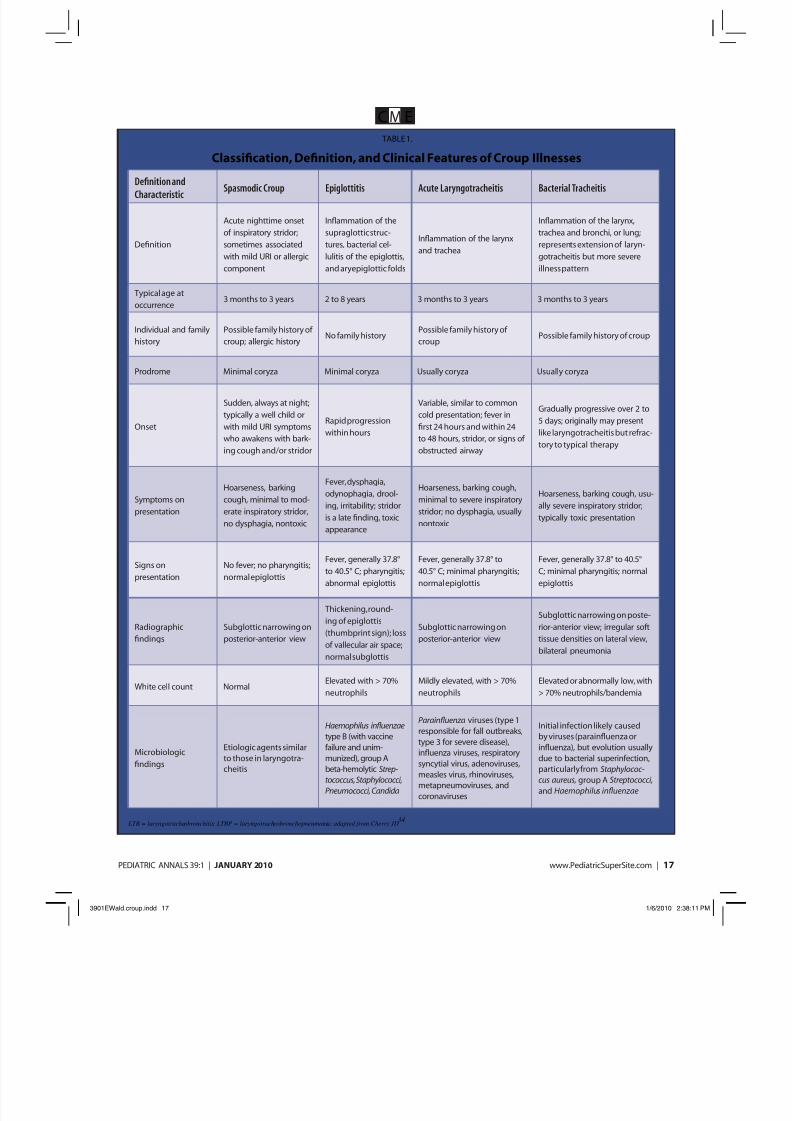
Classification, Definition, and Clinical Features of Croup Illnesses
Definition and
CharacteristicSpasmodic Croup Epiglottitis Acute Laryngotracheitis Bacterial Tracheitis
Definition
Acute nighttime onset
of inspiratory stridor;
sometimes associated
with mild URI or allergic
component
Inflammation of the
supraglottic struc-
tures, bacterial cel-
lulitis of the epiglottis,
and aryepiglottic folds
Inflammation of the larynx
and trachea
Inflammation of the larynx,
trachea and bronchi, or lung;
represents extension of laryn-
gotracheitis but more severe
illness pattern
Typical age at
occurrence3 months to 3 years 2 to 8 years 3 months to 3 years 3 months to 3 years
Individual and family
history
Possible family history of
croup; allergic historyNo family history
Possible family history of
croupPossible family history of croup
Prodrome Minimal coryza Minimal coryza Usually coryza Usually coryza
Onset
Sudden, always at night;
typically a well child or
with mild URI symptoms
who awakens with bark-
ing cough and/or stridor
Rapid progression
within hours
Variable, similar to common
cold presentation; fever in
first 24 hours and within 24
to 48 hours, stridor, or signs of
obstructed airway
Gradually progressive over 2 to
5 days; originally may present
like laryngotracheitis but refrac-
tory to typical therapy
Symptoms on
presentation
Hoarseness, barking
cough, minimal to mod-
erate inspiratory stridor,
no dysphagia, nontoxic
Fever, dysphagia,
odynophagia, drool-
ing, irritability; stridor
is a late finding, toxic
appearance
Hoarseness, barking cough,
minimal to severe inspiratory
stridor; no dysphagia, usually
nontoxic
Hoarseness, barking cough, usu-
ally severe inspiratory stridor;
typically toxic presentation
Signs on
presentation
No fever; no pharyngitis;
normal epiglottis
Fever, generally 37.8°
to 40.5° C; pharyngitis;
abnormal epiglottis
Fever, generally 37.8° to
40.5° C; minimal pharyngitis;
normal epiglottis
Fever, generally 37.8° to 40.5°
C; minimal pharyngitis; normal
epiglottis
Radiographic
findings
Subglottic narrowing on
posterior-anterior view
Thickening, round-
ing of epiglottis
(thumbprint sign); loss
of vallecular air space;
normal subglottis
Subglottic narrowing on
posterior-anterior view
Subglottic narrowing on poste-
rior-anterior view; irregular soft
tissue densities on lateral view,
bilateral pneumonia
White cell count NormalElevated with > 70%
neutrophils
Mildly elevated, with > 70%
neutrophils
Elevated or abnormally low, with
> 70% neutrophils/bandemia
Microbiologic
findings
Etiologic agents similarto those in laryngotra-cheitis
Haemophilus influenzae type B (with vaccinefailure and unim-munized), group Abeta-hemolytic Strep-
