Epilepsia, 48(5):990–1001, 2007 Blackwell Publishing, Inc. C 2007 International League Against Epilepsy ILAE Commission Report Cross-Country Measures for Monitoring Epilepsy Care ∗ Charles E. Begley, †Gus A. Baker, ‡Ettore Beghi, §James Butler, ¶Daniel Chisholm, ∗∗ John T. Langfitt, ††Pierre Levy, ‡‡Christoph Pachlatko, §§Samuel Wiebe, and ¶¶Karen Lee Donaldson on behalf of the ILAE Commission on Healthcare Policy ∗ School of Public Health, University of Texas, U.S.A.; †Division of Neurosciences, University of Liverpool, Liverpool, United Kingdom; ‡Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy; §Department of Neurology, University of Stellenbosch, Johannesburg, South Africa; ¶ Department of Mental Health and Substance Abuse, World Health Organization, Geneva, Switzerland; ∗∗ Department of Neurology, University of Rochester School of Medicine, Rochester, U.S.A.; ††Place du Marechal de Lattre de Tassigny, Universite Paris-Dauphine, Paris, France; ‡‡Swiss Epilepsy Centre, Switzerland; §§Division of Neurology, Foothills Medical Centre, Calgary, Canada; ¶¶ Epilepsy Action, Leeds, U.K. Summary: Purpose: The International League Against Epilepsy (ILAE) Commission on Healthcare Policy in consulta- tion with the World Health Organization (WHO) examined the applicability and usefulness of various measures for monitoring epilepsy healthcare services and systems across countries. The goal is to provide planners and policymakers with tools to analyze the impact of healthcare services and systems and evaluate efforts to improve performance. Methods: Commission members conducted a systematic lit- erature review and consulted with experts to assess the nature, strengths, and limitations of the treatment gap and resource avail- ability measures that are currently used to assess the adequacy of epilepsy care. We also conducted a pilot study to determine the feasibility and applicability of using new measures to as- sess epilepsy care developed by the WHO including Disability- Adjusted Life Years (DALYs), responsiveness, and financial fair- ness. Results: The existing measures that are frequently used to assess the adequacy of epilepsy care focus on structural or pro- cess factors whose relationship to outcomes are indirect and may vary across regions. The WHO measures are conceptually supe- rior because of their breadth and connection to articulated and agreed upon outcomes for health systems. However, the WHO measures require data that are not readily available in developing countries and most developed countries as well. Conclusion: The epilepsy field should consider adopting the WHO measures in country assessments of epilepsy burden and healthcare performance whenever data permit. Efforts should be made to develop the data elements to estimate the measures. Key Words: Healthcare—Evaluation—International—Survey A major contributor to the global burden of epilepsy is the lack of adequate healthcare services, particularly in de- veloping countries but also in parts of developed countries as well. One of the greatest challenges to health planners and policymakers is obtaining meaningful data to mea- sure these inadequacies at the community or country level. While it is easy to conceptualize indicators that might pro- vide some insights, obtaining the data can be difficult. Relatively simple measures that have been developed to assess the adequacy of epilepsy healthcare at the coun- Accepted October 23, 2006. Address correspondence and reprint requests to Charles E. Beg- ley, School of Public Health, The University of Texas Health Science Center, 1200 Herman Pressler, Houston, Texas 77030, U.S.A. E-mail: [email protected] doi: 10.1111/j.1528-1167.2007.00981.x try level are the treatment gap and availability of key re- sources. These measures have been useful because they provide a basic indication of unmet need and require data that is relatively easy to obtain for most countries. In the 1990s, the World Health Organization (WHO) defined a broader set of healthcare measures to be used across diseases and countries to assess healthcare performance. Disability-Adjusted Life Years (DALYs) is proposed as an indicator of the health effects of healthcare systems. Patients’ perceptions of treatment responsiveness are pro- posed as a measure. Financial fairness defined as health- care spending relative to capacity to pay (CTP) is proposed as a measure. Over the last 3 years, the members of the Interna- tional League Against Epilepsy (ILAE) Commission on Healthcare Policy examined the general strengths and 990

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Epilepsia, 48(5):990–1001, 2007Blackwell Publishing, Inc.C© 2007 International League Against Epilepsy
ILAE Commission Report
Cross-Country Measures for Monitoring Epilepsy Care
∗Charles E. Begley, †Gus A. Baker, ‡Ettore Beghi, §James Butler, ¶Daniel Chisholm,∗∗John T. Langfitt, ††Pierre Levy, ‡‡Christoph Pachlatko, §§Samuel Wiebe,and ¶¶Karen Lee Donaldson on behalf of the ILAE Commission on Healthcare Policy
∗School of Public Health, University of Texas, U.S.A.; †Division of Neurosciences, University of Liverpool, Liverpool, UnitedKingdom; ‡Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy; §Department of Neurology, University of Stellenbosch,
Johannesburg, South Africa; ¶Department of Mental Health and Substance Abuse, World Health Organization, Geneva, Switzerland;∗∗Department of Neurology, University of Rochester School of Medicine, Rochester, U.S.A.; ††Place du Marechal de Lattre deTassigny, Universite Paris-Dauphine, Paris, France; ‡‡Swiss Epilepsy Centre, Switzerland; §§Division of Neurology, Foothills
Medical Centre, Calgary, Canada; ¶¶Epilepsy Action, Leeds, U.K.
Summary: Purpose: The International League AgainstEpilepsy (ILAE) Commission on Healthcare Policy in consulta-tion with the World Health Organization (WHO) examined theapplicability and usefulness of various measures for monitoringepilepsy healthcare services and systems across countries.The goal is to provide planners and policymakers with toolsto analyze the impact of healthcare services and systems andevaluate efforts to improve performance.
Methods: Commission members conducted a systematic lit-erature review and consulted with experts to assess the nature,strengths, and limitations of the treatment gap and resource avail-ability measures that are currently used to assess the adequacyof epilepsy care. We also conducted a pilot study to determinethe feasibility and applicability of using new measures to as-sess epilepsy care developed by the WHO including Disability-
Adjusted Life Years (DALYs), responsiveness, and financial fair-ness.
Results: The existing measures that are frequently used toassess the adequacy of epilepsy care focus on structural or pro-cess factors whose relationship to outcomes are indirect and mayvary across regions. The WHO measures are conceptually supe-rior because of their breadth and connection to articulated andagreed upon outcomes for health systems. However, the WHOmeasures require data that are not readily available in developingcountries and most developed countries as well.
Conclusion: The epilepsy field should consider adopting theWHO measures in country assessments of epilepsy burden andhealthcare performance whenever data permit. Efforts should bemade to develop the data elements to estimate the measures.Key Words: Healthcare—Evaluation—International—Survey
A major contributor to the global burden of epilepsy isthe lack of adequate healthcare services, particularly in de-veloping countries but also in parts of developed countriesas well. One of the greatest challenges to health plannersand policymakers is obtaining meaningful data to mea-sure these inadequacies at the community or country level.While it is easy to conceptualize indicators that might pro-vide some insights, obtaining the data can be difficult.
Relatively simple measures that have been developedto assess the adequacy of epilepsy healthcare at the coun-
Accepted October 23, 2006.Address correspondence and reprint requests to Charles E. Beg-
ley, School of Public Health, The University of Texas Health ScienceCenter, 1200 Herman Pressler, Houston, Texas 77030, U.S.A. E-mail:[email protected]
doi: 10.1111/j.1528-1167.2007.00981.x
try level are the treatment gap and availability of key re-sources. These measures have been useful because theyprovide a basic indication of unmet need and require datathat is relatively easy to obtain for most countries. In the1990s, the World Health Organization (WHO) defineda broader set of healthcare measures to be used acrossdiseases and countries to assess healthcare performance.Disability-Adjusted Life Years (DALYs) is proposed asan indicator of the health effects of healthcare systems.Patients’ perceptions of treatment responsiveness are pro-posed as a measure. Financial fairness defined as health-care spending relative to capacity to pay (CTP) is proposedas a measure.
Over the last 3 years, the members of the Interna-tional League Against Epilepsy (ILAE) Commission onHealthcare Policy examined the general strengths and
990

MONITORING EPILEPSY CARE 991
weaknesses of the existing measures used to assessepilepsy care at the country level and the feasibility andapplicability to epilepsy of the recently developed WHOindicators. The members of the Commission included twoneurologists, two neuropsychologists, a health economist,an epidemiologist, and a health care administrator. Inaddition, an economist from the WHO was added as aconsultant to assist Commission members in understand-ing and applying the WHO approach to epilepsy. TheCommission conducted workshops and organized panelpresentations at international congresses, held meetings,and worked with the WHO consultant. This paper sum-marizes the methods and findings of the Commission onthe adequacy of existing measures and the pros and consof adopting the WHO indicators as a way of extendingand improving upon them.
