NEW RESEARCH Crime and Psychiatric Disorders Among Youth in the US Population: An Analysis of the National Comorbidity Survey–Adolescent Supplement Kendell L. Coker, PhD, JD, Philip H. Smith, PhD, Alexander Westphal, MD, PhD, Howard V. Zonana, MD, Sherry A. McKee, PhD Objective: Current knowledge regarding psychiatric disorders and crime in youth is limited to juvenile justice and community samples. This study examined relationships between psychi- atric disorders and self-reported crime involvement in a sample of youth representative of the US population. Method: The National Comorbidity Survey–Adolescent Supplement (N ¼ 10,123; ages 13–17 years; 2001–2004) was used to examine the relationship between life- time DSM-IV–based diagnoses, reported crime (property, violent, other), and arrest history. Logistic regression compared the odds of reported crime involvement with specific psychiatric disorders to those without any diagnoses, and examined the odds of crime by psychiatric comorbidity. Results: Prevalence of crime was 18.4%. Youth with lifetime psychiatric disorders, compared to no disorders, had significantly greater odds of crime, including violent crime. For violent crime resulting in arrest, conduct disorder (CD) (odds ratio OR ¼ 57.5; 95% CI ¼ 30.4, 108.8), alcohol use disorders (OR ¼ 19.5; 95% CI ¼ 8.8, 43.2), and drug use disorders (OR ¼ 16.1; 95% CI ¼ 9.3, 27.7) had the greatest odds with similar findings for violent crime with no arrest. Psychiatric comorbidity increased the odds of crime. Youth with 3 or more diagnoses (16.0% of population) accounted for 54.1% of those reporting arrest for violent crime. Youth with at least 1 diagnosis committed 85.8% of crime, which was reduced to 67.9% by removing individuals with CD. Importantly, 88.2% of youth with mental illness reported never having committed any crime. Conclusion: Our findings highlight the impor- tance of improving access to mental health services for youthful offenders in community set- tings, given the substantial associations found between mental illness and crime in this nationally representative epidemiological sample. J. Am. Acad. Child Adolesc. Psychiatry, 2014;53(8):888–898. Key Words: youth, psychiatric disorders, crime, arrest, US population T he relationship between crime and mental illness is an issue that is often in the national spotlight. Although large-scale, nationally representative epidemiological studies have established associations between crime and mental illness in adults, 1-3 such investigations have not been conducted with adolescent sam- ples, resulting in a lack of data to inform critical prevention and intervention efforts occurring within mental health and juvenile justice systems. Population studies examining crime and mental illness have generated an understanding of the complexity of this relationship in adults. For example, some studies have found that the presence of severe mental disorders and sub- stance use disorders in adults is generally asso- ciated with property crimes, 4 and the presence of psychotic symptoms elevates their risk to commit a violent offense. 5 Other studies using prospec- tive longitudinal evaluations of crime and mental illness in adults find that violent crime is modestly associated with psychiatric disorders, and that this relationship is strengthened when substance use disorders are comorbid with other psychiatric disorders. 1,2 Supplemental material cited in this article is available online. JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY 888 www.jaacap.org VOLUME 53 NUMBER 8 AUGUST 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

88
EW RESEARCH
N8
Crime and Psychiatric Disorders Among Youthin the US Population: An Analysis of theNational Comorbidity Survey–Adolescent
SupplementKendell L. Coker, PhD, JD, Philip H. Smith, PhD, Alexander Westphal, MD, PhD,
Howard V. Zonana, MD, Sherry A. McKee, PhD
Objective: Current knowledge regarding psychiatric disorders and crime in youth is limited tojuvenile justice and community samples. This study examined relationships between psychi-atric disorders and self-reported crime involvement in a sample of youth representative ofthe US population. Method: The National Comorbidity Survey–Adolescent Supplement(N ¼ 10,123; ages 13–17 years; 2001–2004) was used to examine the relationship between life-time DSM-IV–based diagnoses, reported crime (property, violent, other), and arrest history.Logistic regression compared the odds of reported crime involvement with specific psychiatricdisorders to those without any diagnoses, and examined the odds of crime by psychiatriccomorbidity. Results: Prevalence of crime was 18.4%. Youth with lifetime psychiatricdisorders, compared to no disorders, had significantly greater odds of crime, including violentcrime. For violent crime resulting in arrest, conduct disorder (CD) (odds ratio OR ¼ 57.5;95% CI ¼ 30.4, 108.8), alcohol use disorders (OR ¼ 19.5; 95% CI ¼ 8.8, 43.2), and druguse disorders (OR ¼ 16.1; 95% CI ¼ 9.3, 27.7) had the greatest odds with similar findings forviolent crime with no arrest. Psychiatric comorbidity increased the odds of crime. Youth with3 or more diagnoses (16.0% of population) accounted for 54.1% of those reporting arrest forviolent crime. Youth with at least 1 diagnosis committed 85.8% of crime, which was reducedto 67.9% by removing individuals with CD. Importantly, 88.2% of youth with mental illnessreported never having committed any crime. Conclusion: Our findings highlight the impor-tance of improving access to mental health services for youthful offenders in community set-tings, given the substantial associations found between mental illness and crime in thisnationally representative epidemiological sample. J. Am. Acad. Child Adolesc. Psychiatry,2014;53(8):888–898. Key Words: youth, psychiatric disorders, crime, arrest, US population
he relationship between crime and mentalillness is an issue that is often in the national
T spotlight. Although large-scale, nationallyrepresentative epidemiological studies haveestablished associations between crime andmental illness in adults,1-3 such investigationshave not been conducted with adolescent sam-ples, resulting in a lack of data to inform criticalprevention and intervention efforts occurringwithin mental health and juvenile justice systems.
Supplemental material cited in this article is available online.
JOURN
www.jaacap.org
Population studies examining crime andmental illness have generated an understandingof the complexity of this relationship in adults.For example, some studies have found that thepresence of severe mental disorders and sub-stance use disorders in adults is generally asso-ciated with property crimes,4 and the presence ofpsychotic symptoms elevates their risk to commita violent offense.5 Other studies using prospec-tive longitudinal evaluations of crime and mentalillness in adults find that violent crime ismodestly associated with psychiatric disorders,and that this relationship is strengthened whensubstance use disorders are comorbid with otherpsychiatric disorders.1,2
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 53 NUMBER 8 AUGUST 2014
CRIME AND PSYCHIATRIC DISORDERS IN YOUTH
Current knowledge about associations be-tween crime and mental illness in adolescentscomes mainly from youth involved with the ju-venile justice system,6 a population that has highrates of psychiatric comorbidity7,8 when com-pared with nonarrested peers.9 Several studiesalso demonstrate strong relationships betweensubstance use and arrests for both violent andnonviolent crime.10,11 Studies have found thatdetained youth were more than twice as likely asthose not incarcerated to have an externalizingdisorder.7 Other studies based on juvenile justicesamples found that, on average, nearly one-fourth of the youth met criteria for any affectivedisorder or anxiety disorder, and as many as one-half met criteria for any disruptive behavior dis-order or any substance use disorder.8 In addition,research based on self-reported offending pat-terns among large-scale adolescent communitysamples found that violent offenders had signif-icant externalizing symptoms12 and dispropor-tionately used alcohol and marijuana.13
The extent and strength of association betweencrime and mental illness in adolescence in thegeneral US population is unclear. Furthermore, weknow little about the association between mentalillness and crime among youth who are not arres-ted. This is an important limitation, because only asmall percentage of youth are arrested for theircrimes, and even fewer are referred to juvenilecourt.14 Most offenses committed by youth includestatus offenses, property offenses, and some violentoffenses that do not result in serious injury andtherefore are not reported to the authorities.14 It isalso unknown whether existing findings from jus-tice or community-based samples of youth applymore broadly to the larger portion of youth andcrimes that are not reported to criminal justiceagencies,13,15 highlighting the importance of exam-ining this issue in epidemiological-level samples.
The present study examined self-reported ar-rests and crime using data from the NationalComorbidity Survey–Adolescent Supplement(NCS-A). The NCS-A is the only nationallyrepresentative sample available that includesDSM-IV–based diagnostic data on youth aged 13to 18 years16 and includes reported crime. Thegoals of this report are to describe the relationshipbetween specific psychiatric disorders and re-ported crime involvement (violent, property,other), distinguishing between youths arrestedfor crime versus youth who have never beenarrested; and to examine whether associ-ations between psychiatric disorders and crime
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME 53 NUMBER 8 AUGUST 2014
strengthen with increasing numbers of psychiat-ric comorbidities.