tococcus, Staphylococci,Pneumococci, Candida
Parainfluenza viruses (type 1responsible for fall outbreaks,type 3 for severe disease),influenza viruses, respiratorysyncytial virus, adenoviruses,
measles virus, rhinoviruses,metapneumoviruses, andcoronaviruses
Initial infection likely causedby viruses (parainfluenza orinfluenza), but evolution usuallydue to bacterial superinfection,particularly from Staphylococ-
cus aureus, group A Streptococci, and Haemophilus influenzae
LTB = laryngotracheobronchitis; LTBP = laryngotracheobronchopneumonia; adapted from Cherry JD34
CM E
3901EWald croup indd 173901EWald.croup.indd 17 1/6/2010 2:38:11 PM1/6/2010 2:38:11 PM

8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 4/8
18 | www.PediatricSuperSite.com PEDIATRIC ANNALS 39:1 | JANUARY 2010
tability and respiratory distress. Drool-
ing is common secondary to airway ob-
struction and odynophagia. Patients are
usually toxic appearing, often assum-
ing a sniffing position with the chin
thrust forward to open their airway, ora tripod position, leaning forward on
both arms to allow maximal use of ac-
cessory respiratory muscles. Notably, a
croupy cough is absent, and stridor is
a late clinical finding. Secondary sites
of infection, such as meningitis, otitis
media, and cellulitis, are present 50%
of the time, and pneumonia is reported
in up to 25% of cases.1,10
If the diagnosis is uncertain after
performance of the history and physi-
cal examination, a lateral radiograph
of the neck can aid in confirmation. In
epiglottitis, the lateral neck radiograph
often reveals a swollen and edematous
epiglottis (thumbprint sign), with loss
of the vallecular air space.
Once epiglottitis is suspected, a mul-
tidisciplinary team should be assembled,
including pediatric intensive care physi-
cians, anesthesiologists, and otolaryn-
gologists. To confirm the diagnosis, the
child should proceed to the operating
room for anesthesia, to obtain intrave-
nous access, and to perform laryngosco-
py with direct visualization and airway
placement. It is recommended that per-
sonnel be available to perform an emer-
gency tracheostomy if an airway cannot
be secured with an endotracheal tube.
Once the airway is secure, some prefer
changing the oral endotracheal tube to a
nasotracheal tube for easier positioning,
to minimize secretions and to prevent un-
necessary trauma. Cultures of the blood
and surface of the epiglottis should be
obtained for precise microbiologic diag-nosis. Antibiotics active against H. influ-
enzae type b and group A Streptococcus
should be started; children usually re-
quire intubation for 24 to 72 hours, until
reduction in airway edema occurs.