STRENGTHS AND LIMITATIONSOF EXISTING MEASURES
Overview of treatment gap and resourceavailability measures
The treatment gap was defined by the ILAE Commis-sion on the Developing World (1) as: The difference be-tween the number of people with active epilepsy and thenumber whose seizures are being appropriately treated ina given population at a given point of time, expressedas a percentage. The Commission defined an operationalmeasure of active epilepsy as: two or more unprovokedepileptic seizures on different days in the prior year thatare disabling to the individual. Appropriate treatment wasdefined as: diagnosis and treatment of underlying cause,and treatment of recurrent seizures according to interna-tional standards.
The treatment gap typically measures underutilizationin terms of the lack of available drug therapies. If dataare available, the gap can be derived for any servicesuch as diagnostic services (the diagnostic gap) or theavailability of specialized treatment for severe epilepsy,such as surgery (the surgery gap). The treatment gap hasbeen used to assess need in demonstration projects spon-sored by the ILAE, International Bureau for Epilepsy(IBE), and WHO in China, Brazil, Senegal, Zimbabwe,and elsewhere (Wang et al., 2003; Ndoye et al., 2005).
Another approach to determining community need, asdefined by the ILAE Commission on European Affairs,involves determining the availability of a specified set ofkey resources for epilepsy care (Malmgren et al., 2003).This resource availability measure consists of the quantityof certain types of health care resources involved in thedirect provision of medical care, such as physicians andhospitals, as well as key nonmedical resources such as thepresence of lay associations for people with epilepsy, andthe availability of funding for services. Data on each ofa series of key resources are related to population data toderive per capita estimates of resource availability that can
be compared to other communities in the region and world.The availability of key resources measure has recentlybeen applied in a unique collaborative effort of the WHO,ILAE, and IBE: “Atlas on Epilepsy Care in the World2005 (World Health Organization/International Bureau ofEpilepsy/International League Against Epilepsy, 2005).”
Evaluation methods and resultsThe members of the Commission conducted a system-
atic review of the literature on the development and ap-plication of the treatment gap and resource availabilitymeasures in assessing epilepsy care. In order to identifyrelevant articles we searched three databases: Ovid Med-line, EBSCO MEDLINE, and PubMed. We also searchedfor online articles using the Scirus scientific informationsearch engine, as well as Google. Search keywords per-taining to epilepsy epidemiology, health care assessment,needs assessment, economic evaluation, and health plan-ning were used alone and in combination. In addition,all issues of Epilepsia and Epilepsy Research since 1980were reviewed for relevant titles. Relevant articles wereidentified and discussed by members of the Commission.Kristina Malmgren, Chair, ILAE Commission of Euro-pean Affairs, and Harry Meinardi, Chair, ILAE Commis-sion on the Developing World, were invited to two of theCommission’s meetings for interviews on the pros andcons of existing measures of assessment and their appli-cation.
There is widespread agreement that the main strengthof the treatment gap measure is its relative simplicity andease of estimation. Direct methods for measuring the treat-ment gap involve finding out through population-basedprevalence studies how many detected cases there are inan area that are not receiving treatment. Indirect methods,which can be applied when data are scarce, involve com-paring prevalence data on cases to the estimated numberof people in treatment, estimated by dividing the amountof antiepileptic drugs sold in an area by the defined dailydose. Lacking data on prevalence, an estimate may bemade by applying a reasonable rate of active epilepsy ina population, such as a minimum of 0.5% (Kale, 2002).
A major limitation of the treatment gap is that it revealslittle about the alternative factors that may cause a gap.Such factors may include, for example, insufficient avail-ability of drugs, poorly organized health care systems,access barriers such as lack of transportation and healthinsurance, or inhibiting population characteristics abouthealthcare seeking behavior. Understanding the influenceof these factors can be vital to policymakers in developinga definitive diagnosis of community need or pinpointing anintervention to address the need. The likelihood of reduc-ing the treatment gap in an area by expanding healthcareresources may not be effective if people with epilepsy arereluctant to seek treatment either due to a lack of knowl-edge about their condition, a sense of shame or guilt, or
Epilepsia, Vol. 48, No. 5, 2007
992 C. E. BEGLEY ET AL.
because they feel they will be discriminated against if theydisclose their condition.
Like the treatment gap measure, the resource availabil-ity measure is relatively easy to estimate but provides onlya basic indication of the lack of services for epilepsy inan area. The application of this approach recently accom-plished for European countries (Malmgren et al., 2003)divided the task into two parts, the first involved obtainingofficial population data and data about the medical pro-fession (e.g., total number of physicians and number ofphysicians in specialties relevant for epilepsy treatment).The second involved obtaining subjective assessments ofepilepsy experts of the availability of specialty care re-sources in a country and the most important problemswith epilepsy care.
A major limitation of the resource availability mea-sures is the lack of community standards of what isconsidered a minimal, satisfactory, or optimal amountof epilepsy healthcare resources that could be appliedacross countries. Healthcare problems are suggested bydata showing wide variation in resource availability in Eu-ropean countries (Malmgren et al., 2003) and around theworld (World Health Organization/ International Bureauof Epilepsy/International League Against Epilepsy, 2005).However, in a low-income country the most cost-effectiveway to expand epilepsy care may be to train primary caredoctors or nurses to diagnose and treat epilepsy, yet theresource availability measure may point to a severe short-age of epilepsy specialists in the country as the problem.Until there are clear connections drawn between the levelof resources needed to achieve a specific outcome in thequality and effectiveness of care, this measure can onlybe used as a suggestive indicator of a problem, at best.Another limitation of the resource availability approach isthat, like the treatment gap approach, it reveals little aboutother possible factors that cause underutilization and pooroutcomes besides the availability of resources, such as ac-cess barriers, or the attitudes and beliefs of patients andtheir families.
DALYs
Overview of the measureIn developing its framework for health systems perfor-
mance assessment in the 1990s, the WHO established acommon set of measures for evaluating healthcare servicesin systems (World Health Organization, 2000; Murray andEvans, 2003). The primary motivation of the work was toprovide analysts with standardized tools to assess the per-formance of healthcare systems across diseases and coun-tries. In the WHO framework, maintaining and improvingpopulation health was defined by the WHO as the ultimategoal of healthcare services. DALYs is proposed as the op-erational indicator of the extent to which the health goalis being achieved. It defines population health in negative
terms taking into account both premature death causedby disease and the loss of healthy life due to disability(Murray, 1996; Murray et al., 2002). As a broad indicatorof the adequacy of healthcare services, DALYs reflect anumber of factors including disease incidence, disabilityand mortality effects, and the availability, accessibility,and effectiveness of treatments.
DALYs are the sum of years of life lost to prematuredeath (YLL) and years lived with a disabling condition(YLD) among those who survive. YLL is calculated asthe number of deaths attributable to the condition, multi-plied by the years that would have been lived in the absenceof a premature death. Similarly, YLD is calculated as theyears of life lived with the condition, adjusted for the per-ceived severity of the condition. For a given calendar yearand condition, YLL and YLD are calculated for age- andgender-specific cohorts. YLL and YLD are then summedacross cohorts to yield global DALYs per condition.
YLL and YLD that occur in the relatively young andrelatively old are discounted using an age-weight functionthat reflects the broader societal impact of losses of life andhealth in the more productive middle years. YLL and YLDthat occur in the future are discounted to reflect the greatersocial value of preventing near-term death and disability.As discounting reflects nonuniversal value judgments, re-sults may be presented with and without age-weightingand discounting.
Evaluation methods and resultsThe Commission’s examination of the DALY was
guided by Dr. Chisholm who attended the Commission’smeetings and conferences and led us in obtaining andtranslating literature on this WHO measure. With Dr.Chisholm’s assistance, we performed an exercise to testthe applicability of DALYs as an indicator of epilepsyhealthcare in five developed countries (Canada, France,Italy, United Kingdom, and the United States) and onedeveloping country (South Africa) using basic epidemio-logical and health care data. The goals of the exercise wereto: (1) test the feasibility of calculating country-specificDALYs, using published epidemiologic data; (2) identifygaps in the data required for estimating DALYs for specificregions, and (3) identify aspects of the DALY method thatrequire qualification or further refinement to ensure that itvalidly captures the burden of epilepsy. We did not set outto provide definitive burden estimates for each country,which would have required more systematic and precisedata estimates than resources permitted.
