Cranial Nerves 8 th :vestibulocochlear N. 9 th : glossopharyngeal N. 10 th : vagus N. 11 th : accessory N. 12 th : hypoglossal N.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cranial Nerves8th:vestibulocochlear N.9th : glossopharyngeal N. 10th: vagus N.11th: accessory N.12th: hypoglossal N.
Done by shaima’a Hmaid

Vestibulo cochlear n.(CN VIII)
Type: special sensory n. that convey the special senses from the inner ear to brain stem.
formed of 2 parts
(1)cochlear part: carrying hearing impulses from the organ of corti in the cochlea.
( 2)Vestibular part: carrying equilibrium impulses Course : is very short, leaves at pontomedullary junction, it enters
internal auditory meatus with facial n. and labyrinthine artery, where it travels within the auditory
canal of the petrous temporal bone .• within the petrous bone it split in to:
_ the cochlear nerve (formed of spiral ganglion) ends in the cochlea.
_ the vestibular nerve (formed of vestibular ganglion) ends in the utricle, saccule and the 3 semicircal canals .


The auditory pathways:

-Each central process of cochlear parts of the eight cranial divides as it enters the brainstem.
-One branch goes to the dorsal cochlear nucleus and the other one to the ventral cochlear nucleus.
-The neurons consisting the auditory pathways ascend from the cochlear nuclei to the inferior colliculi of midbrain.
-Many neurons make intermediate synaptic connections in superior olivary nuclei located at level of pontomedullary junction.
-The superior olivary nuclei determine the delay between sounds forms each ear and thus determine the direction of the origin of sound.
-The directly projecting neurons synapse in contra lateral inferior colliculus

-But those that synapse in the superior olivary nucleus project to both colliculi post_synaptic neurons project from the inferior colliculus to the medial geniculate nucleus of thalamus.
-Neurons project from the thalamus via the sublentiform part of the internal capsule to the auditory cortex in the temporal lobe of the cerebral hemisphere.

The vestibular pathways:
-The structures in the inner ear
served by the vestibular components
provides information to CNS, which
plays a major part in maintaining equilibrium.
-The vestibular parts of vestibulocochlear nerves originate from receptor cells in the various parts of vestibular labyrinth and join with cochlear portion to follow the same route to brainstem.
-Their cell bodies form vestibular ganglion close to the lateral end of the internal acoustic meatus, their central processes constitute the vestibular nerve.
Most of the central processes synapse in vestibular nuclei of the brainstem which make connections with the cerebellum, spinal cord brainstem and cerebral cortex, but some pass directly to the cerebellum.

Clinical correlation of CNVIII
-Due to close relationship of the vestibular nerve and cochlear nerve, lesions of one usually effect the other, Leading to both tinnitus, vertigo and impaired hearing.
-In fact usually the cause of vertigo after head trauma is a peripheral vestibular nerve lesion.
There are two forms of hearing loss:
-Conductive hearing loss –CNV lll is working but bone conduction of sound is impaired, due to the external auditory canal/middle ear not transmitting sound waves .
-Sensor neural hearing loss-physical ear structures are preserved, however there is damage to the cochlea or neuron that is impairing hearing .