Another potentially life-threaten-
ing infection that often represents the
evolution of common croup to a more
acute disease is bacterial tracheitis. First
described in the American literature in
1912, it was re-described in 1979.11,12
Jones et al reported eight cases of a dis-
ease that shared features of croup and
epiglottitis. They called it “bacterial
tracheitis.”12 It occurs predominantly in
the fall and winter months in children 6
months to 6 years but has been reported
in older children. The most common
etiologic agent isolated is S. aureus, but
other pathogens, such as H. influenzae,
alpha-hemolytic Streptococcus, group A
Streptococcus, moraxella species, and
pneumococci, have also been reported.
Most view the disease as a complication
of viral laryngotracheitis in which injury
to respiratory epithelium predisposes to
bacterial superinfection.
The clinical presentation of bacterial
tracheitis is not as rapid as epiglottitis;
children usually have a mild to moder-
ate illness (typical of classic viral croup)
for several days before an acute change
or decompensation is noted. High fever,
productive cough, and a toxic appear-
ance is common, without odynophagia
or drooling. These last two features
are useful in differentiating bacterialtracheitis from epiglottitis. These pa-
tients often have an increased oxygen
requirement but respond poorly to
therapies, such as racemic epinephrine
and steroids that are aimed at reducing
airway edema. About 60% to 80% of
these children will require endotracheal
intubation and respiratory support due
to thick tracheal secretions that are the
cause of the obstruction.13,14 At the time
of endoscopy for intubation, subglottic
edema, thick inflammatory exudates,
mucosal ulceration, and sloughed mu-
cosa are observed. A bacterial culture
of tracheal secretions and a viral cul-
ture of the pharynx should be obtained
at the time of intubation to help guide
therapy. Concurrent sites of infection
are seen often with up to 60% of pa-
tients also having pneumonia.1 Lateral
neck x-rays can aid in diagnosis, reveal-
ing a hazy tracheal air column and soft
densities representing purulent material
or pseudomembranes. Treatment con-
sists of close airway monitoring and in-
travenous antibiotics active against the
common pathogens for 10 to 14 days.
A recent study found that bacterial tra-
cheitis was three times more likely to
cause respiratory failure than croup and
epiglottitis combined.14
TABLE 2.
Assessment of the Severity of Croup*
Level of Severity Characteristics
Mild Occasional barking cough, no audible stridor at rest, no chest wall retractions
Moderate Frequent barking cough, audible st ridor at rest, mi ld che st wa ll retra ctions at rest but no agitat ion
Severe Frequent barking cough, prominent stridor, tachypnea, and marked chest wall retractions; agitation and/or distress
Impending respiratory failureFrequent barking cough, stridor at rest, chest wall retractions (cough, stridor, retractions may not be prominent
due to increasing fatigue/airway compromise), lethargy or decreased level of consciousness, cyanosis
*Adapted from the Alberta Medical Association16
CM E
3901EWald croup indd 183901EWald.croup.indd 18 1/6/2010 2:38:12 PM1/6/2010 2:38:12 PM

8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 5/8
PEDIATRIC ANNALS 39:1 | JANUARY 2010 www.PediatricSuperSite.com | 19
Other rare causes of stridor in chil-
dren presenting with croup-like symp-
toms include foreign body aspiration,
peritonsillar or retropharyngeal abscess,
angioneurotic edema, and laryngealdiphtheria. In foreign body aspiration,
there is usually a history of aspiration,
and symptoms are acute in onset, with-
out signs of prodrome or local or sys-
temic infection. Deep neck space infec-
tions tend to be preceded by viral upper
respiratory tract infections and a high
index of clinical suspicion is necessary
to diagnose them. Clinical findings, such
as fever, neck pain and swelling, and tor-
ticollis, are common, whereas signs of
airway obstruction, such as wheezing
and stridor, are relatively rare initially.
Drooling, limitation in neck movement,and cervical lymphadenopathy are other
presenting signs that may prompt medi-
cal attention. Angioedema or allergic
reactions are often associated with an
offending allergen, have an acute on-
set, and may be accompanied by other
findings, such as swollen lips and facial
tissue or urticarial rash. Finally, in the
unimmunized pediatric population, la-
ryngeal diphtheria must always be con-
sidered. Although there have been no
cases in the United States since 2003,
diphtheria still occurs in Asia, Africa,
and the former Soviet Union. It presents
with all of the hallmarks of laryngotra-
cheitis, but a membranous pharyngitis is
notable on physical examination.