Calculations of epilepsy-related DALYs were madeusing a modified version of the WHO spreadsheet (avail-able from www.who.int/entity/healthinfo/bodreferencedalycalculationtemplate.xls). We identified region-,condition-, age-, and gender-specific data on population,incidence, prevalence, duration, mortality, and disabilityvia literature review. We chose the most representative
Epilepsia, Vol. 48, No. 5, 2007
MONITORING EPILEPSY CARE 993
TABLE 1. Epidemiologic parameters for calculating country-specific DALYs
Population death Incidence PrevalenceCountry rate (per 1,000) (per 1,000) (per 1,000) Treated (%) Controlled (%)
United States 0.095a 0.33–1.01b 2.8–10.2f 72i 63i
Canada 0.055a 0.33–1.01b 2.8–6.9g 90j 63l
United Kingdom 0.125a 0.33–1.01b 2.8–10.2f 90j 63l
Italy 0.028a 0.07–1.38c 1.3–19.2c 90j 63l
France 0.096a 0.31–2.15d 2.8–10.2f 90k 63l
South Africa 0.281a 0.83e 3.1–15.8h 10h 63l
Sources:aMoran et al., 2000bMoeller and Sonntag, 2002cDepartment of Economic and Social Affairs, 2003dMacDonald et al., 2000ePreux and Druet-Cabanac, 2005f Hauser and Kurland, 1975gTellez-Zenteno et al., 2004hLeonardi and Ustun, 2002iBegley et al., 2001jJacoby et al., 1998kJallon et al., 2001lKwan and Brodie, 2001
data, based on consultation with epidemiological expertsand used the standard WHO age-weights and a 3%discount rate to facilitate comparisons. Of necessity,we included data only from studies whose age strataoverlapped the strata in the WHO worksheet.
Country-specific parameter estimates are shown inTable 1. Country-specific data were not available in allcases, so estimates based on regional studies or studies ofother countries were applied where populations, economicconditions, or healthcare systems were considered suffi-ciently similar. Epidemiologic estimates for epilepsy arenot available for South Africa, for example, so parameterswere selected from studies of other sub-Saharan countries.In the absence of country-specific data, standardized mor-tality ratios (1.1–4.0, depending on age) obtained throughliterature review were applied to all countries.
In the WHO calculation of DALYs, different disabilityweights due to epilepsy depend only on treatment status.We modified the WHO worksheet to reflect both the pro-
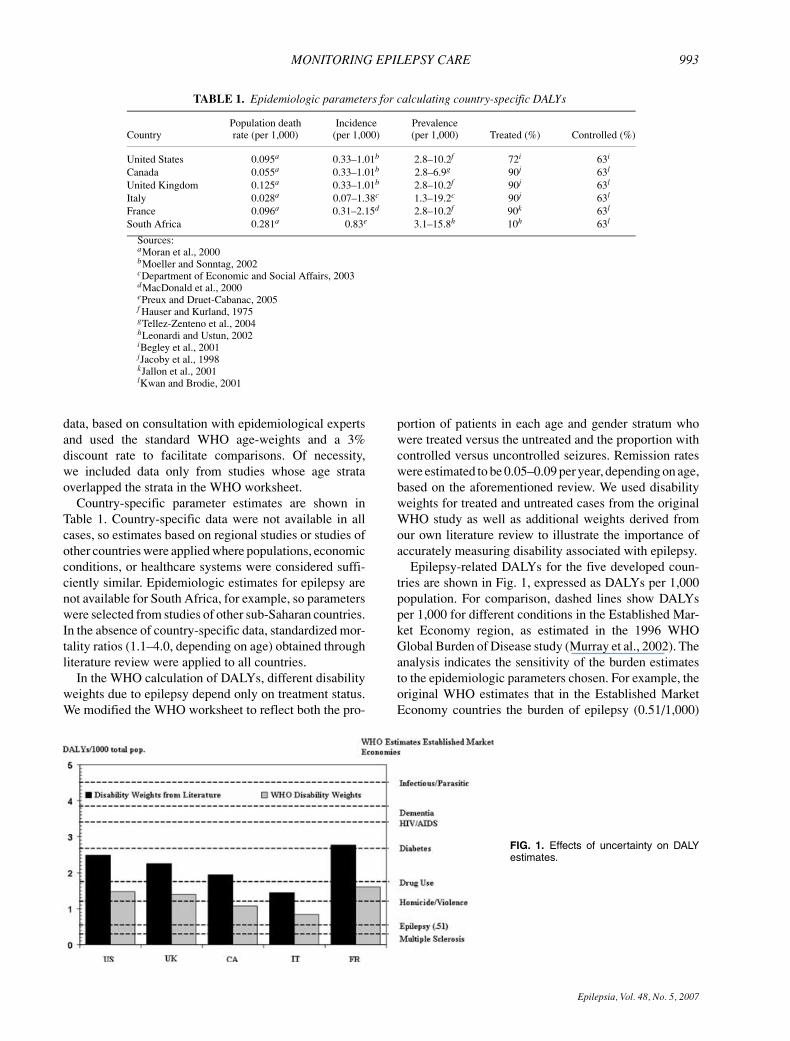
FIG. 1. Effects of uncertainty on DALYestimates.
portion of patients in each age and gender stratum whowere treated versus the untreated and the proportion withcontrolled versus uncontrolled seizures. Remission rateswere estimated to be 0.05–0.09 per year, depending on age,based on the aforementioned review. We used disabilityweights for treated and untreated cases from the originalWHO study as well as additional weights derived fromour own literature review to illustrate the importance ofaccurately measuring disability associated with epilepsy.
Epilepsy-related DALYs for the five developed coun-tries are shown in Fig. 1, expressed as DALYs per 1,000population. For comparison, dashed lines show DALYsper 1,000 for different conditions in the Established Mar-ket Economy region, as estimated in the 1996 WHOGlobal Burden of Disease study (Murray et al., 2002). Theanalysis indicates the sensitivity of the burden estimatesto the epidemiologic parameters chosen. For example, theoriginal WHO estimates that in the Established MarketEconomy countries the burden of epilepsy (0.51/1,000)
Epilepsia, Vol. 48, No. 5, 2007
994 C. E. BEGLEY ET AL.
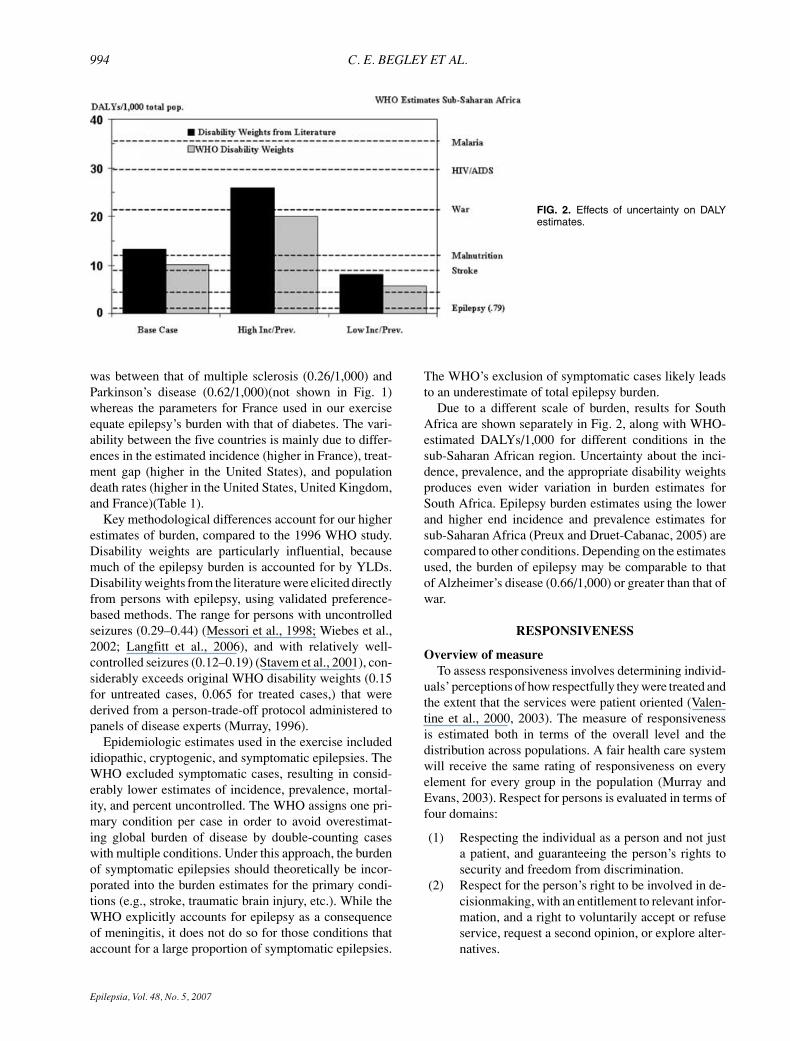
FIG. 2. Effects of uncertainty on DALYestimates.
was between that of multiple sclerosis (0.26/1,000) andParkinson’s disease (0.62/1,000)(not shown in Fig. 1)whereas the parameters for France used in our exerciseequate epilepsy’s burden with that of diabetes. The vari-ability between the five countries is mainly due to differ-ences in the estimated incidence (higher in France), treat-ment gap (higher in the United States), and populationdeath rates (higher in the United States, United Kingdom,and France)(Table 1).