GLOSSOPHARYNGEAL NERVES (CNIX)
Type: Mixed n. containing sensory, motor and parasympathitic fibers.
Glossopharyngeal nerve nuclei :
.
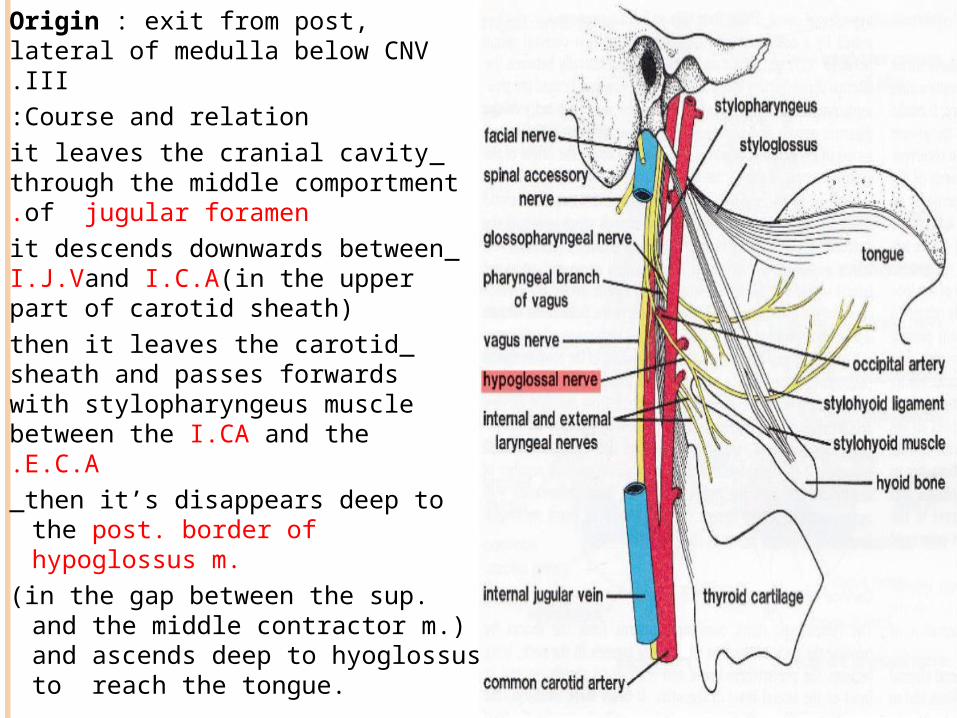
Origin : exit from post, lateral of medulla below CNV III.Course and relation:
_it leaves the cranial cavity through the middle comportment of jugular foramen.
_it descends downwards between I.J.Vand I.C.A(in the upper part of carotid sheath)
_then it leaves the carotid sheath and passes forwards with stylopharyngeus muscle between the I.CA and the E.C.A._then it’s disappears deep to the
post. border of hypoglossus m.
(in the gap between the sup. and the middle contractor m.) and ascends deep to hyoglossus to reach the tongue.

Termination : it ends by dividing in to terminal branches supplying the mucous membranes of pharynx, tonsil and post.1/3 of tongue.
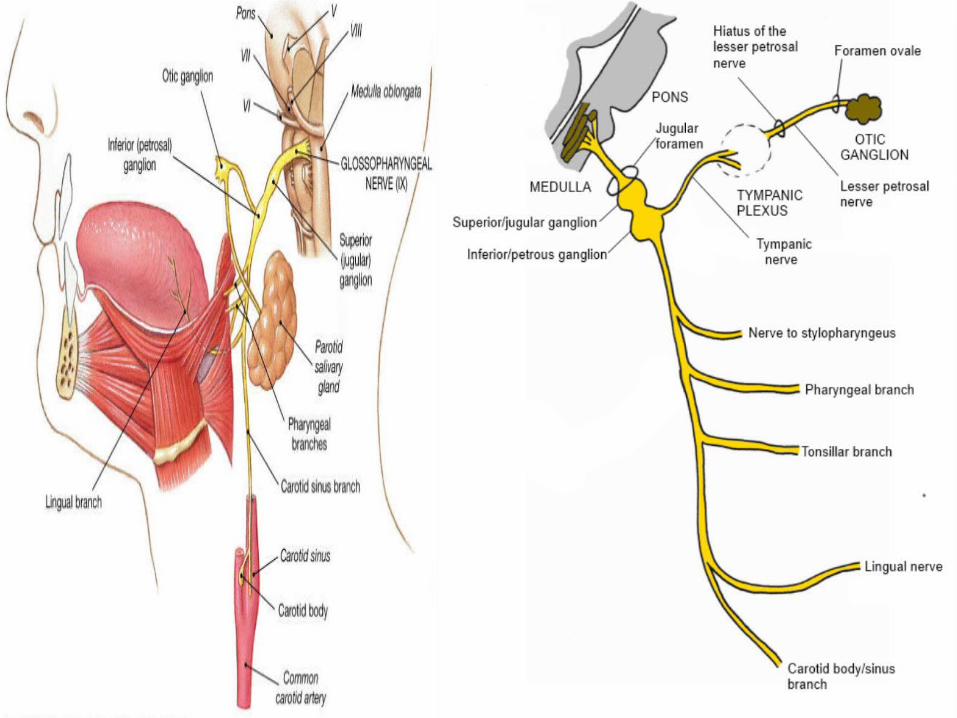
Ganglia of glossopharyngyal : it has 2 sensory ganglia in the jugular foramen:
(1) sup. Ganglion : small and gives no branch.
(2) Inf. ganglion: large and give tympanic branch.