METHODThe NCS-A is a nationally representative, face-to-facesurvey that was administered to adolescents (aged13–17 years) between February 2, 2001, and January 31,2004, by professional interviewers from the Institute forSocial Research at the University of Michigan, AnnArbor. The NCS-A used a dual-frame sample thatincluded household and school subsamples.16,17 Thehousehold sample consisted of 904 adolescents, and theschool sample consisted of 9,244 adolescents. Theresponse rates were 82.5% for the household sampleand 83.7% for the school sample. The Human SubjectsCommittee of both Harvard Medical School and theUniversity of Michigan approved the recruitment andconsent procedures. The study also obtained a certifi-cate of confidentiality, and this was documented andexplained in the parental and adolescent consent forms.The interviewers answered questions and addressedconcerns regarding participation before obtainingwritten informed consent from the parent and writteninformed assent from the adolescent. After completionof the surveys, cases were weighted for variation inwithin-household likelihood of selection (in thehousehold sample) and for residual variations betweenthe sample and the US population based on socio-demographic and geographic variables. Additional in-formation on weighting procedures can be found in theNCS-A user guide.17,18 Overall, approximately one-halfof the sample was male (51.3%), with slightly fewerfemales (48.7%), and the mean age was 15.2 years. Alarger proportion of the sample were youth betweenthe ages of 13 and 14 years (36.2%), and the remainingage distribution of the sample was relatively equalbetween youth aged 15 to 16 and 17 to 18 years. Thesample consisted of 65.6% non-Hispanic white, 15.1%non-Hispanic black, and 14.4% Hispanic adolescents.
MeasuresAssessment of DSM-IV Disorders. Adolescents wereadministered the World Health Organization Com-posite International Diagnostic Interview (CIDI), astructured interview to determine DSM-IV diagnoses,which was modified for administration to adoles-cents.16,19 Anxiety disorders, behavioral disorders,eating disorders, mood disorders, and substance usedisorders were assessed based on lifetime DSM-IVcriteria and exclusion rules. With the exception ofoppositional defiant disorder (ODD) with or withoutconduct disorder (CD) and substance use disorders(SUD; abuse and dependence), all other diagnoses weremade using the DSM-IV diagnostic hierarchy rules.The NCS-A used specific evidence-based probing pro-cedures to improve the participants’ recall, whichincreased reliability in identifying lifetime disorderprevalence.20,21
Y
www.jaacap.org 889
COKER et al.
Arrests and Offending Variables. Adolescents wereasked about their involvement in crimes and whetheror not these crimes had led to arrest. The participantswere asked whether they “ever had any of thefollowing experiences: being arrested for a propertycrime, such as theft or burglary; being arrested for aviolent crime, such as assault or armed robbery; beingarrested for any other type of crime; committing aproperty crime, but not getting caught or arrested;committing a violent crime, but not getting caught orarrested; committing any other type of crime, but notgetting caught or arrested.” The participants were notasked any additional information about the actual re-ported crime. When examining arrests with crime, weanalyzed data from the entire sample. When examiningcrimes without arrest, we selected for youth who hadnever been arrested (n ¼ 9,397). This was done to studyassociations between mental illness and crime, differ-entiating between youth who did and did not reportinvolvement with the criminal justice system.
Summary of Analyses. We conducted all analysesusing Stata version 13.0.22 All analyses accounted forthe survey design using procedures specified in theNCS-A documentation.17,18 We calculated a series oflogistic regression models to compare the odds ofcrime outcomes among youth with psychiatricdisorders to those with no lifetime psychiatric di-agnoses. For example, when examining the associa-tion between attention-deficit/hyperactivity disorder(ADHD) and arrests for violent crime, we calculatedthe odds ratio (OR) for violent crime, comparingyouth with a lifetime ADHD diagnosis to thosewithout any lifetime diagnoses. When calculatingthese estimates, we controlled for age, gender, income,and race/ethnicity. To account for multiple testing,we used a Bonferroni-adjusted significance cut-off ofp � .00036. In our second series of models, we exam-ined the odds of committing crime for youth with 0, 1,2, or 3 or more psychiatric diagnoses. Using outcomessimilar to those outlined above, we used logisticregression to calculate these estimates, controlling forage, gender, income, and race/ethnicity. We con-ducted analyses for the overall sample, and then afterexcluding youth with a CD diagnosis. In our finalanalyses, we calculated population attributable frac-tions (PAF) of reporting any crime (with or withoutarrest) for each category of number of diagnoses. First,we calculated the OR of committing any crime asso-ciated with each group, adjusting for age, gender,income, and race/ethnicity. We then converted theseOR estimates to relative risks using the followingformula: RRe ¼ ORe=½ð1� PoÞ þ ðPo*OReÞ�, where Po
is the prevalence of the outcome in the nonexposedgroup (0 diagnoses), ORe is the OR associated with theexposure, and RRe is the risk ratio associated with theexposure. Using these relative risks, we calculatedpopulation attributable fractions for each category ofnumber of diagnoses using the following formula:
JOURN
890 www.jaacap.org
PAF ¼ PeðRRe � 1Þ=½1þ PeðRRe � 1Þ�, where Pe is theprevalence of the exposure group.
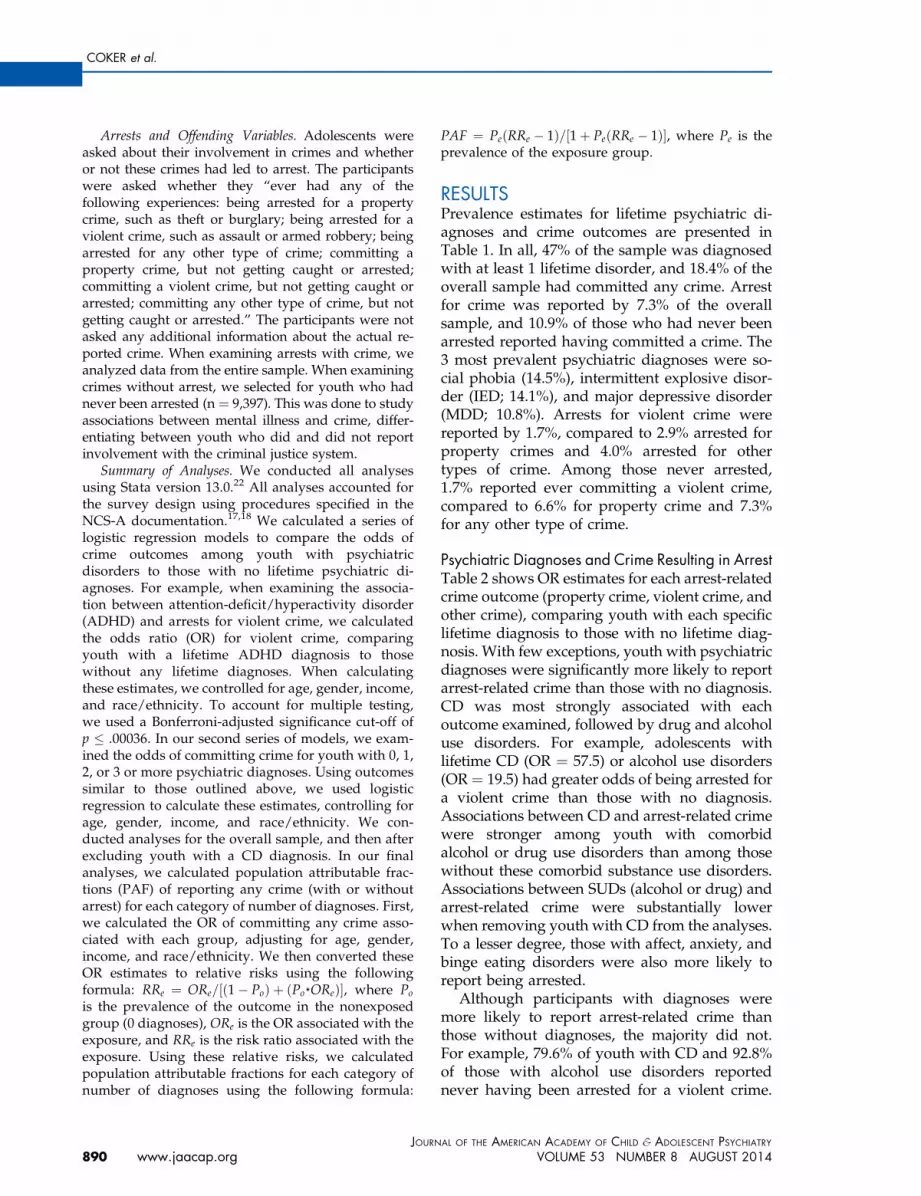
RESULTSPrevalence estimates for lifetime psychiatric di-agnoses and crime outcomes are presented inTable 1. In all, 47% of the sample was diagnosedwith at least 1 lifetime disorder, and 18.4% of theoverall sample had committed any crime. Arrestfor crime was reported by 7.3% of the overallsample, and 10.9% of those who had never beenarrested reported having committed a crime. The3 most prevalent psychiatric diagnoses were so-cial phobia (14.5%), intermittent explosive disor-der (IED; 14.1%), and major depressive disorder(MDD; 10.8%). Arrests for violent crime werereported by 1.7%, compared to 2.9% arrested forproperty crimes and 4.0% arrested for othertypes of crime. Among those never arrested,1.7% reported ever committing a violent crime,compared to 6.6% for property crime and 7.3%for any other type of crime.