Key methodological differences account for our higherestimates of burden, compared to the 1996 WHO study.Disability weights are particularly influential, becausemuch of the epilepsy burden is accounted for by YLDs.Disability weights from the literature were elicited directlyfrom persons with epilepsy, using validated preference-based methods. The range for persons with uncontrolledseizures (0.29–0.44) (Messori et al., 1998; Wiebes et al.,2002; Langfitt et al., 2006), and with relatively well-controlled seizures (0.12–0.19) (Stavem et al., 2001), con-siderably exceeds original WHO disability weights (0.15for untreated cases, 0.065 for treated cases,) that werederived from a person-trade-off protocol administered topanels of disease experts (Murray, 1996).
Epidemiologic estimates used in the exercise includedidiopathic, cryptogenic, and symptomatic epilepsies. TheWHO excluded symptomatic cases, resulting in consid-erably lower estimates of incidence, prevalence, mortal-ity, and percent uncontrolled. The WHO assigns one pri-mary condition per case in order to avoid overestimat-ing global burden of disease by double-counting caseswith multiple conditions. Under this approach, the burdenof symptomatic epilepsies should theoretically be incor-porated into the burden estimates for the primary condi-tions (e.g., stroke, traumatic brain injury, etc.). While theWHO explicitly accounts for epilepsy as a consequenceof meningitis, it does not do so for those conditions thataccount for a large proportion of symptomatic epilepsies.
The WHO’s exclusion of symptomatic cases likely leadsto an underestimate of total epilepsy burden.
Due to a different scale of burden, results for SouthAfrica are shown separately in Fig. 2, along with WHO-estimated DALYs/1,000 for different conditions in thesub-Saharan African region. Uncertainty about the inci-dence, prevalence, and the appropriate disability weightsproduces even wider variation in burden estimates forSouth Africa. Epilepsy burden estimates using the lowerand higher end incidence and prevalence estimates forsub-Saharan Africa (Preux and Druet-Cabanac, 2005) arecompared to other conditions. Depending on the estimatesused, the burden of epilepsy may be comparable to thatof Alzheimer’s disease (0.66/1,000) or greater than that ofwar.
RESPONSIVENESS
Overview of measureTo assess responsiveness involves determining individ-
uals’ perceptions of how respectfully they were treated andthe extent that the services were patient oriented (Valen-tine et al., 2000, 2003). The measure of responsivenessis estimated both in terms of the overall level and thedistribution across populations. A fair health care systemwill receive the same rating of responsiveness on everyelement for every group in the population (Murray andEvans, 2003). Respect for persons is evaluated in terms offour domains:
(1) Respecting the individual as a person and not justa patient, and guaranteeing the person’s rights tosecurity and freedom from discrimination.
(2) Respect for the person’s right to be involved in de-cisionmaking, with an entitlement to relevant infor-mation, and a right to voluntarily accept or refuseservice, request a second opinion, or explore alter-natives.
Epilepsia, Vol. 48, No. 5, 2007
MONITORING EPILEPSY CARE 995
(3) Respect for privacy and confidentiality by ensur-ing personal health information is kept private andconfidential.
(4) Respect of a person’s entitlement to obtain promptservice with access to closely located facilities, andto be taken care of in a timely manner.
Patient orientation consists of the following four do-mains:
(1) Adequate quality of basic amenities of healthcarefacilities.
(2) Health care workers’ ability to positively and ef-fectively interact with patients and their familiesduring the delivery of care, taking into account lan-guage or cultural preferences.
(3) Access to social support networks, whether suchsupport is received from family or community.
(4) Choice of care provider. Healthcare systems shouldrespect a person’s right to choose.
The domains are weighted according to impor-tance as follows: Respect for persons (50% which in-cludes: Respect for dignity—1/3; Confidentiality—1/3;and Autonomy—1/3), and Client orientation (50% whichincludes Prompt attention—20%; Quality of amenities—15%; Access to support networks—10%; Choice ofprovider—5%).
In a recent WHO survey, no single preferred instrumentfor measuring responsiveness was identified (DeSilva,2000). However, the Consumer Assessment of HealthPlans (CAHPS) questionnaire, a measure covering sev-eral domains, was identified as an appropriate tool formeasuring responsiveness. The question format reducessubjectivity by asking about the frequency of events inthe form of a Likert scale (always, usually, sometimes,never). Nine questions from CAHPS were included in theWHO responsiveness module of the key informant’s sur-vey, which estimated responsiveness levels in 191 coun-tries (Darby et al., 2000).
Evaluation methods and resultsTo examine the applicability of the WHO responsive-
ness measure, we explored the psychometric properties(reliability and validity) of the CAHPS, as a measure ofresponsiveness in people with epilepsy. We drew evidencefrom the published data produced by the WHO for assess-ing responsiveness in other health conditions. There wasno data in existence for epilepsy and as a consequence wedesigned our study to obtain such data. An integral partof the study involved developing a questionnaire that in-corporated responsiveness items from the WHO CAHPS.The first section contained questions about the clinical anddemographic details of the participants; the second sectioncontained the nine questions from the CAHPS scale per-taining to responsiveness; and the third section includedthe Liverpool Impact of Epilepsy Scale, Liverpool Stigma
of Epilepsy Scale, and Liverpool Adverse Drug EffectsProfile. One thousand questionnaires were randomly dis-tributed in the U.K. to members of Epilepsy Action, alarge epilepsy support group, of which there were 279responses. The reliability of the scale was assessed byassessing the internal structure using Chronbach’s alpha.Equal weighting was applied to each of the eight elementson the Likert scale. The criterion validity of the scale wasassessed by comparing the results of the responsivenessscales with other measures. The a priori hypothesis wasthat there would be a strong correlation between results ofthe responsiveness scale and patient perceived impact ofepilepsy. Correlation analysis was conducted to determinethe strength of the relationships.
There were 279 respondents who completed the ques-tionnaire of which 48% were male. The mean age was 47years. In terms of marital status, 36% were single, 53%were married, 7% were separated, and 3% were widowed.Of the sample 45% were in paid employment, 7% wereunemployed, 23% retired, 13% permanent sick, and 8%were students, the remaining 3% were unclassified. Re-spondents were asked to provide information about theirlocation: 10% reported living in the inner city, 57% re-ported living in an urban district, and 33% reported liv-ing in a rural area. In terms of their clinical status, 54%reported being seizure free in the last 12 months, 32%reported having less than 1 seizure per month, and 14%more than 1 seizure per month.
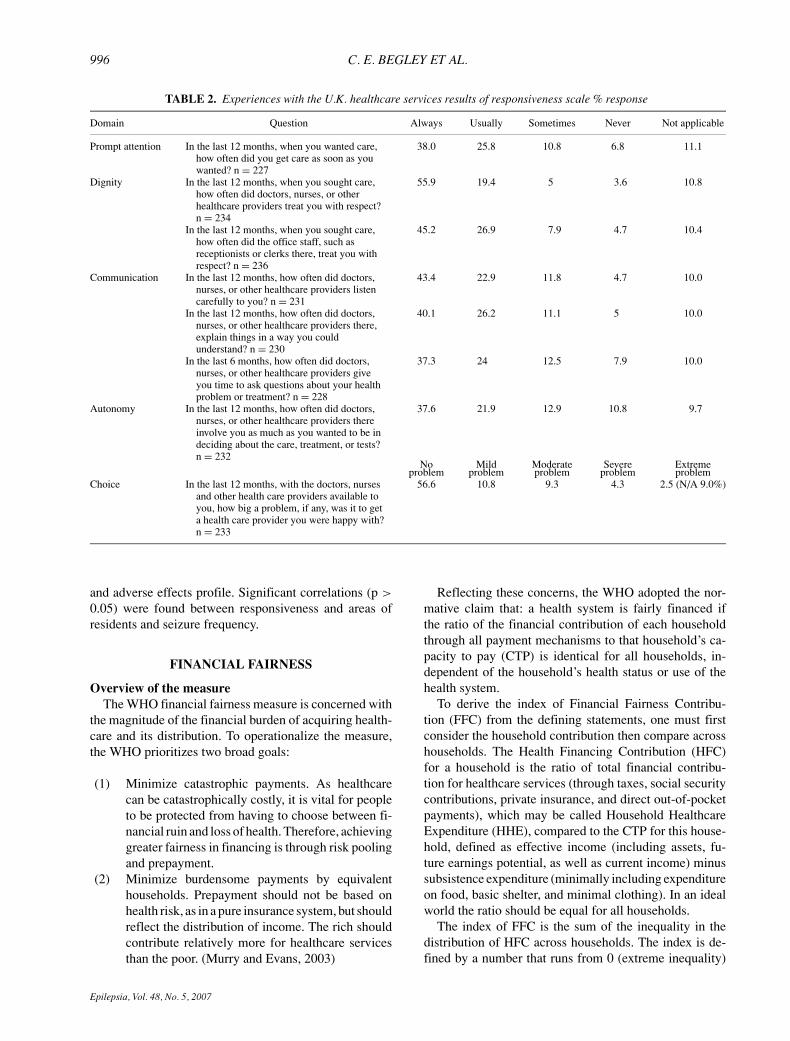
The mean score on the responsiveness scale was 14(SD = 5.68). Overall, people with epilepsy report a highlevel of satisfaction with healthcare services in the U.K.(see Table 2). Respondents reported particularly high lev-els of satisfaction with the domains of dignity and choicewith more than 50% of participants stating that the ser-vice was always responsive to their expectations. Ten percent of respondents expressed dissatisfaction with theirinteraction with healthcare providers and a further 10%indicated that they had not sought healthcare services inthe last 12 months. Lower satisfaction scores were ob-served in the domains of communication and prompt at-tention. The lowest score was provided for the domain ofautonomy.