ASSESSMENT OF SEVERITY
The diagnosis of croup usually re-
lies solely on astute clinical assessment.
The best known croup severity score,
the Westley score, evaluates five com-
ponents in the child with respiratory
distress: air entry, stridor, cyanosis, re-
tractions, and level of consciousness.15
In recent years, a more clinically use-
ful severity scale and clinical practice
guidelines were developed by the Alber-
ta Clinical Practice Guideline Working
Group.16 Based on this scale, less than
1% of children seen in 21 emergency
departments in Alberta, Canada, had se-
vere croup, while 85% of children had
mild croup17 (see Table 2, page 18).
TREATMENT
Despite the large body of anecdotal
testimonials supporting humidified air for
croup syndromes, there is no evidence-
based medicine to support its use. Sev-
eral randomized, controlled trials showed
no difference among groups in terms
of croup score, need for epinephrine or
steroid treatment, or need for additional
medical care or hospital admission.18,19
Corticosteroid Therapy
Until recently, a controversial is-
sue surrounding the treatment of croup
— corticosteroid therapy — is now uni-
formly recommended for croup of all lev-
els of severity. Meta-analyses of 37 trials
revealed lower croup scores at 6 hours
postmedication, a decrease in return vis-
its (in some cases up to 50% reduction)
and a decrease in time spent during the
emergency room visit or hospitalization.20
These benefits occurred in children with
mild to moderate croup and moderate to
severe croup. There was a fivefold de-
crease in the rate of intubation in children
with severe croup (or impending respira-
tory failure) among those who receivedsteroids.21 In children already intubated,
one-third less time was spent on the ven-
tilator, and there was a sevenfold decrease
in frequency of reintubation.22
Corticosteroid trials in croup have
investigated an assortment of drugs,
dosages, and routes of administration.
Single dose dexamethasone [0.6 mg/kg
given orally or intramuscularly (IM)]
has been studied and compared most
frequently. Oral dexamethasone, when
compared with other steroid prepara-
tions, such as oral prednisone, has been
found equivalent or superior in reducingcroup scores and in the rate of return to
medical care.23 Oral and IM administra-
tion of dexamethasone have been com-
pared, and no differences were seen in
reduction of croup scores, escalation of
medical care, return to medical care, or
hospital admission rates.24,25 Oral and
IM routes of administration have also
been compared with inhalational routes
(chiefly comparing inhaled budenoside
with oral dexamethasone) and they were
found to be equivalent. In some cases,
oral and IM routes were found to be su-
perior to inhalation.26,27 At the bedside,
the route of administration of steroid
may vary according to the tolerance of
the child and the associated symptoms
and severity of illness.
Dosing regimens for corticosteroids
have also been evaluated in various stud-
ies. Randomized trials showed the effi-
cacy of a single-dose administration and
multiple-dose administration of steroids
in croup. Because the duration of ac-
tion for a single dose of dexamethasone
is 48 to 96 hours, it seems sufficient to
treat the most common croup symptoms
in children. No studies have performed
outcome analyses comparing single
dose therapy with multiple dose treat-
ment schedules. Randomized, controlled
Corticosteroid trials in
croup have investigated an
assortment of drugs, dosages,
and routes of administration.
CM E
3901EWald croup indd 193901EWald.croup.indd 19 1/6/2010 2:38:12 PM1/6/2010 2:38:12 PM

8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 6/8
20 | www.PediatricSuperSite.com PEDIATRIC ANNALS 39:1 | JANUARY 2010
studies have shown that 0.15 mg/kg of
dexamethasone may be adequate in chil-
dren with croup, although the severity of
illness in those studies was variable.28,29
In contrast, a meta-analysis of severalstudies reported that a higher initial dose
of steroids was associated with clinical
improvement in a larger proportion of
hospitalized croup patients.21
Steroid treatment for croup is gener-
ally thought to be safe, especially when
limited to a single dose. The American
Academy of Pediatrics (AAP) and the
U.S. Food and Drug Administration
(FDA) recommend caution when using
steroids in children exposed to the vari-
cella virus, although there is controversy
about whether inhaled steroids or a sin-
gle systemic dose can be harmful.