Branches:1. Maningeal branch : sensory to the meninges of post. Cranial fossa.
2. Carotid branch : General visceral sensory neurons in the glossopharyngeal n.supply barorecptors in the carotid sinus and the chemoreceptors in the carotid body, the cell bodies of these fibers are situated in the inferior ganglion of the nerve, Their central processes enter the tractus solitarius and end in caudal part of its nucleus.
3. Nerve to stylopharyngeus n.: derived from the third pharyngeal arch. The special visceral motor neurons to this muscle begin in the rostral part of the nucleus ambiguus
4. Tonsillar branch(sensory):shares the lesser palatine n. in supplying palatine tonsil
5. pharyngeal branches(sensory):they enter in the formation of pharyngeal plexus on lat. surface of the middle constrictor m. of pharynx
the pharyngeal plexus receives also :
- motor branch: the pharyngeal branch of vagus
- sympathatic branch: the pharyngeal branch of the superior cervical sympathetic ganglion.
6. Terminal lingual branches : supply general and taste sensations to the post 1/3of tongue.
.
(7 )Tympanic branch : preganglionic visceral motor fibers in glossopharyngeal n. begin in the inferior salivatory nucleus .
-Origin : arise from inf. ganglion of glossopharyngeal n. in the jugular fossa.
-course: 1 -it reaches the middle ear cavity where it breaks to
form the tympanic plexus. 2 -lesser S. petrosal nerve arise from the tympanic
plexus and reaches the middle cranial fossa via hiatus carrying its name.
3 -then the lesser S. petrosal n. pass through the foramen ovale to reach the infra temporal fossa to relay in the otic ganglion.
4 -the postganglionic fibers join the auriculotemporal n. to reach parotid gland.
Clinical Correlation of CNIX
-The most frequent causes of damage to the nerve are by compression from space _occupying lesions in pharynx or posterior tongue or invasion by malignant tumors in these areas.
-when they occur, taste is absent on the post.1\3 of tongue, alongside an absence of the gag reflex.
-the sensory nerves from the pharynx are the afferent components of the gag reflex which is stimulated by touching the pharyngeal wall with a blunt object with the mouth closed .
Vagus Nerveo Type: mixed nerve containing: parasympathatic, motor and
sensory fiberso origin: from posterior lateral surface of medulla o vagus nerve nuclei : main motor nucleus
This nucleus lies deep in the reticular formation of medulla oblongata and is formed by the nucleus ambiguus
parasympathatic nucleus
This nucleus forms the dorsal nucleus of the vagus sensory nucleus
This nucleus is the lower part of the nucleus of tractus solitarius
sensation of taste travel through the peripheral axons of nerve cells situated in the inferior ganglion on the vagus nerve
Affrent information concerning common sensation enter the brain stem through the superior ganglion of the vagus nerve but end in the spinal nucleus of trigeminal nerve

Course and relations in the neck : it leaves the cranial cavity through
the middle compartment of the
jugular foramen, here it has 2
sensory ganglia: sup. Ganglion( in the jugular f.) inferior ganglion ( just below
the jugular foramen). The cranial root of accessory
nerve joins the inferior ganglion of vagus just below the jugular f. The vagus descend vertically downwards inside the carotid
sheath :
-First between I.J.V and I.C.A ( passing with them deep to styloid apparatus and posterior belly of digastric ) till the upper border of thyroid cartilage.
-lower than, it descends between the I.J.V and C.C.A At the root of the neck, the vagus nerve crosses infront of first
part of subclavian artery to enter the thorax

Branches of the vagus in the neck: 2 branches arise from the sup. Ganglion:
I. meningeal br. Sensory to the dura matter of the post. cranial fossa
II. auricular br. Sensory to the skin of medial side of auricle, post. Wall of external auditory meatus and tympanic membrane.
2 branches arise from the inferior ganglion
I. Pharyngeal branch ( motor) - its fibers are mostly derivesd from the cranial accessory nerve and supply the pharyngeal m. ( except the stylopharyngeal m.) + all muscle of the soft palat ( except the tensor palatine muscle)
II. superiorlaryngeal nerve (mixed)
- its divided into
A. internal laryngeal nerve ( sensory ): accompanies the sup. Laryngeal artery and supply the mucous membrane of the upper ½ of larynx.
B. external laryngeal nerve (motor) : supply cricothyroid muscle.