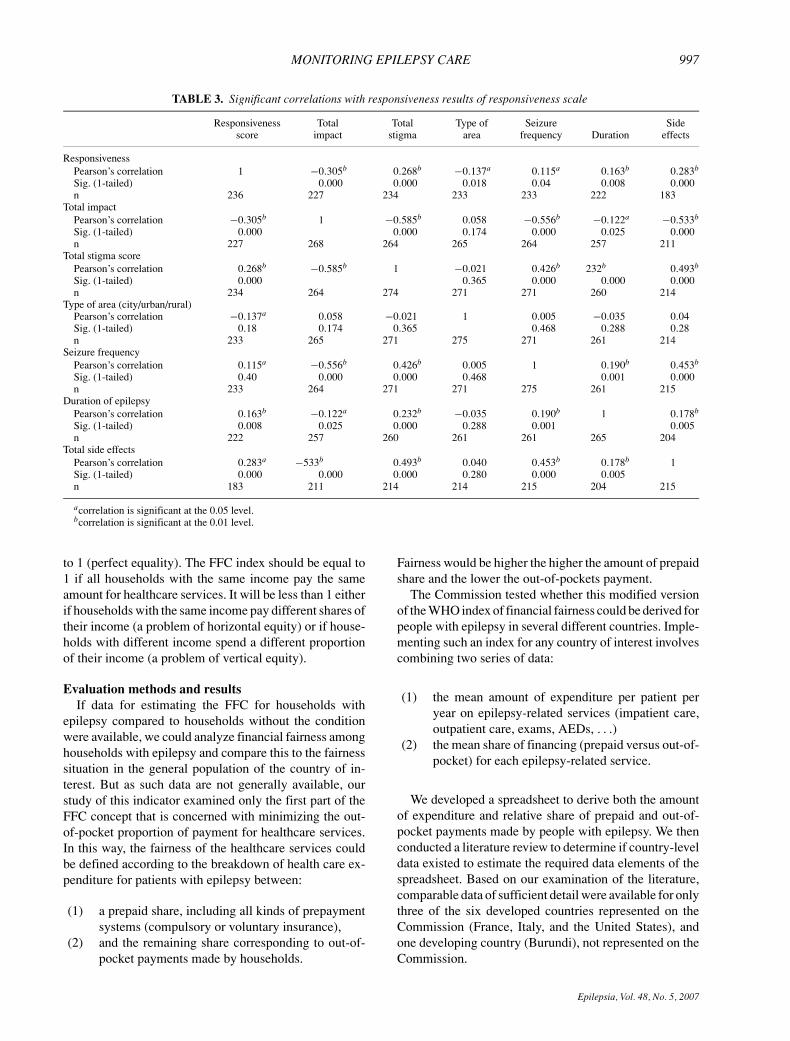
The results of the assessment of reliability revealed aChronbach’s Alpha score of 0.90 for the whole popula-tion indicating that the CAHPS scale has high internalconsistency in this population. Correlation analysis wasconducted between the responsiveness score and the vari-ables: age, sex, seizure type, and duration of epilepsy, lo-cation, impact of epilepsy, seizure frequency, stigma andtotal adverse effects score. No significant correlation wasfound between responsiveness and age or sex in this sam-ple. Significant correlations with responsiveness are pre-sented (see Table 3). Significant correlations (p > 0.01)were found between responsiveness and total impact ofepilepsy score, total stigma score, duration of the epilepsy,
Epilepsia, Vol. 48, No. 5, 2007
996 C. E. BEGLEY ET AL.
TABLE 2. Experiences with the U.K. healthcare services results of responsiveness scale % response
Domain Question Always Usually Sometimes Never Not applicable
Prompt attention In the last 12 months, when you wanted care,how often did you get care as soon as youwanted? n = 227
38.0 25.8 10.8 6.8 11.1
Dignity In the last 12 months, when you sought care,how often did doctors, nurses, or otherhealthcare providers treat you with respect?n = 234
55.9 19.4 5 3.6 10.8
In the last 12 months, when you sought care,how often did the office staff, such asreceptionists or clerks there, treat you withrespect? n = 236
45.2 26.9 7.9 4.7 10.4
Communication In the last 12 months, how often did doctors,nurses, or other healthcare providers listencarefully to you? n = 231
43.4 22.9 11.8 4.7 10.0
In the last 12 months, how often did doctors,nurses, or other healthcare providers there,explain things in a way you couldunderstand? n = 230
40.1 26.2 11.1 5 10.0
In the last 6 months, how often did doctors,nurses, or other healthcare providers giveyou time to ask questions about your healthproblem or treatment? n = 228
37.3 24 12.5 7.9 10.0
Autonomy In the last 12 months, how often did doctors,nurses, or other healthcare providers thereinvolve you as much as you wanted to be indeciding about the care, treatment, or tests?n = 232
37.6 21.9 12.9 10.8 9.7
No Mild Moderate Severe Extremeproblem problem problem problem problem
Choice In the last 12 months, with the doctors, nursesand other health care providers available toyou, how big a problem, if any, was it to geta health care provider you were happy with?n = 233
56.6 10.8 9.3 4.3 2.5 (N/A 9.0%)
and adverse effects profile. Significant correlations (p >
0.05) were found between responsiveness and areas ofresidents and seizure frequency.
FINANCIAL FAIRNESS
Overview of the measureThe WHO financial fairness measure is concerned with
the magnitude of the financial burden of acquiring health-care and its distribution. To operationalize the measure,the WHO prioritizes two broad goals:
(1) Minimize catastrophic payments. As healthcarecan be catastrophically costly, it is vital for peopleto be protected from having to choose between fi-nancial ruin and loss of health. Therefore, achievinggreater fairness in financing is through risk poolingand prepayment.
(2) Minimize burdensome payments by equivalenthouseholds. Prepayment should not be based onhealth risk, as in a pure insurance system, but shouldreflect the distribution of income. The rich shouldcontribute relatively more for healthcare servicesthan the poor. (Murry and Evans, 2003)
Reflecting these concerns, the WHO adopted the nor-mative claim that: a health system is fairly financed ifthe ratio of the financial contribution of each householdthrough all payment mechanisms to that household’s ca-pacity to pay (CTP) is identical for all households, in-dependent of the household’s health status or use of thehealth system.
To derive the index of Financial Fairness Contribu-tion (FFC) from the defining statements, one must firstconsider the household contribution then compare acrosshouseholds. The Health Financing Contribution (HFC)for a household is the ratio of total financial contribu-tion for healthcare services (through taxes, social securitycontributions, private insurance, and direct out-of-pocketpayments), which may be called Household HealthcareExpenditure (HHE), compared to the CTP for this house-hold, defined as effective income (including assets, fu-ture earnings potential, as well as current income) minussubsistence expenditure (minimally including expenditureon food, basic shelter, and minimal clothing). In an idealworld the ratio should be equal for all households.