Psychiatric Diagnoses and Crime Resulting in ArrestTable 2 shows OR estimates for each arrest-relatedcrime outcome (property crime, violent crime, andother crime), comparing youth with each specificlifetime diagnosis to those with no lifetime diag-nosis. With few exceptions, youth with psychiatricdiagnoses were significantly more likely to reportarrest-related crime than those with no diagnosis.CD was most strongly associated with eachoutcome examined, followed by drug and alcoholuse disorders. For example, adolescents withlifetime CD (OR ¼ 57.5) or alcohol use disorders(OR ¼ 19.5) had greater odds of being arrested fora violent crime than those with no diagnosis.Associations between CD and arrest-related crimewere stronger among youth with comorbidalcohol or drug use disorders than among thosewithout these comorbid substance use disorders.Associations between SUDs (alcohol or drug) andarrest-related crime were substantially lowerwhen removing youth with CD from the analyses.To a lesser degree, those with affect, anxiety, andbinge eating disorders were also more likely toreport being arrested.
Although participants with diagnoses weremore likely to report arrest-related crime thanthose without diagnoses, the majority did not.For example, 79.6% of youth with CD and 92.8%of those with alcohol use disorders reportednever having been arrested for a violent crime.
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 53 NUMBER 8 AUGUST 2014
TABLE 1 Frequencies for Specific Disorders, PsychiatricComorbidity Subgroups, and Crime Outcomes(N ¼ 10,123)
Disorder or Diagnosis
Total sample
n %
Attention/disruptive behavior/impulse control disordersADHD 432 4.15CD 586 5.44Without alcohol or drug abuse 278 2.65With alcohol or drug abuse 308 2.79
IED 1,389 14.09ODD 1,047 10.14
Affective disordersBipolar (I or II) 231 2.27Dysthymia 335 0.34MDD 1,123 10.82
Anxiety disordersAgoraphobia 293 2.66GAD 298 3.19Panic disorder 238 2.35PTSD 388 4.01SAD 772 7.63Social phobia 1,434 14.46
Eating DisordersAny binge disorder 532 4.95
SUDsa
Alcohol use disorders 678 6.43Drug use disorders 880 8.93Nicotine dependence 713 7.04
No. of diagnoses0 5,402 52.61 2,009 20.62 1,110 10.93þ 1,627 15.96
CrimeArrestedProperty/theft/burglary 281 2.89Violent 175 1.74Other 420 4.03
Never arrestedb
Property/theft/burglary 621 6.55Violent 185 1.71Other 671 7.29
Note: Percentages accounted for the survey design. Listed diagnosesare lifetime prevalence. ADHD ¼ attention-deficit/hyperactivity dis-order; CD ¼ conduct disorder; GAD ¼ generalized anxiety disor-der; IED ¼ intermittent explosive disorder; MDD ¼ major depressivedisorder; ODD ¼ oppositional defiant disorder; PTSD ¼ post-traumatic stress disorder, SAD ¼ separation anxiety disorder;SUDs ¼ substance use disorders.aAlcohol use disorders (abuse þ dependence); drug use disorders
(abuse þ dependence; note that the Composite InternationalDiagnostic Interview [CIDI] skip patterns do not assess depen-dence in the absence of abuse); Nicotine dependence (withoutalcohol or drug use disorder).
bn ¼ 9,397.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME 53 NUMBER 8 AUGUST 2014
CRIME AND PSYCHIATRIC DISORDERS IN YOUTH
This pattern was particularly true for those withaffect, anxiety, and eating disorders. The largeORs in Table 1 are due to comparisons with ratesof arrested crime that were near zero amongthose without psychiatric diagnoses; for example,there was a rate of 0.37% for violent crime arrestsin this subpopulation.
Psychiatric Diagnoses and Committed CrimeWithout ArrestsThe pattern of findings for reports of crime amongyouth who reported never having been arrestedwas similar to the pattern presented above forcrimes with arrest (Table 3). Similar to crimes withan arrest, youth with diagnoses who were neverarrested were substantially more likely to reportcorresponding crimes. The highest rates of crimewere again found among youth with lifetimeconduct, drug, or alcohol use disorders. Similar towhen examining arrest-related crime, associationsbetween CD and crime among those not arrestedwere stronger among respondents with comorbidalcohol or drug use disorders than among thosewithout these comorbid SUDs. However, associa-tions between substance use disorders (alcohol ordrug) and arrest-related crime did not substan-tially decrease when removing youth with CDfrom the analyses. The majority of youth withpsychiatric diagnoses who had never been arres-ted reported they had never committed acrime (88.2%).
Psychiatric Comorbidity and Crime Outcomes,Overall SampleApproximately 21% of the overall sample had 1psychiatric diagnosis, 10.7% had 2, and 16.1%had 3 or more. Of those with 1 diagnosis, themost common disorders were social phobia(20.1%), IED (19.7%), and separation anxietydisorder (SAD; 10.0%). The most common disor-ders among those with 2 diagnoses were IED(28.3%), social phobia (30.0%), and MDD (21.9%).Of those with 3 or more diagnoses, the mostcommon disorders were again social phobia(40.8%), IED (43.5%), and MDD (40.8%).
Tables 2 and 3 display associations betweenpsychiatric comorbidity and all crime outcomes.We compared those with 1, 2, and 3 or more di-agnoses to those with no diagnoses. Having greaternumbers of diagnoses was generally associatedwith increasingly higher prevalence of crime for alloutcomes. For example, youth with 1 diagnosishad 6.3 times greater odds of reporting arrest for aviolent crime compared to those with no diagnoses,
Y
www.jaacap.org 891

TABLE 2 Prevalence and Odds Ratios for Crimes With Arrest Based on Specific Diagnoses (N ¼ 10,123)
Diagnosisa
Property Crime/Theft/Burglary Arrest
ViolentCrime Arrest
Any OtherCrime Arrest
% OR 95% CI % OR 95% CI % OR 95% CI
No lifetime disorder 0.84 Ref. — 0.37 Ref. — 1.08 — Ref.Attention/disruptivebehavior/impulse CDsADHD 4.84 4.96* 2.58, 9.54 6.80 18.49* 8.80, 38.85 10.47 9.54* 5.67, 16.05CD 22.70 30.65* 17.02, 55.18 20.42 57.47* 30.35, 108.82 34.11 38.21* 22.71, 64.28Without alcohol or
drug use disorder19.84 25.93* 12.30, 54.67 20.59 49.05* 23.88, 100.76 22.47 20.24* 9.73, 42.09
With alcohol or druguse disorder
25.19 35.18* 17.43, 71.02 20.25 61.67* 32.19, 118.13 45.19 54.74* 31.62, 94.77
IED 5.30 6.17* 3.25, 11.70 4.29 11.00* 5.73, 21.11 9.81 8.80* 5.56, 13.91ODD 6.36 7.55* 4.56, 12.49 4.54 11.80* 6.88, 20.23 12.96 12.67* 7.34, 21.89
Affective DisordersBipolar (I or II) 11.70 17.17* 7.49, 39.34 4.45 11.60* 5.46, 24.67 8.16 7.02* 3.10, 15.92Dysthymia 4.03 6.25* 2.83, 13.82 5.16 16.91* 8.88, 32.22 10.19 11.17* 5.37, 23.22MDD 4.63 6.50* 3.91, 10.80 2.90 9.53* 5.13, 17.70 7.60 7.84* 4.43, 13.86
Anxiety DisordersAgoraphobiab 0.86 1.33 0.44, 4.04 5.72 18.91* 5.57, 64.15 4.91 5.46* 3.16, 9.41GAD 5.53 9.73* 4.86, 19.48 1.56 4.66* 2.05, 10.59 5.94 6.35* 3.27, 12.38Panic disorder 5.27 4.96* 2.33, 10.59 2.69 6.28* 2.64, 14.92 5.28 4.78 1.69, 13.58PTSD 3.94 7.88* 3.89, 15.97 2.92 11.76* 5.68, 24.33 9.51 14.15* 7.12, 28.13SAD 2.56 3.34 1.52, 7.32 2.82 8.57* 3.86, 19.01 4.76 4.71* 2.88, 7.70Social Phobia 4.41 5.45 2.34, 12.67 2.31 6.99* 3.31, 14.75 5.68 5.46* 3.54, 8.42
Eating DisordersAny binge disorder 3.71 5.04 2.13, 11.94 3.43 9.42* 3.21, 27.66 5.38 5.33* 3.28, 8.66
SUDsc
Alcohol use disorder 13.06 18.94* 9.91, 36.22 7.25 19.47* 8.79, 43.15 21.65 19.42* 13.08, 28.83Drug use disorder 13.40 18.62* 10.19, 34.03 6.24 16.06* 9.32, 27.66 20.93 18.54* 11.68, 29.42Nicotine dependence 7.76 12.19 4.59, 32.36 6.09 15.55* 6.78, 35.63 9.33 9.32* 4.83, 17.98
No. of diagnoses0 0.84 Ref. — 0.36 Ref. — 1.08 Ref. —
1 2.91 3.56* 1.83, 6.93 2.22 6.26* 3.09, 12.68 3.42 3.13* 1.81, 5.402 4.94 6.32* 3.33, 11.98 1.39 3.59 1.23, 10.47 4.85 4.26* 2.59, 6.993þ 8.19 10.49* 6.20, 17.78 5.88 16.07* 9.53, 27.09 13.97 13.26* 8.63, 20.39
Note: All estimates accounted for the survey design. Estimates were adjusted for income, age, gender, and race/ethnicity. ADHD ¼ attention-deficit/hyperactivity disorder; CD ¼ conduct disorder; GAD ¼ generalized anxiety disorder; IED ¼ intermittent explosive disorder; MDD ¼ major depres-sive disorder; ODD ¼ oppositional defiant disorder; OR ¼ odds ratio, calculated using logistic regression; PTSD ¼ posttraumatic stress disorder; Ref. ¼reference; SAD ¼ separation anxiety disorder; SUDs ¼ substance use disorder.aListed diagnoses are lifetime prevalence.bAgoraphobia with/without panic disorder.cAlcohol use disorders (abuse þ dependence); drug use disorders (abuse þ dependence; note that the Composite International Diagnostic Interview
[CIDI] skip patterns do not assess dependence in the absence of abuse); nicotine dependence (without alcohol or drug use disorder).*p � .00036 (Bonferroni-adjusted p value).