2 cardiac branches : superior and inferior (parasympathetic)
recurrent laryngeal nerve: mixed ( motor and sensory)
I. right recurrent laryngeal nerve
II. Left recurrent laryngeal nerve- Branches of each recurrent laryngeal nerve :
A. motor: to all laryngeal muscle ( except cricothyroid ) and it also gives a branches to trachea, esophagus and inferior constrictor muscle of pharynx.
B. Sensory : to the mucous membrane of the lower ½ of larynx (below focal cords)
Clinical correlation - The vagus nerve are relatively deep and are affected mainly
by – occupying lesions compressing the nerve or invasion by malignant tumors
-The major cause of damage to the vagus nerve is usually through damage to nuclei through brainstem stroke.
-loss of innervations of a laryngeal muscles will produce dysphonia .
- paralysis of muscle of soft palate will also affect those components of speech requirement movement of the soft palate, producing some degree of dysatheria.
-deficiency of muscle activity in the pharynx produces difficulty with swallowing ( dysphagia ) commonly any dysphagia can lead to aspiration pneumonia due to impaired swallowing in an individual and its frequently a cause of a death.
- Lesion to the recurrent laryngeal nerve lead to horsenence or absence of voice as a symptom of vagus nerve palsy.

accessory nerve Type: purely motor nerve origin : it arises by 2 roots : cranial and spinalo cranial root : formed from the axons of nerve cell of
nucleus ambiguus (arises from posterolateral sulcus of medulla )
o Spinal root : formed from axon of nerve cells in the spinal nucleus ( arise from the upper 5 or 6 cervical segment of the spinal cord)
Course and relation :1. the spinal root ascends through the foramen magnum to join the
cranial root inside the cranial cavity.
2. the united accessory nerve leave the cranial cavity through the middle compartment of the jugular foramen.
3. Just below the jugular foramen the 2 roots of accessory nerve separate from each other
4. The cranial root join the inferior ganglia of vagus nerve and is distributed with its pharyngeal an laryngeal branches.
5. The spinal root : has the following course in the neck
A. it descends inside the upper part of the carotid sheath deep to styloid apparatus and between I.J.V and the I.C.A
B. Then it passes backwards between I.J.V and posterior belly of digastric muscle
C. It pierces the deep surface of sternomastoid muscles, supplying it then it emerges from its posterior border above its middle
D. It crosses the posterior triangle of the neck
E. Finally it pierces the posterior border of trapezius muscle about 5cm about the clavicle and ends by supplying it


Branches of accessory nerve
1. the cranial accessory nerve : joins the vagus nerve and distributed with its :
A. pharyngeal br. : supplying all muscle of pharynx ( except stylopharyngius ) and all muscles of palate (except tensor palatine muscles)
B. Laryngeal branch : supplying the muscle of the larynx
2. The spinal accessory nerve: supplies 2 muscles :
C. sternomastoid
D. trapezius