The index of FFC is the sum of the inequality in thedistribution of HFC across households. The index is de-fined by a number that runs from 0 (extreme inequality)
Epilepsia, Vol. 48, No. 5, 2007
MONITORING EPILEPSY CARE 997
TABLE 3. Significant correlations with responsiveness results of responsiveness scale
Responsiveness Total Total Type of Seizure Sidescore impact stigma area frequency Duration effects
ResponsivenessPearson’s correlation 1 −0.305b 0.268b −0.137a 0.115a 0.163b 0.283b
Sig. (1-tailed) 0.000 0.000 0.018 0.04 0.008 0.000n 236 227 234 233 233 222 183
Total impactPearson’s correlation −0.305b 1 −0.585b 0.058 −0.556b −0.122a −0.533b
Sig. (1-tailed) 0.000 0.000 0.174 0.000 0.025 0.000n 227 268 264 265 264 257 211
Total stigma scorePearson’s correlation 0.268b −0.585b 1 −0.021 0.426b 232b 0.493b
Sig. (1-tailed) 0.000 0.365 0.000 0.000 0.000n 234 264 274 271 271 260 214
Type of area (city/urban/rural)Pearson’s correlation −0.137a 0.058 −0.021 1 0.005 −0.035 0.04Sig. (1-tailed) 0.18 0.174 0.365 0.468 0.288 0.28n 233 265 271 275 271 261 214
Seizure frequencyPearson’s correlation 0.115a −0.556b 0.426b 0.005 1 0.190b 0.453b
Sig. (1-tailed) 0.40 0.000 0.000 0.468 0.001 0.000n 233 264 271 271 275 261 215
Duration of epilepsyPearson’s correlation 0.163b −0.122a 0.232b −0.035 0.190b 1 0.178b
Sig. (1-tailed) 0.008 0.025 0.000 0.288 0.001 0.005n 222 257 260 261 261 265 204
Total side effectsPearson’s correlation 0.283a −533b 0.493b 0.040 0.453b 0.178b 1Sig. (1-tailed) 0.000 0.000 0.000 0.280 0.000 0.005n 183 211 214 214 215 204 215
acorrelation is significant at the 0.05 level.bcorrelation is significant at the 0.01 level.
to 1 (perfect equality). The FFC index should be equal to1 if all households with the same income pay the sameamount for healthcare services. It will be less than 1 eitherif households with the same income pay different shares oftheir income (a problem of horizontal equity) or if house-holds with different income spend a different proportionof their income (a problem of vertical equity).
Evaluation methods and resultsIf data for estimating the FFC for households with
epilepsy compared to households without the conditionwere available, we could analyze financial fairness amonghouseholds with epilepsy and compare this to the fairnesssituation in the general population of the country of in-terest. But as such data are not generally available, ourstudy of this indicator examined only the first part of theFFC concept that is concerned with minimizing the out-of-pocket proportion of payment for healthcare services.In this way, the fairness of the healthcare services couldbe defined according to the breakdown of health care ex-penditure for patients with epilepsy between:
(1) a prepaid share, including all kinds of prepaymentsystems (compulsory or voluntary insurance),
(2) and the remaining share corresponding to out-of-pocket payments made by households.
Fairness would be higher the higher the amount of prepaidshare and the lower the out-of-pockets payment.
The Commission tested whether this modified versionof the WHO index of financial fairness could be derived forpeople with epilepsy in several different countries. Imple-menting such an index for any country of interest involvescombining two series of data:
(1) the mean amount of expenditure per patient peryear on epilepsy-related services (impatient care,outpatient care, exams, AEDs, . . .)
(2) the mean share of financing (prepaid versus out-of-pocket) for each epilepsy-related service.
We developed a spreadsheet to derive both the amountof expenditure and relative share of prepaid and out-of-pocket payments made by people with epilepsy. We thenconducted a literature review to determine if country-leveldata existed to estimate the required data elements of thespreadsheet. Based on our examination of the literature,comparable data of sufficient detail were available for onlythree of the six developed countries represented on theCommission (France, Italy, and the United States), andone developing country (Burundi), not represented on theCommission.
Epilepsia, Vol. 48, No. 5, 2007
998 C. E. BEGLEY ET AL.
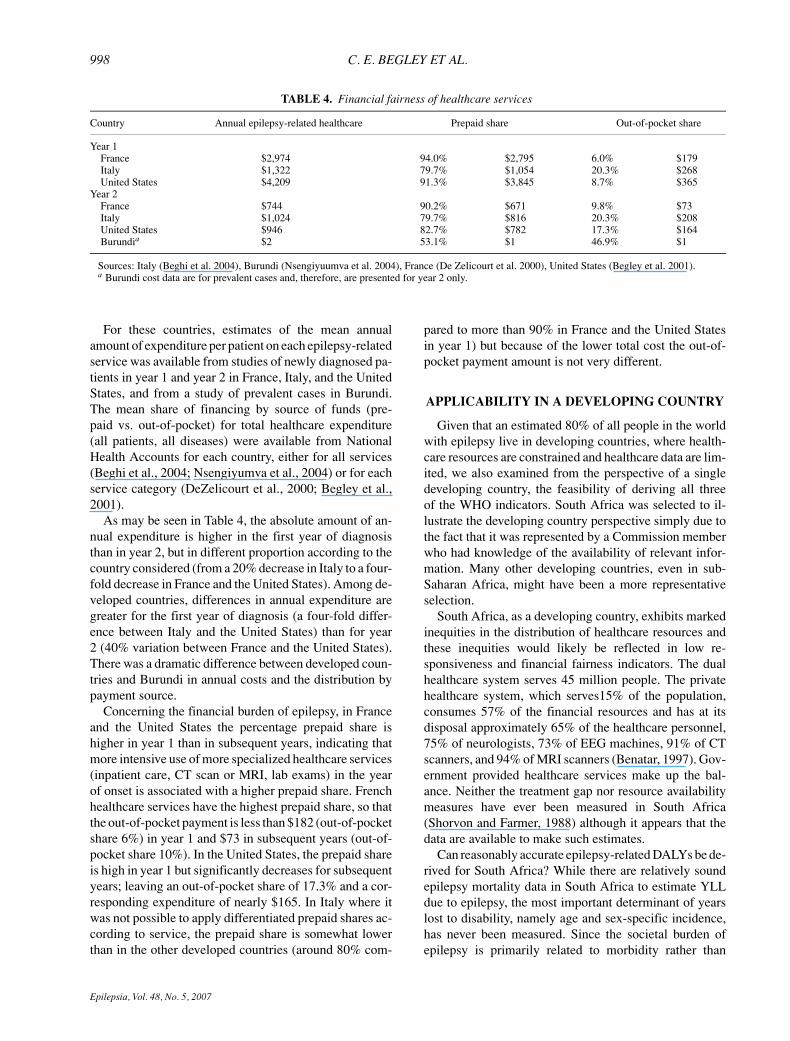
TABLE 4. Financial fairness of healthcare services
Country Annual epilepsy-related healthcare Prepaid share Out-of-pocket share
Year 1France $2,974 94.0% $2,795 6.0% $179Italy $1,322 79.7% $1,054 20.3% $268United States $4,209 91.3% $3,845 8.7% $365
Year 2France $744 90.2% $671 9.8% $73Italy $1,024 79.7% $816 20.3% $208United States $946 82.7% $782 17.3% $164Burundia $2 53.1% $1 46.9% $1
Sources: Italy (Beghi et al. 2004), Burundi (Nsengiyuumva et al. 2004), France (De Zelicourt et al. 2000), United States (Begley et al. 2001).a Burundi cost data are for prevalent cases and, therefore, are presented for year 2 only.
For these countries, estimates of the mean annualamount of expenditure per patient on each epilepsy-relatedservice was available from studies of newly diagnosed pa-tients in year 1 and year 2 in France, Italy, and the UnitedStates, and from a study of prevalent cases in Burundi.The mean share of financing by source of funds (pre-paid vs. out-of-pocket) for total healthcare expenditure(all patients, all diseases) were available from NationalHealth Accounts for each country, either for all services(Beghi et al., 2004; Nsengiyumva et al., 2004) or for eachservice category (DeZelicourt et al., 2000; Begley et al.,2001).
As may be seen in Table 4, the absolute amount of an-nual expenditure is higher in the first year of diagnosisthan in year 2, but in different proportion according to thecountry considered (from a 20% decrease in Italy to a four-fold decrease in France and the United States). Among de-veloped countries, differences in annual expenditure aregreater for the first year of diagnosis (a four-fold differ-ence between Italy and the United States) than for year2 (40% variation between France and the United States).There was a dramatic difference between developed coun-tries and Burundi in annual costs and the distribution bypayment source.