COKER et al.
and those with 3 or more diagnoses had 15.7 timesgreater odds of reporting arrest for a violent crime.Similar patterns were found when examining crimeamong youth who had not been arrested.
Figure 1 displays the proportions of youthreporting crime accounted for by each psychi-atric comorbidity subgroup. Adolescents withmultiple diagnoses accounted for a substantiallygreater proportion of those reporting crime than
JOURN
892 www.jaacap.org
would be expected given their populationprevalence. For example, those with 3 or morediagnoses made up 16.1% of the population butaccounted for nearly 54% of those reporting vi-olent crimes with an arrest (and 48% of thosewho had never been arrested and reported vio-lent crime). This was in comparison to youthwho had no diagnoses, making up approxi-mately 50% of the population but accounting for
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 53 NUMBER 8 AUGUST 2014
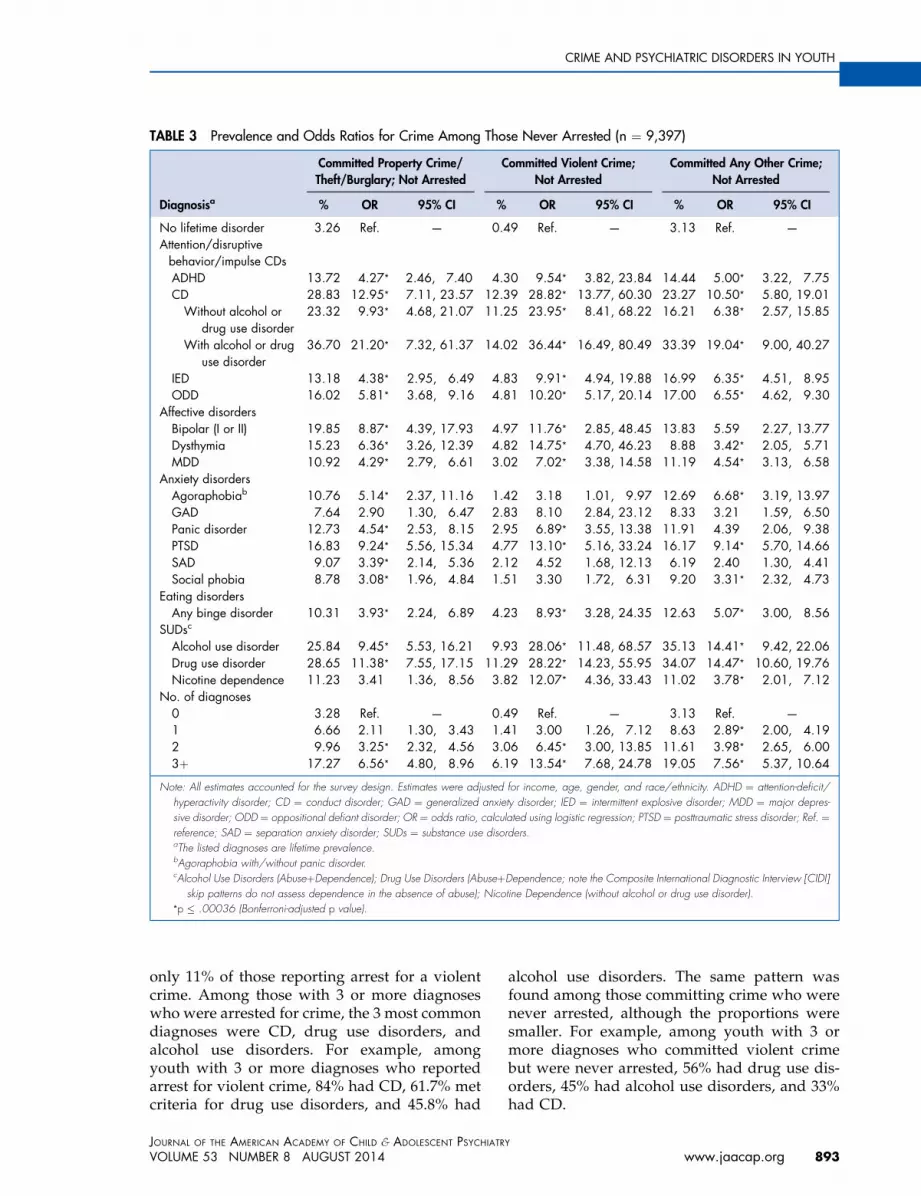
TABLE 3 Prevalence and Odds Ratios for Crime Among Those Never Arrested (n ¼ 9,397)
Diagnosisa
Committed Property Crime/Theft/Burglary; Not Arrested
Committed Violent Crime;Not Arrested
Committed Any Other Crime;Not Arrested
% OR 95% CI % OR 95% CI % OR 95% CI
No lifetime disorder 3.26 Ref. — 0.49 Ref. — 3.13 Ref. —
Attention/disruptivebehavior/impulse CDsADHD 13.72 4.27* 2.46, 7.40 4.30 9.54* 3.82, 23.84 14.44 5.00* 3.22, 7.75CD 28.83 12.95* 7.11, 23.57 12.39 28.82* 13.77, 60.30 23.27 10.50* 5.80, 19.01Without alcohol or
drug use disorder23.32 9.93* 4.68, 21.07 11.25 23.95* 8.41, 68.22 16.21 6.38* 2.57, 15.85
With alcohol or druguse disorder
36.70 21.20* 7.32, 61.37 14.02 36.44* 16.49, 80.49 33.39 19.04* 9.00, 40.27
IED 13.18 4.38* 2.95, 6.49 4.83 9.91* 4.94, 19.88 16.99 6.35* 4.51, 8.95ODD 16.02 5.81* 3.68, 9.16 4.81 10.20* 5.17, 20.14 17.00 6.55* 4.62, 9.30
Affective disordersBipolar (I or II) 19.85 8.87* 4.39, 17.93 4.97 11.76* 2.85, 48.45 13.83 5.59 2.27, 13.77Dysthymia 15.23 6.36* 3.26, 12.39 4.82 14.75* 4.70, 46.23 8.88 3.42* 2.05, 5.71MDD 10.92 4.29* 2.79, 6.61 3.02 7.02* 3.38, 14.58 11.19 4.54* 3.13, 6.58
Anxiety disordersAgoraphobiab 10.76 5.14* 2.37, 11.16 1.42 3.18 1.01, 9.97 12.69 6.68* 3.19, 13.97GAD 7.64 2.90 1.30, 6.47 2.83 8.10 2.84, 23.12 8.33 3.21 1.59, 6.50Panic disorder 12.73 4.54* 2.53, 8.15 2.95 6.89* 3.55, 13.38 11.91 4.39 2.06, 9.38PTSD 16.83 9.24* 5.56, 15.34 4.77 13.10* 5.16, 33.24 16.17 9.14* 5.70, 14.66SAD 9.07 3.39* 2.14, 5.36 2.12 4.52 1.68, 12.13 6.19 2.40 1.30, 4.41Social phobia 8.78 3.08* 1.96, 4.84 1.51 3.30 1.72, 6.31 9.20 3.31* 2.32, 4.73
Eating disordersAny binge disorder 10.31 3.93* 2.24, 6.89 4.23 8.93* 3.28, 24.35 12.63 5.07* 3.00, 8.56
SUDsc
Alcohol use disorder 25.84 9.45* 5.53, 16.21 9.93 28.06* 11.48, 68.57 35.13 14.41* 9.42, 22.06Drug use disorder 28.65 11.38* 7.55, 17.15 11.29 28.22* 14.23, 55.95 34.07 14.47* 10.60, 19.76Nicotine dependence 11.23 3.41 1.36, 8.56 3.82 12.07* 4.36, 33.43 11.02 3.78* 2.01, 7.12
No. of diagnoses0 3.28 Ref. — 0.49 Ref. — 3.13 Ref. —
1 6.66 2.11 1.30, 3.43 1.41 3.00 1.26, 7.12 8.63 2.89* 2.00, 4.192 9.96 3.25* 2.32, 4.56 3.06 6.45* 3.00, 13.85 11.61 3.98* 2.65, 6.003þ 17.27 6.56* 4.80, 8.96 6.19 13.54* 7.68, 24.78 19.05 7.56* 5.37, 10.64
Note: All estimates accounted for the survey design. Estimates were adjusted for income, age, gender, and race/ethnicity. ADHD ¼ attention-deficit/hyperactivity disorder; CD ¼ conduct disorder; GAD ¼ generalized anxiety disorder; IED ¼ intermittent explosive disorder; MDD ¼ major depres-sive disorder; ODD ¼ oppositional defiant disorder; OR ¼ odds ratio, calculated using logistic regression; PTSD ¼ posttraumatic stress disorder; Ref. ¼reference; SAD ¼ separation anxiety disorder; SUDs ¼ substance use disorders.aThe listed diagnoses are lifetime prevalence.bAgoraphobia with/without panic disorder.cAlcohol Use Disorders (AbuseþDependence); Drug Use Disorders (AbuseþDependence; note the Composite International Diagnostic Interview [CIDI]
skip patterns do not assess dependence in the absence of abuse); Nicotine Dependence (without alcohol or drug use disorder).*p � .00036 (Bonferroni-adjusted p value).