Epinephrine
Nebulized epinephrine has been well
studied and is usually reserved for chil-
dren with moderate to severe croup, serv-
ing as a temporary treatment bridge to
allow the steroids to take effect. It likely
works by stimulating the alpha-adrener-
gic receptors in airway mucosa, resulting
in vasoconstriction of precapillary arteri-
oles. This decreases hydrostatic pressure,
allows fluid absorption, and decreases air-
way edema. Racemic epinephrine, a 1:1
mixture of the levo and dextro isomers of
epinephrine, has been used in the United
States since 1971. Early trials of 2.25%
racemic epinephrine (0.5 mL in 2.5 mL
normal saline) administered via intermit-
tent positive pressure breathing showed
reduction of croup severity scores.15,30
Later trials revealed that nebulized ad-
ministration of racemic epinephrine was
an equally effective route for treating air-
way obstruction, improving croup scores
within 10 to 30 minutes.31 Nebulization
of L-epinephrine (1:1000) diluted in 5
mL of saline provides similar efficacy in
children with moderate to severe croup,
although the racemic form is most com-
monly used in the United States.32 Clini-
cal effects last up to 1 to 2 hours, and with
the development of rebound tracheal ede-
ma, patients may return to their baseline
level of distress but rarely worsen.15,33
Repeated doses are often necessary and
have been reported to reduce the needfor intubation in children with severe
croup.34 Prospective studies suggest that
patients receiving epinephrine and ste-
roids may be discharged home safely
from the emergency department after an
observation period of 2 to 4 hours, as long
as their symptoms have not recurred.35,36
If treatment fails to abolish croup symp-
toms, or multiple epinephrine doses have
been used, admission for clinical obser-
vation is warranted.
Although nebulized epinephrine is
generally safe, one case report describes
ventricular tachycardia and myocardial
infarction in a previously healthy child
with severe croup who received three
nebulized treatments within 1 hour.37
Helium
Helium-oxygen mixtures (heliox)
have been demonstrated to be an effective
treatment for upper airway obstruction,
including croup syndromes. Because
the density of helium is one-seventh that
of air, heliox decreases turbulence and
improves gas flow through high-resis-tance airways. A 70:30 helium:oxygen
mixture of heliox was compared with
racemic epinephrine in a small prospec-
tive, randomized, double-blind trial in
hospitalized children with moderate to
severe croup who were already receiv-
ing steroids.38 There was no difference
in the modified croup score between the
two treatment groups. A significant oxy-
gen requirement (greater than 40%) lim-
its the use of heliox, as does its expense
and complexity of setup. It also serves
more as a therapeutic bridge because it
lacks a direct effect on inflamed, edema-tous airways. Heliox can reduce work of
breathing enough to prevent intubation
and allow other medications to reach
therapeutic peak. Heliox has a lower
side effect profile than corticosteroids
and epinephrine, however, and may be
useful in those children in whom those
medications are contraindicated.
Other Treatments
Children experiencing hypoxia with
moderate to severe croup should receive
oxygen therapy. Antitussive and decon-
gestant agents have no role in the treat-
ment of croup illnesses. Antibiotics are
unnecessary in the treatment of laryn-
gotracheitis and spasmodic croup unless
clinical symptoms, laboratory data, or
microbiology support the presence of
secondary bacterial infection. Antiviral
therapy can be considered in cases of in-
fluenza virus infection.
CONCLUSIONS AND FUTURE
CONSIDERATIONS
Croup in its most common form
(laryngotracheitis) is a pediatric respi-
ratory illness that provokes anxiety in
the patient and their parents because of
airway obstruction. Despite anecdotal
evidence, cool mist or humidified air
Heliox can reduce work of
breathing enough to prevent
intubation and allow for
other medications to reach
therapeutic peak.
CM E
3901EWald croup indd 203901EWald.croup.indd 20 1/6/2010 2:38:13 PM1/6/2010 2:38:13 PM

8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 7/8
PEDIATRIC ANNALS 39:1 | JANUARY 2010 www.PediatricSuperSite.com | 21
has not been proven to be effective in
the treatment of croup. Regardless of
the level of illness acuity, corticoste-
roid therapy (0.6 mg/kg dexamethasone
either orally or IM) is now the standardof care. In cases of milder disease, re-
assurance and close outpatient obser-
vation is recommended. Patients with
moderate symptoms or those who fail
to respond to corticosteroids should be
evaluated in an emergency department.