Concerning the financial burden of epilepsy, in Franceand the United States the percentage prepaid share ishigher in year 1 than in subsequent years, indicating thatmore intensive use of more specialized healthcare services(inpatient care, CT scan or MRI, lab exams) in the yearof onset is associated with a higher prepaid share. Frenchhealthcare services have the highest prepaid share, so thatthe out-of-pocket payment is less than $182 (out-of-pocketshare 6%) in year 1 and $73 in subsequent years (out-of-pocket share 10%). In the United States, the prepaid shareis high in year 1 but significantly decreases for subsequentyears; leaving an out-of-pocket share of 17.3% and a cor-responding expenditure of nearly $165. In Italy where itwas not possible to apply differentiated prepaid shares ac-cording to service, the prepaid share is somewhat lowerthan in the other developed countries (around 80% com-
pared to more than 90% in France and the United Statesin year 1) but because of the lower total cost the out-of-pocket payment amount is not very different.
APPLICABILITY IN A DEVELOPING COUNTRY
Given that an estimated 80% of all people in the worldwith epilepsy live in developing countries, where health-care resources are constrained and healthcare data are lim-ited, we also examined from the perspective of a singledeveloping country, the feasibility of deriving all threeof the WHO indicators. South Africa was selected to il-lustrate the developing country perspective simply due tothe fact that it was represented by a Commission memberwho had knowledge of the availability of relevant infor-mation. Many other developing countries, even in sub-Saharan Africa, might have been a more representativeselection.
South Africa, as a developing country, exhibits markedinequities in the distribution of healthcare resources andthese inequities would likely be reflected in low re-sponsiveness and financial fairness indicators. The dualhealthcare system serves 45 million people. The privatehealthcare system, which serves15% of the population,consumes 57% of the financial resources and has at itsdisposal approximately 65% of the healthcare personnel,75% of neurologists, 73% of EEG machines, 91% of CTscanners, and 94% of MRI scanners (Benatar, 1997). Gov-ernment provided healthcare services make up the bal-ance. Neither the treatment gap nor resource availabilitymeasures have ever been measured in South Africa(Shorvon and Farmer, 1988) although it appears that thedata are available to make such estimates.
Can reasonably accurate epilepsy-related DALYs be de-rived for South Africa? While there are relatively soundepilepsy mortality data in South Africa to estimate YLLdue to epilepsy, the most important determinant of yearslost to disability, namely age and sex-specific incidence,has never been measured. Since the societal burden ofepilepsy is primarily related to morbidity rather than
Epilepsia, Vol. 48, No. 5, 2007

MONITORING EPILEPSY CARE 999
mortality, quantifying morbidity, and therefore incidence,is of considerable importance. Prevalence of epilepsy, apotential substitute measure, has also not been estimatedin South Africa. Duration and distribution by severity havenot been determined, but since these variables have farless of a determining effect on DALYs, they may deservea lower research priority.
There are strong indications that the incidence andprevalence of epilepsy is greater in developing comparedto developed nations (Preux and Druet-Cabanac, 2005).Estimates of the incidence of epilepsy in sub-SaharanAfrican countries have varied between 64 and 156 per100,000, compared with estimates in the range of 40–70 per 100,000 for developed countries (South AfricanHealth Review, 2005). Studies of prevalence have simi-larly been higher in sub-Saharan African countries (me-dian estimates of 1.5%, ranging from 0.5% to 7.4%)compared to developed countries (estimates of approx-imately 0.5–0.9%). In South Africa the effects of theHIV epidemic, estimated at between 5 and 6.5 mil-lion people in the total population of about 45 mil-lion, on the burden of epilepsy remains unknown (avail-able from http://www.cdc.gov/nchs/data/ad/ad303.pdf;http://www.mrc.ac.za/bod/initialbodestimates.pdf). HIVinfection in the brain and common secondary infec-tions, such as tuberculosis, may increase the burden ofepilepsy in the population. Homicide, motor vehicle ac-cidents, and infections such as neurocysticercosis toomay contribute to an increased burden of epilepsy inthe South African population, as it may in other devel-oping nations (Thomson, 1993; Fingerhut et al., 1998;Leary et al., 1999; Preti and Miotto, 2000; Mafojaneet al., 2003; Phiri et al., 2003; Sander, 2003 avail-able from http://www.paho.org/english/dd/ais/be v25nl-acctransito.htm).
There are no cost studies of epilepsy in South Africaand no studies of the population’s experience with health-care services. Therefore, estimating financial fairness andobtaining representative responsiveness information for acountry such as South Africa will require considerablenew efforts in primary data collection.
In summary, limited health care resources are typicallyparalleled by a paucity of research and data availability formaking even approximate estimates of the WHO measuresof healthcare performance. If the WHO measures are to beestimated for South Africa, high quality incidence studiesmerit priority, since incidence is the principle determinantof DALYs. Financial information and healthcare serviceexperience data will also have to be gathered.
CONCLUSIONS AND DISCUSSION
Our overall findings are that the treatment gap and re-source availability measures have limited value for plan-
ners and policymakers and the epilepsy field should con-sider adopting the broader WHO measures in country as-sessments of epilepsy burden and healthcare performancewhenever data permit. The WHO measures are clearly su-perior at the conceptual level and have several potentialadvantages. The DALY directly measures the ultimate,distal outcome of interest (health) on a single scale that isapplicable to all conditions. DALY estimates also createthe opportunity to discuss the flip side of burden, that is,avoidable burden, which in the case of epilepsy is a largepercentage of attributable burden that can be achieved atrelatively low cost (Chisholm, 2005).
Responsiveness is a desirable measure because it re-flects a consumer perspective on healthcare treatment andoutcomes. Our survey indicated that the responsivenessscale is a reliable and valid instrument in people withepilepsy in the U.K. No problems were found with itsuse and the findings of this study are in line with previousresponsiveness studies in other health conditions (WorldHealth Organization, 2000).
The modified WHO financial fairness index gives us themean prepaid share for all patients with epilepsy but noinformation concerning differences among patients withepilepsy or persons with epilepsy compared to the generalpopulation. It was possible to estimate for three of theseven countries represented on our Commission.
Our findings on the WHO measures must be qualifiedby a number of limitations, however. There is ongoing de-bate about how certain assumptions (e.g., differential age-weighting or keeping disability weights constant across re-gions) may skew DALY estimates and result in inequitableresource distribution (Allotey et al., 2003; Arnesen andKapiriri, 2004). Current DALY methods do not reflect theburden attributable to comorbid epilepsy in stroke, trau-matic brain injury, and other conditions that account for themajority of symptomatic epilepsies. In addition, the origi-nal WHO disability weights underestimate burden relativeto weights obtained in actual persons with epilepsy usingstandard survey methods.
The reliability and validity study of the responsivenessscale undertaken by the Commission had several limita-tions including: the sample was drawn from members of aU.K. support group; the response rate was relatively low,both these factors may have implications for the gener-alizability of the results. The psychometric properties ofthe scale need to be tested further, across different cul-tures before results may be meaningfully compared on aninternational basis.
The primary limitation of all the WHO measures isthat they require data that are not available in developingcountries and most developed countries. At the presenttime, their main value is that they define data elementsthat need to be obtained if more complete and mean-ingful assessments of epilepsy-related healthcare services
Epilepsia, Vol. 48, No. 5, 2007
1000 C. E. BEGLEY ET AL.
are to be made. Until then, planners and policymakerswill have to rely on existing measures, perhaps supple-mented by WHO measures that are based on hypotheticalestimates.
Acknowledgments: The authors would like to thankEpilepsy Action for supporting the responsiveness study, Mar-garet Rawnsley (Research Officer, Epilepsy Action) for her assis-tance in administering the questionnaire and Dr. Jayne Brookesfor her help with statistical analysis. We would also like to thankthe ILAE Executive Committee for their support of the Commis-sion’s work and Dr. Leonid L. Prilipko for his assistance withthe WHO framework.
REFERENCES
Allotey P, Reidpath D, Kouame A, Cummins R. (2003) The DALY,context and the determinants of the severity of disease: an exploratorycomparison of paraplegia in Australia and Cameroon. Social Scienceand Medicine 57:949–958.
Arnesen T, Kapiriri L. (2004). Can the value choices in DALYs influenceglobal priority-setting? Health Policy 70:137–149.
Beghi E, Garattini L, Ricci E, Cornago D, Parazzini F, EPICOS Group.(2004) Direct cost of medical management of epilepsy among adultsin Italy: a prospective cost-of-illness study (EPICOS). Epilepsia45:171–178.
Begley CE, Lairson DR, Reynolds TF, Coan S. (2001). Early treatmentcost in epilepsy and how it varies with seizure type and frequency.Epilepsy Research 47:205–213.
Benatar SR. (1997) Health care reform in the new South Africa. NewEngland Journal of Medicine 336:891–895.
Chisholm D. (2005) Cost-effectiveness of first-line antiepileptic drugtreatments in the developing world: a population-level analysis.Epilepsia 46:751–759.