CRIME AND PSYCHIATRIC DISORDERS IN YOUTH
only 11% of those reporting arrest for a violentcrime. Among those with 3 or more diagnoseswho were arrested for crime, the 3 most commondiagnoses were CD, drug use disorders, andalcohol use disorders. For example, amongyouth with 3 or more diagnoses who reportedarrest for violent crime, 84% had CD, 61.7% metcriteria for drug use disorders, and 45.8% had
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME 53 NUMBER 8 AUGUST 2014
alcohol use disorders. The same pattern wasfound among those committing crime who werenever arrested, although the proportions weresmaller. For example, among youth with 3 ormore diagnoses who committed violent crimebut were never arrested, 56% had drug use dis-orders, 45% had alcohol use disorders, and 33%had CD.
Y
www.jaacap.org 893

FIGURE 1 Percentages of crime accounted for by youth with varying numbers of psychiatric diagnoses, relative topopulation prevalence. Note: Estimates were calculated using logistic regression, accounting for the survey design.Results showed that despite making up a smaller portion of the total population, adolescents with substantial psychiatriccomorbidity accounted for a much larger portion of reported crime. For example, youth with no psychiatric diagnosesmade up more than 50% of the population, and accounted for 15.8% of those never arrested who committed violentcrime, whereas youth with 3 or more diagnoses made up only 16.0% of the population, and accounted for 48.4% ofthose never arrested who committed violent crime.
COKER et al.
Psychiatric Comorbidity and Crime Outcomes,Excluding Those With CDSupplemental Tables 1 and 2 (available online)display associations between specific psychiatricdiagnoses and crime outcomes, excluding youthwith a CD diagnosis from the sample. Themajority of associations between psychiatric di-agnoses and arrest-related crime became non-significant after youth with CD were removedfrom the sample. For example, for violent crimearrest, only associations with agoraphobia andnicotine dependence (without comorbid alcoholor drug abuse) remained significant. For prop-erty crime/theft/burglary, only associationswith alcohol and drug use disorders remainedsignificant. When examining reports of crimeamong youth who had never been arrested,removing those with a CD diagnosis had lessimpact on the results. The majority of associa-tions with property crime/theft/burglary, violent
JOURN
894 www.jaacap.org
crime, and other crime remained significant.Associations with anxiety disorders were mostlikely to become nonsignificant after removingCD, although associations with posttraumaticstress disorder (PTSD) remained significant for all3 crime outcomes.
Population Attributable FractionsFigure 2 displays population attributable frac-tions (PAF) of committing any crime associatedwith each number of diagnoses. PAF can beinterpreted as the maximum expected reductionin crime that could be expected if each groupwere no longer included in the population,assuming a fully causal association. Results arepresented both with and without youth with CDincluded in the analyses. Including youth withCD, PAF was highest for those with 3 or morediagnoses (43.6%). In total, one could expect amaximum 85.8% reduction in crime if all mental
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 53 NUMBER 8 AUGUST 2014

CRIME AND PSYCHIATRIC DISORDERS IN YOUTH
illness were eliminated from US adolescents.Excluding those with CD, one could expect amaximum 67.9% reduction in crime.
DISCUSSIONThe NCS-A Supplement was analyzed to examine,for the first time, associations between psychiatricdisorders and reported crime involvement amongyouth with and without an arrest history in a na-tionally representative sample. We found that18.4% of the sample reported engaging in crime.Of particular note, 10.9% of the sample reportedcommitting crime but never being arrested, whichis consistent with existing literature suggestingthat most crime goes undetected14 and highlightsthe importance of examining this issue among thegeneral population of youth. Overall, the analysesrevealed that youth with lifetime externalizing
FIGURE 2 Population attributable fraction (PAF) ofyouth who committed any crime, by number ofdiagnoses. Note: results are presented both with andwithout youth with conduct disorder (CD) included in thesample. One could expect up to 86% of crime to bereduced if there were no mental illness (68% when youthwith CD were eliminated from the sample). PAF wascalculated using the following formula:PAF ¼ PeðRRe � 1Þ=½1þ PeðRRe � 1Þ�, where Pe is theprevalence of the exposure group and RRe is the relativerisk associated with the exposure group. To obtain RRe,odds ratios (ORs) were calculated using logisticregression, accounting for the survey design andadjusting for income, age, gender, and race/ethnicity.These ORs (ORe) were then converted to RRe using thefollowing formula: RRe ¼ ORe=½ð1� PoÞ þ ðPo*OReÞ�,where Po is the prevalence of the outcome in the non-exposed group (0 diagnoses).
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME 53 NUMBER 8 AUGUST 2014
and SUDs were significantly more likely thanthose without any psychiatric disorders to reportinvolvement in crime. CD, drug use disorders,and alcohol use disorders generally demonstratedgreater odds of crime involvement when com-pared to internalizing disorders such as anxietyand affective disorders. Overall, youth with atleast 1 diagnosis committed 85.8% of crime, whichwas reduced to 67.9% by removing those with CD.Our findings also revealed a strong relationshipbetween psychiatric comorbidity and crime,including crimes among those who were neverarrested. Youth with 3 or more diagnoses were athighest risk for reported involvement in crime,including violent, property, and other types ofcrime. However, it is important to note that 88.2%of youth with mental illness reported never havingcommitted any crime.
The high rates of crime evidenced in youthwith externalizing and SUDs is consistent withthe literature demonstrating that these youth tendto be impulsive and often fail to consider conse-quences or merely disregard rules and regula-tions.6 Studies have shown that youth who abusesubstances were likely to engage in criminal ac-tivities such as property and person offenses toobtain drugs.24 Thus, diverting these youth intosubstance abuse treatment may prevent themfrom getting involved in crimes that arecommitted to support their substance use. Also,involvement in drug-related crimes places theseyouth at higher risk for engaging in violence andbecoming victims of violence.25
Although most delinquency is limited toadolescence,23 this warrants attention, as CD is anidentified risk factor for criminal behavior inadulthood.6,26 It is important to note that associ-ations between CD and crime are high, as CDrepresents a collection of behaviors that violatesocietal norms, and most of these behaviors arecriminal offenses. Thus criminal activity repre-sents both predictor and outcome in the case ofCD and crime. To address this tautology, weremoved the effect of CD and continue to findhigh rates of crime among those with psychiatricdiagnosis but without CD diagnosis. Moreover,CD was of particular importance when exam-ining arrests, as most of the associations betweenpsychiatric diagnoses and arrests were no longersignificant when youth with CD were removedfrom the sample. However, associations withcrime that did not result in arrest mostlyremained significant and strong after removingyouth with CD. This suggests that comorbidity
Y
www.jaacap.org 895

COKER et al.
with CD may be less important as a determinantof whether youth with psychiatric disorders aremore likely to commit crime, but more importantin determining whether crime results in arrest.Given the available data in the NCS-A Supple-ment, we were unable to determine what may bedriving the association between CD and arrest;however, it is possible that youth with CDcommitted more frequent and/or more seriouscrimes.