clinical correlation of CNXI
Lesion of spinal part of accessory nerve may occur anywhere along its course and may result from tumors or trauma from stab or gunshot wounds in the neck.
Lesion of the spinal part of accessory nerve will result in paralysis of the sternocledomastoid and trapezius muscles.
The sternocledomastoid muscle will atrophy and there will be weakness in turning the head to the opposite side.
the trapezius muscle will also atrophy and the shoulder will drop into that side, there will be also weakness an difficulty in rising the arm about the horizontal.
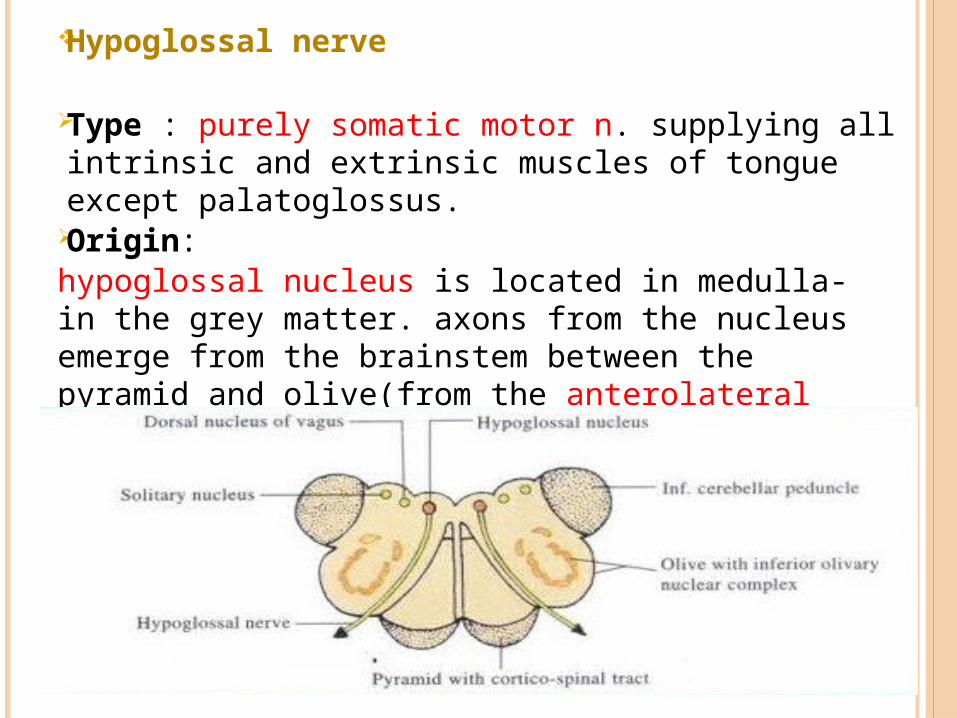
Hypoglossal nerve
Type : purely somatic motor n. supplying all intrinsic and extrinsic muscles of tongue except palatoglossus.
Origin:-hypoglossal nucleus is located in medulla in the
grey matter. axons from the nucleus emerge from the brainstem between the pyramid and olive(from the anterolateral sulcus of medulla).
-It leaves cranuim via hypoglossal canal ang receives a communicating branch from C1 .
i

Course and relations:
-it leave the cranial cavity through the ant. condylar foramen then forms a half spiral turn around vagus nerve.
-then it descends vertically
downwards inside the upper
part of carotid sheath superficial
to vagus n. between I.J.V and I.C.A.
-it descends deep to the
styloid process. styloid muscle and post. belly of digastrics muscle.
-then it turns forwards crossing the following structures: (a ). .I C A ) ( b occipital . ) ( a c . .E C A ) ( d t he loop of
lingual a.

-it disappears deep to the intermediate tendon of digastrics m. to reach the submandibular region where it runs on hyoglossus m. and covered superficially by submandibular gland.
-it disappears deep to mylohyoid m. below the lingual n. and submandibular duct.
-finally it dips in the interval between the hyoglossus and genioglossus where it breaks in to the terminal branches supplying the muscle of the tongue.(except palatoglossus).

Branches: arising from hypoglossal n. itself innervates all of
the intrinsic and most of the extrinsic muscle of the tongue ( genioglossus, styloglossus and hyoglossus muscles) except palatoglossus m.
derived from C1 joining hypoglossus.
(1 )Meningeal br.(sensory)to dura mater (2 )n. to geniohyoid m
(3 )n. to thyrohyoid m .(4 )descendents hypoglossai forming the sup limb of
ansacervicalis (supplying infrahyoid mucsles )


Clinical correlation of CNXII
-upper motor neurons that control tongue movement decussate within the corticobulbar tracts before arriving at the hypoglossal nuclei.
-This means UMN lesions of primary motor cortex cause contra lateral weakness of the tongue, whereas LMN lesions of the hypoglossal nuclei cause ipsilateral weakness of the tongue.
-Tongue weakness causes
the tongue upon protrusion
to deviate towards the weak
side due to overactive
compensatory action of the
other hypoglassal n.-CNIII damage also cause
tongue muscle to atrophy.

Thank youThank you
Related Documents