There is evidence to support the use
of epinephrine for short-term relief of
symptoms, and it may be a useful thera-
peutic bridge until the effect of steroids
is realized. In children who appear toxic
or in severe respiratory distress, endos-
copy, blood work, as well as bacterial
and viral cultures, may be useful. Re-peated epinephrine doses and inhaled
helium-oxygen mixture may help avoid
intubation in severe cases. Admission
to the ICU, intravenous antibiotics, and
intubation may be required to support
these children through severe illness.
REFERENCES 1. Jardine DS, Martin LD. Specific Diseases of
the Respiratory System: Upper Airway. In:
Fuhrman BP, Zimmerman J. Pediatric Criti-
cal Care. 3rd ed. Philadelphia, PA: Mosby
Elsevier; 2006:571-587.
2. Denny FW, Murphy TF, Clyde WA, Col-
lier AM, Henderson FW. Croup: an 11-year
study in a pediatric practice. Pediatrics.
1983;71(6):871-876.
3. Segal AO, Crighton EJ, Moineddin R, Mam-
dani M, Upshur RE. Croup hospitalizations in
Ontario: a 14-year time-series analysis. Pedi-
atrics. 2005;116(1):51-55.
4. Marx A, Torok T, Holman R, Clarke M, An-
derson L. Pediatric hospitalizations for croup
(laryngotracheobronchitis): biennial increases
associated with human parainfluenza virus 1 epi-
demics. J Infect Dis. 1997;176(6):1423-1427.
5. van der Hoek L, Sure K, Ihorst G, et al. Human
coronavirus NL63 infection is associated with
croup. Adv Exp Med Biol. 2006;581:485-491.
6. Calhoun W. Nocturnal asthma. Chest.
2003;123(3 Suppl):399-405.
7. Bjornson CL, Johnson DW. Croup. Lancet.
2008;371(9609):329-339.
8. Theisen CF. Angina epiglottidea anterior:
report of three cases. Albany Med Ann.
1900;21:395-405.
9. Shah RK, Roberson DW, Jones DT. Epiglot-
titis in the hemophilus influenza type B vac-
cine era: changing trends. Laryngoscope.
2004;114(3):557-560.
10. Stroud RH, Friedman NR. An update on in-
flammatory disorders of the pediatric airway:
epiglottitis, croup, and tracheitis. Amer J Oto-
laryng. 2001;22(4):268-275.
11. Jackson C. Influenzal tracheitis. Laryngo-
scope. 1912;22:130.
12. Jones R, Santos JI, Overall JC. Bacterial tra-
cheitis. JAMA. 1979;242(8):721-726.
13. Bernstein T, Brilli R, Jacobs B. Is bacterial
tracheitis changing? A 14-month experience
in a pediatric intensive care unit. Clin Infect
Dis. 1998;27(3):458-462.
14. Hopkins A, Lahiri T, Salerno R, Heath B.
Changing epidemiology of life-threaten-
ing upper airway infections: the reemer-
gence of bacterial tracheitis. Pediatrics.
2006;118(4):1418-1421.
15. Westley CR, Cotton EK, Brooks JG. Nebu-
lized racemic epinephrine by IPPB for the
treatment of croup: a double-blind study. Am
J Dis Child. 1978;132(5):484-487.
16. Guideline for the diagnosis and management
of croup. Alberta, ON, Canada: Alberta Medi-
cal Association; 2007.
17. Bjornson CL, Johnson DW. Croup —
treatment update. Pediatr Emerg Care.
2005;21(12):863-873.
18. Moore M, Little P. Humidified air inhalation
for treating croup. Cochrane Database Syst
Rev, 2006;3:CD002870.
19. Scolnik D, Coates AL, Stephens D, Da Silva
Z, Lavine E, Schuh S. Controlled delivery of
high vs low humidity vs mist therapy for croup
in emergency departments: a randomized con-
trolled trial. JAMA. 2006;295(11):1274-1280.
20. Russell K, Wiebe N, Saenz A, et al. Gluco-
corticoids for croup. Cochrane Database Syst
Rev. 2004;1:CD001955.