Although internalizing disorders generallyhad lower associations with crime whencompared to externalizing and SUDs, internal-izing disorders also conferred significant associ-ations with crime. Both anxiety and affectivedisorders demonstrate significant associationswith crime, and increased risk of arrest.6,8 Forexample, studies have found alarmingly highrates of PTSD in juvenile justice samples,27 butless is known about these rates among youth incommunity settings who engage in crime.6 Thecurrent data showed strong associations betweencrime and internalizing disorders that areconsistent with literature suggesting that treatinganxiety and affective disorders may be a criticalfactor in reducing future risk of crime.28,29
Psychiatric comorbidity resulted in strong as-sociations with crime involvement. Youth with 3or more psychiatric diagnoses accounted for only16% of the sample, yet these youth accounted for54% of those reporting arrest for a violent crime.Among this subsample, CD and drug and alcoholuse disorders were disproportionately represented.There has been ample research documenting thehigh rates of psychiatric comorbidity in detainedand correctional juvenile samples.7,8 However, toour knowledge, this is the first study to date todocument the high rates of psychiatric comorbidityamong youth who commit crime in a nationallyrepresentative community-based sample of youth.The findings from this study revealed that manyyouth with greater psychiatric comorbidity do notnecessarily end up in the juvenile justice system.There were substantial numbers of youth with 3 ormore diagnoses reporting crime and never havingbeen arrested, highlighting the importance ofcommunity-based services designed to engage at-risk youth.
Our findings demonstrate the importance ofimproving psychiatric and substance use assess-ment, prevention, and intervention efforts foryouthful offenders outside of the juvenile justicesystem. Our data revealed that many youth arenot arrested for their crimes, particularly for
JOURN
896 www.jaacap.org
nonviolent crimes. For instance, 29% of youthwith a drug use diagnosis reported that they hadcommitted a property crime and had never beenarrested, yet only 13% of youth with this diag-nosis reported having been arrested for commit-ting a property crime. Therefore, useful strategiesmay include expanding early detection of psy-chiatric disorders as well as school- and/orcommunity-based services for youth.
Studies have already also shown a significantrelationship between persistent drug use andpersistent delinquency30 and juvenile crime andpsychiatric comorbidity. Although Moffitt23
argued that the majority of youth are adoles-cence-limited offenders, there is considerablevalue in identifying youth who will become life-course persistent offenders due to their psychi-atric illness, including addiction.31 Improvingaccess to treatment can be instrumental inbreaking a link in the pathway from juveniledelinquency to adult offending. Proper identifi-cation of youth for whom offending is related totheir substance use and/or psychiatric illness iscrucial because it allows them to receive appro-priate treatment. Also, providing interventions tothose who do not need it may be unnecessary ormay even have criminogenic effects.30 Our find-ings echo the need to treat delinquency not withpunitive sanctions but rather through greateremphasis on psychiatric and substance use pre-vention programs and interventions.32 Youthwho receive treatment are at lower risk for sub-sequent incarceration,31 and community-basedservices as well as diversion programs can pro-vide effective treatment without compromisingpublic safety.32 Furthermore, CD does not inevi-tably lead to adult offending, and there areseveral interventions documented in the litera-ture that are promising in the treatment ofbehavioral disorders among community-basedand justice-involved youth.33,34
There are several limitations to this study.First, criminal involvement was based entirely onyouth self-report and was not supplemented withofficial crime data. Youth may underreport theircriminal involvement. However, studies haveshown that adolescents accurately report delin-quent involvement and, albeit not perfect, self-report is a more comprehensive measure of thetrue extent of delinquency.14,30,35,36 Self-reportcan capture adolescents who are not included incrime statistics, including many adolescents whoare not arrested for their involvement in illegalbehaviors and thus fail to come into contact with
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 53 NUMBER 8 AUGUST 2014

CRIME AND PSYCHIATRIC DISORDERS IN YOUTH
the juvenile justice system.14,30,35,36 Moreover,experts argue that we need more studies aboutthe psychiatric needs of youth who commitcrimes but do not come to the attention of theauthorities.6 Consistent with existing literaturearguing that most youth are not arrested for theirdelinquent behavior, our data revealed that thepercentages of youth reporting involvement incrime not resulting in arrest was higher than thepercentages of youth reporting being arrested forthose same crimes, with the exception of violentcrime. The CIDI questions the respondent aboutdependence only when criteria for abuse are met,which may lead to underdiagnosing alcohol and/or drug dependence in the absence of abuse.37
There were no follow-up questions for theyouth to specify their actual crimes, which mayhave distinguished severity of offenses withincategories. Furthermore, there was no specifica-tion of the types of crime that fell in the “anyother crime” category, and having this informa-tion may have allowed further elucidation of thehigher percentages seen in this category. Becausedrug use is a crime, the high percentages of youthwith SUDs in the “any other crime” category mayhave been for drug-related arrests such as sellingor possession of narcotics. In addition, the datasetdid not include information about any of thedevelopmental disorders or psychotic spectrumdisorders, both of which are associated withincreased risk for crime.35
It is possible that youth with mental illnessmay have been less inhibited and consequentlymore likely or willing to report criminalinvolvement. However, our data show that for alldiagnostic categories, despite higher rates ofreporting crime involvement among mentally illyouth, the majority of youth with psychiatricdisorders reported no criminal involvement at all.Also, the cross-sectional nature of this designdoes not allow us to evaluate whether psychiatricdisorders preceded crime involvement. Using a
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME 53 NUMBER 8 AUGUST 2014
longitudinal design with a nationally represen-tative sample would help clarify the time courseof the relationship between psychiatric disordersand crime in youth.
Despite these limitations, our results revealedthat youth with psychiatric disorders and morepsychiatric comorbidity were significantly morelikely to report involvement in arrest-related vi-olent and nonviolent crimes. This same patternwas evident for reported involvement in violentand nonviolent crimes among youth who werenever arrested. Most of the literature on psychi-atric disorders and crime among youth are basedon juvenile justice samples; but, as previouslynoted, many crimes go unreported or undetected.The current study demonstrates that evenamong youth who have not been involved in thecriminal justice system, those with psychiatricdisorders are disproportionately involved incrime, suggesting the need for improving accessto community-based mental health services. &
Y
Accepted June 6, 2014.
This article was reviewed under and accepted by deputy editorDouglas K. Novins, MD.
Drs. Coker, Smith, Westphal, Zonana, and McKee are with YaleUniversity School of Medicine, New Haven, CT. Dr. Smith is also withthe School of Public Health at Yale University School of Medicine. Dr.Westphal is also with the Yale Child Study Center.
Support for this research was provided by National Institutes of Healthgrants T32DA007238, T32MH014235, and the State of Con-necticut Department of Mental Health and Addiction Services.
Dr. Smith served as the statistical expert for this research.
Disclosure: Dr. Westphal has received funding from the Alan B. SlifkaFoundation and Fondation Rumsey Cartier. Dr. McKee has receivedinvestigator-initiated grants from Pfizer to study vareniclineealcoholinteractions. Drs. Coker, Smith, and Zonana report no biomedicalfinancial interests or potential conflicts of interest.
Correspondence to Sherry McKee PhD, Yale University School ofMedicine, 2 Church Street South, Suite 109, New Haven, CT06519; e-mail: [email protected]
0890-8567/$36.00/ª2014 American Academy of Child andAdolescent Psychiatry
http://dx.doi.org/10.1016/j.jaac.2014.05.007
REFERENCES
1. Elbogen EB, Johnson SC. The intricate link between violence andmental disorder: results from the National Epidemiologic Survey onAlcoholandRelatedConditions.ArchGenPsychiatry. 2009;66:152-161.
2. Van Dorn R, Volavka J, Johnson N. Mental disorder and violence:is there a relationship beyond substance use? Soc PsychiatryPsychiatr Epidemiol. 2012;47:487-503.
3. Swanson JW, Holzer CE 3rd, Ganju VK, Jono RT. Violence andpsychiatric disorder in the community: evidence from the Epide-miologic Catchment Area surveys. Hosp Community Psychiatry.1990;41:761-770.
4. Vinkers DJ, de Beurs E, Barendregt M, Rinne T, Hoek HW. Therelationship between mental disorders and different types ofcrime. Crim Behav Ment Health. 2011;21:307-320.
5. Link BG, Stueve A. Psychotic symptoms and the violent/illegalbehavior of mental patients compared to community controls. In:Monahan J, Steadman HJ, eds. Violence and Mental Disorder:Developments in Risk Assessment. Chicago: University of Chi-cago Press; 1996:137-159.
6. Grisso T. Adolescent offenders with mental disorders. FutureChild. 2008;18:143-164.
7. Wasserman G, McReynolds L, Schwalbe CS, Keating JM,Shane AJ. Psychiatric disorder, comorbidity, and suicidal behaviorin juvenile justice youth. Crim Justice Behav. 2010;37:1361-1376.
8. Abram KM, Teplin LA, McClelland GM, Dulcan MK. Comorbidpsychiatric disorders in youth in juvenile detention. Arch GenPsychiatry. 2003;60:1097-1108.
www.jaacap.org 897

COKER et al.
9. Hirschfield P, Maschi T, White HR, Traub LG, Loeber R. Mentalhealth and juvenile arrests: criminality, criminalization, orcompassion? Criminology. 2006;44:593-630.
10. Cuellar AE, Markowitz S, Libby AM. The Relationships BetweenMental Health and Substance Abuse Treatment and JuvenileCrime. Cambridge, MA: National Bureau of EconomicResearch; 2003.
11. National Institute of Justice. 1995 Drug Use Forecasting: AnnualReport on Adult and Juvenile Arrestees. Washington, DC: U.S.Department of Justice, Office of Justice Programs, National Insti-tute of Justice; 1996.