Darby C, Valentine N, Murray CJL, de Silva A. (2000). WHO: strat-egy on measuring responsiveness. Geneva, World Health Orga-nization, Evidence and Information for Policy Discussion PaperNo. 23.
United Nations, Department of Economic and Social Affairs. (2003)World population prospects: The 2000 Revision New York: UnitedNations.
De Silva A. (2000). A Framework for Measuring Responsiveness.Geneva World Health Organisation, Evidence and Information forPolicy Discussion paper No. 32.
De Zelicourt M, Buteau L, Fagnani F, Buteau L, Fagnani F,Jallon P. (2000) The contributing factors to medical costof epilepsy: an estimation based on a French prospec-tive cohort study of patients with newly diagnosed epilep-tic seizures (the CAROLE study). Active Coordination of theLongitudinal Observational Network in Epilepsy. Seizure 9:88–95.
Fingerhut LA, Cox CS, Warner M. (1998) International comparativeanalysis of injury mortality. Findings from the ICE on injury statis-tics. International collaborative effort on injury statistics. AdvanceData 303:1–20.
Hauser WA, Kurland LT. (1975) The epidemiology of epilepsy inRochester, Minnesota, 1935 through 1967. Epilepsia 16:1–66.
Jacoby A, Buck D, Baker G, McNamee P, Graham-Jones S, ChadwickD. (1998) Uptake and costs of care for epilepsy: findings from a U.K.regional study. Epilepsia 39:776–786.
Jallon P, Loiseau P, Loiseau J. (2001) Newly diagnosed unprovokedepileptic seizures: presentation at diagnosis in CAROLE study.Epilepsia 42:464–475.
Kale R. (2002) The treatment gap. Epilepsia 43(suppl.6):31–33.Kwan P, Brodie MJ. (2001). Effectiveness of first antiepileptic drug.
Epilepsia 42:1255–1260.Langfitt JT, Vickrey BG, McDermott M, Messing S, Berg AT, Spencer
SS, Sperling MR, Bazil CW, Shinnar S. (2006) Validity and respon-siveness of generic preference-based HRQOL instruments in chronicepilepsy. Quality of Life Research 15:899–914.
Leary PM, Riordan G, Schlegel B, Morris S. (1999). Childhood sec-ondary (symptomatic) epilepsy, seizure control, and intellectualhandicap in a nontropical region of South Africa. Epilepsia 40:1110–1113.
Leonardi M, Ustun TB. (2002) The global burden of epilepsy. Epilepsia43(suppl. 6):21–5.
MacDonald BK, Cockerell OC, Sander JWAS, Shorvon SD. (2000)The incidence and lifetime prevalence of neurological disorders ina prospective community-based study in the UK. Brain 123:665–676.
Mafojane NA, Appleton CC, Krecek RC, Michael LM, Willingham ALIII. (2003) The current status of neurocysticercosis in Eastern andSouthern Africa. Acta Tropica 87:25–33.
Malmgren K, Flink R, Guekht AB, Michelucci R, Neville B, Pedersen B,Pinto F, Stephani U, Ozkara C; ILAE Commission of European Af-fairs, Subcommission on European Guidelines (2003). The provisionof epilepsy care across Europe. Epilepsia 44:727–731.
Meinardi H, Scott RA, Reis R, Sander JWAS. (2001) On behalf of theILAE Commission on the Developing World. The treatment gap inepilepsy: the current situation and ways forward. Epilepsia 42:136–149.
Messori A, Trippoli S, Becagli P, Cincotta M, Labbate MG, ZaccaraG. (1998) Adjunctive lamotrigine therapy in patients with refractoryseizures: a lifetime cost-utility analysis. European Journal of ClinicalPharmacology 53:421–427.
Moeller J, Sonntag AK. (2002) Assessing the performance of healthsystems—contributions made by the world health organization. Busi-ness Briefing: Global Healthcare 3:18–21
Moran N, Poole K, Bell G, Solomon J, Kendall S, McCarthy M, Mc-Cormick D, Nashef L, Johnson A, Sander J, Shorvon S. (2000). NHSservices for epilepsy from the patients perspective: a survey of pri-mary, secondary and tertiary care access throughout the UK. Seizure9:559–565.
Murray CJL. (1996). Rethinking DALYs. In Murray CJL, Lopez ED(Eds) The global burden of disease. Harvard School of Public Health,Boston. pp. 1–98.
Murray CJL, Evans DB. (2003) Health systems performance assessment:goals, framework and overview. In Murray CJL, Evans DB (Eds).Health systems performance assessment; debates, methods and em-piricism. WHO, Geneva, Switzerland, 3–19.
Murray CJL, Salomon JA, Mathers CD, Lopez, ED. (2002) Summarymeasures of population health: concepts, ethics, measurement andapplications. World Health Organization, Geneva.
Ndoye NF, Sow AD, Diop AG, Sessouma B, Sene-Diouf F, Boissy L,Wone I, Toure K, Ndiaye M, Ndiaye P, de Boer H, Engel J, Man-dlhate C, Meinardi H, Prilipko L, Sander JW. (2005) Prevalence ofepilepsy its treatment gap and knowledge, attitude and practice of itspopulation in sub-urban Senegal an ILAE/IBE/WHO study. Seizure14:106–111.
Nsengiyumva G, Druet-Cabanac M, Nzisabira L, Preux PM, Vergnene-gre A. (2004). Economic evaluation of epilepsy in Kiremba (Bu-rundi): a case-control study. Epilepsia 45:673–677.
Phiri IK, Ngowi H, Afonso S, Matenga E, Boa M, Mukaratirwa S, Githi-gia S, Saimo M, Sikasunge C, Maingi N, Lubega GW, Kassuku A,Michael L, Siziya S, Krecek RC, Noormahomed E, Vilhena M, DornyP, Willingham AL 3rd. (2003) The emergence of Taenia solium cys-ticercosis in Eastern and Southern Africa as a serious agriculturalproblem and public health risk. Acta Tropuc 87:13–23.
Preti A, Miotto P. (2000) Death by homicide in Italy, 1980–1994: ageand gender differences among victims. Medicine, Science, and theLaw 40:233–240.
Preux PM, Druet-Cabanac M. (2005) Epidemiology and etiology ofepilepsy in sub-Saharan Africa. Lancet Neurology 4:21–31.
Sander JWAS. (2003) The epidemiology of epilepsy revisited. CurrentOpinion in Neurology 16:165–170.
Shorvon SD, Farmer PJ. (1988) Epilepsy in developing countries: areview of epidemiological, sociocultural, and treatment aspects.Epilepsia 29(suppl. 1):S36–S54.
South African Health Review. (2005) Available fromhttp://www.hst.org.za/.
Stavem K, Bjornaes H, Lossius MI. (2001) Properties of the 15D and EQ-5D utility measures in a community sample of people with epilepsy.Epilepsy Research 44:179–189.
Epilepsia, Vol. 48, No. 5, 2007

MONITORING EPILEPSY CARE 1001
Tellez-Zenteno JF, Pondal-Sordo M, Matijevic S, Wiebe S. (2004) Na-tional and regional prevalence of self-reported epilepsy in Canada.Epilepsia 45:1623–9.
Thomson AJ. (1993) Neurocysticercosis—experience at the teachinghospitals of the University of Cape Town. South African MedicalJournal 83:332–334
Valentine NB, de Silva A, Murray CJL. (2000). Estimating Re-sponsiveness Level and Distribution for 191 Countries: Meth-ods and Results. GPE Discussion Paper Series: No. 22. Geneva,WHO.
Valentine NB, de Silva A, Kawabata K, Darby C, Murray CJL, EvansDB. (2003). Health system responsiveness; concepts, domains andoperationalization. In Murray CJL, Evans DB (Eds) Health systems
performance assessment; debates, methods and empiricism. WHO,Geneva, pp. 573–596.
Wang WZ, Wu JZ, Wang DS, Dai XY, Yang B, Wang TP, Yuan CL, ScottRA, Prilipko LL, de Boer HM, Sander JW. (2003) The prevalenceand treatment gap in epilepsy in China. Neurology 60:1544–1545.
Wiebe S, Matijevic S, Eliasziw M, Derry PA. (2002) Clinically importantchange in quality of life in epilepsy. Journal of Neurology, Neuro-surgery, and Psychiatry 73:116–120.
World Health Organization. (2001) World Health Report 2000. WHO,Geneva.
World Health Organization/International Bureau of Epilepsy/International League Against Epilepsy. (2005). Epilepsy Carein the World 2005. Geneva, Switzerland.
Epilepsia, Vol. 48, No. 5, 2007
Related Documents