21. Kairys SW, Olmstead EN, O’Connor GT. Ste-
roid treatment of laryngotracheitis: a meta-
analysis of the evidence from randomized
trials. Pediatrics. 1989;83(5):683-693.
22. Tibballs J, Shann FA, Landau LI. Placebo-con-
trolled trial of prednisolone in children intubated
for croup. Lancet. 1992;340(8822):745-748.
23. Sparrow A, Geelhoed G. Prednisolone versus
dexamethasone in croup: a randomized equiva-
lence trial. Arch Dis Child. 2006;91(7):580-583.
24. Rittichier K, Ledwith C. Outpatient treatment
of moderate croup with dexamethasone: in-
tramuscular versus oral dosing. Pediatrics.
2000;106(6):1344-1348.
25. Donaldson D, Poleski D, Knipple E, et al.
Intramuscular versus oral dexamethasone for
the treatment of moderate-to-severe croup: a
randomized, double-blind trial. Acad Emerg
Med. 2003;10(1):16-21.
26. Geelhoed GC. Budesonide offers no advan-
tage when added to oral dexamethasone in
the treatment of croup. Pediatr Emerg Care.
2005;21(6):359-362.
27. Klassen T, Craig W, Moher D, et al. Nebu-
lized budesonide and oral dexamethasone for
treatment of croup: a randomized controlled
trial. JAMA. 1998;279(20):1629-1632.
28. Geelhoed GC, Macdonald W. Oral dexameth-
asone in the treatment of croup: 0.15 mg/kg
versus 0.3 mg/kg versus 0.6 mg/kg. Pediatr
Pulmonol. 1995;20(6):362-368.
29. Chub-Uppakarn S, Sangsupawanich P. A ran-
domized comparison of dexamethasone 0.15
mg/kg versus 0.6 mg/kg for the treatment of
moderate to severe croup. Internat J Pediatr
Otorhinolaryngol. 2007;71(3):473-477.
30. Taussig LM, Castro O, Beaudry PH, Fox WW,
Bureau M. Treatment of laryngotracheobron-
chitis (croup): use of intermittent positive-
pressure breathing and racemic epinephrine.
Am J Dis Child. 1975;129(7):790-793.
31. Fogel JM, Berg IJ, Gerber MA, Sherter CB.
Racemic epinephrine in the treatment of
croup: nebulization alone versus nebulization
with intermittent positive pressure breathing.
J Pediatr. 1982;101(6):1028-1031.
32. Waisman Y, Klein BL, Boenning DA, et al. Pro-
spective randomized double-blind study com-
paring L-epinephrine and racemic epinephrine
aerosols in the treatment of laryngotracheitis
(croup). Pediatrics. 1992;89(2):302-306.
33. Kristjansson S, Berg-Kelly K, Winso E. Inha-
lation of racemic adrenaline in the treatment
of mild and moderately severe croup: clinical
symptom score and oxygen saturation mea-
surements for evaluation of treatment effects.
Acta Paediatrica. 1994;83(11):1156-1160.
34. Cherry JD. Croup. New Eng J Med.
2008;358(4):384-391.
35. Johnson DW, Jacobson S, Edney P, et al. A
comparison of nebulized budesonide, in-
tramuscular dexamethasone, and placebo
for moderately severe croup. N Engl J Med.
1998;339(8):498-503.
36. Rizos J, DiGravio B, Sehl B, et al. The dis-
position of children with croup treated with
racemic epinephrine and dexamethasone
in the emergency department. J Emer Med.
1998;16(4):535-539.
37. Butte M, Nguyen B, Hutchison T, et al.
Pediatric myocardial infarction after race-
mic epinephrine administration. Pediatrics.
1999;104(1):e9.
38. Weber JE, Chudnofsky CR, Younger JG, et al.
A randomized comparison of helium-oxygen
mixture (Heliox) and racemic epinephrine for
the treatment of moderate to severe croup. Pe-
diatrics. 2001;107(6):E96.
CM E
3901EWald croup indd 213901EWald.croup.indd 21 1/6/2010 2:38:14 PM1/6/2010 2:38:14 PM

8/13/2019 Croup. Sindrome
http://slidepdf.com/reader/full/croup-sindrome 8/8
Reproducedwithpermissionof thecopyrightowner. Further reproductionprohibitedwithoutpermission.
Related Documents