12. Huizinga D, Jakob-Chien C. Contemporaneous co-occurrence ofserious and violent juvenile offending and other problem behav-iors. In: Loeber R, Farrington DP, eds. Serious and Violent JuvenileOffenders: Risk Factors and Successful Interventions. ThousandOaks, CA: SAGE Publications; 1998: 47-67.
13. Thornberry TP, Huzinga D, Loeber R. Prevention of serious de-linquency and violence: implications from the Program ofResearch on the Causes and Correlates of Delinquency. In: HowellJC, Krisberg B, Hawkins JD, Wilson JJ. eds. Sourcebook on Serious,Violent, and Chronic Juvenile Offenders. 1995:213-237.
14. Lawrence RHM. Juvenile Justice: the Essentials. Thousand Oaks,CA: Sage Publications; 2010.
15. Farrington DP, Loeber R. Epidemiology of juvenile violence. ChildAdolesc Psychiatr Clin N Am. 2000;9:733-748.
16. Merikangas KR, Avenevoli S, Costello EJ, Koretz D, Kessler RC.National Comorbidity Survey Replication Adolescent Supplement(NCS-A): I. Background and measures. J Am Acad Child AdolescPsychiatry. 2009;48:367-369.
17. Kessler RC, Avenevoli S, Costello EJ, et al. National ComorbiditySurvey Replication Adolescent Supplement (NCS-A): II. Overviewand design. J Am Acad Child Adolesc Psychiatry. 2009;48:380-385.
18. Kessler RC, Avenevoli S, Costello EJ, et al. Design and field pro-cedures in the U.S. National Comorbidity Survey ReplicationAdolescent Supplement (NCS-A). Int J Methods Psychiatr Res.2009;18:69-83.
19. Swendsen J, Burstein M, Case B, et al. Use and abuse of alcoholand illicit drugs in U.S. adolescents: results of the National Co-morbidity Survey–Adolescent Supplement. Arch Gen Psychiatry.2012;69:390-398.
20. Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ,Poulton R. Prior juvenile diagnoses in adults with mental disorder:developmental follow-back of a prospective-longitudinal cohort.Arch Gen Psychiatry. 2003;60:709-717.
21. Kessler RC, Avenevoli S, Green JG, et al. Methodological studies ofthe Composite International Diagnostic Interview (CIDI) in theU.S. National Comorbidity Survey (NCS). Int J Methods PsychiatrRes. 1998;7:33-55.
JOURN
898 www.jaacap.org
22. Stata Statistical Software: Release 13.0. Version. College Station,TX: StataCorp; 2013.
23. Moffitt TE. Adolescence-limited and life-course-persistent antiso-cial behavior: a developmental taxonomy. Psychol Rev. 1993;100:674-701.
24. Altschuler DM, Brounstein PJ. Patterns of drug use, drug traf-ficking, and other delinquency among inner-city adolescent malesin Washington, D.C. Criminology. 1991;29:589-622.
25. Crowe AH. Drug Identification and Testing in the Juvenile JusticeSystem: Summary. Washington, DC: U.S. Department of Justice,Office of Justice Programs, Office of Juvenile Justice and De-linquency Prevention; 1998.
26. Kratzer LHS. Adult outcomes of child conduct problems: a cohortstudy. J Abnorm Child Psychol. 1997;25:65-81.
27. Steiner H, Garcia IG, Matthews Z. Posttraumatic stress disorder inincarcerated juvenile delinquents. J Am Acad Child Adolesc Psy-chiatry. 1997;36:357-365.
28. Ko SJ, Ford JD, Kassam-Adams N, et al. Creating trauma-informedsystems: child welfare, education, first responders, health care,juvenile justice. Prof Psychol-Res Pract. 2008;39:396-404.
29. Underwood LA, Phillips A, von Dresner K, Knight PD. Criticalfactors in mental health programming for juveniles in correctionsfacilities. Int J Behav Consult Ther. 2006;2:107-140.
30. Huizinga D, Loeber R, Thornberry TP, Cothern L. Co-occurrence ofDelinquency and Other Problem Behaviors. OJJDP. 2000;11:1-8.
31. Schubert CA, Mulvey EP, Glasheen C. Influence of mental healthand substance use problems and criminogenic risk on outcomes inserious juvenile offenders. J Am Acad Child Adolesc Psychiatry.2011;50:925-937.
32. Scott ES, Steinberg L. Adolescent development and the regulationof youth crime. Future Child. 2008;18:15-33.
33. Scott S. IACAPAP e-Textbook of Child and Adolescent MentalHealth. Rey JM, ed. Geneva: International Association for Childand Adolescent Psychiatry and Allied Professions; 2012. J AmAcad Child Adolesc Psychiatry. 2013;52:321-323.
34. National Mental Health Association. Mental Health Treatment forYouth in the Juvenile Justice System: a Compendium of PromisingPractices. Alexandria, VA: National Mental Health Associa-tion; 2004.
35. Jolliffe D, Farrington DP, Hawkins JD, Catalano RF, Hill KG,Kosterman R. Predictive, concurrent, prospective and retrospec-tive validity of self-reported delinquency. Crim Behav MentHealth. 2003;13:179-197.
36. McCord J, Widom CS, Crowell NA. Juvenile Crime, Juvenile Jus-tice. Washington, DC: National Academy Press; 2001.
37. Grant BF, Compton WM, Crowley TJ, et al. Errors in assessingDSM-IV substance use disorders. Arch Gen Psychiatry. 2007;64:379-380. author reply 381-372.
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 53 NUMBER 8 AUGUST 2014
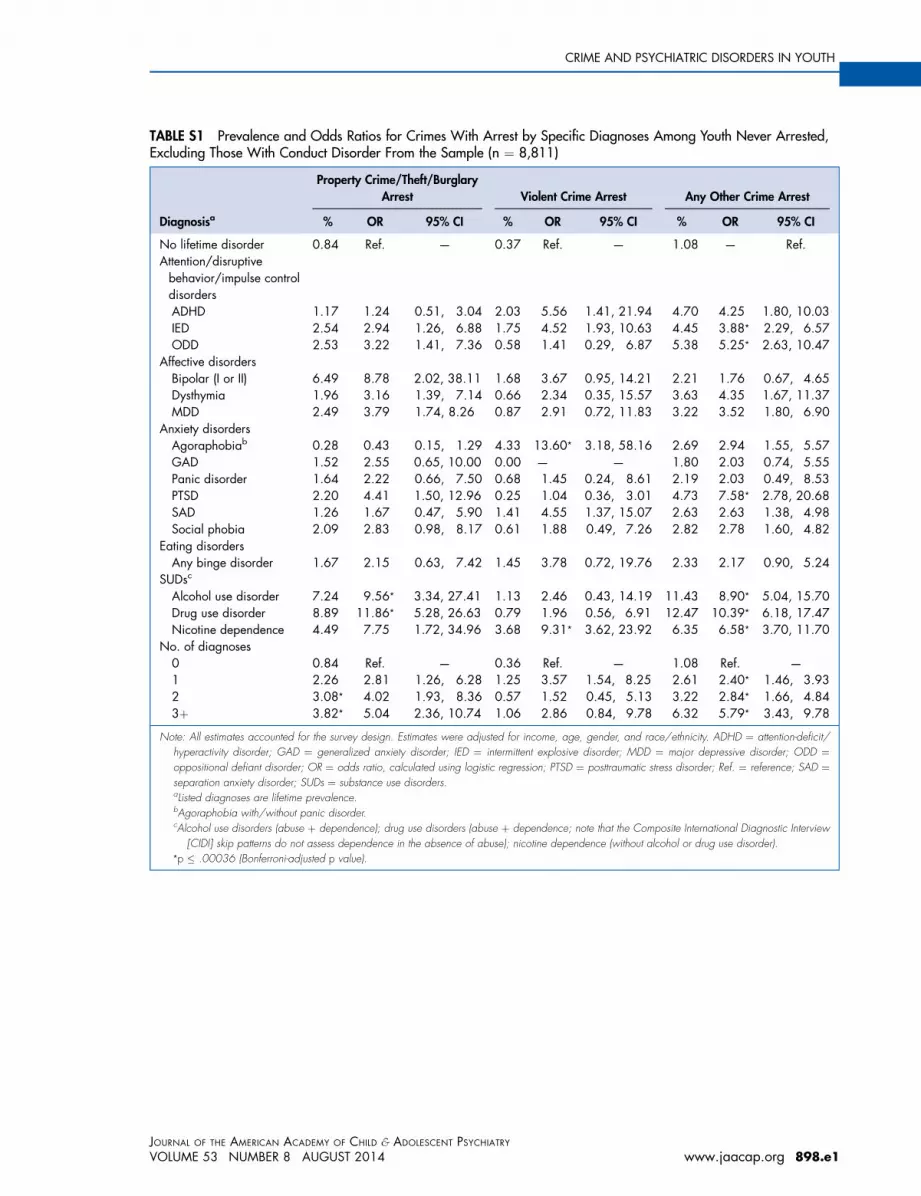
TABLE S1 Prevalence and Odds Ratios for Crimes With Arrest by Specific Diagnoses Among Youth Never Arrested,Excluding Those With Conduct Disorder From the Sample (n ¼ 8,811)
Diagnosisa
Property Crime/Theft/BurglaryArrest Violent Crime Arrest Any Other Crime Arrest
% OR 95% CI % OR 95% CI % OR 95% CI
No lifetime disorder 0.84 Ref. — 0.37 Ref. — 1.08 — Ref.Attention/disruptivebehavior/impulse controldisordersADHD 1.17 1.24 0.51, 3.04 2.03 5.56 1.41, 21.94 4.70 4.25 1.80, 10.03IED 2.54 2.94 1.26, 6.88 1.75 4.52 1.93, 10.63 4.45 3.88* 2.29, 6.57ODD 2.53 3.22 1.41, 7.36 0.58 1.41 0.29, 6.87 5.38 5.25* 2.63, 10.47
Affective disordersBipolar (I or II) 6.49 8.78 2.02, 38.11 1.68 3.67 0.95, 14.21 2.21 1.76 0.67, 4.65Dysthymia 1.96 3.16 1.39, 7.14 0.66 2.34 0.35, 15.57 3.63 4.35 1.67, 11.37MDD 2.49 3.79 1.74, 8.26 0.87 2.91 0.72, 11.83 3.22 3.52 1.80, 6.90
Anxiety disordersAgoraphobiab 0.28 0.43 0.15, 1.29 4.33 13.60* 3.18, 58.16 2.69 2.94 1.55, 5.57GAD 1.52 2.55 0.65, 10.00 0.00 — — 1.80 2.03 0.74, 5.55Panic disorder 1.64 2.22 0.66, 7.50 0.68 1.45 0.24, 8.61 2.19 2.03 0.49, 8.53PTSD 2.20 4.41 1.50, 12.96 0.25 1.04 0.36, 3.01 4.73 7.58* 2.78, 20.68SAD 1.26 1.67 0.47, 5.90 1.41 4.55 1.37, 15.07 2.63 2.63 1.38, 4.98Social phobia 2.09 2.83 0.98, 8.17 0.61 1.88 0.49, 7.26 2.82 2.78 1.60, 4.82
Eating disordersAny binge disorder 1.67 2.15 0.63, 7.42 1.45 3.78 0.72, 19.76 2.33 2.17 0.90, 5.24
SUDsc
Alcohol use disorder 7.24 9.56* 3.34, 27.41 1.13 2.46 0.43, 14.19 11.43 8.90* 5.04, 15.70Drug use disorder 8.89 11.86* 5.28, 26.63 0.79 1.96 0.56, 6.91 12.47 10.39* 6.18, 17.47Nicotine dependence 4.49 7.75 1.72, 34.96 3.68 9.31* 3.62, 23.92 6.35 6.58* 3.70, 11.70
No. of diagnoses0 0.84 Ref. — 0.36 Ref. — 1.08 Ref. —
1 2.26 2.81 1.26, 6.28 1.25 3.57 1.54, 8.25 2.61 2.40* 1.46, 3.932 3.08* 4.02 1.93, 8.36 0.57 1.52 0.45, 5.13 3.22 2.84* 1.66, 4.843þ 3.82* 5.04 2.36, 10.74 1.06 2.86 0.84, 9.78 6.32 5.79* 3.43, 9.78
Note: All estimates accounted for the survey design. Estimates were adjusted for income, age, gender, and race/ethnicity. ADHD ¼ attention-deficit/hyperactivity disorder; GAD ¼ generalized anxiety disorder; IED ¼ intermittent explosive disorder; MDD ¼ major depressive disorder; ODD ¼oppositional defiant disorder; OR ¼ odds ratio, calculated using logistic regression; PTSD ¼ posttraumatic stress disorder; Ref. ¼ reference; SAD ¼separation anxiety disorder; SUDs ¼ substance use disorders.aListed diagnoses are lifetime prevalence.bAgoraphobia with/without panic disorder.cAlcohol use disorders (abuse þ dependence); drug use disorders (abuse þ dependence; note that the Composite International Diagnostic Interview
[CIDI] skip patterns do not assess dependence in the absence of abuse); nicotine dependence (without alcohol or drug use disorder).*p � .00036 (Bonferroni-adjusted p value).
CRIME AND PSYCHIATRIC DISORDERS IN YOUTH
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATR
VOLUME 53 NUMBER 8 AUGUST 2014
Ywww.jaacap.org 898.e1

TABLE S2 Prevalence and Odds Ratios for Crime Among Youth Never Arrested, Based on Specific Diagnoses, ExcludingThose With Conduct Disorder From the Sample (n ¼ 9,537)
Diagnosisa
Committed Property Crime/Theft/Burglary; Not Arrested
Committed Violent Crime;Not Arrested
Committed Any Other Crime;Not Arrested
% OR 95% CI % OR 95% CI % OR 95% CI
No lifetime disorder 3.26 Ref. — 0.49 Ref. — 3.13 Ref. —
Attention/disruptivebehavior/impulse controldisordersADHD 11.99 3.58 1.86, 6.90 3.40 7.60* 2.80, 20.62 12.03 3.99* 2.37, 6.70IED 12.02 3.95* 2.61, 5.98 4.35 9.01* 4.51, 18.03 16.26 6.04* 4.30, 8.48ODD 14.33 5.25* 3.28, 8.41 4.81 6.58* 3.00, 14.43 14.68 5.66* 2.48, 12.95
Affective DisordersBipolar (I or II) 19.38 8.62* 3.94, 18.88 4.85 12.11 2.55, 57.51 13.51 5.47 2.08, 14.42Dysthymia 14.69 6.19* 3.06, 12.50 4.33 13.08* 3.80, 45.05 7.96 3.06* 1.81, 5.18MDD 8.37 3.28* 2.02, 5.35 2.19 5.00* 2.66, 9.42 10.32 4.14* 2.84, 6.02
Anxiety DisordersAgoraphobiab 9.70 4.54 2.08, 9.92 1.04 2.67 0.62, 8.24 12.08 6.26* 2.74, 14.29GAD 6.52 2.39 1.09, 5.21 1.73 4.75 1.47, 15.26 7.46 2.78 1.35, 5.76Panic disorder 9.72 3.29 1.57, 6.89 2.25 5.13* 2.45, 10.71 8.87 3.12 0.73, 13.35PTSD 14.90 8.25* 4.86, 14.00 5.24 15.15* 6.07, 37.80 15.66 8.90* 5.18, 15.27SAD 8.15 3.04* 1.89, 4.87 1.79 3.93 1.39, 11.06 5.84 2.25 1.15, 4.41Social Phobia 6.78 2.32 1.39, 3.88 1.09 2.37 1.13, 4.98 8.49 3.01* 2.03, 4.47
Eating DisordersAny binge disorder 6.93 3.93* 2.24, 6.89 4.25 8.84 2.98, 26.20 12.02 4.74* 2.71, 8.29
SUDsc
Alcohol use disorders 25.04 8.90* 5.18, 15.29 9.80 28.83* 10.65, 78.61 34.34 13.60* 8.53, 21.70Drug use disorders 27.63 10.34* 6.88, 15.54 11.29 25.86* 11.78, 56.78 34.22 14.12* 10.31, 19.33Nicotine dependence 10.19 3.13 1.28, 7.68 2.36 7.21 2.56, 20.32 11.72 4.15* 2.13, 8.10
No. of diagnoses0 3.28 Ref. — 0.49 Ref. — 3.13 Ref. –
1 6.71 2.12 1.31, 3.45 1.39 2.93 1.22, 7.06 8.63 2.89* 1.99, 4.202 10.08 3.30* 2.32, 4.70 2.53 5.35* 2.25, 12.72 11.89 4.11* 2.71, 6.233þ 14.22 5.24* 3.64, 7.54 5.20 11.44* 6.29, 20.80 17.43 6.74* 4.67, 9.72
Note: All estimates accounted for the survey design. Estimates were adjusted for income, age, gender, and race/ethnicity. ADHD ¼ attention-deficit/hyperactivity disorder; GAD ¼ generalized anxiety disorder; IED ¼ intermittent explosive disorder; MDD ¼ major depressive disorder; ODD ¼oppositional defiant disorder; OR ¼ odds ratio, calculated using logistic regression; PTSD ¼ posttraumatic stress disorder; SAD ¼ separation anxietydisorder; SUDs ¼ substance use disorders.aThe listed diagnoses are lifetime prevalence.bAgoraphobia with/without panic disorder.cAlcohol use disorders (abuse þ dependence); drug use disorders (abuse þ dependence; note that the Composite International Diagnostic Interview
[CIDI] skip patterns do not assess dependence in the absence of abuse); nicotine dependence (without alcohol or drug use disorder).*p � .00036 (Bonferroni-adjusted p value).
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
898.e2 www.jaacap.org VOLUME 53 NUMBER 8 AUGUST 2014
COKER et al.
Related Documents